
The Daalbirrwirr Gamambigu (Safe Children) Model: Embedding Cultural Safety in Child Protection Responses for Australian Aboriginal Children in Hospital Settings



 , and
, and .jpeg)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
- Developing appropriate governance and oversight;
- Cultural engagement process and mapping;
- Scoping literature review;
- Yarning groups and in-depth interviews; and
- Clinical utility testing.
2.1. Settings and Context
2.2. Phase 1: Developing Appropriate Governance and Oversight
2.3. Phase 2: Cultural Engagement Process and Mapping
2.4. Phase 3: Scoping Literature Review
2.5. Phase 4: Yarning Groups and In-Depth Interviews
2.6. Phase 5: Clinical Utility Testing
3. Results
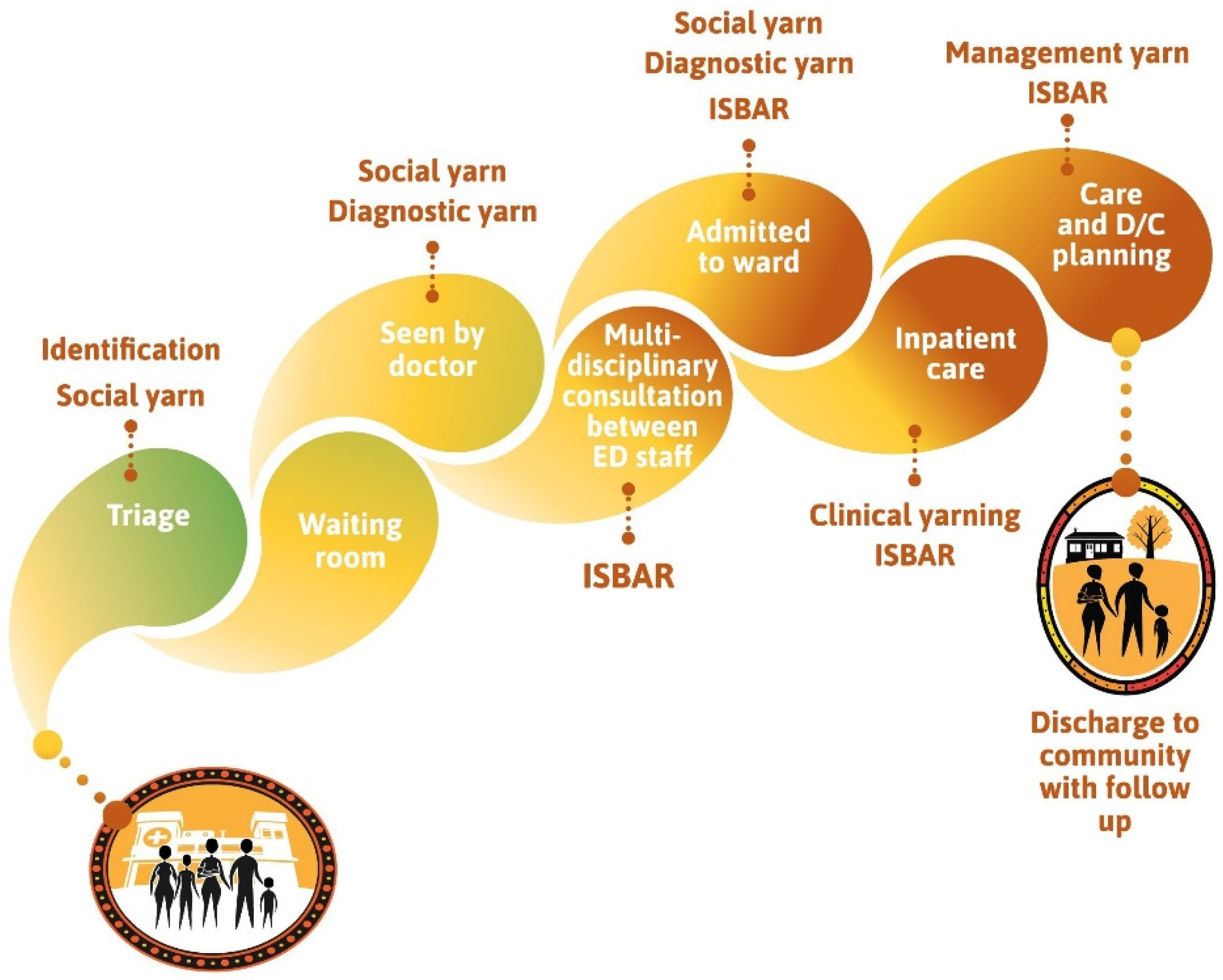
3.1. Thematic Diagram and a Culturally Safe Patient Journey
- The child is at the centre of care and grows up supported by community, family, and Elders (following [2]).
- The many outer contextual factors are depicted as “yellow balls’” and are inspired by the flowers of the Australian tree Acacia Jennerae.
- A ‘tree of life’ inspired by the trauma-informed perspective of the collective healing tree for Stolen Generations members and their descendants [64].
- Thematic nests from yarning groups such as family, community and Elders, reflecting the strengths in the cultural roots of life.
- The critical success factors (following [45]) of cultural safety are shown as building on a foundation of community engagement, strong Aboriginal cultures and safe health services.
3.2. Clinical Yarning
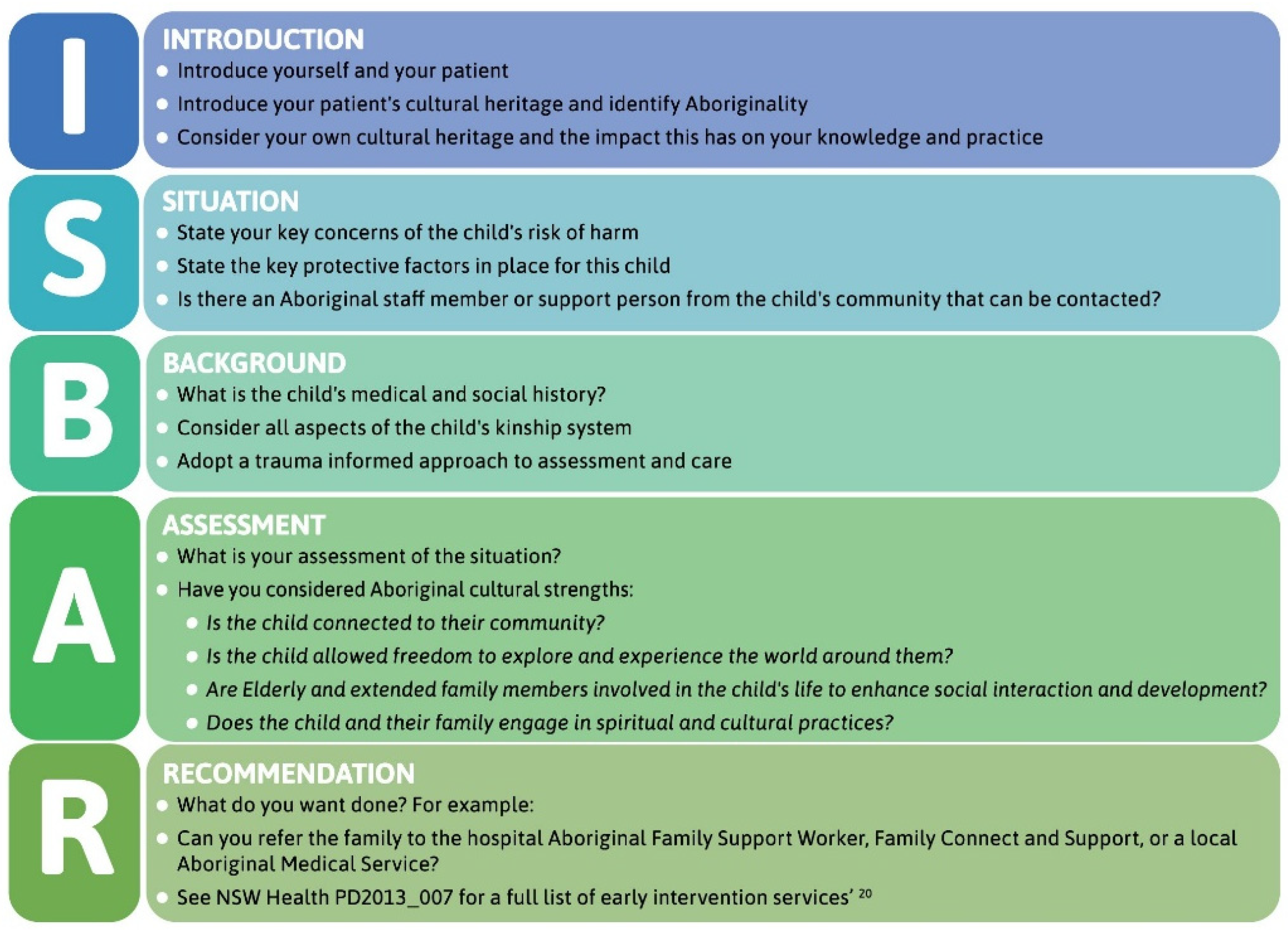
3.3. Culturally Adapted ISBAR
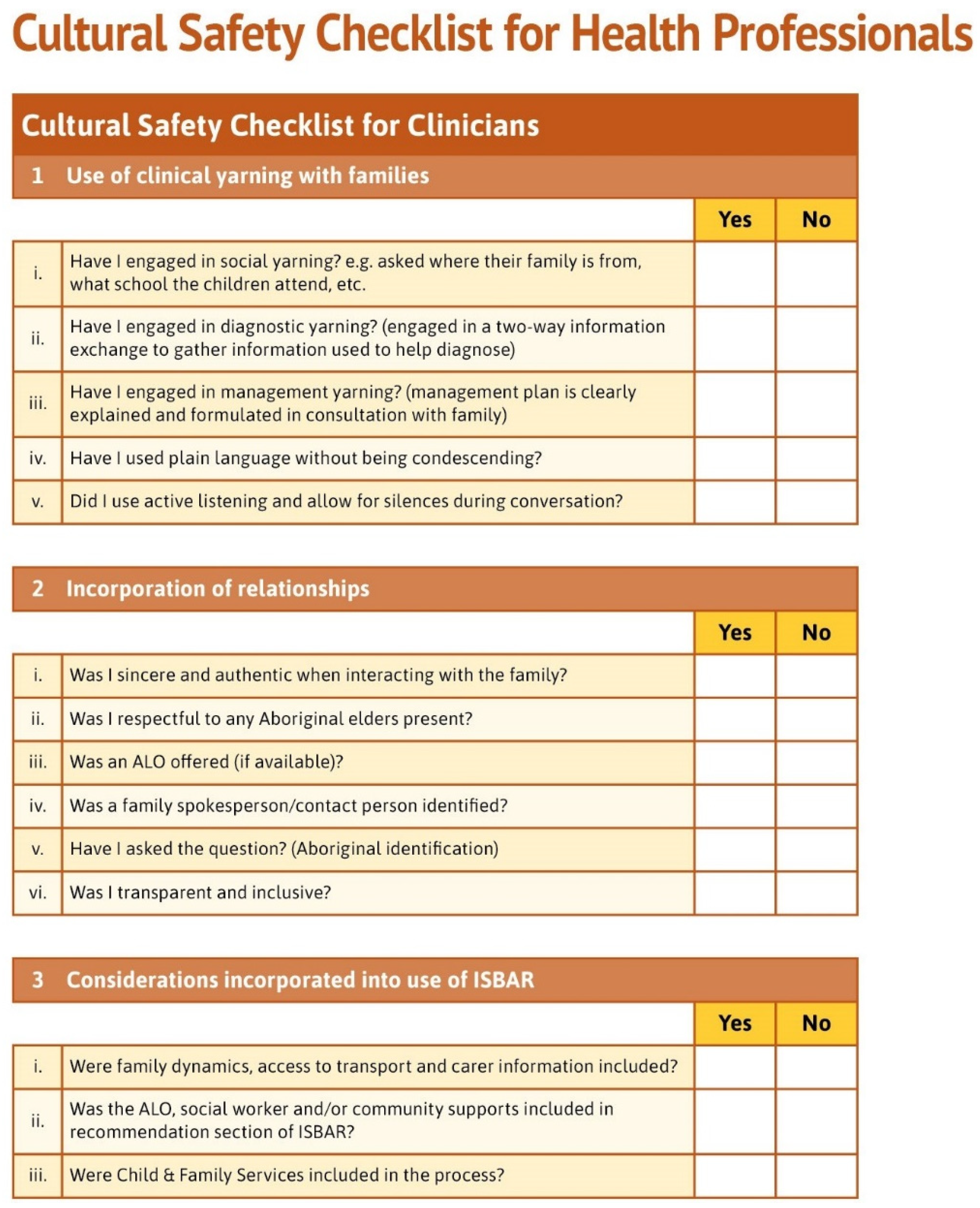
3.4. Cultural Safety Checklist for Clinicians
3.5. Clinical Utility Testing of the Model
4. Discussion
4.1. The Daalbirrwirr Gamambigu (Safe Children) Model of Care
4.2. Appropriate Governance and Cultural Engagement
4.3. A Culturally Safe Patient Journey
4.4. Clinical Yarning
4.5. Culturally Adapted ISBAR
4.6. Daalbirrwirr Gamambigu at the Intersection of Public Health and Child Protection
- can be embedded in health professional accreditation [105];
- can enhance culturally respectful and appropriate emergency department team skills [108];
- influence emergency department care [109];
- inform interdisciplinary approaches to child care [110];
- are a foundation for cultural training for health professionals [111];
- lead to the provision of care that is judged to be culturally safe [112]; and
- can help improve the effectiveness of communication with Australian Aboriginal families [113].
4.7. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- 1.
- Did the research respond to a need or priority determined by the community?
- Unmet need identified by research project steering committee. The Daalbirrwirr Gamambigu Project developed from the SAFE-ED project where the steering committee members recognised the unmet need of responding to Aboriginal children at risk of harm who presented to emergency departments.
- Testing relevance of idea with staff. JF and TF tested the relevance of this idea in discussions with Aboriginal and non-Aboriginal colleagues in the Mid North Coast Local Health District and the Sydney Children’s Hospital Network. JF and TF received affirmation that there was an unmet need in emergency department responses to Aboriginal children at risk of harm.
- Finding research funding. JF and TF investigated opportunities for a Medical Research Future Fund (MRFF) grant entitled “Embedding cultural safety in child protection policies for Aboriginal families in NSW paediatric care settings” with the formal support of the Director of Aboriginal Health (Mid North Coast Local Health District) and Executive Aboriginal Health Manager (Sydney Children’s Hospitals Network).
- Engaging with Aboriginal community in local areas. TF, a long-time community member in the local area, discussed the grant idea further with Aboriginal staff members, who provided TF with advice to contact Aboriginal community (not health staff), such as the Coffs Harbour Aboriginal Community Care Centre Inc. (known as Abcare) and the NSW Child, Family and Community Peak Aboriginal Corporation (AbSec). This engagement involved genuine contact between TF/CG and AbSec staff at many stages of the development of the Daalbirrwirr Gamambigu project. The project team are now finalising endorsement of the Framework and MoC with the AbSec CEO.
- Engaging with Aboriginal Researchers. TF and JF had established the project steering committee which included a number of Aboriginal advisors at the clinical, managerial and executive level from two Local Health Districts. Furthermore, the project team included three Aboriginal project officers at various stages of the project and Aboriginal members of the research team Associate Professor Donna Hartz, Dr Mark J Lock, and Dr Liesa Clague.
- Engaging with Aboriginal staff. The Aboriginal staff involved in the project are listed in an Appendix of the Framework and Model of Care documents are Clinton Gibbs, Joanne Shipp, Joseph Bryant, Robyn Martin, Amanda Ryan, Mick Scarcella, Jessica Morris, and Brenna Bernardino.
- Testing the idea with reference to policy, strategy, and research. There were numerous formal published sources of information where the needs of Aboriginal families and children were noted in regards to hospital care and child protection systems. The scoping literature review demonstrates the depth of investigation that the team went to so that the project aligned with the needs of Aboriginal families as described in the formal literature.
- Occurs within a broader policy context. The idea for the project occurred within an enabling policy context where the Mid North Coast Local Health District and the Sydney Children’s Hospital Network had strategies to Close the Gaps in Aboriginal health outcomes. These organisations operated in accord with NSW Government policy to reduce disadvantages experienced by Aboriginal people. In practice, an enabling organisational environment and policy context allows engagement and consultation activities to occur with Aboriginal people.
- 2.
- Was community consultation and engagement appropriately inclusive?
- The consultation diagram shows the key points of engagement with stakeholders appropriate to researching the intersection between healthcare and child protection systems.
- Project Staff are listed in the Framework and Model. There were two staff from the University of Sydney (lead academic organisation, one non-Aboriginal person and one Aboriginal person); five staff from the Mid North Coast Local Health District (sponsoring organisation, government health agency, four Aboriginal people and one non-Aboriginal person); three staff from the Sydney Children’s Hospitals Network (participating organisation, government health agency, one Aboriginal person and two non-Aboriginal people) and three independent staff, two Aboriginal and one non-Aboriginal. Of the ten project staff, seven were Aboriginal and three were non-Aboriginal peoples. Career spans show that six Aboriginal staff (CG, ML, LC, JS, JB, JM) combined had careers in Aboriginal affairs. Career spans for the two non-Aboriginal staff (JF and TF) were developed in paediatric/midwifery nursing practice, child protection and research, with a high awareness of Aboriginal peoples’ needs in healthcare.
- AbSec Conference Workshop Participants: There were over 50 participants in the workshop that took place in Coffs Harbour on Gumbaynggirr Country in November 2019. This was a culturally appropriate event because of the conference theme (Strong Communities Strong Kids), it was hosted by the AbSec (the NSW Child and Family Peak Aboriginal Corporation), and the conference provided participants with an opportunity to strengthen their skills and knowledge in supporting Aboriginal children, young people and families. The location (Coffs Harbour) was also the site of a sponsoring organisation (the Mid North Coast Local Health District); and the participants were Aboriginal stakeholders with professional and personal interests in the Daalbirrwirr Gamambigu project. The structure of the workshop was designed around circles of yarning, with three roundtable topics (clinical yarning, model of care, and ISBAR). The workshop comments and suggestions informed the implementation of the project.
- Sydney Children’s Hospital Network Staff (SCHN): There were nine staff from the SCHN, including the Chief Investigator (JF, non-Aboriginal), child protection unit director (SM, non-Aboriginal), executive medical director (MM, non-Aboriginal), staff specialist (DT, non-Aboriginal), diversity health coordinator (JC, non-Aboriginal), senior nursing research fellow (SSL, non-Aboriginal), director of nursing and midwifery education (SW, non-Aboriginal), director of clinical integration (MD, non-Aboriginal), and the Aboriginal health management advisor (MS, Aboriginal). Of the nine SCHN members, one is Aboriginal and ten are non-Aboriginal. Their roles and careers are in the fields of nursing, medicine, clinical, information technology, paediatrics, specialists, research, and management. The SCHN members were active in health and child protection areas.
- Aboriginal organisations. Five Aboriginal organisations participated in this project. The Aboriginal Health and Medical Research Council (AH and MRC, the peak advocacy body and Human Research Ethics Committee for Aboriginal community controlled health organisations in NSW); AbSec, the NSW Child and Family Peak Aboriginal Corporation (lead advocacy organisation for Aboriginal child protection in NSW); AbCare (Aboriginal Children/Young People in Out-of-Home-Care, Coffs Harbour, NSW) is the lead organisation in the Mid North Coast Local Health District that provides services for Aboriginal people in out-of-home-care to Aboriginal communities in Coffs Harbour, Bellingen and Clarence Valley areas, the Secretariat National Aboriginal; and Torres Strait Islander Child Care (SNAICC is the national peak body for Aboriginal child protection, of which AbSec is a member); the Congress of Aboriginal and Torres Strait Islander Nurses and Midwives (CATSINaM) is the national peak professional association for Aboriginal and Torres Strait Islander Nurses. These organisations represent Aboriginal communities and professionals in child protection and health care, from the local level (AbCare), to state level (AbSec, AH&MRC), to the national level (SNAICC, CATSINaM).
- 3.
- Did the research have Aboriginal and Torres Strait Islander research leadership?
- The research was not led by Aboriginal researchers. However, Aboriginal researchers were integral to its evolution and development through the governance committee, research assistance, research advice, and in technical aspects of the project such as ethics applications, yarning groups, interviews, conference presentations, data analysis, and writing (ML, LC, CG, JS, JB, MS).
- 4.
- Did the research have Aboriginal and Torres Strait Islander governance?
- The Daalbirrwirr Gamambigu project had a Steering Committee of 21 members representing the three stakeholder organisations: the University of Sydney, the Mid North Coast Local Health District, and the Sydney Children’s Hospital Network. The steering committee had Aboriginal (n = 6) and non-Aboriginal (n = 15) members and was chaired by a non-Aboriginal Executive chairperson.
- 5.
- Were local community protocols respected and followed?
- The protocols for local community engagement were learned through oral communication with Aboriginal people, as cultural authority is learned and understood through the developing of trusting relationships. In this project, the local communities were not only Australian Aboriginal communities but also the communities of practice established around child protection in healthcare settings. Some examples will explain. The Aboriginal staff of the MNCLHD (e.g., RM, AR, CG, JS, and JB) have 75 years of living and working with Aboriginal people throughout the Mid North Coast Local Health District. Key stakeholders in each of the Aboriginal organisations (SNAICC, AbSec, and AbCare) provided direction on community engagement within their respective networks to TF. The degree and extent of engagement, as aligned with local community protocols, was not systematically documented with respect to cultural protocols or yarning and oral knowledge transfer.
- 6.
- Did the researchers negotiate agreements in regards to rights of access to Aboriginal and Torres Strait Islander peoples’ existing intellectual and cultural property?
- This was not explicitly negotiated but will be considered in the evaluation phase.
- 7.
- Did the researchers negotiate agreements to protect Aboriginal and Torres Strait Islander peoples’ ownership of intellectual and cultural property created through the research?
- This was not explicitly negotiated.
- 8.
- Did Aboriginal and Torres Strait Islander peoples and communities have control over the collection and management of research materials?
- The data collection and materials are owned and managed by the University of Sydney, and stored in a secure digitally encrypted location. The control and management of these materials was overseen by the steering committee and administered by the research team. Data collection, analysis and publication was undertaken by Aboriginal and non-Aboriginal staff.
- 9.
- Was the research guided by an Australian Aboriginal research paradigm?
- The methodology was founded on the combination of the Wiradjuri developed Ngaa-bi-nya program evaluation framework and the Western i-PARIHS framework in keeping with the Australian ethic of cultural safety being a shared learning experience.
- The methodology was intersectional in acknowledgement of the cultural interface (following Nakata) between Aboriginal and Western world views as this is reflected in the empirical methodology of data collection such as the scoping literature review and yarning groups.
- The ethic of the project was founded on enabling cultural safety in every point and pathway of healthcare governance which is stated in the Mid North Coast Aboriginal Health Authority endorsed Aboriginal Cultural Safety and Security Framework.
- 10.
- Does the research take a strengths-based approach, acknowledging and moving beyond practices that have harmed Aboriginal and Torres Strait peoples in the past?
- The Daalbirrwirr Gamambigu project privileged the cultural strengths and cultural voices of Aboriginal peoples. This is evidenced in the philosophy informing the project (cultural safety), the methodology (Ngaa-bi-nya, i-PARIHS, Cultural Respect Framework for Aboriginal and Torres Strait Islander Health, and the Family Matters Roadmap), the consultation process which involved many Aboriginal people and Aboriginal organisations (who then formally endorsed the Daalbirrwirr Gamambigu materials), the governance committee, feedback to stakeholders and broader audiences, all aspects of the data analysis and writing, commissioning of the artwork from a local Aboriginal artist, and the use of an Aboriginal language through engagement with an Muurrbay Aboriginal Language and Culture Co-operative.
- 11.
- Did the researchers plan to and translate the findings into sustainable changes in policy and/or practice?
- The methodology, informed by both Ngaa-bi-nya and i-PARIHS, was directed towards translational research that benefits Aboriginal families and the professionals who work with them. The Daalbirrwirr Gamambigu Framework and Model will be cited in policy documents (e.g., NSW Aboriginal Health Plan) as direct evidence of cultural safety research. It will be referenced in peer reviewed journal articles in line with the need to produce a high quality evidence for policy and practice. It was developed into the training resources (the Framework and Model) after extensive stakeholder consultation and practitioner workshops. In 2022, the Daalbirrwirr Gamambigu Model will be trialled and evaluated in both the Sydney Children’s Hospital Network (metropolitan) and the Mid North Coast Local Health District (regional).
- 12.
- Did the research benefit the participants and Aboriginal and Torres Strait Islander communities?
- The benefit is formally demonstrated in the Aboriginal organisational endorsement of the Daalbirrwirr Gamambigu project. This endorsement underscores the determination of the research team to ensure meaningful consultation with Aboriginal stakeholders as a key way to determine if the benefit is seen by Aboriginal people.
- 13.
- Did the research demonstrate capacity strengthening for Aboriginal and Torres Strait Islander individuals?
- There were many Aboriginal people involved in this project from clinical experts, executive officers, project workers, researchers, staff members, and from Aboriginal community organisations. The strengthening is about participation in a formal research translation activity, paid employment as project officers, paid employment as researchers, inclusion in data analysis, inclusion in publications, and inclusion in conference and workshop activities. That is capacity building was evident in employment, research participation, formal publication, and communication and engagement activities. Three Aboriginal project officers employed across the project duration have since gone on to permanent roles in positions of seniority in government health organisations.
- 14.
- Did everyone involved in the research have opportunities to learn from each other?
- We learned from each other as members of the governance committee (how to translate research into practice and Aboriginal community benefit); in communication and engagement activities (workshop design and conduct); in data analysis and writing (collecting data, interpreting data, and writing in formal reports and journal articles); and in routine meetings between non-Aboriginal and Aboriginal researchers.
References
- Rasmussen, M.; Guo, X.; Wang, Y.; Lohmueller, K.E.; Rasmussen, S.; Albrechtsen, A.; Skotte, L.; Lindgreen, S.; Metspalu, M.; Jombart, T.; et al. An Aboriginal Australian genome reveals separate human dispersals into Asia. Science 2011, 334, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Lohoar, S.; Butera, N.; Kennedy, E. Strengths of Australian Aboriginal Cultural Practices in Family Life and Child Rearing; CFCA Paper No. 25; Australian Institute of Family Studies: Melbourne, Australia, 2014. [Google Scholar]
- Lohoar, S. Safe and Supportive Indigenous Families and Communities for Children. A Synopsis and Critique of Australian Research; Child Family Community Australia Paper No. 7; Australian Institute of Family Studies: Melbourne, Australia, 2012. [Google Scholar]
- Dockery, A.M. Inter-generational transmission of Indigenous culture and children’s wellbeing: Evidence from Australia. Int. J. Intercult. Rel. 2020, 74, 80–93. [Google Scholar] [CrossRef]
- Australian Health Practitioner Regulation Agency. Aboriginal and Torres Strait Islander Cultural Health and Safety Strategy 2020–2025; Australian Health Practitioner Regulation Agency: Canberra, Australia, 2020. [Google Scholar]
- Australian Human Rights and Equal Opportunity Commission. Bringing Them Home: Report of the National Inquiry into the Separation of Aboriginal and Torres Strait Islander Children from Their Families; Commonwealth of Australia: Sydney, Australia, 1997; p. 689. [Google Scholar]
- Higgins, I. Stolen Generations Study Reveals Impact of Intergenerational Trauma. Available online: https://www.abc.net.au/news/2018-08-15/stolen-generations-study-impact-of-intergenerational-trauma/10118132 (accessed on 2 February 2022).
- Davis, M. Family Is Culture, Final Report: Independent Review into Aboriginal Out-of-Home-Care in NSW; Family is Culture: Sydney, Australia, 2019. [Google Scholar]
- Cox, L. Fear, Trust and Aborigines: The Historical Experience of State Institutions and Current Encounters in the Health System. Health Hist. 2007, 9, 70–92. [Google Scholar] [CrossRef]
- Harnett, P.H.; Featherstone, G. The role of decision making in the over-representation of Aboriginal and Torres Strait Islander children in the Australian child protection system. Child Youth Serv. Rev. 2020, 113, 105019. [Google Scholar] [CrossRef]
- Webb, C.J.R.; Bywaters, P.; Elliott, M.; Scourfield, J. Income inequality and child welfare interventions in England and Wales. J. Epidemiol. Community Health 2021, 75, 251–257. [Google Scholar] [CrossRef]
- Maguire-Jack, K.; Lanier, P.; Johnson-Motoyama, M.; Welch, H.; Dineen, M. Geographic variation in racial disparities in child maltreatment: The influence of county poverty and population density. Child Abus. Negl. 2015, 47, 1–13. [Google Scholar] [CrossRef]
- Gilbert, R.; Widom, C.S.; Browne, K.; Fergusson, D.; Webb, E.; Janson, S. Burden and consequences of child maltreatment in high-income countries. Lancet 2009, 373, 68–81. [Google Scholar] [CrossRef]
- Hyslop, I.K. Child Protection Reform in Aotearoa-New Zealand: Devolution or Revolution? Int. J. Child Maltreat. 2021, 4, 439–454. [Google Scholar] [CrossRef]
- Dettlaff, A.J. Racial Disproportionality and Disparities in the Child Welfare System, 1st ed.; Springer Nature: Cham, Switzerland, 2021. [Google Scholar]
- Herrenkohl, T.I.; Lonne, B.; Higgins, D.; Scott, D. The Personal Security of Children Demands Bold System Reform. Int. J. Child Maltreat. 2020, 3, 9–17. [Google Scholar] [CrossRef]
- Cross, T.L. Racial Disproportionality and Disparities Among American Indian and Alaska Native Populations. In Racial Disproportionality and Disparities in the Child Welfare System. Child Maltreatment (Contemporary Issues in Research and Policy); Dettlaff, A.J., Ed.; Springer: Cham, Switzerland, 2021; Volume 11, pp. 99–124. [Google Scholar]
- Duthie, D.; Steinhauer, S.; Twinn, C.; Steinhauer, V.; Lonne, B. Understanding Trauma and Child Maltreatment Experienced in Indigenous Communities. In Re-Visioning Public Health Approaches for Protecting Children; Lonne, B., Scott, D., Higgins, D., Herrenkohl, T., Eds.; Springer Publishers: New York, NY, USA, 2019; pp. 327–348. [Google Scholar]
- Lonne, B.; Russ, E.; Harrison, C.; Morley, L.; Harries, M.; Robertson, S.; Pearce, T.; Smith, J. The “Front Door” to Child Protection—Issues and Innovations. Int. J. Child Maltreat. 2021, 3, 351–367. [Google Scholar] [CrossRef]
- Lonne, B.; Scott, D.; Higgins, D.; Herrenkohl, T. (Eds.) Re-Visioning Public Health Approaches for Protecting Children; Springer Publishers: New York, NY, USA, 2019. [Google Scholar]
- Katz, I.; Cortis, N.; Shlonsky, A.; Mildon, R. Modernising Child Protection in New Zealand: Learning from System Reforms in Other Jurisdictions (SPRC Report to Follow/2015); Social Policy Research Centre, UNSW Australia: Sydney, Australia, 2015. [Google Scholar]
- Australian Institute of Health and Welfare. Child Protection Australia 2019–20; Child Welfare Series No. 74. Cat. No. CWS 78; Australian Institute of Health and Welfare: Canberra, Australia, 2021. [Google Scholar]
- SCRGSP (Steering Committee for the Review of Government Service Provision). Report on Government Services 2019; SCRGSP: Canberra, Australia, 2019. [Google Scholar]
- Australian Institute of Health and Welfare. Indigenous Child Safety; Cat. No. IHW 127; Australian Institute of Health and Welfare: Canberra, Australia, 2014. [Google Scholar]
- Snow, P.; McLean, E.; Frederico, M. The language, literacy and mental health profiles of adolescents in out-of-home care: An Australian sample. Child Lang. Teach. Ther. 2020, 36, 151–163. [Google Scholar] [CrossRef]
- Madelaine, S.; Melissa, S.; Heather, M.; Lauren, B.; Helen, S.; Rachael, G. “Surviving not thriving”: Experiences of health among young people with a lived experience in out-of-home care. Int. J. Adolesc. Youth 2020, 25, 809–823. [Google Scholar] [CrossRef]
- Raman, S.; Ruston, S.; Irwin, S.; Tran, P.; Hotton, P.; Thorne, S. Taking culture seriously: Can we improve the developmental health and well-being of Australian Aboriginal children in out-of-home care? Child Care Health Dev. 2017, 43, 899–905. [Google Scholar] [CrossRef] [PubMed]
- Moss, P.; O’Callaghan, R.; Fisher, A.; Kennedy, C.; Tracey, F. Navigate Your Health: A Case Study of Organisational Learnings from an Integrated Care Pilot for Children and Young People in Care. Int. J. Integr. Care 2021, 21, 4. [Google Scholar] [CrossRef] [PubMed]
- Shmerling, E.; Creati, M.; Belfrage, M.; Hedges, S. The health needs of Aboriginal and Torres Strait Islander children in out-of-home care. J. Paediatr. Child Health 2019, 56, 384–388. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Data Tables: Child Protection Australia 2019–20; Child Welfare Series No. 74. Cat No. CWS 78; Australian Institute of Health and Welfare: Canberra, Australia, 2021. [Google Scholar]
- He, V.Y.; Guthridge, S.; Su, J.-Y.; Howard, D.; Stothers, K.; Leach, A. The link between hearing impairment and child maltreatment among Aboriginal children in the Northern Territory of Australia: Is there an opportunity for a public health approach in child protection? BMC Public Health 2020, 20, 449. [Google Scholar] [CrossRef]
- Tanner, L.; Agius, K.; Darbyshire, P. ‘Sometime they run away, that’s how scared they feel’: The paediatric hospitalisation experiences of Indigenous families from remote areas of Australia. Contemp. Nurse 2004, 18, 3–17. [Google Scholar] [CrossRef]
- Flemington, T.; Lock, M.; Shipp, J.; Hartz, D.; Lonne, B.; Fraser, J.A. Cultural Safety and Child Protection Responses in Hospitals: A Scoping Review. Int. J. Child Maltreat. 2021, 4, 5–33. [Google Scholar] [CrossRef]
- Zon, A.; Lindeman, M.; Williams, A.; Hayes, C.; Ross, D.; Furber, M. Cultural safety in child protection: Application to the workplace environment and casework practice. Aust. Soc. Work 2004, 57, 288–298. [Google Scholar] [CrossRef]
- McAuliffe, D.; Tilbury, C.; Chenoweth, L.; Stehlik, D.; Struthers, K.; Aitchison, R. (Re)Valuing Relationships in Child Protection Practice. J. Soc. Work Pract. 2016, 30, 365–377. [Google Scholar] [CrossRef]
- Chamberlain, C.R.; MacLean, S.; Bawden, G.; Kelaher, M.; Munro-Harrison, E.; Boyle, J.; Freeman, K. An ‘equity’ domain could strengthen the utility of a framework for assessing care coordination for Australian Aboriginal families. Int. J. Care Coord. 2016, 19, 42–46. [Google Scholar] [CrossRef]
- Otim, M.; Anderson, I.; Renhard, R. Aboriginal and Torres Strait Islander Hospital Accreditation Project: A Literature Review; Discussion Paper No. 9; Koori Health Research and Community Development Unit: Melbourne, Australia, 2002. [Google Scholar]
- Chapman, R.; Martin, C.; Smith, T. Evaluation of staff cultural awareness before and after attending cultural awareness training in an Australian emergency department. Int. Emerg. Nurs. 2014, 22, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Hunter, S.-A.; Burton, J.; Blacklaws, G.; Soltysik, A.; Mastroianni, A.; Young, J.; Jones, M.; Jayakody, N.; Bhathal, A.; Krakouer, J.; et al. The Family Matters Report 2020: Measuring Trends to Turn the Tide on the Over-Representation of Aboriginal and Torres Strait Islander Children in Out-Of-Home Care in Australia; Secretariat National Aboriginal and Torres Strait Islander Child Care: Collingwood, Australia, 2020. [Google Scholar]
- ABS. Estimates of Aboriginal and Torres Strait Islander Australians, June 2016; Australian Bureau of Statistics: Canberra, Australia, 2018. [Google Scholar]
- Sydney Children’s Hospital Network. ‘Over Our Tracks’: Sydney Children’s Hospital Network Aboriginal Health Strategic Plan 2018-2021; Sydney Children’s Hospital Network: Sydney, NSW, Australia, 2018. [Google Scholar]
- National Health and Medical Research Council. Ethical Conduct in Research with Aboriginal and Torres Strait Islander Peoples and Communities: Guidelines for Researchers and Stakeholders; National Health and Medical Research Council: Canberra, Australia, 2018. [Google Scholar]
- Aboriginal Health and Medical Research Council of NSW Ethics Committee. AH&MRC Guidelines for Research into Aboriginal Health: Key Principles; Aboriginal Health and Medical Research Council of NSW Ethics Committee: Sydney, Australia, 2016. [Google Scholar]
- Australian Health Ministers’ Advisory Council. Cultural Respect Framework for Aboriginal and Torres Strait Islander Health, 2016–2026; Australian Health Ministers’ Advisory Council: Canberra, Australia, 2016. [Google Scholar]
- Williams, M. Ngaa-bi-nya Aboriginal and Torres Strait Islander program evaluation framework. Eval. J. Australas. 2018, 18, 6–20. [Google Scholar] [CrossRef]
- Harvey, G.; Kitson, A. PARIHS revisited: From heuristic to integrated framework for the successful implementation of knowledge into practice. Implement. Sci. IS 2016, 11, 33. [Google Scholar] [CrossRef]
- Williams, R. Cultural safety—What does it mean for our work practice? Aust. N. Z. J. Public Health 1999, 23, 213–214. [Google Scholar] [CrossRef]
- Bin-Sallik, M. Cultural Safety: Let’s Name It! Aust. J. Indig. Educ. 2003, 32, 21–28. [Google Scholar] [CrossRef]
- Nakata, M. The Cultural Interface. Aust. J. Indig. Educ. 2007, 36, 7–14. [Google Scholar] [CrossRef]
- Ryder, C.; Mackean, T.; Coombs, J.; Williams, H.; Hunter, K.; Holland, A.J.A.; Ivers, R.Q. Indigenous research methodology—Weaving a research interface. Int. J. Soc. Res. Methodol. 2019, 23:3, 255–267. [Google Scholar] [CrossRef]
- Salmon, M.; Doery, K.; Dance, P.; Chapman, J.; Gilbert, R.; Williams, R.; Lovett, R. Defining the Indefinable: Descriptors of Aboriginal and Torres Strait Islander Peoples’ Cultures and Their Links to Health and Wellbeing; Lowitja Institute: Carlton South, Australia, 2018. [Google Scholar]
- Gwynn, J.; Lock, M.; Turner, N.; Dennison, R.; Coleman, C.; Kelly, B.; Wiggers, J. Aboriginal and Torres Strait Islander community governance of health research: Turning principles into practice. Aust. J. Rural. Health 2015, 23, 235–242. [Google Scholar] [CrossRef]
- Liaw, S.T.; Wade, V.; Furler, J.S.; Hasan, I.; Lau, P.; Kelaher, M.; Xuan, W.; Harris, M.F. Cultural respect in general practice: A cluster randomised controlled trial. Med. J. Aust. 2019, 210, 263–268. [Google Scholar] [CrossRef]
- National Health and Medical Research Council. Cultural Competency in Health: A Guide for Policy, Partnerships and Participation; National Health and Medical Research Council: Canberra, Australia, 2005. [Google Scholar]
- Hickey, S.; Kildea, S.; Couchman, K.; Watego-Ivory, K.; West, R.; Kruske, S.; Blackman, R.; Watego, S.; Roe, Y.L. Establishing teams aiming to provide culturally safe maternity care for Indigenous families. Women Birth J. Aust. Coll. Midwives 2019, 32:5, 449–459. [Google Scholar] [CrossRef] [PubMed]
- Chamberlain, C.; Gee, G.; Stephanie Janne, B.; Atkinson, J.; Herrman, H.; Gartland, D.; Glover, K.; Clark, Y.; Campbell, S.; Mensah, F.K.; et al. Healing the Past by Nurturing the Future—Co-designing perinatal strategies for Aboriginal and Torres Strait Islander parents experiencing complex trauma: Framework and protocol for a community-based participatory action research study. BMJ Open 2019, 9, e028397. [Google Scholar] [CrossRef] [PubMed]
- AbSec. NSW Aboriginal Child & Family Conference 2019, Conference Report; NSW Child, Family and Community Peak Aboriginal Corporation: Sydney, Australia, 2019. [Google Scholar]
- Fleming, T.; Creedy, D.K.; West, R. The influence of yarning circles: A cultural safety professional development program for midwives. Women Birth 2020, 33, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Rheault, H.; Coyer, F.; Bonner, A. Time to listen: Chronic disease yarning with Aboriginal and Torres Strait Islander peoples living in remote Australia. Collegian 2020, 28, 10–17. [Google Scholar] [CrossRef]
- Gainsford, A.; Robertson, S. Yarning shares knowledge: Wiradyuri storytelling, cultural immersion and video reflection. Law Teach. 2019, 53, 500–512. [Google Scholar] [CrossRef]
- Bessarab, D.; Ng’andu, B. Yarning about yarning as a legitimate method in Indigenous research. Int. J. Crit. Indig. Stud. 2010, 3, 37–50. [Google Scholar] [CrossRef]
- Haynes, M.; O’Rourke, T.; Nash, D.; Baffour, B.; York, S.; Chainey, C.; Betros, G.; Memmott, P. Aboriginal and Torres Strait Islander preferences for healthcare settings: Effective use of design images in survey research. Aust. Health Rev. 2020, 44, 222–227. [Google Scholar] [CrossRef]
- NSW Ministry of Health. Policy Directive—Emergency Department Patients Awaiting Care; NSW Ministry of Health: Sydney, Australia, 2018. [Google Scholar]
- Blignault, I.; Jackson Pulver, L.; Fitzpatrick, S.; Arkles, R.; Williams, M.; Haswell, M.; Grand Ortega, M.; Muru Marri Consultancy Team. A Resource for Collective Healing for Members of the Stolen Generations. Planning, Implementing, and Evaluating Effective Local Responses; Aboriginal and Torres Strait Islander Healing Foundation: Canberra, Australia, 2014. [Google Scholar]
- Lin, I.; Green, C.; Bessarab, D. ‘Yarn with me’: Applying clinical yarning to improve clinician-patient communication in Aboriginal health care. Aust. J. Prim. Health 2016, 22, 377–382. [Google Scholar] [CrossRef]
- Pakcheshm, B.; Bagheri, I.; Kalani, Z. The impact of using “ISBAR” standard checklist on nursing clinical handoff in coronary care units. Nurs. Pract. Today 2020, 7, 266–274. [Google Scholar] [CrossRef]
- Johnson-Motoyama, M.; Ginther, D.K.; Phillips, R.; Beer, O.W.J.; Merkel-Holguin, L.; Fluke, J. Differential Response and the Reduction of Child Maltreatment and Foster Care Services Utilization in the U.S. from 2004 to 2017. Child Maltreat. 2022, 21, 10775595211065761. [Google Scholar] [CrossRef]
- SNAICC. Pathways to Safety and Wellbeing for Aboriginal and Torres Strait Islander Children; Secretariat National Aboriginal and Torres Strait Islander Child Care: Collingwood, Australia, 2015. [Google Scholar]
- Cresp, R.; Clarke, K.; McAuley, K.E.; McAullay, D.; Moylan, C.A.; Peter, S.; Chaney, G.M.; Cook, A.; Edmond, K.M. Effectiveness of the Koorliny Moort out-of-hospital health care program for Aboriginal and Torres Strait Islander children in Western Australia. Med. J. Aust. 2016, 204, 1971e–1977. [Google Scholar] [CrossRef] [PubMed]
- Knoche, D.; Clarke, A.; Shanahan, N.; Rowley, K. ‘Treating Us Right’: A Summary Report Describing and Evaluating Wadja’s New Model of Care for Aboriginal Children and Families at The Royal Children’s Hospital; Onemda VicHealth Koori Health Unit: Melbourne, Australia, 2012. [Google Scholar]
- Berndt, R.M.; Tonkinson, R. Australian Aboriginal Peoples. Available online: https://www.britannica.com/topic/Australian-Aboriginal (accessed on 31 January 2022).
- Harfield, S.; Pearson, O.; Morey, K.; Kite, E.; Canuto, K.; Glover, K.; Gomersall, J.S.; Carter, D.; Davy, C.; Aromataris, E.; et al. Assessing the quality of health research from an Indigenous perspective: The Aboriginal and Torres Strait Islander quality appraisal tool. BMC Med. Res. Methodol. 2020, 20, 79. [Google Scholar] [CrossRef] [PubMed]
- Lock, M.J.; Walker, T.; Browne, J. Promoting cultural rigour through critical appraisal tools in First Nations peoples’ research. Aust. N. Z. J. Public Health 2021, 45, 210–211. [Google Scholar] [CrossRef] [PubMed]
- National Ethics Advisory Committee. National Ethical Standards Health and Disability Research and Quality Improvement; National Ethics Advisory Committee: Wellington, New Zealand, 2019. [Google Scholar]
- Schelbe, L.; Wilson, D.L.; Fickler, W.; Williams-Mbengue, N.; Klika, J.B. Bridging the Gaps Among Research, Policy, and Practice in the Field of Child Maltreatment Through Cross-Sector Training and Innovation. Int. J. Child Maltreatment Res. Policy Pract. 2020, 3, 293–305. [Google Scholar] [CrossRef]
- Doran, F.; Wrigley, B.; Lewis, S. Exploring cultural safety with Nurse Academics. Research findings suggest time to “step up”. Contemp. Nurse 2019, 55, 156–170. [Google Scholar] [CrossRef]
- Curtis, E.; Jones, R.; Tipene-Leach, D.; Walker, C.; Loring, B.; Paine, S.-J.; Reid, P. Why cultural safety rather than cultural competency is required to achieve health equity: A literature review and recommended definition. Int. J. Equity Health 2019, 18, 174. [Google Scholar] [CrossRef]
- Kerrigan, V.; Lewis, N.; Cass, A.; Hefler, M.; Ralph, A.P. „How can I do more?” Cultural awareness training for hospital-based healthcare providers working with high Aboriginal caseload. BMC Med. Educ. 2020, 20, 173. [Google Scholar] [CrossRef]
- Funston, L.; Herring, S.; ACMAG. When Will the Stolen Generations End? A Qualitative Critical Exploration of Contemporary ‘Child Protection’ Practices in Aboriginal and Torres Strait Islander Communities. Sex. Abus. Aust. N. Z. 2016, 7, 51–58. [Google Scholar]
- Sheehan, N.W. Indigenous knowledge and respectful design: An evidence-based approach. Des. Issues 2011, 27, 68–80. [Google Scholar] [CrossRef]
- Kowal, E. Time, indigeneity and white anti-racism in Australia. Aust. J. Anthropol. 2015, 26, 94–111. [Google Scholar] [CrossRef]
- Herring, S.; Spangaro, J.; Lauw, M.; McNamara, L. The Intersection of Trauma, Racism, and Cultural Competence in Effective Work with Aboriginal People: Waiting for Trust. Aust. Soc. Work. 2013, 66, 104–117. [Google Scholar] [CrossRef]
- Frederico, M.; Jackson, A.; Black, C.; Pawsey, R.; Cox, A. Take Two—Implementing a Therapeutic Service for Children who have Experienced Abuse and Neglect: Beyond Evidence-Informed Practice. Child Abuse Rev. 2019, 28, 225–239. [Google Scholar] [CrossRef]
- Daws, K.; Punch, A.; Winters, M.; Posenelli, S.; Willis, J.; MacIsaac, A.; Rahman, M.A.; Worrall-Carter, L. Implementing a working together model for Aboriginal patients with acute coronary syndrome: An Aboriginal Hospital Liaison Officer and a specialist cardiac nurse working together to improve hospital care. Aust. Health Rev. Publ. Aust. Hosp. Assoc. 2014, 38, 552–556. [Google Scholar] [CrossRef]
- Agar, M. Institutional discourse. Text-Interdiscip. J. Study Discourse 1985, 5, 147–168. [Google Scholar] [CrossRef]
- Laverty, M.; McDermott, D.R.; Calma, T. Embedding cultural safety in Australia’s main health care standards. Med. J. Aust. 2017, 207, 15–16. [Google Scholar] [CrossRef] [PubMed]
- Lock, M.J.; Hartz, D.; Martin, R.; Ryan, A.; Curry, R.; Hart, S. An Aboriginal Cultural Safety and Security Framework: Improving Aboriginal Health Outcomes through Culturally Safe and Secure Mainstream Healthcare Governance and Practice; Mid North Coast Local Health District and the Mid North Coast Aboriginal Health Authority: Port Macquarie, Australia, 2019; p. 255. [Google Scholar]
- Bowes, J.; Grace, R. Review of Early Childhood Parenting, Education and Health Intervention Programs for Indigenous Children and Families in Australia; Issues Paper No. 8 Produced for the Closing the Gap Clearinghouse; Australian Institute of Health and Welfare: Canberra, Australia, 2014. [Google Scholar]
- Jennings, W.; Bond, C.; Hill, P.S. The power of talk and power in talk: A systematic review of Indigenous narratives of culturally safe healthcare communication. Aust. J. Prim. Health 2018, 24, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Minnican, C.; O’Toole, G. Exploring the incidence of culturally responsive communication in Australian healthcare: The first rapid review on this concept. BMC Health Serv. Res. 2020, 20, 20. [Google Scholar] [CrossRef]
- Morgan, D.J.R.; Gidgup, R.; Harris, T.; Whitely, M. Identifying the cultural heritage of patients during clinical handover and in hospital medical records. Med. J. Aust. 2019, 210, 220–226. [Google Scholar] [CrossRef]
- Brough, M.; Shannon, C.; Haswell-Elkins, M. To be or not to be: Recording Aboriginal identity on hospital records. Pac. Health Dialog. 2001, 8, 47–53. [Google Scholar]
- Churchill, M.E.; Smylie, J.K.; Wolfe, S.H.; Bourgeois, C.; Moeller, H.; Firestone, M. Conceptualising cultural safety at an Indigenous-focused midwifery practice in Toronto, Canada: Qualitative interviews with Indigenous and non-Indigenous clients. BMJ Open 2020, 10, e038168. [Google Scholar] [CrossRef]
- Byrne, H.; Cirillo, A.; Murphy-Gelderman, W.; Petrucci, D.; Gamondele, N.; Zafran, H. Stories of Pediatric Rehabilitation Practitioners within Indigenous Communities A Guide to Becoming Culturally Safer; McGill University: Montréal, QC, Canada, 2020. [Google Scholar]
- Coombes, J.; Fraser, S.; Hunter, K.; Ivers, R.; Holland, A.; Grant, J.; Mackean, T. “They Are Worth Their Weight in Gold”: Families and Clinicians’ Perspectives on the Role of First Nations Health Workers in Paediatric Burn Care in Australia. Int. J. Environ. Res. Public Health 2021, 18, 2297. [Google Scholar] [CrossRef] [PubMed]
- Mercer, C.; Byrth, J.; Jordan, Z. The experiences of Aboriginal health workers and non-Aboriginal health professionals working collaboratively in the delivery of health care to Aboriginal Australians: A systematic review. JBI Database Syst. Rev. Implement. Rep. 2014, 12, 234–418. [Google Scholar] [CrossRef]
- Gee, G.; Sheridan, S.; Charles, L.; Dayne, L.; Joyce, L.; Stevens, J.; Paradies, Y.; Hulbert, C.; Haslam, N.; Thorpe, R.; et al. The Her Tribe and His Tribe Aboriginal-Designed Empowerment Programs. Int. J. Environ. Res. Public Health 2022, 19, 2381. [Google Scholar] [CrossRef] [PubMed]
- Nyanga, R.; Biviano, L.; Warren, S.; Windsor, J.; Zwi, K.; Gunasekera, H. Aboriginal and Torres Strait Islander health-care delivery: The views of health-care professionals in Sydney’s tertiary paediatric hospitals. J. Paediatr. Child Health 2018, 54, 1023–1030. [Google Scholar] [CrossRef] [PubMed]
- NSW Ministry of Health. Policy Directive—Respecting the Difference: An Aboriginal Cultural Training Framework for NSW Health; NSW Ministry of Health: Sydney, Australia, 2011. [Google Scholar]
- Australian Government Department of Social Services. Fourth Action Plan 2018–2020. Supporting Families, Communities and Organisations to Keep Children safe. National Framework for Protecting Australia’s Children 2009–2020; Commonwealth of Australia: Canberra, Australia, 2018. [Google Scholar]
- AIHW (Australian Institute of Health and Welfare). The Aboriginal and Torres Strait Islander Child Placement Principle Indicators 2018–19: Measuring Progress; Cat. No. CWS 77; Australian Institute of Health and Welfare: Canberra, Australia, 2020. [Google Scholar]
- Joint Council on Closing the Gap. National Agreement on Closing the Gap, July 2020; Australian Government: Canberra, Australia, 2020. [Google Scholar]
- Napier, A.D.; Ancarno, C.; Butler, B.; Calabrese, J.; Chater, A.; Chatterjee, H.; Guesnet, F.; Horne, R.; Jacyna, S.; Jadhav, S.; et al. Culture and health. Lancet 2014, 384, 1607–1639. [Google Scholar] [CrossRef]
- Garvey, G.; Anderson, K.; Gall, A.; Butler, T.L.; Whop, L.J.; Arley, B.; Cunningham, J.; Dickson, M.; Cass, A.; Ratcliffe, J.; et al. The Fabric of Aboriginal and Torres Strait Islander Wellbeing: A Conceptual Model. Int. J. Environ. Res. Public Health 2021, 18, 7745. [Google Scholar] [CrossRef]
- Milligan, E.; West, R.; Saunders, V.; Bialocerkowski, A.; Creedy, D.; Rowe Minniss, F.; Hall, K.; Vervoort, S. Achieving cultural safety for Australia’s First Peoples: A review of the Australian Health Practitioner Regulation Agency-registered health practitioners’ Codes of Conduct and Codes of Ethics. Aust. Health Rev. 2021, 45, 398–406. [Google Scholar] [CrossRef]
- Australian Human Rights Commission. National Principles for Child Safe Organisations; Australian Human Rights Commission: Sydney, Australia, 2018. [Google Scholar]
- Office of the Children’s Guardian. Principles for Child-Safe Organisations; Office of the Children’s Guardian, NSW Government: Sydney, Australia, 2017. [Google Scholar]
- Australasian College for Emergency Medicine. Quality Standards for Emergency Departments and other Hospital-Based Emergency Care Services, 1st ed.; Australasian College for Emergency Medicine: Melbourne, Australia, 2015. [Google Scholar]
- Australasian College for Emergency Medicine. Aboriginal and Torres Strait Islander and Non-Indigenous Presentations to Australian Emergency Departments—AIHW ED Presentation 2014–2015; Australasian College for Emergency Medicine: Melbourne, Australia, 2018. [Google Scholar]
- Australasian College for Emergency Medicine. Policy on Child at Risk; Australasian College for Emergency Medicine: Melbourne, Australia, 2019. [Google Scholar]
- Australian College of Rural and Remote Medicine. Advanced Specialised Training Aboriginal and Torres Strait Islander Health Curriculum; Australian College of Rural and Remote Medicine: Brisbane, Australia, 2016. [Google Scholar]
- Australian College of Children & Young People’s Nurses. Standards of Practice for Children and Young People’s Nurses; Australian College of Children & Young People’s Nurses: Wynnum, Australia, 2016. [Google Scholar]
- The Wardliparingga Aboriginal Research Unit of the South Australian Health and Medical Research Institute. National Safety and Quality Health Service Standards User Guide for Aboriginal and Torres Strait Islander Health; The Wardliparingga Aboriginal Research Unit of the South Australian Health and Medical Research Institute: Sydney, Australia, 2017. [Google Scholar]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flemington, T.; Fraser, J.; Gibbs, C.; Shipp, J.; Bryant, J.; Ryan, A.; Wijetilaka, D.; Marks, S.; Scarcella, M.; Tzioumi, D.; et al. The Daalbirrwirr Gamambigu (Safe Children) Model: Embedding Cultural Safety in Child Protection Responses for Australian Aboriginal Children in Hospital Settings. Int. J. Environ. Res. Public Health 2022, 19, 5381. https://doi.org/10.3390/ijerph19095381
Flemington T, Fraser J, Gibbs C, Shipp J, Bryant J, Ryan A, Wijetilaka D, Marks S, Scarcella M, Tzioumi D, et al. The Daalbirrwirr Gamambigu (Safe Children) Model: Embedding Cultural Safety in Child Protection Responses for Australian Aboriginal Children in Hospital Settings. International Journal of Environmental Research and Public Health. 2022; 19(9):5381. https://doi.org/10.3390/ijerph19095381
Chicago/Turabian StyleFlemington, Tara, Jennifer Fraser, Clinton Gibbs, Joanne Shipp, Joe Bryant, Amanda Ryan, Devika Wijetilaka, Susan Marks, Mick Scarcella, Dimitra Tzioumi, and et al. 2022. "The Daalbirrwirr Gamambigu (Safe Children) Model: Embedding Cultural Safety in Child Protection Responses for Australian Aboriginal Children in Hospital Settings" International Journal of Environmental Research and Public Health 19, no. 9: 5381. https://doi.org/10.3390/ijerph19095381
APA StyleFlemington, T., Fraser, J., Gibbs, C., Shipp, J., Bryant, J., Ryan, A., Wijetilaka, D., Marks, S., Scarcella, M., Tzioumi, D., Ramanathan, S., Clague, L., Hartz, D., Lonne, B., & Lock, M. (2022). The Daalbirrwirr Gamambigu (Safe Children) Model: Embedding Cultural Safety in Child Protection Responses for Australian Aboriginal Children in Hospital Settings. International Journal of Environmental Research and Public Health, 19(9), 5381. https://doi.org/10.3390/ijerph19095381