
Phyx.io: Expert-Based Decision Making for the Selection of At-Home Rehabilitation Solutions for Active and Healthy Aging

 , ,
, ,  , , ,
, , ,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Alternatives
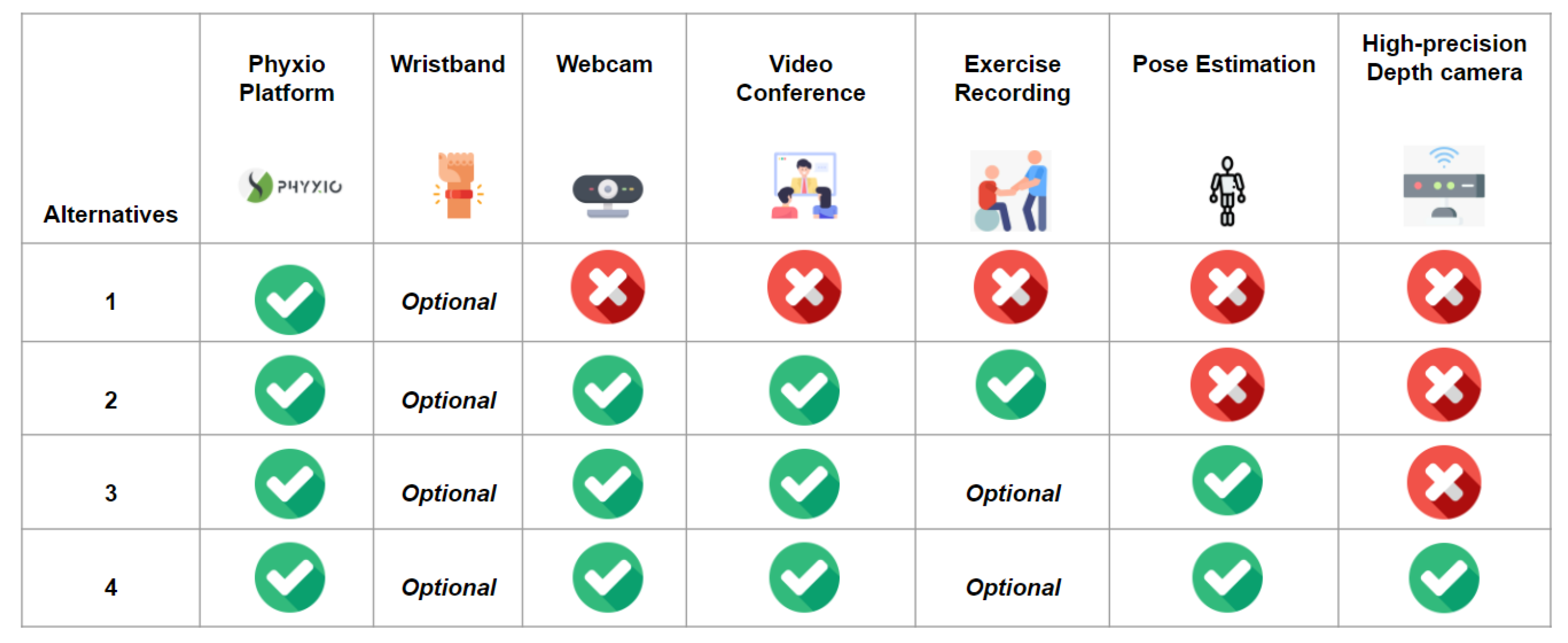
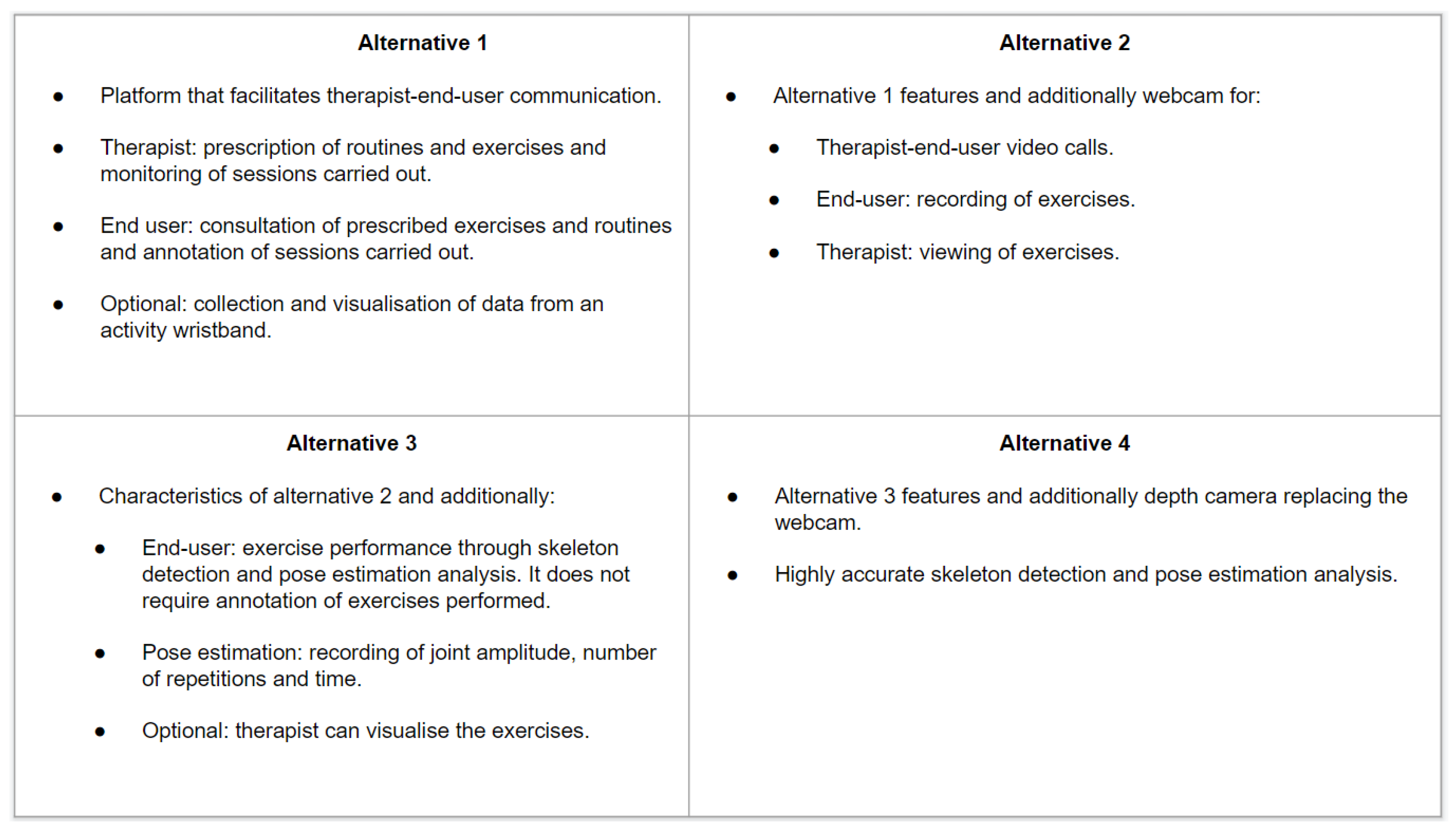
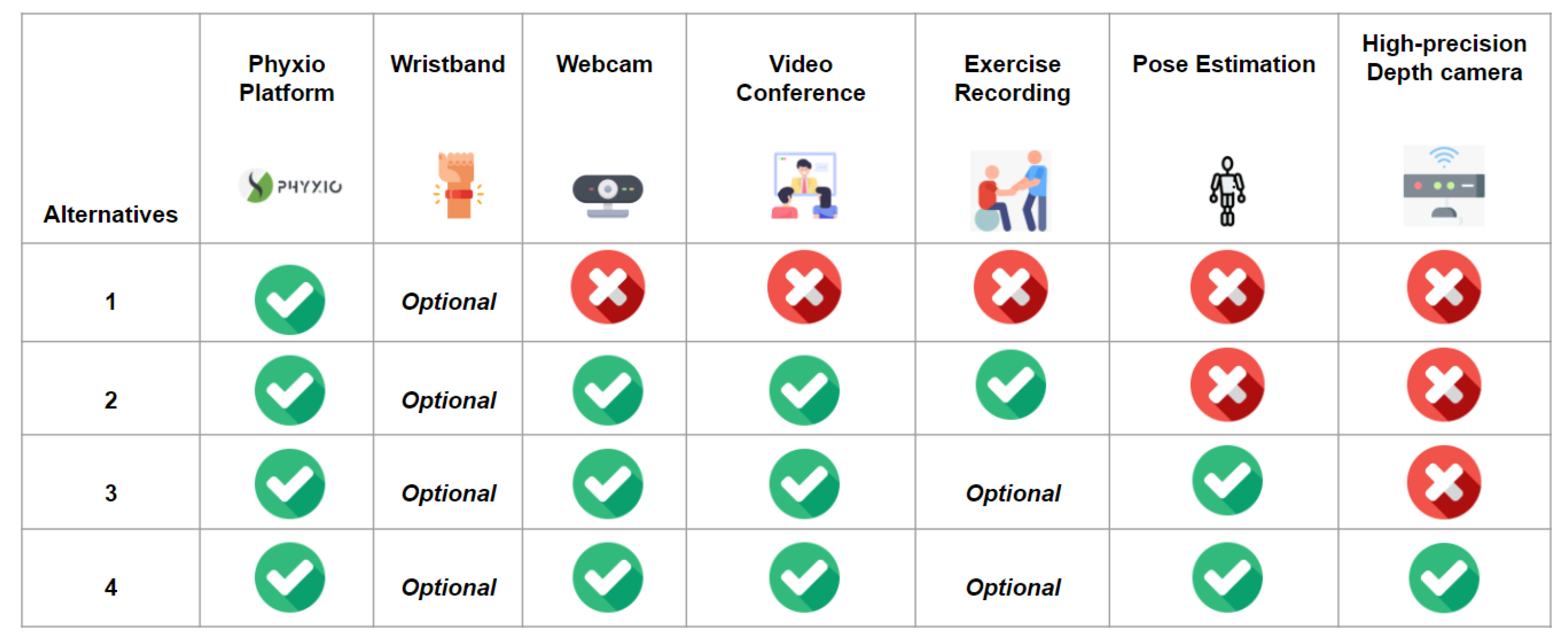
- Alternative 1: A digital solution for physical rehabilitation that does not provide video-based supervision/monitoring support.
- Alternative 2: A digital solution that is equipped with a camera but without any support for posture estimation or, in other words, without support through the supervision/monitoring of exercise performance. The camera is only used for video recording and video call functions.
- Alternative 3: A digital solution with a camera and software that provides information on the estimation of the body posture and therefore supervises or monitors the performance of exercises.
- Alternative 4: A digital solution using a special type of camera with depth information, used for a more accurate estimation of body position.
2.3.1. Alternative 3
- BlazePose Detector: This model is intended to process RGB images and yield one of the following results:
- the position of the center of the detected hips;
- the radius of the circumference surrounding the detected person;
- the inclination angle of the straight line connecting the center of the hips to the center of the shoulders.
- BlazePose GHUM 3D [29]: This model processes both the image and the regions of Interest (ROIs) detected from the previous model, calculating the position of 33 joints that, after a post-processing stage, yields two elements:
- Pose Landmarks: These contain the list of the position, in 3D coordinates, for the 33 joints. The depth information of every joint (i.e., the z coordinate) has its coordinate origin in the hip center, previously calculated. The depth information will increase as the person moves away the camera. Additionally, a percentage of the visibility of every joint is also provided.
- Pose World Landmarks: These contain the same information as the Pose Landmarks, although the values are provided in meters rather than in pixels, as for the previous one.
2.3.2. Alternative 4
- Stereo Vision: This approach closely resembles the way humans see the world, as it uses two cameras to mimic how human eyes collect depth information from the environment.
- Structured Light: This method requires projecting a certain light pattern by means of a projector, while one or more cameras (placed at a known angle with respect to the projector) are in charge of identifying this pattern in the environment. To obtain the depth information, the difference between the projected pattern and the distorted pattern captured by the cameras is calculated.
- Time Of Flight (ToF): In this approach, light patterns are emitted by lasers in the infrared spectrum and their reflection is captured by a receiver. To obtain the depth map, the Time of Flight (ToF) concept is used. This is the time it takes for light to reach a certain distance. Because the speed of light is known, it is possible to determine the distance of objects by interpreting the time it takes for the projected infrared light to come and go. The time required is directly proportional to the distance.
2.4. Procedure
2.4.1. Determining the Attributes
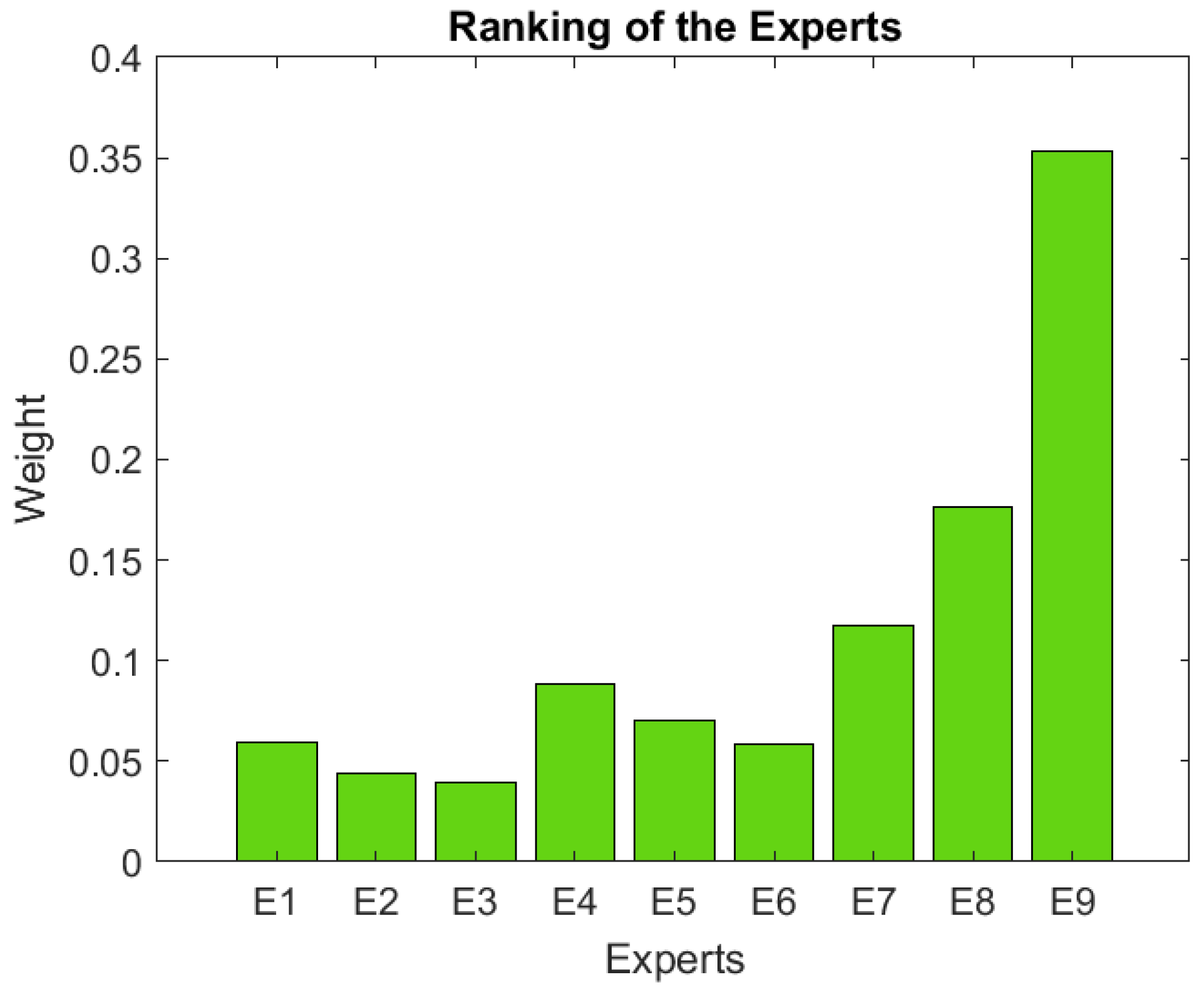
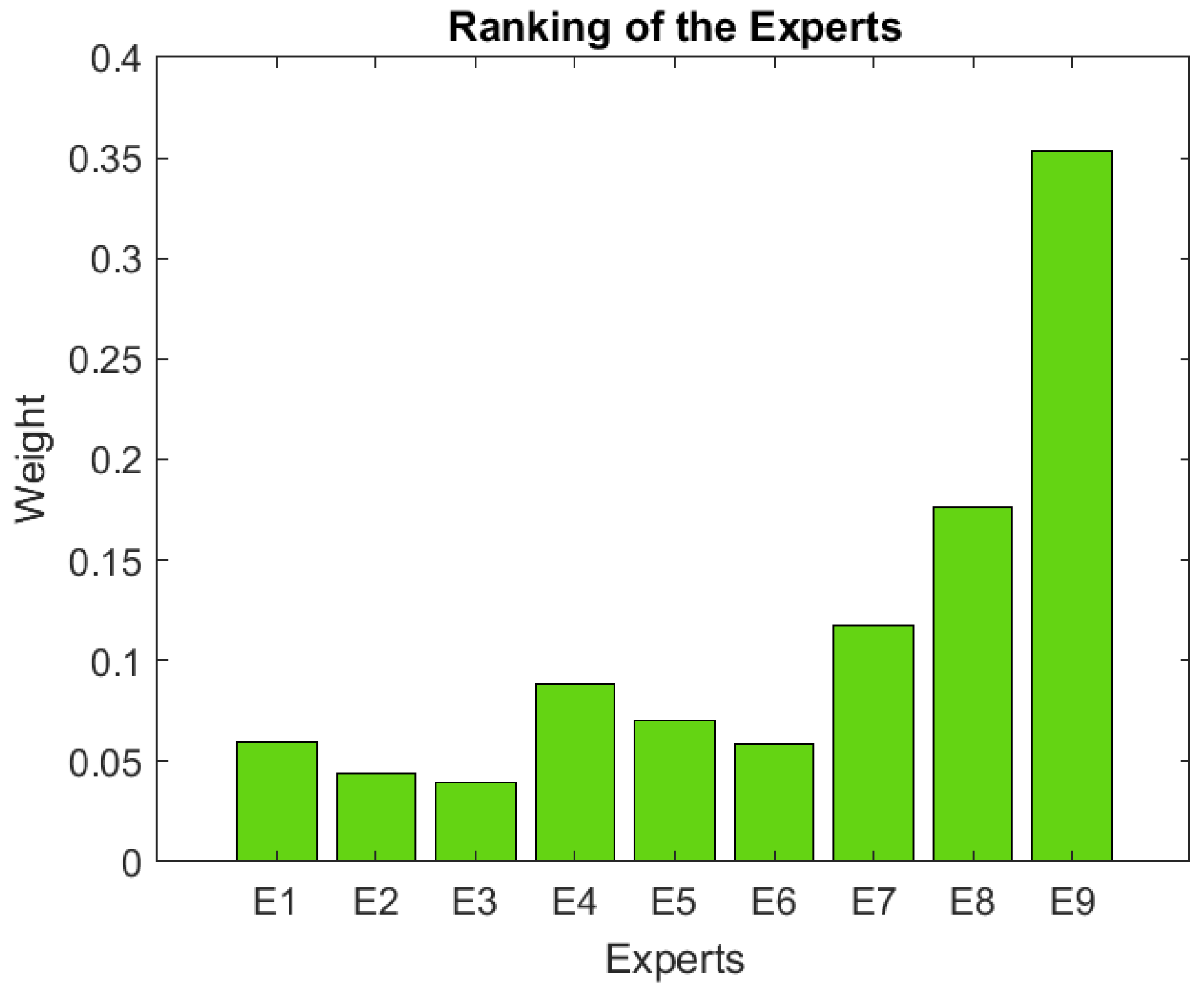
2.4.2. Specifying and Ranking the Experts
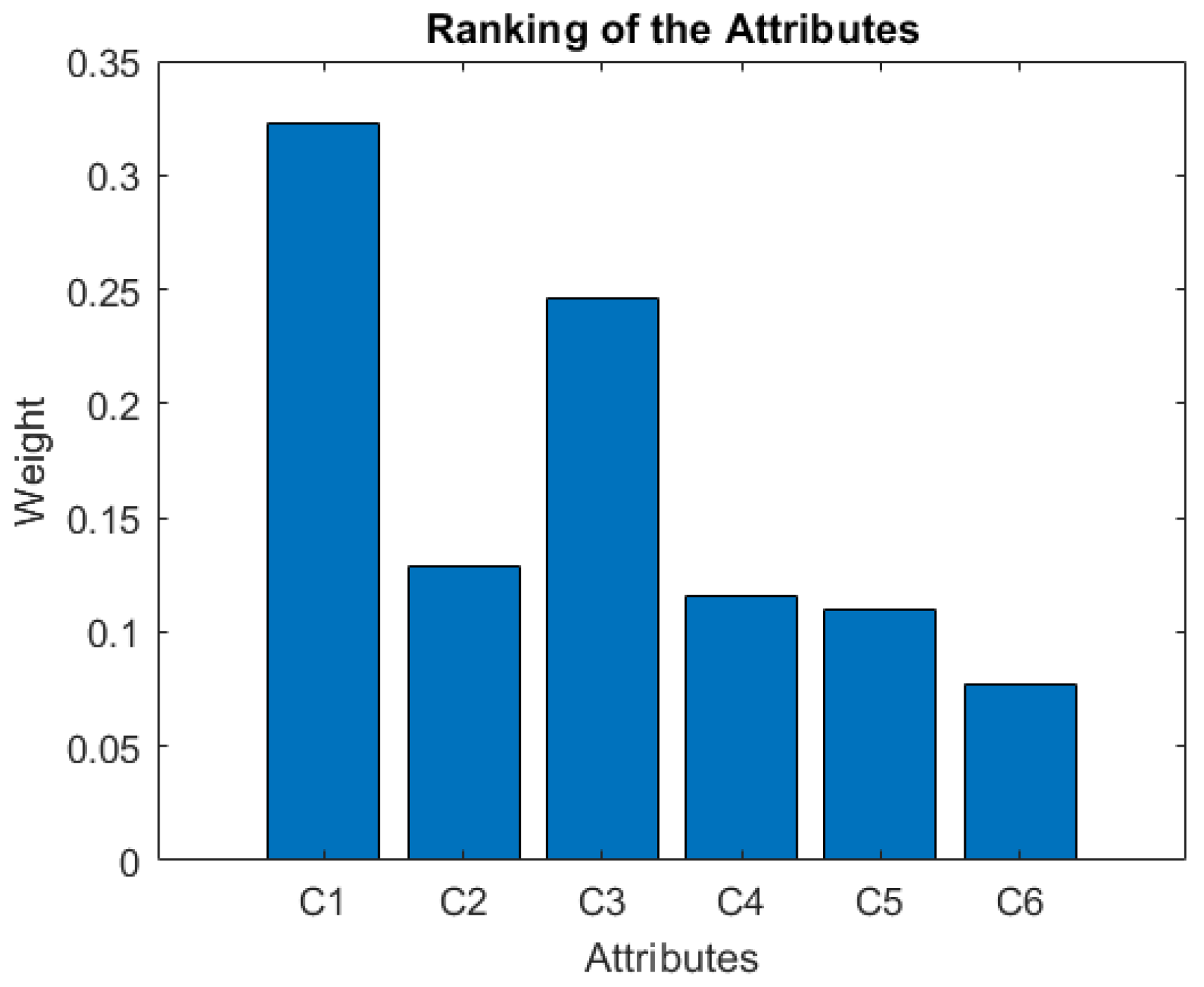
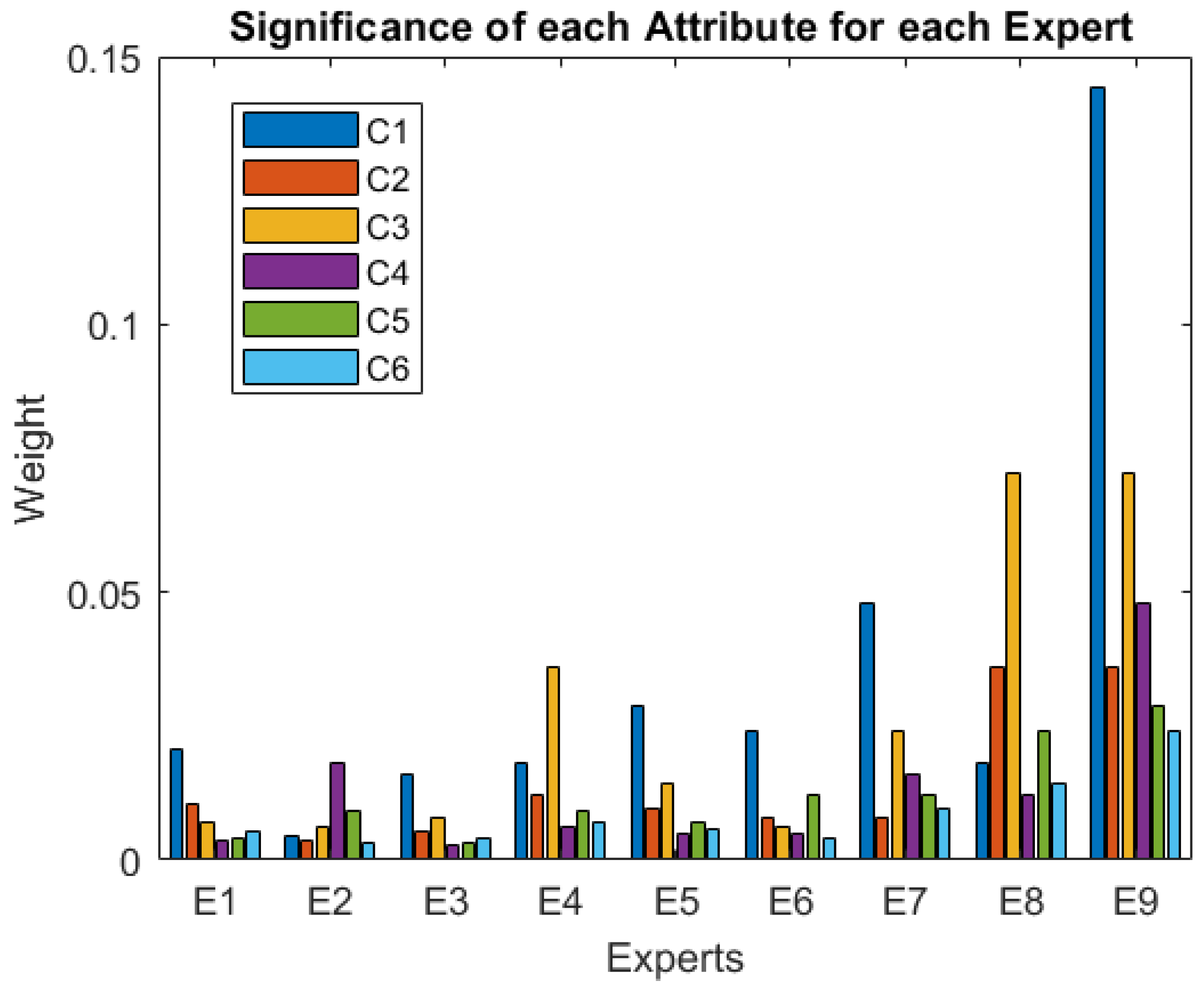
2.4.3. Ranking the Attributes
2.4.4. Ranking the Alternatives in Each Attribute
- Videos explaining the different functionalities of the four alternatives over the Phyx.io Platform (https://youtu.be/sdtMTHLGkFA, accessed on 30 March 2022), the pose estimation video (https://youtu.be/SrbcbDZkhOA, accessed on 30 March 2022), a video showing the performance of an exercise (https://youtu.be/05KisckHgZE, accessed on 30 March 2022) for Alternative 3 and 4, and a video that shows how the video call functionality is accessed using an RFID band (https://youtu.be/SLvdw1IW2fA, accessed on 30 March 2022), which is part of Alternative 2, 3, and 4;
- a table with the main features and functionalities of the four considered alternatives (Figure 1);
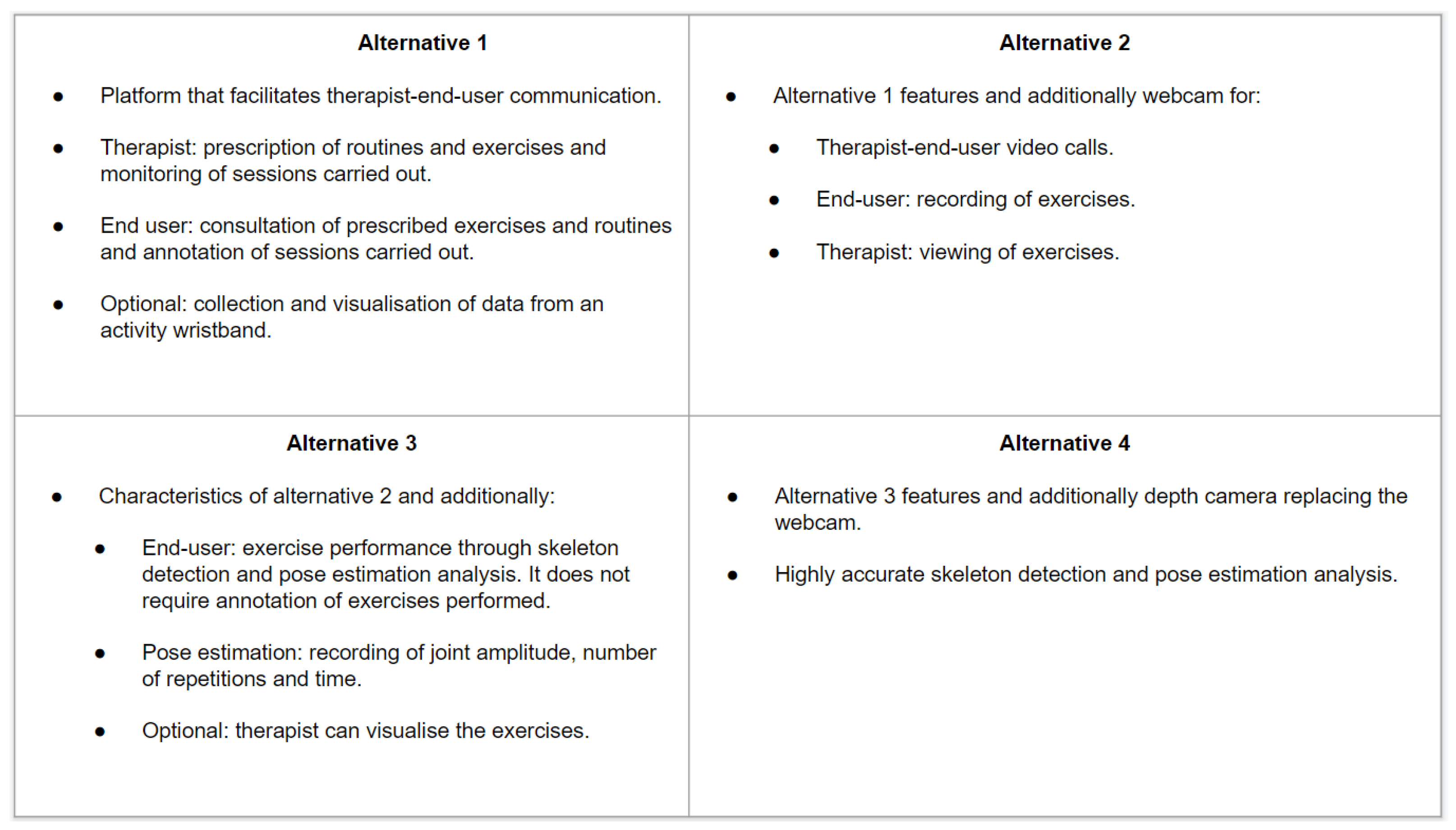
- tables summarizing the four alternatives, according to each of the considered attributes; Figure 2 shows an example of the usefulness attribute for each of the four alternatives.
2.4.5. Solving the Model
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- European Commission. Green Paper on Ageing: Fostering Solidarity and Responsibility between Generations; Technical Report; European Commission Brussels: Brussels, Belgium, 2021. [Google Scholar]
- World Health Organization. Action Plan for the Prevention and Control of Noncommunicable Diseases in the WHO European Region; Technical Report; World Health Organization, Regional Office for Europe: Copenhagen, Denmark, 2016. [Google Scholar]
- Langhammer, B.; Bergland, A.; Rydwik, E. The Importance of Physical Activity Exercise among Older People. BioMed Res. Int. Hindawi 2018, 2018, 7856823. [Google Scholar] [CrossRef] [PubMed]
- Lindley, R.I.; Anderson, C.S.; Billot, L.; Forster, A.; Hackett, M.L.; Harvey, L.A.; Jan, S.; Li, Q.; Liu, H.; Langhorne, P.; et al. Family-led rehabilitation after stroke in India (ATTEND): A randomised controlled trial. Lancet 2017, 390, 588–599. [Google Scholar] [CrossRef]
- Vloothuis, J.D.; Mulder, M.; Nijland, R.H.; Goedhart, Q.S.; Konijnenbelt, M.; Mulder, H.; Hertogh, C.M.; Van Tulder, M.; Van Wegen, E.E.; Kwakkel, G. Caregiver-mediated exercises with e-health support for early supported discharge after stroke (CARE4STROKE): A randomized controlled trial. PLoS ONE 2019, 14, e0214241. [Google Scholar] [CrossRef] [PubMed]
- McCloskey, R.; Donovan, C.; Stewart, C.; Donovan, A. How registered nurses, licensed practical nurses and resident aides spend time in nursing homes: An observational study. Int. J. Nurs. Stud. 2015, 52, 1475–1483. [Google Scholar] [CrossRef]
- de Souto Barreto, P.; Morley, J.E.; Chodzko-Zajko, W.; Pitkala, K.H.; Weening-Djiksterhuis, E.; Rodriguez-Mañas, L.; Barbagallo, M.; Rosendahl, E.; Sinclair, A.; Landi, F.; et al. Recommendations on physical activity and exercise for older adults living in long-term care facilities: A taskforce report. J. Am. Med. Dir. Assoc. 2016, 17, 381–392. [Google Scholar] [CrossRef]
- Sun, V.; Raz, D.J.; Kim, J.Y.; Melstrom, L.; Hite, S.; Varatkar, G.; Fong, Y. Barriers and facilitators of adherence to a perioperative physical activity intervention for older adults with cancer and their family caregivers. J. Geriatr. Oncol. 2020, 11, 256–262. [Google Scholar] [CrossRef] [Green Version]
- Han, B.H.; Sadarangani, T.; Wyatt, L.C.; Zanowiak, J.M.; Kwon, S.C.; Trinh-Shevrin, C.; Lee, L.; Islam, N.S. Correlates of Physical Activity Among Middle-Aged and Older Korean Americans at Risk for Diabetes. J. Nurs. Scholarsh. 2016, 48, 48–57. [Google Scholar] [CrossRef] [Green Version]
- Ige-Elegbede, J.; Pilkington, P.; Gray, S.; Powell, J. Barriers and facilitators of physical activity among adults and older adults from Black and Minority Ethnic groups in the UK: A systematic review of qualitative studies. Prev. Med. Rep. 2019, 15, 100952. [Google Scholar] [CrossRef]
- de Moraes, S.A.; Furlanetto, E.C.; Ricci, N.A.; Perracini, M.R. Sedentary behavior: Barriers and facilitators among older adults after hip fracture surgery. A qualitative study. Braz. J. Phys. Ther. 2020, 24, 407–414. [Google Scholar] [CrossRef]
- Wilkie, R.; Peat, G.; Thomas, E.; Croft, P. The prevalence of person-perceived participation restriction in community-dwelling older adults. Qual. Life Res. 2006, 15, 1471–1479. [Google Scholar] [CrossRef]
- Chaabene, H.; Prieske, O.; Herz, M.; Moran, J.; Höhne, J.; Kliegl, R.; Ramirez-Campillo, R.; Behm, D.; Hortobágyi, T.; Granacher, U. Home-based exercise programmes improve physical fitness of healthy older adults: A PRISMA-compliant systematic review and meta-analysis with relevance for COVID-19. Ageing Res. Rev. 2021, 67, 101265. [Google Scholar] [CrossRef]
- Constandt, B.; Thibaut, E.; De Bosscher, V.; Scheerder, J.; Ricour, M.; Willem, A. Exercising in times of lockdown: An analysis of the impact of COVID-19 on levels and patterns of exercise among adults in Belgium. Int. J. Environ. Res. Public Health 2020, 17, 4144. [Google Scholar] [CrossRef]
- Portegijs, E.; Keskinen, K.E.; Tuomola, E.M.; Hinrichs, T.; Saajanaho, M.; Rantanen, T. Older adults’ activity destinations before and during COVID-19 restrictions: From a variety of activities to mostly physical exercise close to home. Health Place 2021, 68, 102533. [Google Scholar] [CrossRef]
- Amorim, J.S.C.d.; Leite, R.C.; Brizola, R.; Yonamine, C.Y. Virtual reality therapy for rehabilitation of balance in the elderly: A systematic review and META-analysis. Adv. Rheumatol. 2019, 58, 18. [Google Scholar] [CrossRef] [Green Version]
- Porras, D.C.; Siemonsma, P.; Inzelberg, R.; Zeilig, G.; Plotnik, M. Advantages of virtual reality in the rehabilitation of balance and gait: Systematic review. Neurology 2018, 90, 1017–1025. [Google Scholar] [CrossRef]
- Dermody, G.; Whitehead, L.; Wilson, G.; Glass, C. The role of virtual reality in improving health outcomes for community-dwelling older adults: Systematic review. J. Med. Internet Res. 2020, 22, e17331. [Google Scholar] [CrossRef]
- Lincke, A.; Fagerström, C.; Ekstedt, M.; Löwe, W.; Backåberg, S. Skeleton avatar technology as a way to measure physical activity in healthy older adults. Inform. Med. Unlocked 2021, 24, 100609. [Google Scholar] [CrossRef]
- Ataei, Y.; Mahmoudi, A.; Feylizadeh, M.R.; Li, D.F. Ordinal Priority Approach (OPA) in Multiple Attribute Decision-Making. Appl. Soft Comput. 2020, 86, 105893. [Google Scholar] [CrossRef]
- Tzeng, G.H.; Huang, J.J. Multiple Attribute Decision Making: Methods and Applications; CRC Press: Boca Raton, FL, USA, 2011. [Google Scholar]
- Alvarez, P.A.; Ishizaka, A.; Martínez, L. Multiple-criteria decision-making sorting methods: A survey. Expert Syst. Appl. 2021, 183, 115368. [Google Scholar] [CrossRef]
- Ongsulee, P. Artificial intelligence, machine learning and deep learning. In Proceedings of the 2017 15th International Conference on ICT and Knowledge Engineering (ICT KE), Bangkok, Thailand, 22–24 November 2017; pp. 1–6. [Google Scholar] [CrossRef]
- Han, J.; Deng, S.; Lo, D.; Zhi, C.; Yin, J.; Xia, X. An Empirical Study of the Dependency Networks of Deep Learning Libraries. In Proceedings of the 2020 IEEE International Conference on Software Maintenance and Evolution (ICSME), Adelaide, SA, Australia, 28 September–2 October 2020; pp. 868–878. [Google Scholar] [CrossRef]
- Tian, Y.; Zhang, H.; Liu, Y.; Wang, L. Recovering 3D Human Mesh from Monocular Images: A Survey. arXiv 2022, arXiv:2203.01923. [Google Scholar]
- Hub, T. Image Pose Detection. 2021. Available online: https://tfhub.dev/google/movenet/singlepose/lightning/4 (accessed on 20 March 2022).
- Bajpai, R.; Joshi, D. MoveNet: A Deep Neural Network for Joint Profile Prediction Across Variable Walking Speeds and Slopes. IEEE Trans. Instrum. Meas. 2021, 70, 2508511. [Google Scholar] [CrossRef]
- Singh, A.K.; Kumbhare, V.A.; Arthi, K. Real-Time Human Pose Detection and Recognition Using MediaPipe. In International Conference on Soft Computing and Signal Processing; Springer: Berlin/Heidelberg, Germany, 2021; pp. 145–154. [Google Scholar]
- Xu, H.; Bazavan, E.G.; Zanfir, A.; Freeman, W.T.; Sukthankar, R.; Sminchisescu, C. GHUM & GHUML: Generative 3D Human Shape and Articulated Pose Models. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Virtual, 14–19 June 2020; 2020; pp. 6184–6193. [Google Scholar]
- TensorFlow. TensorFlow Optimization. 2021. Available online: https://www.tensorflow.org/model_optimization/guide (accessed on 15 March 2022).
- Condotta, I.C.; Brown-Brandl, T.M.; Silva-Miranda, K.O.; Stinn, J.P. Evaluation of a depth sensor for mass estimation of growing and finishing pigs. Biosyst. Eng. 2018, 173, 11–18. [Google Scholar] [CrossRef]
- Fu, L.; Gao, F.; Wu, J.; Li, R.; Karkee, M.; Zhang, Q. Application of consumer RGB-D cameras for fruit detection and localization in field: A critical review. Comput. Electron. Agric. 2020, 177, 105687. [Google Scholar] [CrossRef]
- Biswas, J.; Veloso, M. Depth camera based indoor mobile robot localization and navigation. In Proceedings of the 2012 IEEE International Conference on Robotics and Automation, Saint Paul, MN, USA, 14–18 May 2012; pp. 1697–1702. [Google Scholar]
- Suay, H.B.; Chernova, S. Humanoid robot control using depth camera. In Proceedings of the 6th International Conference on Human-Robot Interaction, Lausanne, Switzerland, 6–9 March 2011; pp. 401–402. [Google Scholar]
- Osman, H.I.; Hashim, F.H.; Zaki, W.M.D.W.; Huddin, A.B. Entryway detection algorithm using Kinect’s depth camera for UAV application. In Proceedings of the 2017 IEEE 8th Control and System Graduate Research Colloquium (ICSGRC), Shah Alam, Malaysia, 4–5 August 2017; pp. 77–80. [Google Scholar]
- Iacono, M.; Sgorbissa, A. Path following and obstacle avoidance for an autonomous UAV using a depth camera. Robot. Auton. Syst. 2018, 106, 38–46. [Google Scholar] [CrossRef]
- Halim, Z.; Khan, R.U.A.; Waqas, M.; Tu, S. Utilizing 3D joints data extracted through depth camera to train classifiers for identifying suicide bomber. Expert Syst. Appl. 2021, 179, 115081. [Google Scholar] [CrossRef]
- Yamamoto, J.; Inoue, K.; Yoshioka, M. Investigation of customer behavior analysis based on top-view depth camera. In Proceedings of the 2017 IEEE Winter Applications of Computer Vision Workshops (WACVW), Santa Rosa, CA, USA, 24–31 March 2017; pp. 67–74. [Google Scholar]
- Ando, Y.; Ege, T.; Cho, J.; Yanai, K. Depthcaloriecam: A mobile application for volume-based foodcalorie estimation using depth cameras. In Proceedings of the 5th International Workshop on Multimedia Assisted Dietary Management, Nice, France, 21 October 2019; pp. 76–81. [Google Scholar]
- Siddiqi, M.H.; Almashfi, N.; Ali, A.; Alruwaili, M.; Alhwaiti, Y.; Alanazi, S.; Kamruzzaman, M. A Unified Approach for Patient Activity Recognition in Healthcare Using Depth Camera. IEEE Access 2021, 9, 92300–92317. [Google Scholar] [CrossRef]
- Ghose, A.; Sinha, P.; Bhaumik, C.; Sinha, A.; Agrawal, A.; Dutta Choudhury, A. UbiHeld: Ubiquitous healthcare monitoring system for elderly and chronic patients. In Proceedings of the 2013 ACM Conference on Pervasive and Ubiquitous Computing Adjunct Publication, Zurich, Switzerland, 8–12 September 2013; pp. 1255–1264. [Google Scholar]
- Choppin, S.; Wheat, J. The potential of the Microsoft Kinect in sports analysis and biomechanics. Sport. Technol. 2013, 6, 78–85. [Google Scholar] [CrossRef]
- Hegazy, H.; Abdelsalam, M.; Hussien, M.; Elmosalamy, S.; Hassan, Y.M.; Nabil, A.M.; Atia, A. Online detection and classification of in-corrected played strokes in table tennis using IR depth camera. Procedia Comput. Sci. 2020, 170, 555–562. [Google Scholar] [CrossRef]
- Chen, C.; Jafari, R.; Kehtarnavaz, N. Fusion of depth, skeleton, and inertial data for human action recognition. In Proceedings of the 2016 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Shanghai, China, 20–25 March 2016; pp. 2712–2716. [Google Scholar]
- Ji, X.; Cheng, J.; Feng, W.; Tao, D. Skeleton embedded motion body partition for human action recognition using depth sequences. Signal Process. 2018, 143, 56–68. [Google Scholar] [CrossRef]
- Jiang, M.; Kong, J.; Bebis, G.; Huo, H. Informative joints based human action recognition using skeleton contexts. Signal Process. Image Commun. 2015, 33, 29–40. [Google Scholar] [CrossRef]
- Vemulapalli, R.; Arrate, F.; Chellappa, R. Human action recognition by representing 3d skeletons as points in a lie group. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Columbus, OH, USA, 23–28 June 2014; pp. 588–595. [Google Scholar]
- Dorado, J.; del Toro, X.; Santofimia, M.J.; Parreño, A.; Cantarero, R.; Rubio, A.; Lopez, J.C. A computer-vision-based system for at-home rheumatoid arthritis rehabilitation. Int. J. Distrib. Sens. Netw. 2019, 15, 1550147719875649. [Google Scholar] [CrossRef]
- Eichler, N.; Hel-Or, H.; Shmishoni, I.; Itah, D.; Gross, B.; Raz, S. Non-invasive motion analysis for stroke rehabilitation using off the shelf 3d sensors. In Proceedings of the 2018 International Joint Conference on Neural Networks (IJCNN), Rio de Janeiro, Brazil, 8–13 July 2018; pp. 1–8. [Google Scholar]
- Uccheddu, F.; Governi, L.; Carfagni, M. A preliminary 3D depth camera-based system to assist home physiotherapy rehabilitation. In International Conference of the Italian Association of Design Methods and Tools for Industrial Engineering; Springer: Berlin/Heidelberg, Germany, 2019; pp. 696–706. [Google Scholar]
- Jawed, U.; Mazhar, A.; Altaf, F.; Rehman, A.; Shams, S.; Asghar, A. Rehabilitation posture correction using neural network. In Proceedings of the 2019 4th International Conference on Emerging Trends in Engineering, Sciences and Technology (ICEEST), Karachi, Pakistan, 10–11 December 2019; pp. 1–5. [Google Scholar]
- Piraintorn, P.; Sa-ing, V. Stroke rehabilitation based on intelligence interaction system. In Proceedings of the 2020 17th International Conference on Electrical Engineering/Electronics, Computer, Telecommunications and Information Technology (ECTI-CON), Phuket, Thailand, 24–27 June 2020; pp. 648–651. [Google Scholar]
- Mehra, S.; Visser, B.; Cila, N.; van den Helder, J.; Engelbert, R.H.; Weijs, P.J.; Kröse, B.J. Supporting Older Adults in Exercising With a Tablet: A Usability Study. JMIR Hum. Factors 2019, 6, e11598. [Google Scholar] [CrossRef] [PubMed]
- Wildenbos, G.A.; Peute, L.; Jaspers, M. Aging barriers influencing mobile health usability for older adults: A literature based framework (MOLD-US). Int. J. Med. Inform. 2018, 114, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Tsertsidis, A.; Kolkowska, E.; Hedström, K. Factors influencing seniors’ acceptance of technology for ageing in place in the post-implementation stage: A literature review. Int. J. Med. Inform. 2019, 129, 324–333. [Google Scholar] [CrossRef]
- Valdez, A.C.; Ziefle, M. The users’ perspective on the privacy-utility trade-offs in health recommender systems. Int. J. Hum.-Comput. Stud. 2019, 121, 108–121. [Google Scholar] [CrossRef] [Green Version]
- Campbell, R.; Evans, M.; Tucker, M.; Quilty, B.; Dieppe, P.; Donovan, J. Why don’t patients do their exercises? Understanding non-compliance with physiotherapy in patients with osteoarthritis of the knee. J. Epidemiol. Community Health 2001, 55, 132–138. [Google Scholar] [CrossRef] [Green Version]
- Argent, R.; Daly, A.; Caulfield, B. Patient involvement with home-based exercise programs: Can connected health interventions influence adherence? JMIR Mhealth Uhealth 2018, 6, e8518. [Google Scholar] [CrossRef] [Green Version]
- McDonald, M.; Siebert, S.; Coulter, E.; McDonald, D.; Paul, L. Level of adherence to prescribed exercise in spondyloarthritis and factors affecting this adherence: A systematic review. Rheumatol. Int. 2019, 39, 187–201. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Resolution | FPS | USB | Price (€) | |
|---|---|---|---|---|
| Logitech HD Webcam C270 | 1280 × 720 | 30 | 2.0 | 34.99 |
| Logitech HD Pro Webcam C920 | 1920 × 1080 | 60 | 3.0 | 78.97 |
| Logitech HD Webcam C310 | 1280 × 720 | 30 | 2.0 | 61.99 |
| Owlotech Start Webcam 720p | 1280 × 720 | - | 2.0 | 29.99 |
| Krom Kam Webcam 1080P HD | 1920 × 1080 | 30 | 2.0 | 18.98 |
| MoveNetV2 | BlazePose GHUM | |
|---|---|---|
| Joint number | 17 | 33 |
| Is it 3D? | No | Yes |
| Formats (https://www.tensorflow.org/hub/model_formats, accessed on 17 March 2022) | TF, TFLite, TFJS | TFLite, TFJS |
| GPU supported? | TF y TFJS | TFJS |
| Model | Accuracy | Speed |
|---|---|---|
| MoveNetV2 Lightning | Not very good | Good |
| MoveNetV2 Thunder | Good | Not very good |
| BlazePose GHUM Lite | Not very good | Good |
| BlazePose GHUM Full | Good | Not very good |
| BlazePose GHUM Heavy | Very good | Bad |
| Stereo Vision | Structured Light | Time Of Flight | |
|---|---|---|---|
| Range | Good | Low | Good |
| Accuracy | Good | Excelent | Good |
| Indoor performance | Good | Excelent | Excelent |
| Outdoor performance | Good | Low | Low |
| Cost | Medium | Low | Medium |
| Depth Technology | Depth Range (m) | Depth Resolution | Frame Rate (FPS) | Development Tools | Price (USD) | |
|---|---|---|---|---|---|---|
| Microsoft Kinect v1 | Structured light | 0.4–3 | 320 × 240, 640 × 480 | 30 | Kinect for Windows SDK v1.8 | Discontinued |
| Microsoft Kinect v2 | Time of flight | 0.5–4.5 | 512 × 424 | 30 | Kinect for Windows SDK 2.0 | Discontinued |
| Microsoft Azure Kinect | Time of flight | 0.25–5.46 | Narrow Mode: 6540 × 576; Wide Mode: 1024 × 1024 | 30 | Microsoft Azure SDK | 399 |
| Intel RealSense D415 | Active IR Stereo | 0.3–10 | 1920 × 1080 | 30–90 | Intel RealSense SDK 2.0 | 259 |
| Intel RealSense D435 | Active IR Stereo using Global Shutter Sensors | 0.105–10 | 1280 × 720 | 30–90 | Intel RealSense SDK 2.0 | 299 |
| ASUS® XtionPro Live | Structured light | 0.8–3.5 | 640 × 480 | 30 | Xtion PRO SDK (discontinued) | Discontinued |
| Stereolabs ZED 2 | Neural Stereo Depth Sensing | 0.2–20 | 4416 × 1242 | 100 | ZED SDK | 449 |
| OAK-D Pro | Embedded stereo | 0.2–35 | 1280 × 800 | 120 | DepthAI SDK | 299 |
| OAK-D-LITE | Embedded stereo | 0.2–19.1 | 640 × 480 | 200 | DepthAI SDK | 149 |
| Acusense A1 | Structured light | 0.2–2 | 640 × 400, 1280 × 800 | 44836 | Acusense SDK | 966 |
| Orbbec Astra (PRO) | Infrared Coded Structured Light | 0.6–8 | 640 × 480 | 30 | Astra SDK | 149 |
| ifm O3X100 | Time of flight | 0.05–3 | 224 × 172 | 20 | third-party tools | 675 |
| e-Con Systems Tara Stereo Camera | Embedded stereo | 0.05–0.3 | 752 × 480 | 60 | third-party tools | 299 |
| Nerian Scarlet 3D Depth Camera | Embedded stereo | 0.14–to infinity | 2432 × 2048 | 120 | third-party tools | not available |
| SO | Processor | RAM | GPU | Skeleton Tracking | Face Tracking | Price | Support | |
|---|---|---|---|---|---|---|---|---|
| Kinect for Windows SDK v1.8 | Windows 7, Windows 8 | Dual-core 2.66-GHz or faster processor | 2 GB | - | Yes | Yes | Free | Discontinued |
| Kinect for Windows SDK 2.0 | Windows 8 | Physical dual-core 3.1 GHz | 4 GB | DX11 capable graphics adapter | Yes | Yes | Free | Discontinued |
| Microsoft Azure SDK | Windows 10, Ubuntu 18 or later version | Seventh Gen Intel CoreTM i5 Processor (Quad Core 2.4 GHz or faster) | 4 GB | NVIDIA GEFORCE GTX 1050 or equivalent | Yes | No | Free | Active |
| Intel RealSense SDK 2.0 | Windows 10, Ubuntu 18.04 | 6th to 10th generation Intel Core™ and Xeon Processors | - | Intel Iris Pro, Intel HD Graphics 520, 530, 630 | Yes | Yes | Free | Active |
| Xtion PRO SDK (discontinued) | - | - | - | - | - | - | - | Discontinued |
| ZED SDK | Windows 10, Ubuntu 16.04 or 18.04 | Quad-core 2.7 GHz or faster | 8 GB | GTX1060 or higher | Yes | third-party tools | Free | Active |
| DepthAI SDK | Windows 10, Ubuntu, macOS, Raspberry Pi OS, Jestson Nano/Xavier | - | - | - | third-party tools | third-party tools | Free | Active |
| Acusense SDK | Windows 10, Ubuntu 18.04 | - | - | - | third-party tools | third-party tools | Free | Active |
| Astra SDK | Windows, Linux, Android | x86 processor 1.8 GHz | 4 GB | - | third-party tools | third-party tools | Free | New version 2021 in beta (Orbbec SDK Beta)) |
| Attribute | Sub-Attribute | Description | Index |
|---|---|---|---|
| Usefulness | Importance given to the utility derived from its use. | ||
| Cost of system | Importance given to the cost of the total system considering the cost savings of each alternative. | ||
| Easiness | Use | Importance given to the ease of use of the system. | |
| Technical Development | Importance given to the ease of technical development of the system. | ||
| Maintenance | Importance given to the ease of maintenance of the system. | ||
| Privacy | Importance given to the use of different devices that may invade privacy. |
| Expert | Role | Professional Position | Experience (in Years) | Level of Education | Index |
|---|---|---|---|---|---|
| E1 | Developer | Professionals, scientists and intellectuals | 15–20 | Doctorate (Ph.D.) | |
| E2 | Developer | Professionals, scientists and intellectuals | 10–15 | Doctorate (Ph.D.) | |
| E3 | Developer | Technicians and mid-level and professionals | 10–15 | Upper Secondary | |
| E4 | Therapist/Physiotherapist | Professionals, scientists and intellectuals | 10-15 | Ordinary degree | |
| E5 | Therapist/Physiotherapist | Professionals, scientists and intellectuals | 5–10 | Ordinary degree | |
| E6 | Therapist/Physiotherapist | Technicians and mid-level and professionals | 5–10 | Postgraduate | |
| E7 | End-user/Caregiver | Elementary occupations | 1–5 | Lower Secondary | |
| E8 | End-user/Caregiver | Elementary occupations | more than 20 | Primary | |
| E9 | End-user/Caregiver | Technicians and mid-level and professionals | more than 20 | Technical/vocational |
| Experts | Weight | Rank |
|---|---|---|
| E1 | 0.0505 | 7 |
| E2 | 0.0442 | 8 |
| E3 | 0.0393 | 9 |
| E4 | 0.0884 | 4 |
| E5 | 0.0707 | 5 |
| E6 | 0.0589 | 6 |
| E7 | 0.1178 | 3 |
| E8 | 0.1767 | 2 |
| E9 | 0.3535 | 1 |
| Attributes | Weight | Rank |
|---|---|---|
| (C1) Usefulness | 0.3225 | 1 |
| (C2) Cost of the system | 0.1291 | 3 |
| (C3) Easiness. Use | 0.2457 | 2 |
| (C4) Easiness. Technical development | 0.1159 | 4 |
| (C5) Easiness. Maintenance | 0.1095 | 5 |
| (C6) Privacy | 0.0773 | 6 |
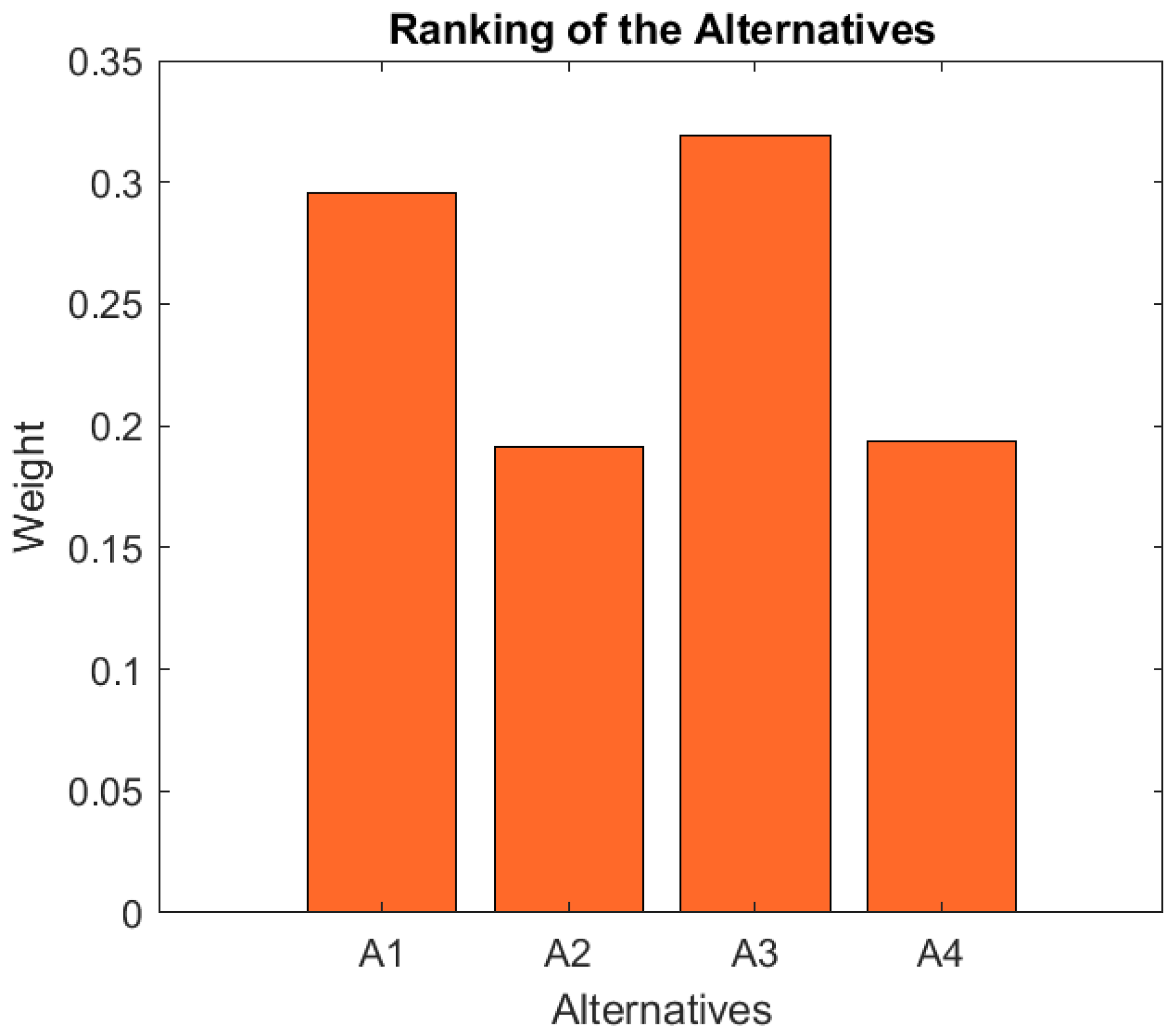
| Alternative | Weight | Rank |
|---|---|---|
| (A1) Alternative 1 | 0.2958 | 2 |
| (A2) Alternative 2 | 0.1916 | 4 |
| (A3) Alternative 3 | 0.3190 | 1 |
| (A4) Alternative 4 | 0.1936 | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dorado Chaparro, J.; Fernández-Bermejo Ruiz, J.; Santofimia Romero, M.J.; del Toro García, X.; Cantarero Navarro, R.; Bolaños Peño, C.; Llumiguano Solano, H.; Villanueva Molina, F.J.; Gonçalves Silva, A.; López, J.C. Phyx.io: Expert-Based Decision Making for the Selection of At-Home Rehabilitation Solutions for Active and Healthy Aging. Int. J. Environ. Res. Public Health 2022, 19, 5490. https://doi.org/10.3390/ijerph19095490
Dorado Chaparro J, Fernández-Bermejo Ruiz J, Santofimia Romero MJ, del Toro García X, Cantarero Navarro R, Bolaños Peño C, Llumiguano Solano H, Villanueva Molina FJ, Gonçalves Silva A, López JC. Phyx.io: Expert-Based Decision Making for the Selection of At-Home Rehabilitation Solutions for Active and Healthy Aging. International Journal of Environmental Research and Public Health. 2022; 19(9):5490. https://doi.org/10.3390/ijerph19095490
Chicago/Turabian StyleDorado Chaparro, Javier, Jesús Fernández-Bermejo Ruiz, María José Santofimia Romero, Xavier del Toro García, Rubén Cantarero Navarro, Cristina Bolaños Peño, Henry Llumiguano Solano, Félix Jesús Villanueva Molina, Anabela Gonçalves Silva, and Juan Carlos López. 2022. "Phyx.io: Expert-Based Decision Making for the Selection of At-Home Rehabilitation Solutions for Active and Healthy Aging" International Journal of Environmental Research and Public Health 19, no. 9: 5490. https://doi.org/10.3390/ijerph19095490
APA StyleDorado Chaparro, J., Fernández-Bermejo Ruiz, J., Santofimia Romero, M. J., del Toro García, X., Cantarero Navarro, R., Bolaños Peño, C., Llumiguano Solano, H., Villanueva Molina, F. J., Gonçalves Silva, A., & López, J. C. (2022). Phyx.io: Expert-Based Decision Making for the Selection of At-Home Rehabilitation Solutions for Active and Healthy Aging. International Journal of Environmental Research and Public Health, 19(9), 5490. https://doi.org/10.3390/ijerph19095490