
Towards a Holistic Model Explaining Hearing Protection Device Use among Workers

 ,
,  ,
,
Abstract
1. Introduction
1.1. Understanding HPD Consistency of Use through Behavioral Models
1.2. Limitations of Existing Behavioral Models
1.3. Complexity of Comfort-Related Aspects and How They Are Addressed
1.4. Synthesis of the Literature
1.5. Purpose of the Article: Research Focus
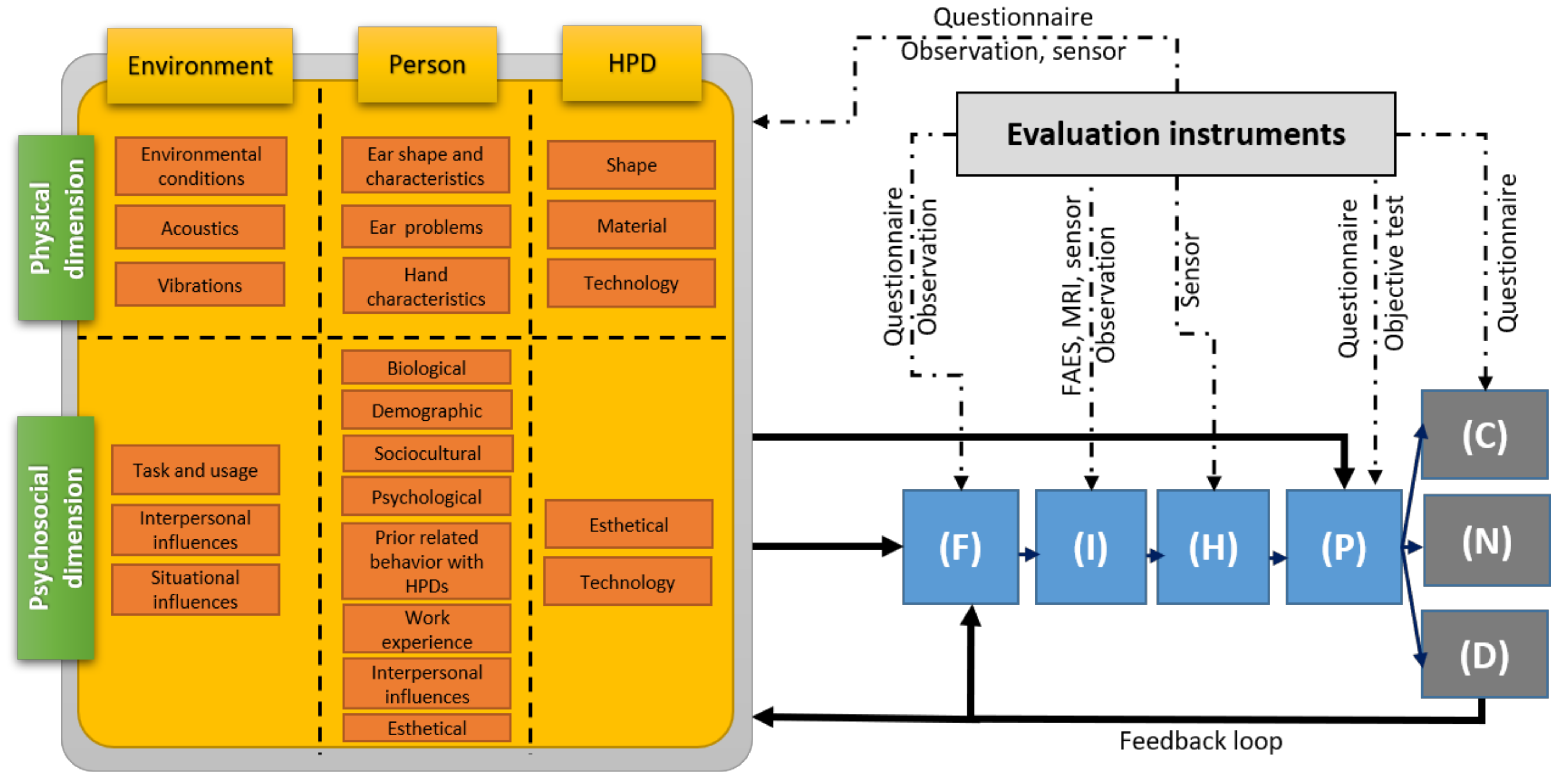
2. HPD Comfort Model
2.1. Comfort Model Phases
2.2. Comfort Model Outcomes
2.3. Comfort Model Inputs
2.4. Links between Comfort Model Components
2.5. Comfort Model Evaluation Instruments
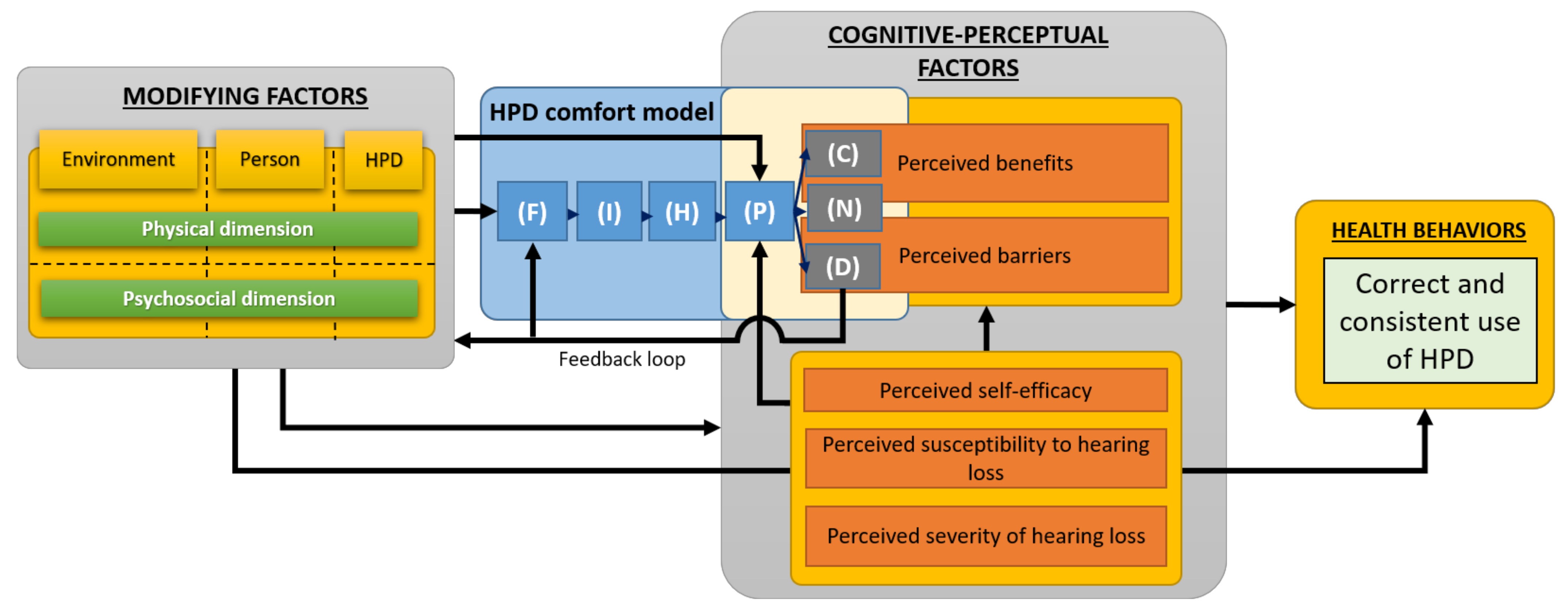
3. Time-Independent Model of HPD Use
3.1. HPD Use Model Components
3.2. HPD Use Model Inputs
3.3. HPD Use Model Outcomes
3.4. Links between HPD Use Model Components
3.5. HPD Use Model Evaluation Instruments
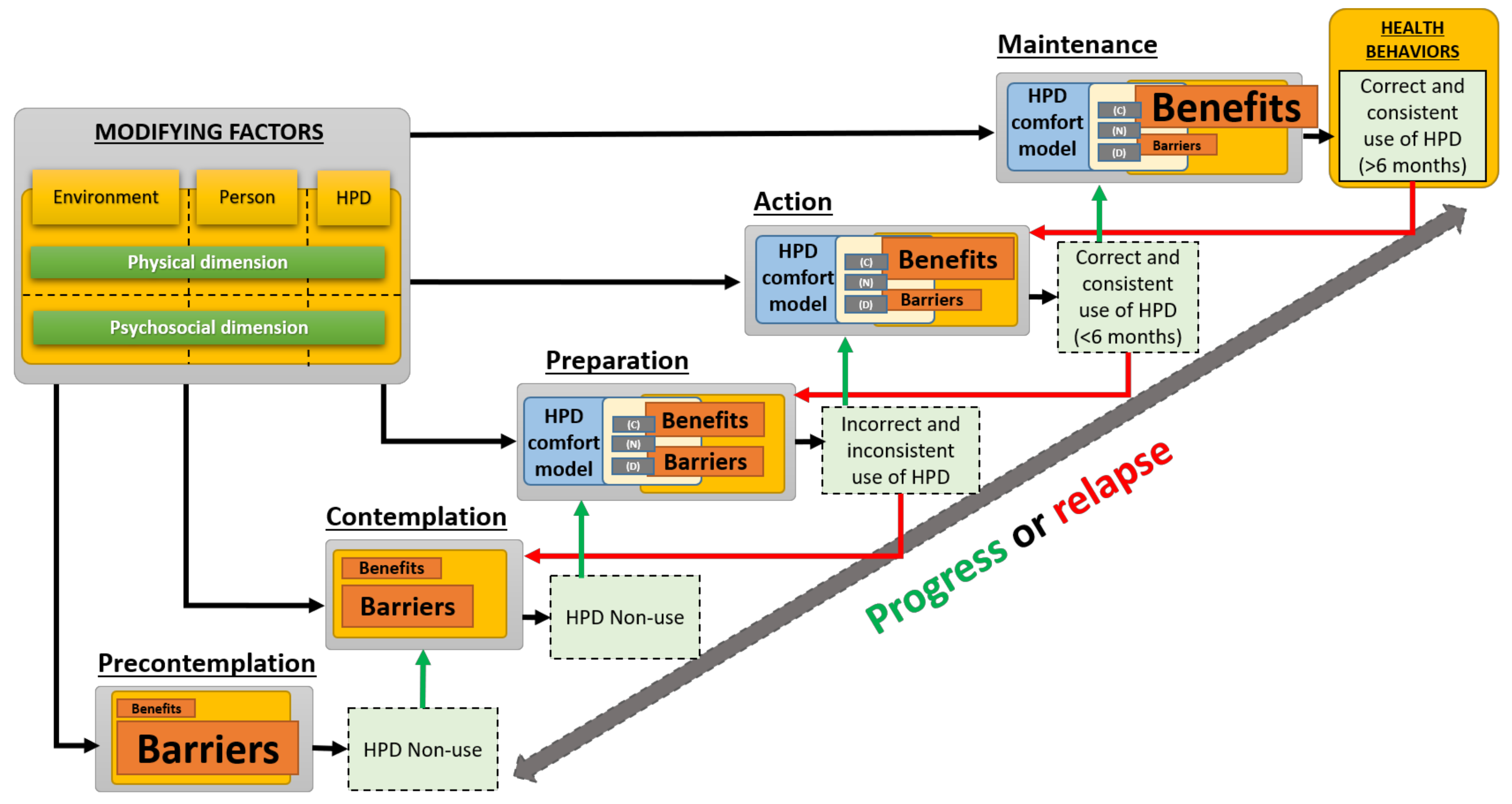
4. Holistic Model of HPD Use
4.1. Holistic Model Stages
4.2. Integration of the Time-Independent Model
4.3. Holistic Model Inputs and Outcomes
5. Conclusions and Discussion
5.1. Summary
5.2. Comparison with Other Research
5.3. Strengths and Limitations
5.4. Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Berger, E.H.; Voix, J. Hearing Protection Devices (Chapter 11). In The Noise Manual, 6th ed.; Meinke, D.K., Berger, E.H., Neitzel, R.L., Driscoll, D.P., Bright, K., Eds.; AIHA Press: Falls Church, VA, USA, 2022. [Google Scholar]
- Tikka, C.; Verbeek, J.H.; Kateman, E.; Morata, T.C.; Dreschler, W.A.; Ferrite, S. Interventions to Prevent Occupational Noise-induced Hearing Loss. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef] [PubMed]
- Brennan-Jones, C.G.; Tao, K.F.M.; Tikka, C.; Morata, T.C. Cochrane Corner: Interventions to Prevent Hearing Loss Caused by Noise at Work. Int. J. Audiol. 2020, 59, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Tikka, C.; Verbeek, J.; Kateman, E.; Morata, T.C.; Dreschler, W.; Ferrite, S. Cochrane Method for Systematic Review and Meta-Analysis of Interventions to Prevent Occupational Noise-Induced Hearing Loss—Abridged. CoDAS 2020, 32, e20190127. [Google Scholar] [CrossRef] [PubMed]
- Groenewold, M.R.; Masterson, E.A.; Themann, C.L.; Davis, R.R. Do Hearing Protectors Protect Hearing? Am. J. Ind. Med. 2014, 57, 1001–1010. [Google Scholar] [CrossRef] [PubMed]
- Kalampakorn, S. Stages of Construction Workers’ Use of Hearing Protection. Ph. D. Thesis, University of Michigan, Ann Arbor, MI, USA, 2000. [Google Scholar]
- Edelson, J.; Neitzel, R.; Meischke, H.; Daniell, W.E.; Sheppard, L.; Stover, B.; Seixas, N. Predictors of Hearing Protection Use in Construction Workers. Ann. Occup. Hyg. 2009, 53, 605–615. [Google Scholar] [CrossRef] [PubMed]
- Lusk, S.L.; Ronis, D.L.; Hogan, M.M. Test of the Health Promotion Model as a Causal Model of Construction Workers’ Use of Hearing Protection. Res. Nurs. Health 1997, 20, 183–194. [Google Scholar] [CrossRef]
- Ronis, D.L.; Hong, O.; Lusk, S.L. Comparison of the Original and Revised Structures of the Health Promotion Model in Predicting Construction Workers’ Use of Hearing Protection. Res. Nurs. Health 2006, 29, 3–17. [Google Scholar] [CrossRef]
- Seixas, N.S.; Neitzel, R.; Stover, B.; Sheppard, L.; Daniell, B.; Edelson, J.; Meischke, H. A Multi-Component Intervention to Promote Hearing Protector Use among Construction Workers. Int. J. Audiol. 2011, 50, S46–S56. [Google Scholar] [CrossRef]
- Stephenson, M.R.; Shaw, P.B.; Stephenson, C.M.; Graydon, P.S. Hearing Loss Prevention for Carpenters: Part 2—Demonstration Projects Using Individualized and Group Training. Noise Health 2011, 13, 122–131. [Google Scholar] [CrossRef]
- Lusk, S.L.; Kerr, M.J.; Ronis, D.L.; Eakin, B.L. Applying the Health Promotion Model to Development of a Worksite Intervention. Am. J. Health Promot. 1999, 13, 219–227. [Google Scholar] [CrossRef]
- Stephenson, M.R. Hearing Protection in the 21st Century: They’re Not Your Father’s Earplugs Anymore. Semin. Hear. 2009, 30, 56–64. [Google Scholar] [CrossRef]
- Hong, O.; Chin, D.L.; Kerr, M.J.; Ronis, D.L. Stages of Change in Hearing-Protection Behavior, Cognition, and Hearing Status. Am. J. Health Behav. 2012, 36, 811–822. [Google Scholar] [CrossRef]
- Hong, O.; Lusk, S.L.; Ronis, D.L. Ethnic Differences in Predictors of Hearing Protection Behavior between Black and White Workers. Res. Theory Nurs. Pract. 2005, 19, 63–76. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Jeong, I.; Hong, O. Predictors of Hearing Protection Behavior among Power Plant Workers. Asian Nurs. Res. 2010, 4, 10–18. [Google Scholar] [CrossRef][Green Version]
- Smith, P.S.; Monaco, B.A.; Lusk, S.L. Attitudes toward Use of Hearing Protection Devices and Effects of an Intervention on Fit-Testing Results. Workplace Health Saf. 2014, 62, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Tantranont, K.; Codchanak, N. Predictors of Hearing Protection Use among Industrial Workers. Workplace Health Saf. 2017, 65, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Lusk, S.L.; Roms, D.L.; Kerr, M.J.; Atwood, J.R. Test of the Health Promotion Model as a Causal Model of Workers’ Use of Hearing Protection. Nurs. Res. 1994, 43, 151–157. [Google Scholar] [CrossRef]
- Rabinowitz, P.M.; Duran, R. Is Acculturation Related to Use of Hearing Protection? Am. Ind. Hyg. Assoc. 2001, 62, 611–614. [Google Scholar] [CrossRef]
- Kerr, M.J.; Lusk, S.L.; Ronis, D.L. Explaining Mexican American Workers’ Hearing Protection Use with the Health Promotion Model. Nurs. Res. 2002, 51, 100–109. [Google Scholar] [CrossRef]
- Svensson, E.B.; Morata, T.C.; Nylén, P.; Krieg, E.F.; Johnson, A.-C. Beliefs and Attitudes among Swedish Workers Regarding the Risk of Hearing Loss. Int. J. Audiol. 2004, 43, 585–593. [Google Scholar] [CrossRef]
- Lusk, S.L.; Ronis, D.L.; Kazanis, A.S.; Eakin, B.L.; Hong, O.; Raymond, D.M. Effectiveness of a Tailored Intervention to Increase Factory Workers’ Use of Hearing Protection. Nurs. Res. 2003, 52, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Raymond, D.M.; Lusk, S.L. Testing Decisional Balance and Self-Efficacy Applied to Workers’ Use of Hearing Protection. Nurs. Res. 2006, 55, 328–335. [Google Scholar] [CrossRef] [PubMed]
- McCullagh, M.C.; Lusk, S.L.; Ronis, D.L. Factors Influencing Use of Hearing Protection among Farmers: A Test of the Pender Health Promotion Model. Nurs. Res. 2002, 51, 33–39. [Google Scholar] [CrossRef] [PubMed]
- McCullagh, M.C.; Ronis, D.L.; Lusk, S.L. Predictors of Use of Hearing Protection among a Representative Sample of Farmers. Res. Nurs. Health 2010, 33, 528–538. [Google Scholar] [CrossRef]
- McCullagh, M.C.; Banerjee, T.; Yang, J.J.; Bernick, J.; Duffy, S.; Redman, R. Gender Differences in Use of Hearing Protection Devices among Farm Operators. Noise Health 2016, 18, 368–375. [Google Scholar]
- Kelly, A.C.; Boyd, S.M.; Henehan, G.T. Perceived Barriers to Hearing Protection Use by Employees in Amplified Music Venues, a Focus Group Study. Health Educ. J. 2015, 74, 458–472. [Google Scholar] [CrossRef]
- Hong, O.; Chin, D.L.; Ronis, D.L. Predictors of Hearing Protection Behavior Among Firefighters in the United States. Int. J. Behav. Med. 2013, 20, 121–130. [Google Scholar] [CrossRef]
- Pender, N.J.; Walker, S.N.; Sechrist, K.R.; Frank-Stromborg, M. Predicting Health-Promoting Lifestyles in the Workplace. Nurs. Res. 1990, 39, 326–332. [Google Scholar] [CrossRef]
- Pender, N.J.; Murdaugh, C.L.; Parsons, M.A. Health Promotion in Nursing Practice, 7th ed.; Pearson: Boston, MA, USA, 2015; ISBN 978-0-13-310876-7. [Google Scholar]
- Trabeau, M.; Neitzel, R.; Meischke, H.; Daniell, W.E.; Seixas, N.S. A Comparison of “Train-the-Trainer” and Expert Training Modalities for Hearing Protection Use in Construction. Am. J. Ind. Med. 2008, 51, 130–137. [Google Scholar] [CrossRef]
- Costa, S.; Arezes, P.M. On the Nature of Hearing Protection Devices Usage Prediction. In Occupational Safety and Hygiene; Taylor & Francis Group: London, UK, 2013; pp. 453–456. ISBN 978-1-138-00047-6. [Google Scholar]
- Corbett, D.; Whitelaw, J. Does Perception Equal Protection? Occupational Noise Exposure & Hearing Protective Device Utilisation for Engineering Trades. In Proceedings of the Australian Institute of Occupational Hygienists 34th Annual Conference, Gold Coast, QLD, Australia, 3–7 December 2016; pp. 43–53. [Google Scholar]
- Stephenson, C.M.; Stephenson, M.R. Hearing Loss Prevention for Carpenters: Part 1—Using Health Communication and Health Promotion Models to Develop Training That Works. Noise Health 2011, 13, 113–121. [Google Scholar] [CrossRef]
- Melamed, S.; Rabinowitz, S.; Feiner, M.; Weisberg, E.; Ribak, J. Usefulness of the Protection Motivation Theory in Explaining Hearing Protection Device Use Among Male Industrial Workers. Health Psychol. 1996, 15, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Gates, D.M.; Jones, M.S. A Pilot Study to Prevent Hearing Loss in Farmers. Public Health Nurs. 2007, 24, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Pursley, A.J.; Saunders, G.H. Knowledge, Attitudes, Behaviors, and Noise Exposure of Baristas. Int. J. Audiol. 2016, 55, 184–188. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Meinke, D.K.; Stephenson, M.R. Noise-Induced Hearing Loss: Models for Prevention (Chapter 12). In An Essential Guide to Hearing and Balance Disorders; Ackley, R.S., Decker, T.N., Limb, C.J., Eds.; Psychology Press: New York, NY, USA, 2018; ISBN 978-1-351-57669-7. [Google Scholar]
- Kushnir, T.; Avin, L.; Neck, A.; Sviatochevski, A.; Polak, S.; Peretz, C. Dysfunctional Thinking Patterns and Immigration Status as Predictors of Hearing Protection Device Usage. Ann. Behav. Med. 2006, 32, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Quick, B.L.; Stephenson, M.T.; Witte, K.; Vaught, C.; Booth-Butterfield, S.; Patel, D. An Examination of Antecedents to Coal Miners’ Hearing Protection Behaviors: A Test of the Theory of Planned Behavior. J. Saf. Res. 2008, 39, 329–338. [Google Scholar] [CrossRef]
- Raymond, D.M.; Lusk, S.L. Staging Workers’ Use of Hearing Protection Devices: Application of the Transtheoretical Model. AAOHN J. 2006, 54, 165–172. [Google Scholar] [CrossRef]
- Reed, D.B.; Kidd, P.S.; Westneat, S.C.; Rayens, M.K. Agricultural Disability Awareness and Risk Education (AgDARE) for High School Students. Inj. Prev. 2001, 7, i59–i63. [Google Scholar] [CrossRef]
- Kidd, P.S.; Reed, D.B.; Weaver, L.; Westneat, S.C.; Rayens, M.K. The Transtheoretical Model of Change in Adolescents: Implications for Injury Prevention. J. Saf. Res. 2003, 34, 281–288. [Google Scholar] [CrossRef]
- Robertson, C.; Kerr, M.; Garcia, C.; Halterman, E. Noise and Hearing Protection: Latino Construction Workers’ Experiences. AAOHN J. 2007, 55, 153–160. [Google Scholar] [CrossRef]
- Reddy, R.; Thorne, P.; Welch, D.; Ameratunga, S. Hearing Protection Use in Manufacturing Workers: A Qualitative Study. Noise Health 2012, 14, 202–209. [Google Scholar] [CrossRef]
- Reddy, R.; Welch, D.; Ameratunga, S.; Thorne, P. Development of the Hearing Protection Assessment (HPA-2) Questionnaire. Occup. Med. 2014, 64, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Reddy, R.; Welch, D.; Ameratunga, S.; Thorne, P. An Ecological Approach to Hearing-Health Promotion in Workplaces. Int. J. Audiol. 2017, 56, 316–327. [Google Scholar] [CrossRef] [PubMed]
- Tantranont, K.; Srisuphan, W.; Kaewthummanukul, T.; Suthakorn, W.; Jormsri, P.; Salazar, M.K. Factors Affecting Thai Workers’ Use of Hearing Protection. AAOHN J. 2009, 57, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Rabinowitz, S.; Melamed, S.; Feiner, M.; Weisberg, E.; Ribak, J. Hostility and Hearing Protection Behavior: The Mediating Role of Personal Beliefs and Low Frustration Tolerance. J. Occup. Health Psychol. 1996, 1, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.W.; Rosenman, K.D.; Kotowski, M.R.; Glazer, E.; McFeters, C.; Keesecker, N.M.; Law, A. Using the EPPM to Create and Evaluate the Effectiveness of Brochures to Increase the Use of Hearing Protection in Farmers and Landscape Workers. J. Appl. Commun. Res. 2008, 36, 200–218. [Google Scholar] [CrossRef]
- Patel, D.S.; Witte, K.; Zuckerman, C.; Murray-Johnson, L.; Orrego, V.; Maxfield, A.M.; Meadows-Hogan, S.; Tisdale, J.; Thimons, E.D. Understanding Barriers to Preventive Health Actions for Occupational Noise-Induced Hearing Loss. J. Health Commun. 2001, 6, 155–168. [Google Scholar] [CrossRef] [PubMed]
- Murray-Johnson, L.; Witte, K.; Patel, D.; Orrego, V.; Zuckerman, C.; Maxfield, A.M.; Thimons, E.D. Using the Extended Parallel Process Model to Prevent Noise-Induced Hearing Loss Among Coal Miners in Appalachia. Health Educ. Behav. 2004, 31, 741–755. [Google Scholar] [CrossRef] [PubMed]
- Arezes, P.M.; Miguel, A.S. Individual Perception of Noise Exposure and Hearing Protection in Industry. Hum. Factors 2005, 47, 683–692. [Google Scholar] [CrossRef]
- Bockstael, A.; De Bruyne, L.; Vinck, B.B. Attitudes and Beliefs Concerning Hearing Protectors and Noise Exposure. Can. Acoust. 2011, 39, 92–93. [Google Scholar]
- Morata, T.C.; Fiorini, A.C.; Fischer, F.M.; Krieg, E.F.; Gozzoli, L.; Colacioppo, S. Factors Affecting the Use of Hearing Protectors in a Population of Printing Workers. Noise Health 2001, 4, 21–28. [Google Scholar]
- Wadud, S.E.; Kreuter, M.W.; Clarkson, S. Risk Perception, Beliefs about Prevention, and Preventive Behaviors of Farmers. J. Agric. Saf. Health 1998, 4, 15–24. [Google Scholar] [CrossRef]
- Hass-Slavin, L.; McColl, M.A.; Pickett, W. Challenges and Strategies Related to Hearing Loss Among Dairy Farmers. J. Rural Health 2005, 21, 329–336. [Google Scholar] [CrossRef] [PubMed]
- McCullagh, M.C.; Robertson, C. Too Late Smart: Farmers’ Adoption of Self-Protective Behaviors in Response to Exposure to Hazardous Noise. AAOHN J. 2009, 57, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Melamed, S.; Rabinowitz, S.; Green, M.S. Noise Exposure, Noise Annoyance, Use of Hearing Protection Devices and Distress among Blue-Collar Workers. Scand. J. Work. Environ. Health 1994, 20, 294–300. [Google Scholar] [CrossRef]
- Doutres, O.; Sgard, F.; Terroir, J.; Perrin, N.; Jolly, C.; Gauvin, C.; Negrini, A. A Critical Review of the Literature on Comfort of Hearing Protection Devices: Definition of Comfort and Identification of Its Main Attributes for Earplug Types. Int. J. Audiol. 2019, 58, 824–833. [Google Scholar] [CrossRef]
- Prochaska, J.O.; Redding, C.A.; Evers, K.E. The Transtheoretical Model and Stages of Change (Chapter 5). In Health Behavior and Health Eudcation: Theory, Research, and Practice; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; Jossey-Bass: San Francisco, CA, USA, 2008. [Google Scholar]
- CSA Z94.2-14; Hearing Protection Devices: Performance, Selection, Care and Use. CSA Group: Toronto, ON, Canada, 2014.
- CSA Z1007-16; Hearing Loss Prevention Program (HLPP) Management. CSA Group: Toronto, ON, Canada, 2016.
- Doutres, O.; Sgard, F.; Terroir, J.; Perrin, N.; Jolly, C.; Gauvin, C.; Negrini, A. A Critical Review of the Literature on Comfort of Hearing Protection Devices: Analysis of the Comfort Measurement Variability. Int. J. Occup. Saf. Ergon. 2020, 1–36. [Google Scholar] [CrossRef]
- Berger, E.H. EARLOG Monographs on Hearing and Hearing Protection: Hearing Protector Performance: How They Work-and-What Goes Wrong in the Real World, EARLOG 5; Cabot Safety Corporation: Indianapolis, IN, USA, 1980; p. 4. [Google Scholar]
- Ivarsson, A.; Toremalm, N.G.; Brühl, P. Eczema, Itching, Heat and Humidity Problems-Impediments to the Effective Use of Hearing Protectors. In Proceedings of the Internoise 1990, Göteborg, Sweden, 13 August 1990; Volume 90, pp. 1093–1096. [Google Scholar]
- Davis, R.R.; Shaw, P.B. Heat and Humidity Buildup under Earmuff-Type Hearing Protectors. Noise Health 2011, 13, 93. [Google Scholar] [CrossRef]
- Laroche, C.; Giguère, C.; Vaillancourt, V.; Marleau, C.; Cadieux, M.-F.; Laprise-Girard, K.; Gula, E.; Carroll, V.; Bibeau, M.; Nélisse, H. Effect of Hearing and Head Protection on the Localization of Tonal and Broadband Reverse Alarms. Hum. Factors J. Hum. Factors Ergon. Soc. 2021, 001872082199222. [Google Scholar] [CrossRef]
- John, G.W.; Grynevych, A.; Welch, D.; McBride, D.; Thorne, P.R. Noise Exposure of Workers and the Use of Hearing Protection Equipment in New Zealand. Arch. Environ. Occup. Health 2014, 69, 69–80. [Google Scholar] [CrossRef]
- Hétu, R. The Hearing Conservation Paradigm and the Experienced Effects of Occupational Noise Exposure. Can. Acoust. 1994, 22, 3–19. [Google Scholar]
- de Looze, M.P.; Kuijt-Evers, L.F.M.; van DieëN, J. Sitting Comfort and Discomfort and the Relationships with Objective Measures. Ergonomics 2003, 46, 985–997. [Google Scholar] [CrossRef]
- Gardner, R. Polymeric Foam Earplug. U.S Patent 5,203,352, 20 April 1993. [Google Scholar]
- U.S. Environmental Protection Agency (EPA). Noise Labeling Requirements for Hearing Protectors; U.S. Environmental Protection Agency (EPA): Washington, DC, USA, 1979; pp. 56130–56147. [Google Scholar]
- Vink, P.; Hallbeck, S. Editorial: Comfort and Discomfort Studies Demonstrate the Need for a New Model. Appl. Ergon. 2012, 43, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Moes, N.C.C.M. Analysis of Sitting Discomfort, A Review. In Contemporary Ergonomics; Taylor & Francis: Oxfordshire, UK, 2005; pp. 200–204. [Google Scholar]
- Naddeo, A.; Cappetti, N.; Vallone, M.; Califano, R. New Trend Line of Research about Comfort Evaluation: Proposal of a Framework for Weighing and Evaluating Contributes Coming from Cognitive, Postural and Physiologic Comfort Perceptions. In Proceedings of the 5th International Conference on Applied Human Factors and Ergonomics, Kraków, Poland, 19 July 2014; Ahram, T.W., Karwowski, W., Marek, T., Eds.; p. 12. [Google Scholar]
- Branson, D.H.; Sweeney, M.M. Conceptualization and Measurement of Clothing Comfort: Toward a Metatheory. In Critical Linkages in Textiles and Clothing: Theory, Method and Practice; S. Kaiser and M.L. Damhorst: Monument, CO, USA, 1991; pp. 94–105. [Google Scholar]
- Kolcaba, K.Y.; Kolcaba, R.J. An Analysis of the Concept of Comfort. J. Adv. Nurs. 1991, 16, 1301–1310. [Google Scholar] [CrossRef] [PubMed]
- Kolcaba, K. Comfort. In Middle Range Theories: Application to Nursing Research and Practice; Wolters Kluwer: Philadelphia, PA, USA, 2016; pp. 196–211. ISBN 978-0-06-000044-8. [Google Scholar]
- Chappells, H. Comfort, Well-Being and the Socio-Technical Dynamics of Everyday Life. Intell. Build. Int. 2010, 2, 286–298. [Google Scholar]
- Vischer, J.C. Towards an Environmental Psychology of Workspace: How People Are Affected by Environments for Work. Archit. Sci. Rev. 2008, 51, 97–108. [Google Scholar] [CrossRef]
- Zemp, R.; Taylor, W.R.; Lorenzetti, S. Are Pressure Measurements Effective in the Assessment of Office Chair Comfort/Discomfort? A Review. Appl. Ergon. 2015, 48, 273–282. [Google Scholar] [CrossRef]
- Zhang, L.; Helander, M.G.; Drury, C.G. Identifying Factors of Comfort and Discomfort in Sitting. Hum. Factors 1996, 38, 377–389. [Google Scholar] [CrossRef]
- Behar, A. Best Hearing Protectors Ever? Int. J. Environ. Res. Public. Health 2022, 19, 2165. [Google Scholar] [CrossRef]
- Themann, C.L.; Masterson, E.A. Occupational Noise Exposure: A Review of Its Effects, Epidemiology, and Impact with Recommendations for Reducing Its Burden. J. Acoust. Soc. Am. 2019, 146, 3879–3905. [Google Scholar] [CrossRef]
- Mansfield, N.; Naddeo, A.; Frohriep, S.; Vink, P. Integrating and Applying Models of Comfort. Appl. Ergon. 2020, 82, 102917. [Google Scholar] [CrossRef]
- Naddeo, A. Towards Predicting the (Dis)Comfort Performance by Modelling: Methods and Findings. Ph.D. Thesis, Delft University of Technology, Delft, The Netherlands, 2017. [Google Scholar]
- Pontrelli, G.J. Partial Analysis of Comfort’s Gestalt. In Clothing Comfort: Interaction of Thermal, Ventilation, Construction, and Assessment Factors; Hollies, N.R.S., Goldman, R.F., Eds.; Ann Arbor Science: Ann Arbor, MI, USA, 1977; pp. 71–80. [Google Scholar]
- American National Standards Institute (ANSI); Acoustical Society of America (ASA). Performance Criteria for Systems That Estimate the Attenuation of Passive Hearing Protectors for Individual Users; American National Standard: New York, NY, USA, 2018. [Google Scholar]
- Benacchio, S.; Doutres, O.; Varoquaux, A.; Wagnac, E.; Le Troter, A.; Callot, V.; Sgard, F. Use of Magnetic Resonance Image Registration to Estimate Displacement in the Human Earcanal Due to the Insertion of In-Ear Devices. J. Acoust. Soc. Am. 2019, 146, 2452–2465. [Google Scholar] [CrossRef] [PubMed]
- Arezes, P.M.; Abelenda, C.; Braga, A.C. An Evaluation of Comfort Afforded by Hearing Protection Devices. In Proceedings of the AHFE 2008, Las Vegas, NV, USA, 14 July 2008; pp. 1–8. [Google Scholar]
- Tinoco, H.C.; Lima, G.B.A.; Sant’Anna, A.P.; Gomes, C.F.S.; dos Santos, J.A.N. Risk Perception in the Use of Personal Protective Equipment against Noise-Induced Hearing Loss. Gest. Amp Produção 2019, 26, e1611. [Google Scholar] [CrossRef]
- Lusk, S.L.; Ronis, D.L.; Baer, L.M. A Comparison of Multiple Indicators: Observations, Supervisor Report, and Self-Report as Measures of Workers’ Hearing Protection Use. Eval. Health Prof. 1995, 18, 51–63. [Google Scholar] [CrossRef] [PubMed]
- Griffin, S.C.; Neitzel, R.; Daniell, W.E.; Seixas, N.S. Indicators of Hearing Protection Use: Self-Report and Researcher Observation. J. Occup. Environ. Hyg. 2009, 6, 639–647. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Arezes, P.M.; Miguel, A.S. Assessing the Use of Hearing Protection in Industrial Settings: A Comparison between Methods. Int. J. Ind. Ergon. 2013, 43, 518–525. [Google Scholar] [CrossRef]
- Garcia, S. Hearing Protection Use and Intertemporal Choice in Industrial Workers. Ph. D. Thesis, University of Pittsburgh ETD, Pittsburgh, PA, USA, 2019. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Attribute | Comfort Dimension 1 | |
|---|---|---|
| Barriers | Aspects related to the mechanical contact between the HPD and the body (e.g., unpleasant mechanical pressure and irritation) | Physical |
| Communication difficulties (hearing and speech) | Acoustical | |
| Difficulty hearing useful machine sounds and danger signals | Acoustical | |
| Difficulty in inserting the HPD | Functional | |
| Benefits | Protect hearing/prevent hearing loss | Functional |
| Prevent tinnitus (ringing in the ears) | Physical/ Functional | |
| Reduce headaches and fatigue | Physical | |
| Avoid noise annoyance | Functional/Acoustical/psychological | |
| Enhance communication | Acoustical | |
| Enhance ability to hear useful machinery noise | Acoustical |
| HPD/Person | Every disposable earplug cannot fit correctly in every earcanal, and every earmuff is not suited for all head shapes [1,66] |
| Earplug use is not recommended in the presence of an earcanal medical condition (e.g., infections, eczema) [1,67] | |
| Earmuff protection efficiency can be affected by the presence of hair, eyeglass temples or caps [1] | |
| Earplugs are preferred by individuals favoring discrete hearing protectors and/or concerned with their hairstyle [1] | |
| HPD/Work environment | Earmuffs can be difficult to wear in hot environments [1,67,68] |
| Over-attenuating HPDs can block important environmental sounds such as alarm signals, machine sound and colleagues’ speech [1] | |
| Earmuffs reduce the localization of the noise sources more than earplugs [69] | |
| Earplug insertion and removal can be time consuming and incompatible with work tasks when many removals are required during the work shift (and thus, earmuff are preferred in this case [1,70]) | |
| Earmuffs can interfere with movements when work is carried out in a tight space [1] | |
| Compared to earmuffs, earplug efficiency is more dependent on user training, skill and motivation [1] | |
| HPD requiring a periodic re-positioning is not adapted to work tasks based on a fast pace of repetitive movements [71] |
| Phases | Outcomes | ||||
|---|---|---|---|---|---|
| Fitting/Positioning (F) | Interactions (I) | Internal Human Body Effects (H) | Perceived Effects (P) | Comforts (C) | Discomforts (D) |
| Physical/Functional dimension Earplugs: Pull the pinna prior to insertion. Compress the foam earplugs prior to insertion. Choose the insertion depth. Ensure that hair is not inserted inside the earcanal together with the earplug Add lubricant over custom molded earplug. Earmuffs: Remove all hair underneath ear cushions. Seal the cushions firmly against the head. Ensure that the earcups are not fitted crooked or askew over the ears. | Physical dimension During the insertion or removal of the HPD: Large normal and shear stress applied to the ear (pinna, concha and earcanal…), tissue deformation. Once the HPD is worn: added static mechanical pressure distributed in the contact area between person and HPD, tissue deformation. Acoustical dimension Modification of the acoustic pressure at the eardrum created either by an external acoustic source or internal mechanical source (e.g., voice...). | Physical dimension Compression of nerves and blood vessels. Acoustical dimension Conversion of the acoustical and vibratory energy transmitted to the cochlea through airborne and structure-borne pathways to electrical impulses in the auditory nerves. | Physical dimension Perception of a foreign object in contact with the ear. Acoustical dimension Modification of the perceived noise/sound created either by an external acoustic source or internal mechanical source (e.g., voice). | Functional dimension Protect hearing/prevent hearing loss, avoid noise annoyance, stay in position. Acoustical dimension Reduction of the useless external noise, ease of communication, ability to hear useful machinery noise and danger signals. Psychological dimension Trust, habituation, satisfaction. | Physical dimension Pain, irritation. Functional dimension Difficulty in fitting/positioning, annoyance, unhandy, unstable, intrusion (inhibit head and body movements). Acoustical dimension Difficulty in communication, difficulty in hearing useful machinery noise and danger signals, difficulty in localizing sounds, occlusion effect. Psychological dimension Esthetical concerns, isolation from the external environment. |
| Work Environment | Person | HPD |
|---|---|---|
| Environmental conditions: air temperature, relative humidity, atmospheric pressure, air quality (dust). Acoustics: noise environment (e.g., spectrum, noise level, noise type, direction), presence of useful acoustic signals (e.g., alarms, machine, discussions with colleagues) and their characteristics (e.g., spectrum, noise level, noise type). Vibrations: presence of vibrations from hand tool, ground. | Ear characteristics: size and shape of the pinna and external auditory canal, flexibility of the pinna and external auditory canal, auditory canal hairiness, propensity to the build up of earwax. Ear problems: ear infections, otitis, eczema, hearing loss, tinnitus. Hand characteristics: hand dominance, hand dexterity. Susceptibility to the effects of noise exposure. Other attributes that may interact with the use of HPD (related or not to esthetical aspects): short or long hair, wear eyeglasses, cap, hat. | Earplugs: Design: shape (e.g., cylinder, bullet shape, conical, custom molded…) size, corded/uncorded, with stem/without stem, need for lubricant. Material properties: softness, weight, texture, heat transfer properties, moisture/vapor transfer properties, made of inert non-toxic substance, expansion time after compression, resistance to humidity. Embedded technology: presence of acoustic filters, active vs. passive. Earmuffs: Design: headband, cushion, cup. Material properties: cushion and headband stiffness, cup weight, texture, heat transfer properties, moisture/vapor transfer properties, made of inert non-toxic substance. Embedded technology: active vs. passive. |
| Work Environment | Person | HPD |
|---|---|---|
| Task and usage: type of work (manual, non-manual, mixed), physical activity (body, head or jaw movements), type of equipment/tools used, necessity to wear other personal protective equipment, necessity to insert/remove regularly HPD during work (task-related or noise exposure-related), necessity to hear useful signals (e.g., machines/engines, alarms), necessity to communicate with colleagues (teamwork), time aspects (e.g., work duration, full time or part time paid employees, noise exposure duration). Interpersonal influences (peers, co-workers, hierarchy): social models, social norms, interpersonal support. Situational influences: workplace rules (mandatory hearing protection policy), perceptions of accessibility and availability of HPD, perception of exposition of high noise levels, organizational support for health, HPD training (existence and duration (in hours)), hearing examination/re-examination, job position in organization chart, gratification, salary, hearing protection requirement status, plant site. | Biological: gender. Demographic: age, ethnicity. Sociocultural: acculturation, education, immigration status, socioeconomic status. Psychological: personality, self-esteem, self-motivation, perceived health status, perceived hearing status, self-experienced hearing symptoms (tinnitus and noise sensitivity), low frustration tolerance (LFT). Prior related behavior (previous experience with HPDs): experience with HPD use, preferred HPD, ideal HPD, expectations regarding HPD comfort/discomfort, care of HPD (e.g., clean, regular inspection, change damaged, compromised or aged parts). Work experience: years trade experience, years at the plant, years of work in a noisy environment, total years worked, whether prior workplace was noisy, unionized or not. Interpersonal influences (family, friends): social models, social norms, interpersonal support. Esthetical: concerned with hairstyle. | Esthetical: discreetness, color, aesthetic design (e.g., earplug having a screw shape), attractiveness of the product (e.g., custom molded, active products). Other: availability and quality of the instructions for proper fit. |
| Stage of Change | Brief Definition from [62] | Application to HPD-Related Health Behaviors from [14] |
|---|---|---|
| Precontemplation | No intention to take action within the next 6 months | Workers are not using HPDs and have no intention to do so |
| Contemplation | Intends to take action within the next 6 months | Workers are not using HPDs but have intention to do so |
| Preparation | Intends to take action within the next 30 days and has taken some behavioral steps in this direction | Workers use HPDs but inconsistently |
| Action | Changed overt behavior for less than 6 months | Workers use HPDs consistently during a continuous period from 0 to 6 months |
| Maintenance | Changed overt behavior for more than 6 months | Workers use HPDs consistently for more than 6 months |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doutres, O.; Terroir, J.; Jolly, C.; Gauvin, C.; Martin, L.; Negrini, A. Towards a Holistic Model Explaining Hearing Protection Device Use among Workers. Int. J. Environ. Res. Public Health 2022, 19, 5578. https://doi.org/10.3390/ijerph19095578
Doutres O, Terroir J, Jolly C, Gauvin C, Martin L, Negrini A. Towards a Holistic Model Explaining Hearing Protection Device Use among Workers. International Journal of Environmental Research and Public Health. 2022; 19(9):5578. https://doi.org/10.3390/ijerph19095578
Chicago/Turabian StyleDoutres, Olivier, Jonathan Terroir, Caroline Jolly, Chantal Gauvin, Laurence Martin, and Alessia Negrini. 2022. "Towards a Holistic Model Explaining Hearing Protection Device Use among Workers" International Journal of Environmental Research and Public Health 19, no. 9: 5578. https://doi.org/10.3390/ijerph19095578
APA StyleDoutres, O., Terroir, J., Jolly, C., Gauvin, C., Martin, L., & Negrini, A. (2022). Towards a Holistic Model Explaining Hearing Protection Device Use among Workers. International Journal of Environmental Research and Public Health, 19(9), 5578. https://doi.org/10.3390/ijerph19095578