
Exploring Hepatocellular Carcinoma Mortality Using Weighted Regression Estimation for the Cohort Effect in Taiwan from 1976 to 2015



Abstract
:1. Introduction
2. Methods
2.1. Data Sources
2.2. Multiphase Method with Weighted Regression Model in Obtaining the Measure of Cohort Effects
3. Results
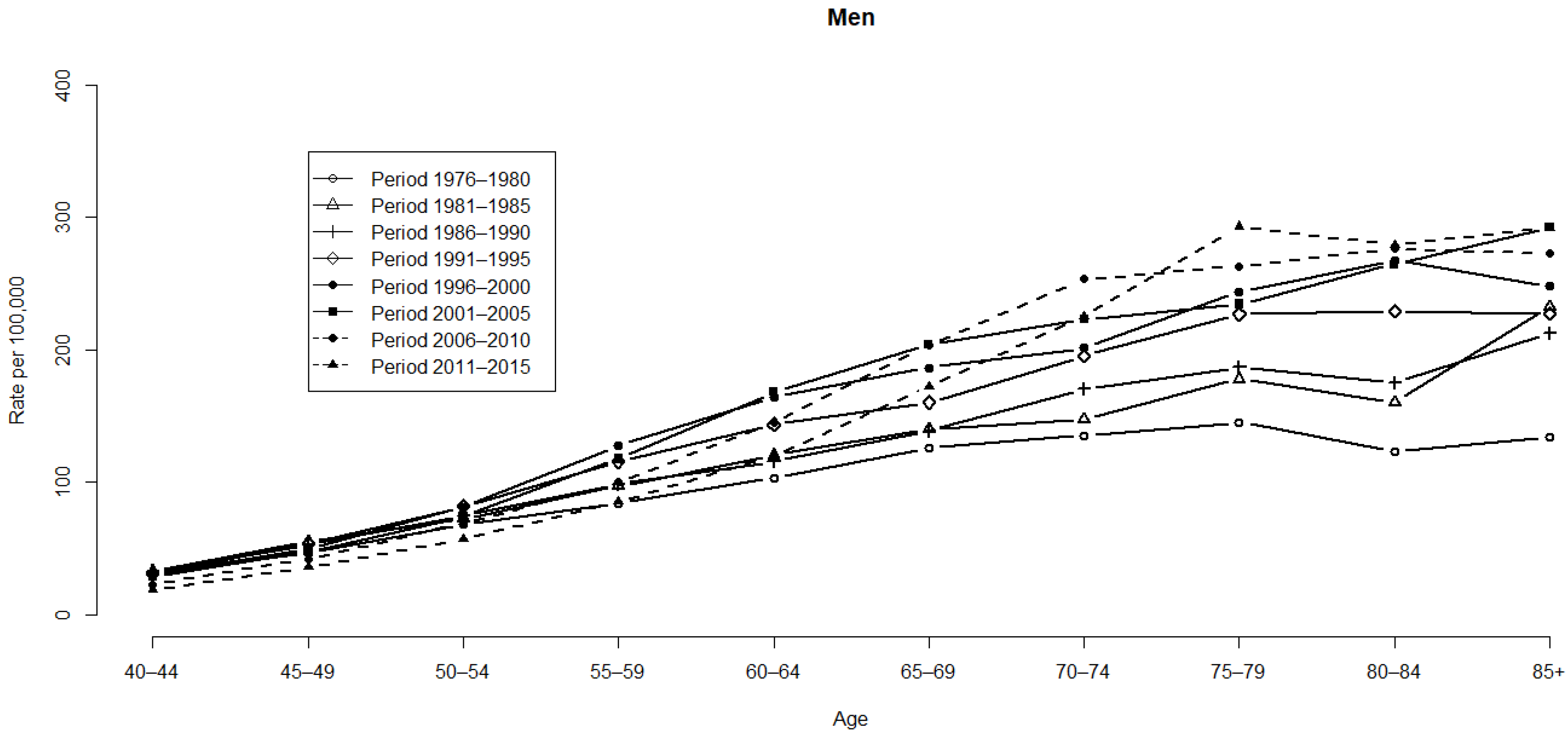
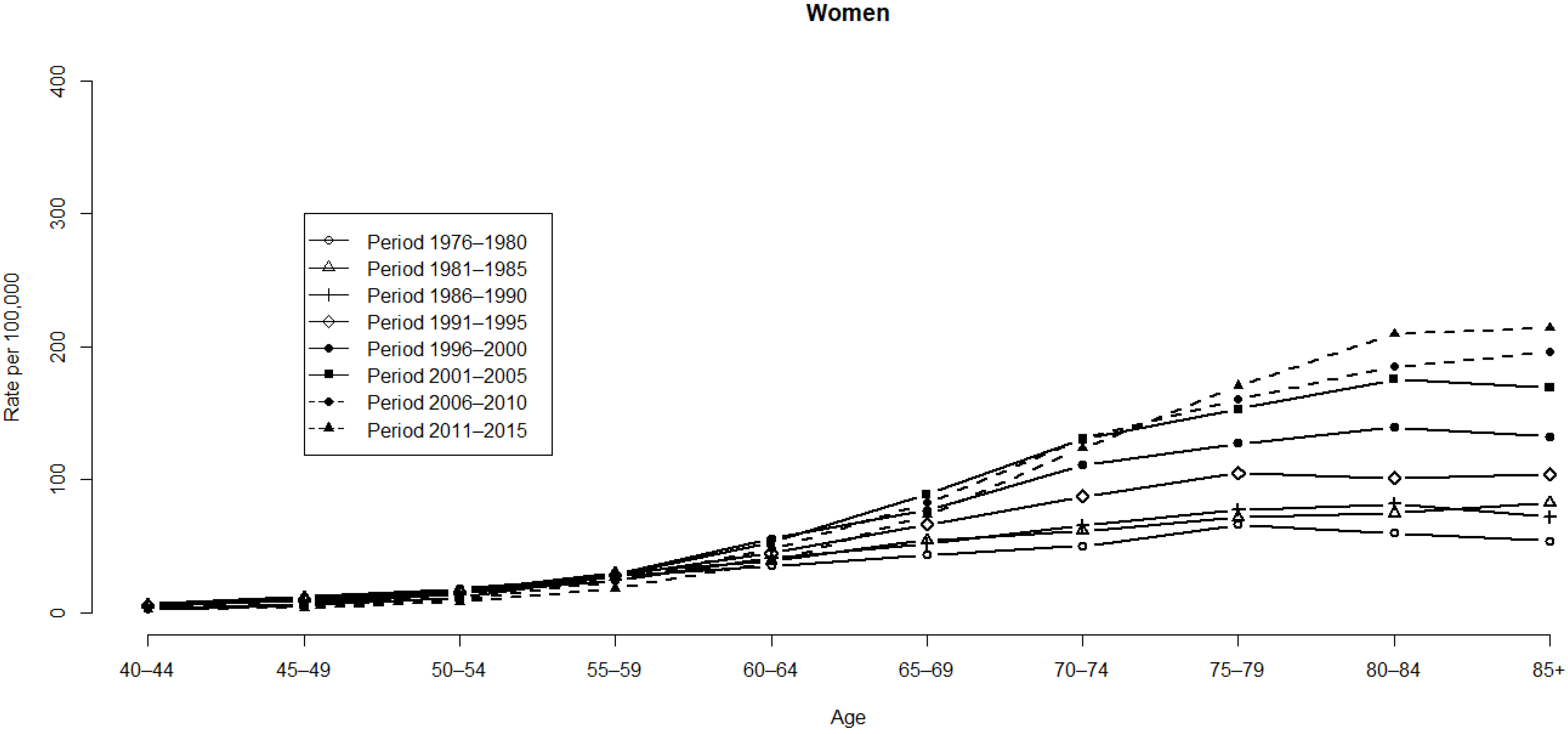
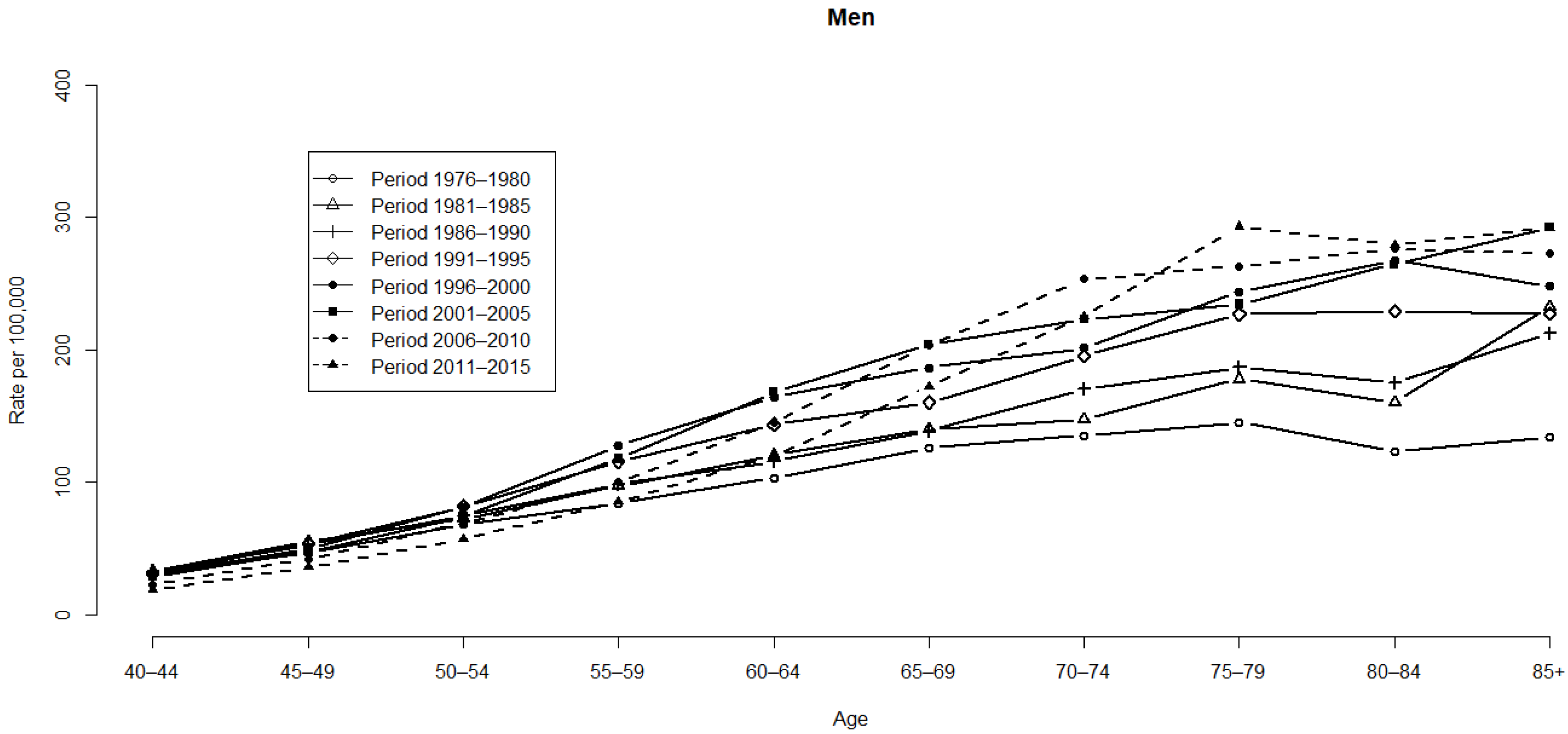
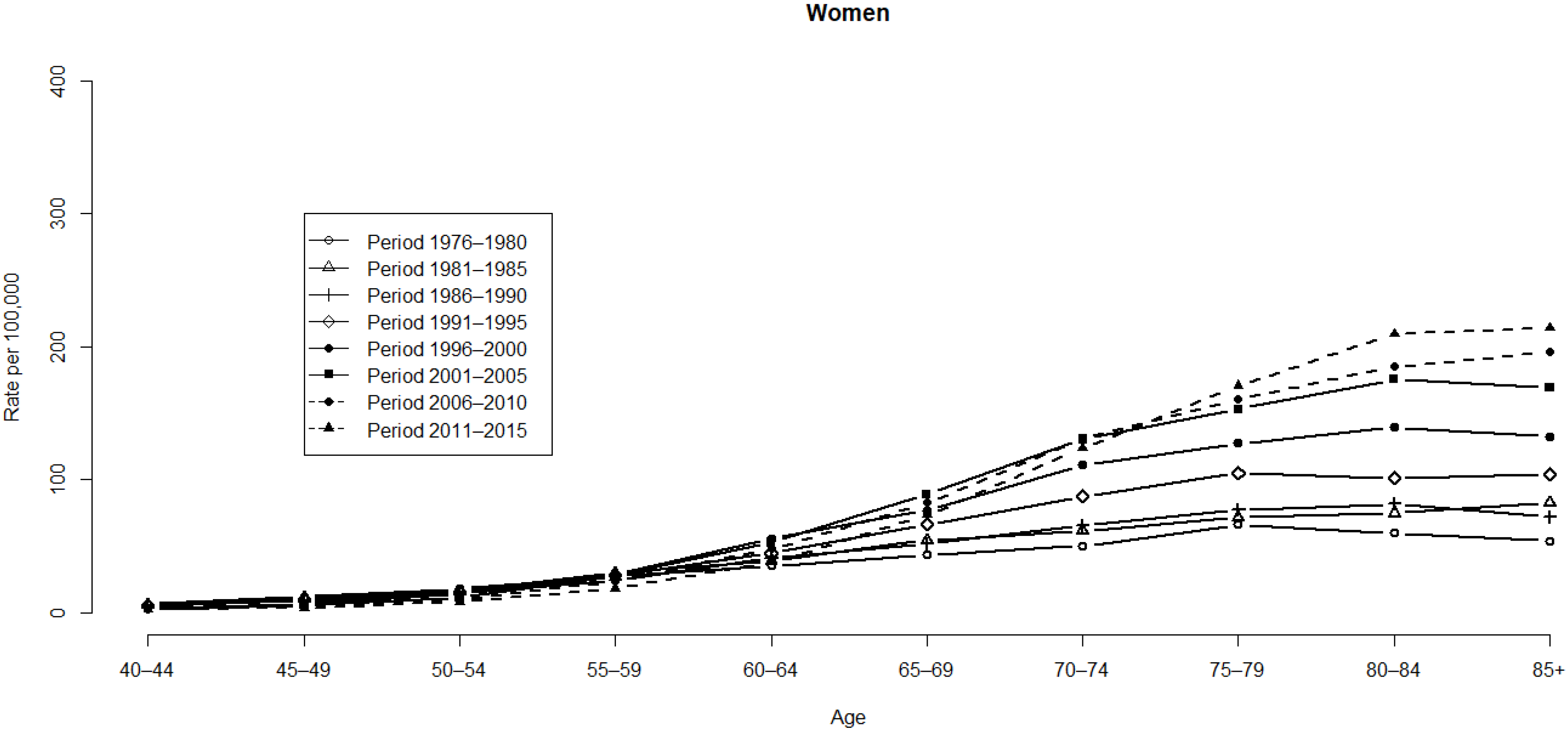
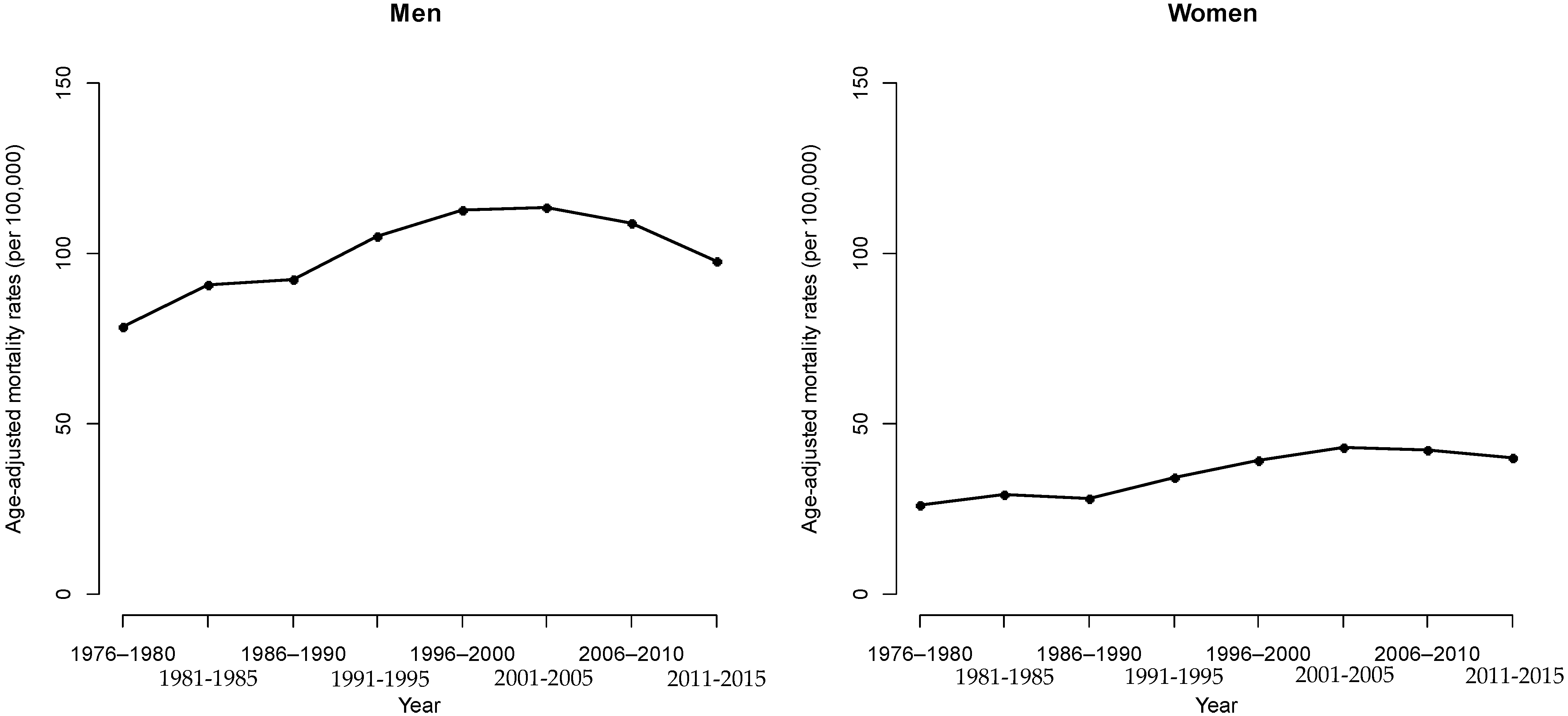
3.1. HCC Mortality Rates
3.2. APC Model
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Balogh, J.; Victor, D., 3rd; Asham, E.H.; Burroughs, S.G.; Boktour, M.; Saharia, A.; Li, X.; Ghobrial, R.M.; Monsour, H.P., Jr. Hepatocellular carcinoma: A review. J. Hepatocell. Carcinoma 2016, 3, 41–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global Cancer Observatory. Available online: https://gco.iarc.fr/ (accessed on 14 March 2022).
- McGlynn, K.A.; Tsao, L.; Hsing, A.W.; Devesa, S.S.; Fraumeni, J.F., Jr. International trends and patterns of primary liver cancer. Int. J. Cancer 2001, 94, 290–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosch, F.X.; Ribes, J.; Diaz, M.; Cleries, R. Primary liver cancer: Worldwide incidence and trends. Gastroenterology 2004, 127, 5S–16S. [Google Scholar] [CrossRef] [PubMed]
- Keyes, K.M.; Li, G. A multiphase method for estimating cohort effects in age-period contingency table data. Ann. Epidemiol. 2010, 20, 779–785. [Google Scholar] [CrossRef] [Green Version]
- Tukey, J. Exploratory Data Anlaysis Reading; Addison-Wesley Publishing Company: Boston, MA, USA, 1977. [Google Scholar]
- Selvin, S. Statistical Analysis of Epidemiologic Data; Oxford University Press: New York, NY, USA, 1996. [Google Scholar]
- Légaré, G.; Hamel, D. An age-period-cohort approach to analyzing trends in suicide in Quebec between 1950 and 2009. Can. J. Public Health 2013, 104, e118–e123. [Google Scholar] [CrossRef]
- Wang, J.; Bai, Z.; Wang, Z.; Yu, C. Comparison of Secular Trends in Cervical Cancer Mortality in China and the United States: An Age-Period-Cohort Analysis. Int. J. Environ. Res. Public Health 2016, 13, 1148. [Google Scholar] [CrossRef] [Green Version]
- Pinter, M.; Trauner, M.; Peck-Radosavljevic, M.; Sieghart, W. Cancer and liver cirrhosis: Implications on prognosis and management. ESMO Open 2016, 1, e000042. [Google Scholar] [CrossRef] [Green Version]
- El-Serag, H.B.; Mason, A.C. Risk factors for the rising rates of primary liver cancer in the United States. Arch. Intern. Med. 2000, 160, 3227–3230. [Google Scholar] [CrossRef]
- Einhorn, H.J.; Hogarth, R.M. Unit weighting schemes for decision making. Organ. Behav. Hum. Perform. 1975, 13, 171–192. [Google Scholar] [CrossRef]
- Wang, W.; Tian, S.L.; Wang, H.; Shao, C.C.; Wang, Y.Z.; Li, Y.L. Association of Hepatitis B Virus DNA Level and Follow-up Interval With Hepatocellular Carcinoma Recurrence. JAMA Netw. Open 2020, 3, e203707. [Google Scholar] [CrossRef]
- Roddy, H.; Meyer, T.; Roddie, C. Novel Cellular Therapies for Hepatocellular Carcinoma. Cancers 2022, 14, 504. [Google Scholar] [CrossRef] [PubMed]
- Sonbol, M.B.; Riaz, I.B.; Naqvi, S.A.A.; Almquist, D.R.; Mina, S.; Almasri, J.; Shah, S.; Almader-Douglas, D.; Uson, P.L.S., Jr.; Mahipal, A.; et al. Systemic Therapy and Sequencing Options in Advanced Hepatocellular Carcinoma: A Systematic Review and Network Meta-analysis. JAMA Oncol. 2020, 22, e204930. [Google Scholar] [CrossRef] [PubMed]
- Tzeng, I.S.; Lee, W.C. Forecasting hepatocellular carcinoma mortality in Taiwan using an age-period-cohort model. Asia-Pac. J. Public Health 2015, 27, NP65–NP73. [Google Scholar] [CrossRef] [PubMed]
- Tzeng, I.S.; Kuo, C.Y.; Wang, C.C. Forecasting Hepatocellular Carcinoma Mortality using a Weighted Regression Model to Estimate Cohort Effects in Taiwan. J. Vis. Exp. 2021, 174, e62253. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, O.B.; Boschi-Pinto, C.; Lopez, A.D.; Murray, C.J.L.; Lozano, R.; Inoue, M. Age Standardization of Rates: A New WHO Standard; GPE Discussion Paper Series: No. 31; World Health Organization: Geneva, Switzerland, 2001; pp. 1–14. [Google Scholar]
- Tzeng, I.S.; Ng, C.Y.; Chen, J.Y.; Chen, L.S.; Wu, C.C. Using weighted regression model for estimating cohort effect in age-period contingency table data. Oncotarget 2018, 9, 19826–19835. [Google Scholar] [CrossRef]
- Wilmoth, J.R. Computational Methods for Fitting and Extrapolating the Lee-Carter Model of Mortality Change; Technical Report; University of California: Berkeley, CA, USA, 1993. [Google Scholar]
- Lavanchy, D. Hepatitis B virus epidemiology, disease burden, treatment, and current and emerging prevention and control measures. J. Viral Hepat. 2004, 11, 97–107. [Google Scholar] [CrossRef]
- Chang, M.H.; Chen, C.J.; Lai, M.S.; Hsu, H.M.; Wu, T.C.; Kong, M.S.; Liang, D.C.; Shau, W.Y.; Chen, D.S. Universal hepatitis B vaccination in Taiwan and the incidence of hepatocellular carcinoma in children. Taiwan Childhood Hepatoma Study Group. N. Eng. J. Med. 1997, 336, 1855–1859. [Google Scholar] [CrossRef] [Green Version]
- Da Silva, C.P.; Emídio, E.S.; de Marchi, M.R. Method validation using weighted linear regression models for quantification of UV filters in water samples. Talanta 2015, 131, 221–227. [Google Scholar] [CrossRef] [Green Version]
- Dawes, R.M. The robust beauty of improper linear models in decision making. Am. Psychol. 1979, 34, 571–582. [Google Scholar] [CrossRef]
- Dawes, R.M.; Corrigan, B. Linear models in decision making. Psychol. Bull. 1974, 81, 95–106. [Google Scholar] [CrossRef]
- Holford, T.R. The estimation of age, period and cohort effects for vital rates. Biometrics 1983, 39, 311–324. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1976–1980 | 1981–1985 | 1986–1990 | 1991–1995 | 1996–2000 | 2001–2005 | 2006–2010 | 2006–2015 | ||
|---|---|---|---|---|---|---|---|---|---|
| Men | 40–44 | 31.41 | 33.10 | 33.20 | 31.24 | 30.40 | 29.10 | 23.26 | 19.30 |
| 45–49 | 46.50 | 55.13 | 52.88 | 53.61 | 49.79 | 47.66 | 42.25 | 36.25 | |
| 50–54 | 68.11 | 72.47 | 74.56 | 81.73 | 81.65 | 74.19 | 69.12 | 56.96 | |
| 55–59 | 84.12 | 97.32 | 98.96 | 115.57 | 127.55 | 117.70 | 100.19 | 85.59 | |
| 60–64 | 103.58 | 120.45 | 115.71 | 143.74 | 164.14 | 168.20 | 145.35 | 119.83 | |
| 65–69 | 126.15 | 140.12 | 138.76 | 160.29 | 186.58 | 204.31 | 203.50 | 172.15 | |
| 70–74 | 135.44 | 147.79 | 170.44 | 195.56 | 201.40 | 223.00 | 253.46 | 225.23 | |
| 75–79 | 145.41 | 178.22 | 186.70 | 226.86 | 243.87 | 234.63 | 263.24 | 293.21 | |
| 80–84 | 123.63 | 160.33 | 175.09 | 229.23 | 267.55 | 264.61 | 276.39 | 278.95 | |
| 85+ | 133.97 | 232.56 | 212.33 | 227.57 | 248.07 | 292.51 | 272.51 | 291.86 | |
| Women | 40–44 | 6.75 | 6.14 | 4.90 | 5.11 | 3.46 | 2.88 | 3.03 | 2.44 |
| 45–49 | 11.99 | 11.10 | 9.21 | 9.76 | 6.49 | 5.76 | 4.90 | 3.79 | |
| 50–54 | 18.20 | 16.23 | 14.78 | 15.53 | 14.15 | 11.78 | 10.20 | 8.17 | |
| 55–59 | 27.57 | 30.06 | 24.45 | 28.43 | 28.65 | 28.04 | 23.68 | 18.34 | |
| 60–64 | 35.23 | 39.48 | 41.09 | 44.75 | 55.75 | 52.97 | 48.01 | 37.94 | |
| 65–69 | 43.49 | 54.68 | 52.09 | 66.36 | 76.92 | 89.05 | 82.80 | 73.44 | |
| 70–74 | 50.40 | 61.49 | 65.48 | 87.47 | 111.46 | 130.60 | 131.32 | 123.96 | |
| 75–79 | 66.47 | 72.02 | 77.57 | 105.09 | 127.37 | 153.26 | 160.98 | 170.88 | |
| 80–84 | 60.12 | 74.79 | 81.83 | 101.26 | 139.41 | 175.41 | 184.90 | 209.80 | |
| 85+ | 54.22 | 82.91 | 71.93 | 103.98 | 132.42 | 169.12 | 196.03 | 214.09 |
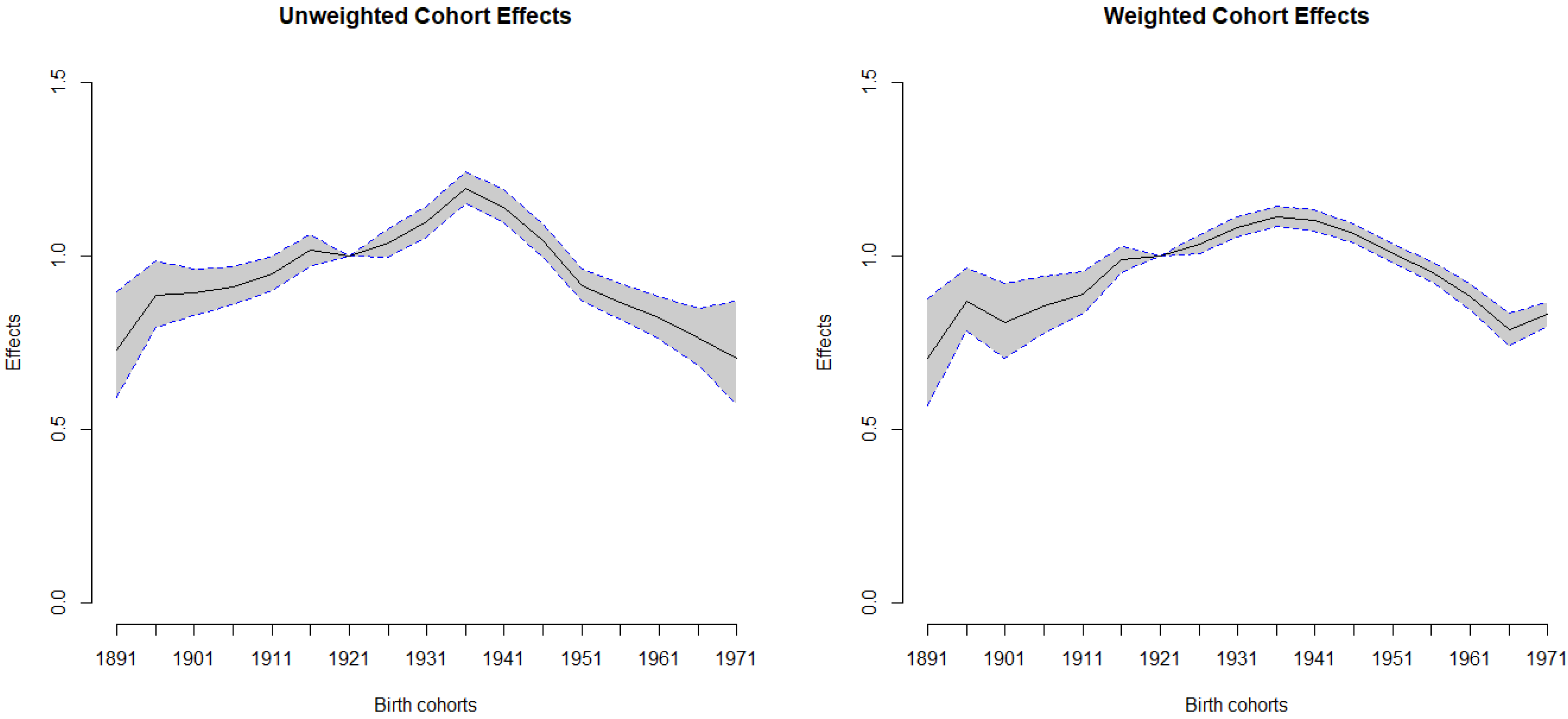
| Cohort | Unweighted | Weighted | ||
|---|---|---|---|---|
| (1891~1971) | Effects | 95% CI for Effects | Effects | 95% CI for Effects |
| 1891 | 0.73 | 0.591–0.898 | 0.71 | 0.567–0.877 |
| 1896 | 0.88 | 0.795–0.986 | 0.87 | 0.784–0.967 |
| 1901 | 0.89 | 0.828–0.962 | 0.81 | 0.706–0.922 |
| 1906 | 0.91 | 0.859–0.967 | 0.85 | 0.777–0.940 |
| 1911 | 0.95 | 0.901–0.998 | 0.89 | 0.832–0.956 |
| 1916 | 1.01 | 0.970–1.062 | 0.99 | 0.950–1.027 |
| 1921 | 1.00 | REF | 1.00 | REF |
| 1926 | 1.04 | 0.997–1.079 | 1.03 | 1.007–1.060 |
| 1931 | 1.10 | 1.055–1.142 | 1.08 | 1.056–1.111 |
| 1936 | 1.20 | 1.149–1.243 | 1.11 | 1.083–1.145 |
| 1941 | 1.14 | 1.094–1.190 | 1.10 | 1.072–1.131 |
| 1946 | 1.04 | 0.997–1.092 | 1.06 | 1.036–1.093 |
| 1951 | 0.91 | 0.868–0.961 | 1.00 | 0.978–1.033 |
| 1956 | 0.87 | 0.817–0.921 | 0.96 | 0.927–0.985 |
| 1961 | 0.82 | 0.761–0.884 | 0.88 | 0.847–0.922 |
| 1966 | 0.76 | 0.685–0.849 | 0.79 | 0.740–0.834 |
| 1971 | 0.71 | 0.573–0.870 | 0.83 | 0.796–0.866 |
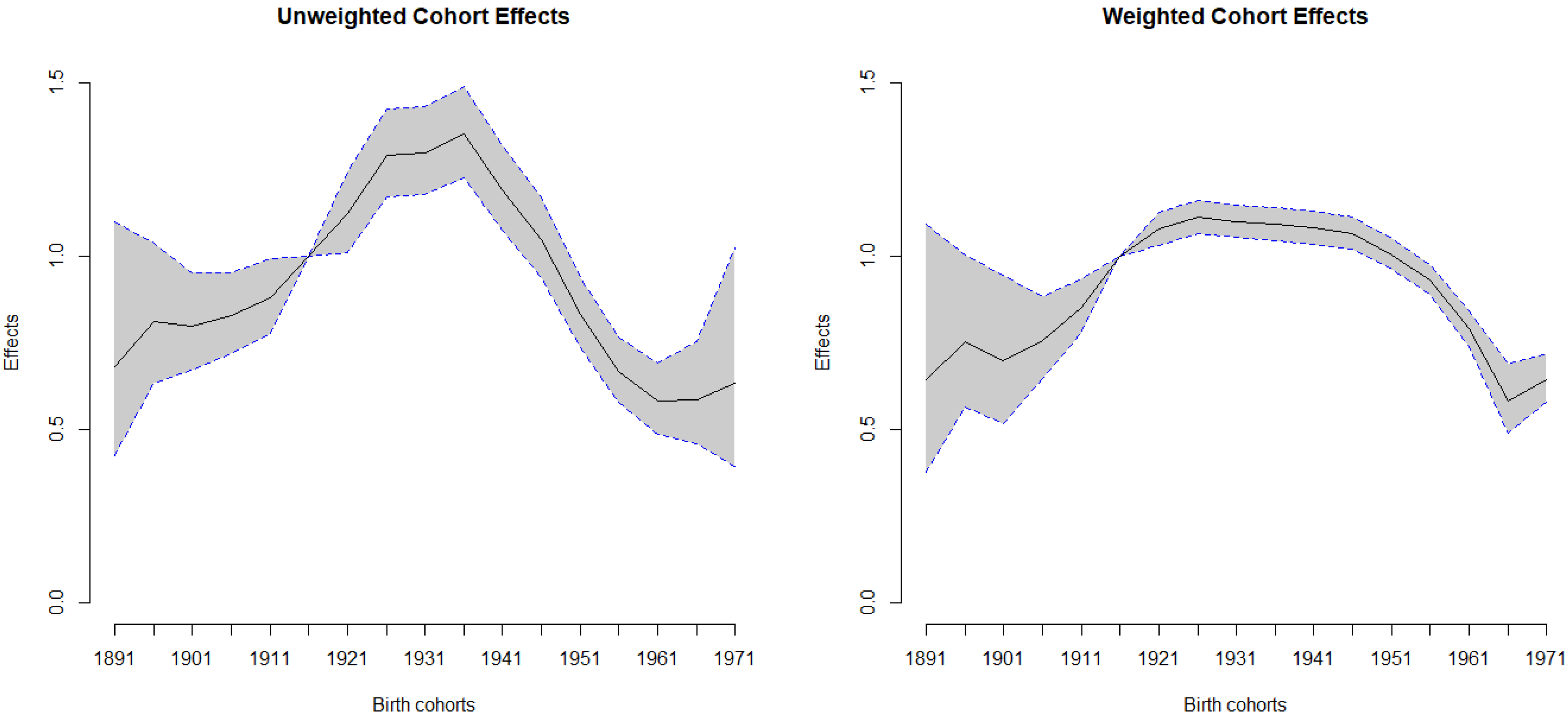
| Cohort | Unweighted | Weighted | ||
|---|---|---|---|---|
| (1891~1971) | Effects | 95% CI for Effects | Effects | 95% CI for Effects |
| 1891 | 0.68 | 0.423–1.099 | 0.64 | 0.378–1.090 |
| 1896 | 0.81 | 0.632–1.038 | 0.75 | 0.564–1.001 |
| 1901 | 0.80 | 0.669–0.951 | 0.70 | 0.516–0.944 |
| 1906 | 0.83 | 0.718–0.953 | 0.76 | 0.648–0.884 |
| 1911 | 0.88 | 0.778–0.994 | 0.85 | 0.779–0.935 |
| 1916 | 1.00 | REF | 1.00 | REF |
| 1921 | 1.12 | 1.011–1.243 | 1.08 | 1.031–1.125 |
| 1926 | 1.29 | 1.169–1.422 | 1.11 | 1.065–1.159 |
| 1931 | 1.30 | 1.178–1.432 | 1.10 | 1.053–1.147 |
| 1936 | 1.35 | 1.224–1.490 | 1.09 | 1.044–1.139 |
| 1941 | 1.19 | 1.073–1.320 | 1.08 | 1.035–1.129 |
| 1946 | 1.05 | 0.937–1.170 | 1.06 | 1.019–1.112 |
| 1951 | 0.83 | 0.735–0.939 | 1.00 | 0.961–1.049 |
| 1956 | 0.67 | 0.579–0.768 | 0.93 | 0.890–0.977 |
| 1961 | 0.58 | 0.487–0.692 | 0.79 | 0.740–0.843 |
| 1966 | 0.59 | 0.458–0.752 | 0.58 | 0.490–0.689 |
| 1971 | 0.63 | 0.394–1.023 | 0.64 | 0.577–0.721 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tzeng, I.-S.; Chen, J.-H. Exploring Hepatocellular Carcinoma Mortality Using Weighted Regression Estimation for the Cohort Effect in Taiwan from 1976 to 2015. Int. J. Environ. Res. Public Health 2022, 19, 5573. https://doi.org/10.3390/ijerph19095573
Tzeng I-S, Chen J-H. Exploring Hepatocellular Carcinoma Mortality Using Weighted Regression Estimation for the Cohort Effect in Taiwan from 1976 to 2015. International Journal of Environmental Research and Public Health. 2022; 19(9):5573. https://doi.org/10.3390/ijerph19095573
Chicago/Turabian StyleTzeng, I-Shiang, and Jiann-Hwa Chen. 2022. "Exploring Hepatocellular Carcinoma Mortality Using Weighted Regression Estimation for the Cohort Effect in Taiwan from 1976 to 2015" International Journal of Environmental Research and Public Health 19, no. 9: 5573. https://doi.org/10.3390/ijerph19095573
APA StyleTzeng, I.-S., & Chen, J.-H. (2022). Exploring Hepatocellular Carcinoma Mortality Using Weighted Regression Estimation for the Cohort Effect in Taiwan from 1976 to 2015. International Journal of Environmental Research and Public Health, 19(9), 5573. https://doi.org/10.3390/ijerph19095573