
Perspectives and Factors Affecting the Preventive Behavior Pertinent to COVID-19 among School Employees in Chiang Mai, Thailand: A Cross-Sectional Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
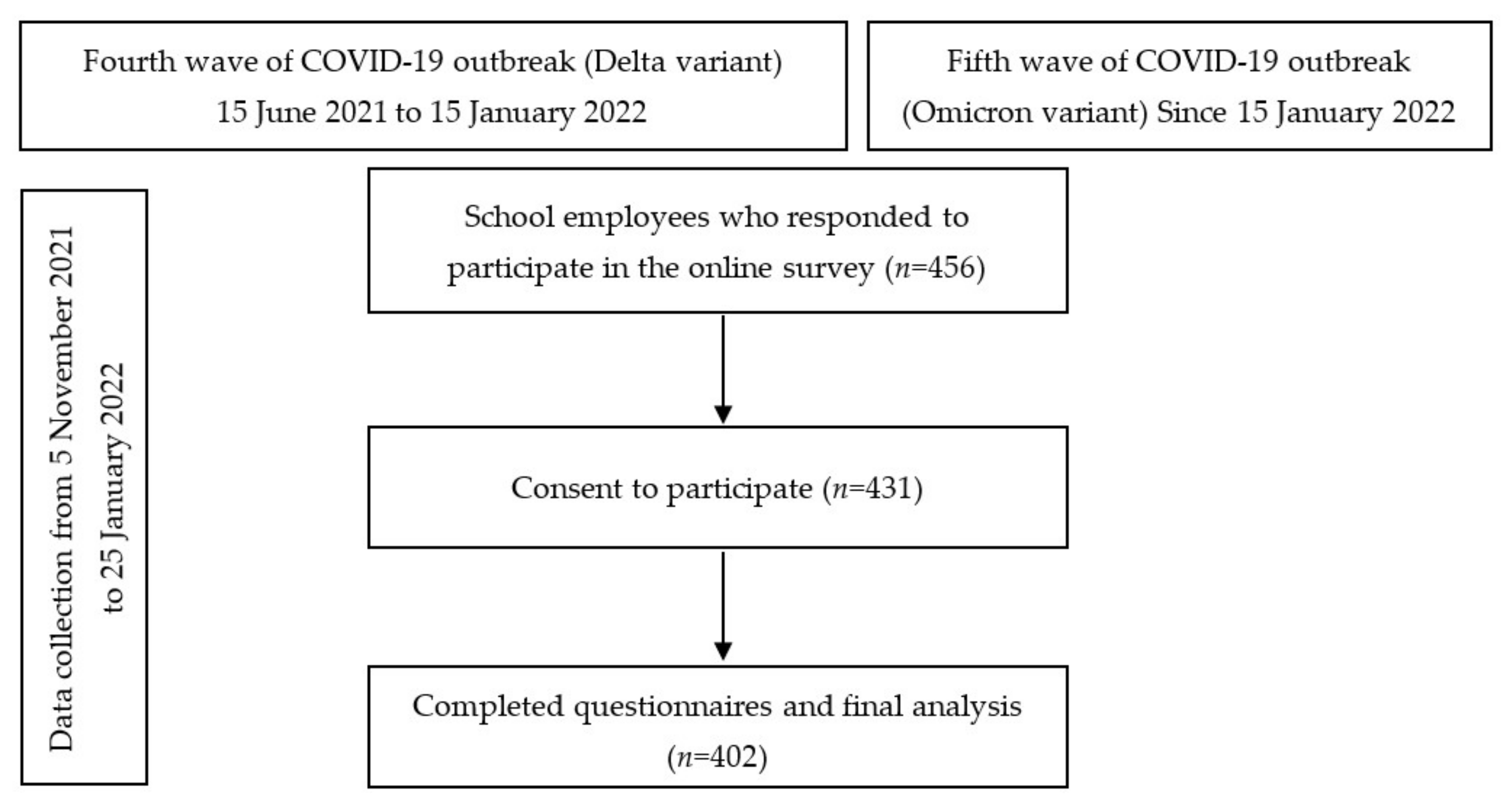
2.1. Study Design and Participants
2.2. Questionnaire Design
- (1)
- Personal information including socio-demographic characteristics (age, gender, and household income), occupational information (length of working’s experience, school affiliation, and school roles), personal preventive activities (COVID-19 vaccination status and cost of COVID-19 prevention per month)
- (2)
- School employees perceptions of the readiness of the school and employees for the re-opening of the school for on-site education (possible answers were the four categories: “strongly agree”, “agree”, “disagree”, and “strongly disagree”) and the employees concerns regarding the re-opening of schools for on-site education (again, possible answers were from four categories: “very concerned and do not agree with school opening”, “very concerned but agree with school opening”, “moderately concerned and agree with school opening”, and “slightly concerned”)
- (3)
- The questions for assessing school employees’ agreement and actions on COVID-19 preventive practices were designed in accordance with the measures and recommendations for school employees in the prevention of the spread of the epidemic of COVID-19 in Thailand. These measures and recommendations were developed by the national committee, including public health experts and infectious disease specialists from the department of health, and educational experts from the ministry of education. These consisted of eleven preventive measures to be performed by the employees to prevent the spread of the disease in school. This part of questionnaire was divided into two sub sections including the participant’s opinion with regard to every measure (possible answers being “agree” or “disagree” to each measure) and what were the actions of the participants as regards the carrying out of these preventive measures (possible answers were “consistently performed”, “partially performed”, and “not performed”). The reliability test of 11 questions for assessing school employees’ agreements and actions in accordance with the preventive measures obtained a Cronbach’s coefficient alpha of 0.83 and 0.89, respectively (Table S1).
2.3. Statistical Analysis
2.4. Ethical Considerations
3. Results
3.1. Characteristics of the Participants
3.2. Opinion Regarding the Measures and Recommendations for School Re-Opening
3.3. Factors Affecting the Action of Participants
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Health Organization Coronavirus (COVID-19) Dashboard, Thailand Situation. Available online: https://covid19.who.int/region/searo/country/th (accessed on 1 March 2022).
- Department of Disease Control of Thailand. Thailand Coronavirus (COVID-19) Dashboard. Available online: https://ddc.moph.go.th/viralpneumonia (accessed on 1 March 2022).
- Vermund, S.H.; Pitzer, V.E. Asymptomatic Transmission and the Infection Fatality Risk for COVID-19: Implications for School Reopening. Clin. Infect. Dis. 2021, 72, 1493–1496. [Google Scholar] [CrossRef] [PubMed]
- Mukhtar, K.; Javed, K.; Arooj, M.; Sethi, A. Advantages, Limitations and Recommendations for online learning during COVID-19 pandemic era. Pak. J. Med. Sci. 2020, 36, S27–S31. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Guidance for COVID-19 Prevention in K-12 Schools. Available online: https://www.cdc.gov/coronavirus/2019-ncov/community/schools-childcare/k-12-guidance.html (accessed on 1 March 2022).
- Occupational Safety and Health Administration. Protecting Workers: Guidance on Mitigating and Preventing the Spread of COVID-19 in the Workplace. Available online: https://www.osha.gov/coronavirus/safework (accessed on 1 March 2022).
- Department of Health of Thailand. The Practices for School Employees in Prevention of the Spread of the Epidemic of COVID-19 in Thailand. Available online: http://www.oic.go.th/fileweb/cabinfocenter17/drawer002/general/data0002/00002647.pdf (accessed on 1 March 2022).
- Nguyen, N.P.T.; Hoang, T.D.; Tran, V.T.; Vu, C.T.; Siewe Fodjo, J.N.; Colebunders, R.; Dunne, M.P.; Vo, T.V. Preventive behavior of Vietnamese people in response to the COVID-19 pandemic. PLoS ONE 2020, 15, e0238830. [Google Scholar] [CrossRef] [PubMed]
- Prem, K.; Liu, Y.; Russell, T.W.; Kucharski, A.J.; Eggo, R.M.; Davies, N.; Jit, M.; Klepac, P.; Flasche, S.; Clifford, S.; et al. The effect of control strategies to reduce social mixing on outcomes of the COVID-19 epidemic in Wuhan, China: A modelling study. Lancet Public Health 2020, 5, e261–e270. [Google Scholar] [CrossRef] [Green Version]
- Gutu, B.; Legese, G.; Fikadu, N.; Kumela, B.; Shuma, F.; Mosisa, W.; Regassa, Z.; Shiferaw, Y.; Tesfaye, L.; Yohannes, B.; et al. Assessment of preventive behavior and associated factors towards COVID-19 in Qellam Wallaga Zone, Oromia, Ethiopia: A community-based cross-sectional study. PLoS ONE 2021, 16, e0251062. [Google Scholar] [CrossRef] [PubMed]
- Karout, L.; Serwat, A.; El Mais, H.; Kassab, M.; Khalid, F.; Ruiz Mercedes, B. COVID-19 Prevalence, Risk Perceptions, and Preventive Behavior in Asymptomatic Latino Population: A Cross-Sectional Study. Cureus 2020, 12, e10707. [Google Scholar] [CrossRef] [PubMed]
- Machida, M.; Nakamura, I.; Saito, R.; Nakaya, T.; Hanibuchi, T.; Takamiya, T.; Odagiri, Y.; Fukushima, N.; Kikuchi, H.; Amagasa, S.; et al. The actual implementation status of self-isolation among Japanese workers during the COVID-19 outbreak. Trop. Med. Health 2020, 48, 63. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, B.G.; Mahendraratnam, N.; Nguyen, T.V.; Benzing, L.; Beliveau, J.; Silcox, C.; Wong, C.A. Factors Associated with Initial Public School Reopening Plans During the US COVID-19 Pandemic: A Retrospective Study. J. Gen. Intern. Med. 2021, 36, 852–854. [Google Scholar] [CrossRef] [PubMed]
- Soh, S.M.; Kim, Y.; Kim, C.; Jang, U.S.; Lee, H.R. The rapid adaptation of SARS-CoV-2-rise of the variants: Transmission and resistance. J. Microbiol. 2021, 59, 807–818. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus 2019 (COVID-19) WHO Thailand Weekly Situation Update—15 Feb 2022 no. 223. Available online: https://reliefweb.int/sites/reliefweb.int/files/resources/2022_02_15_tha-sitrep-223-covid-19_eng.pdf (accessed on 1 March 2022).
- Levinson, M.; Cevik, M.; Lipsitch, M. Reopening Primary Schools during the Pandemic. N. Engl. J. Med. 2020, 383, 981–985. [Google Scholar] [CrossRef] [PubMed]
- Lizana, P.A.; Vega-Fernadez, G.; Gomez-Bruton, A.; Leyton, B.; Lera, L. Impact of the COVID-19 Pandemic on Teacher Quality of Life: A Longitudinal Study from before and during the Health Crisis. Int. J. Environ. Res. Public Health 2021, 18, 3764. [Google Scholar] [CrossRef] [PubMed]
- Vargas Rubilar, N.; Oros, L.B. Stress and Burnout in Teachers During Times of Pandemic. Front Psychol. 2021, 12, 756007. [Google Scholar] [CrossRef] [PubMed]
- Hepburn, S.J.; Carroll, A.; McCuaig, L. Exploring a Complementary Stress Management and Wellbeing Intervention Model for Teachers: Participant Experience. Int. J. Environ. Res. Public Health 2021, 18, 9009. [Google Scholar] [CrossRef] [PubMed]
- Solís García, P.; Lago Urbano, R.; Real Castelao, S. Consequences of COVID-19 Confinement for Teachers: Family-Work Interactions, Technostress, and Perceived Organizational Support. Int. J. Environ. Res. Public Health 2021, 18, 11259. [Google Scholar] [CrossRef] [PubMed]
- Stojanovic, J.R.V.; Boccia, S.; Bacon, S.L.; Lavoie, K.L.; iCARE Study Team. Public perceptions and behavioural responses to the first COVID-19 pandemic wave in Italy: Results from the iCARE study. Eur. J. Public Health 2021, 31, 1270–1277. [Google Scholar] [CrossRef] [PubMed]
- Meng, N.; Liu, Z.; Wang, Y.; Feng, Y.; Liu, Q.; Huang, J.; Li, X. Beyond Sociodemographic and COVID-19-Related Factors: The Association Between the Need for Psychological and Information Support from School and Anxiety and Depression. Med. Sci. Monit. 2021, 27, e929280. [Google Scholar] [CrossRef] [PubMed]
- Esposito, S.; Cotugno, N.; Principi, N. Comprehensive and safe school strategy during COVID-19 pandemic. Ital. J. Pediatrics 2021, 47, 6. [Google Scholar] [CrossRef] [PubMed]
- Huber, S.G.; Helm, C. COVID-19 and schooling: Evaluation, assessment and accountability in times of crises-reacting quickly to explore key issues for policy, practice and research with the school barometer. Educ. Assess. Eval. Account. 2020, 32, 237–270. [Google Scholar] [CrossRef] [PubMed]
- Many Schools in Thailand Hit by COVID-19 Clusters after Reopening. Available online: https://newsinfo.inquirer.net/1548787/many-schools-in-thailand-hit-by-covid-19-clusters-after-reopening (accessed on 1 March 2022).
- Centers for Disease Control and Prevention. Omicron Variant: What You Need to Know. Available online: https://www.cdc.gov/coronavirus/2019-ncov/variants/omicron-variant.html (accessed on 1 March 2022).
- Panovska-Griffiths, J.; Kerr, C.C.; Stuart, R.M.; Mistry, D.; Klein, D.J.; Viner, R.M.; Bonell, C. Determining the optimal strategy for reopening schools, the impact of test and trace interventions, and the risk of occurrence of a second COVID-19 epidemic wave in the UK: A modelling study. Lancet Child Adolesc. Health 2020, 4, 817–827. [Google Scholar] [CrossRef]
- Goldhaber-Fiebert, J.D.; Studdert, D.M.; Mello, M.M. School Reopenings and the Community During the COVID-19 Pandemic. JAMA Health Forum 2020, 1, e201294. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristics | n = 402 | |
|---|---|---|
| n | % | |
| Age (years), mean ± SD | 38.4 | ±11.1 |
| Gender | ||
| Female | 299 | 74.4 |
| Male | 103 | 25.6 |
| School affiliation | ||
| Government school | 65 | 16.2 |
| Private school | 317 | 78.9 |
| Demonstration school | 20 | 4.9 |
| Length of working’s experience, median (IQR) | 10 | (4–20) |
| School roles | ||
| Teaching | 362 | 90.1 |
| Non-teaching | 40 | 9.9 |
| Income (baht/month) | ||
| ≤20,000 | 209 | 52.0 |
| 20,001–30,000 | 119 | 29.6 |
| 30,001–40,000 | 28 | 7.0 |
| 40,001–50,000 | 30 | 7.4 |
| 50,001–60,000 | 12 | 3.0 |
| >60,000 | 4 | 1.0 |
| Cost for COVID-19 prevention (baht/month) | ||
| <100 | 58 | 14.4 |
| 100–300 | 176 | 43.8 |
| >300 | 168 | 41.8 |
| COVID-19 vaccination | ||
| No | 11 | 2.7 |
| Incomplete | 26 | 6.5 |
| Complete | 365 | 90.8 |
| COVID-19 Prevention Measures | Agreement | Action | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Agree | Disagree | Consistently Performed | Partially Performed | Not Performed | ||||||
| n | (%) | n | (%) | n | (%) | n | (%) | n | (%) | |
| 1. You must follow the information on the epidemic situation from reliable sources. | 400 | 99.5 | 2 | 0.5 | 387 | 96.3 | 15 | 3.7 | - | - |
| 2. You must observe your own abnormal symptoms. If there are any respiratory symptoms, you should stop working and consult a medical team immediately. | 400 | 99.5 | 2 | 0.5 | 388 | 96.5 | 11 | 2.7 | 3 | 0.8 |
| 3. You must strictly follow preventive measures such as washing your hands often, wearing a cloth mask or a mask and keeping distance between people and avoid going to crowded places. | 402 | 100.0 | - | - | 393 | 97.8 | 9 | 2.2 | - | - |
| 4. You must inform parents of supervising students bringing their own personal items and protective equipment to school. | 399 | 99.3 | 3 | 0.7 | 379 | 94.3 | 20 | 5.0 | 3 | 0.7 |
| 5. You must communicate knowledge. Advice or provision of public relations materials to prevent and reduce the risk of spreading COVID-19. | 399 | 99.3 | 3 | 0.7 | 370 | 92.0 | 27 | 6.7 | 5 | 1.3 |
| 6. You must clean the teaching aids or equipment that is a high-risk touch point after every use. | 397 | 98.8 | 5 | 1.2 | 379 | 94.3 | 19 | 4.7 | 4 | 1.0 |
| 7. You must supervise the seating arrangements within the school premises in accordance with the basic principle, the distance between people is at least 1–2 m. | 399 | 99.3 | 3 | 0.7 | 382 | 95.0 | 18 | 4.5 | 2 | 0.5 |
| 8. You must inspect, supervise, and follow up on student attendance. | 400 | 99.5 | 2 | 0.5 | 386 | 96.0 | 13 | 3.2 | 3 | 0.8 |
| 9. You must perform health screening for everyone who enters the school according to the procedures. | 392 | 97.5 | 10 | 2.5 | 379 | 94.3 | 19 | 4.7 | 4 | 1.0 |
| 10. You must observe groups of students with behavioural problems or students who do not cooperate with the measures set by the teacher in order to receive assistance. | 400 | 99.5 | 2 | 0.5 | 384 | 95.5 | 13 | 3.2 | 5 | 1.3 |
| 11. You must communicate your knowledge of stress and the stress management process for students and personnel in educational institutions. | 396 | 98.5 | 6 | 1.5 | 367 | 91.3 | 30 | 7.5 | 5 | 1.2 |
| Perceptions of School’s Employees | Strongly Agree | Agree | Disagree | Strongly Disagree | ||||
| n | (%) | n | (%) | n | (%) | n | (%) | |
| Your school was ready for on-site education. | 186 | 46.3 | 181 | 45.0 | 24 | 6.0 | 11 | 2.7 |
| Your school staff were ready for on-site education. | 199 | 49.5 | 181 | 45.0 | 16 | 4.0 | 6 | 1.5 |
| School Employees Concerns | Very Concerned and not Agree with School Opening | Very Concerned but Agree with School Opening | Moderately Concerned and Agree with School Opening | Slightly Concerned | ||||
| n | (%) | n | (%) | n | (%) | n | (%) | |
| Concerned regarding school re-opening for on-site education. | 90 | 22.4 | 180 | 44.8 | 98 | 24.4 | 34 | 8.4 |
| Factors | aOR | 95% CI | p-Value |
|---|---|---|---|
| Characteristics | |||
| Age | 1.03 | 0.98 to 1.08 | 0.263 |
| Gender | |||
| Male | 0.43 | 0.23 to 0.80 | 0.008 ** |
| Female | (ref.) | ||
| School affiliation | |||
| Private school | 1.52 | 0.70 to 3.28 | 0.289 |
| University demonstration school | 0.76 | 0.16 to 3.42 | 0.724 |
| Government school | (ref.) | ||
| Length of working’s experience | 0.98 | 0.93 to 1.04 | 0.558 |
| School roles | |||
| Teaching | 1.39 | 0.55 to 3.52 | 0.487 |
| Non-teaching | (ref.) | ||
| Teachers’ perceptions and concern | |||
| Your school was ready for on-site education | |||
| Strongly agree | 2.03 | 0.28 to 14.59 | 0.478 |
| Agree | 2.50 | 0.42 to 14.82 | 0.312 |
| Disagree | 1.17 | 0.18 to 7.35 | 0.870 |
| Strongly disagree | (ref.) | ||
| Your school staff were ready for on-site education | |||
| Strongly agree | 4.53 | 0.42 to 48.78 | 0.212 |
| Agree | 1.56 | 0.18 to 13.61 | 0.688 |
| Disagree | 1.85 | 0.18 to 19.17 | 0.606 |
| Strongly disagree | (ref.) | ||
| Concern regarding school opening for on-site education | |||
| Very concerned and not in agreement with school opening | 3.78 | 1.04 to 13.70 | 0.043 * |
| Very concerned but agree with school opening | 1.79 | 0.60 to 5.33 | 0.298 |
| Moderately concerned and agree with school opening | 2.50 | 0.75 to 8.26 | 0.134 |
| Slightly concerned | (ref.) | ||
| Agreement regarding the measures and recommendations for the COVID-19 prevention and control in school | |||
| ≥2 disagreements | 0.03 | 0.01 to 0.23 | 0.001 ** |
| 1 disagreement | 0.04 | 0.01 to 0.19 | <0.001 ** |
| All agree | (ref.) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Assavanopakun, P.; Promkutkao, T.; Promkutkeo, S.; Sirikul, W. Perspectives and Factors Affecting the Preventive Behavior Pertinent to COVID-19 among School Employees in Chiang Mai, Thailand: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 5662. https://doi.org/10.3390/ijerph19095662
Assavanopakun P, Promkutkao T, Promkutkeo S, Sirikul W. Perspectives and Factors Affecting the Preventive Behavior Pertinent to COVID-19 among School Employees in Chiang Mai, Thailand: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(9):5662. https://doi.org/10.3390/ijerph19095662
Chicago/Turabian StyleAssavanopakun, Pheerasak, Tharntip Promkutkao, Suchat Promkutkeo, and Wachiranun Sirikul. 2022. "Perspectives and Factors Affecting the Preventive Behavior Pertinent to COVID-19 among School Employees in Chiang Mai, Thailand: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 9: 5662. https://doi.org/10.3390/ijerph19095662
APA StyleAssavanopakun, P., Promkutkao, T., Promkutkeo, S., & Sirikul, W. (2022). Perspectives and Factors Affecting the Preventive Behavior Pertinent to COVID-19 among School Employees in Chiang Mai, Thailand: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 19(9), 5662. https://doi.org/10.3390/ijerph19095662