
Priority Analysis of Educational Needs of Forest Healing Instructors Related to Programs for Cancer Survivors: Using Borich Needs Assessment and the Locus for Focus Model



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Ethical Approval
2.3. Measures and Data Collection
2.3.1. Questionnaire
2.3.2. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Forest Healing Instructors’ Knowledge Level and Perceived Importance of Forest Healing Programs for Cancer Survivors
3.3. Differences in Knowledge Level and Perceived Importance of Cancer Survivors according to General Characteristics of Forest Healing Instructors
3.4. Borich Needs Assessment Analysis of Educational Needs for Forest Healing Programs for Cancer Survivors
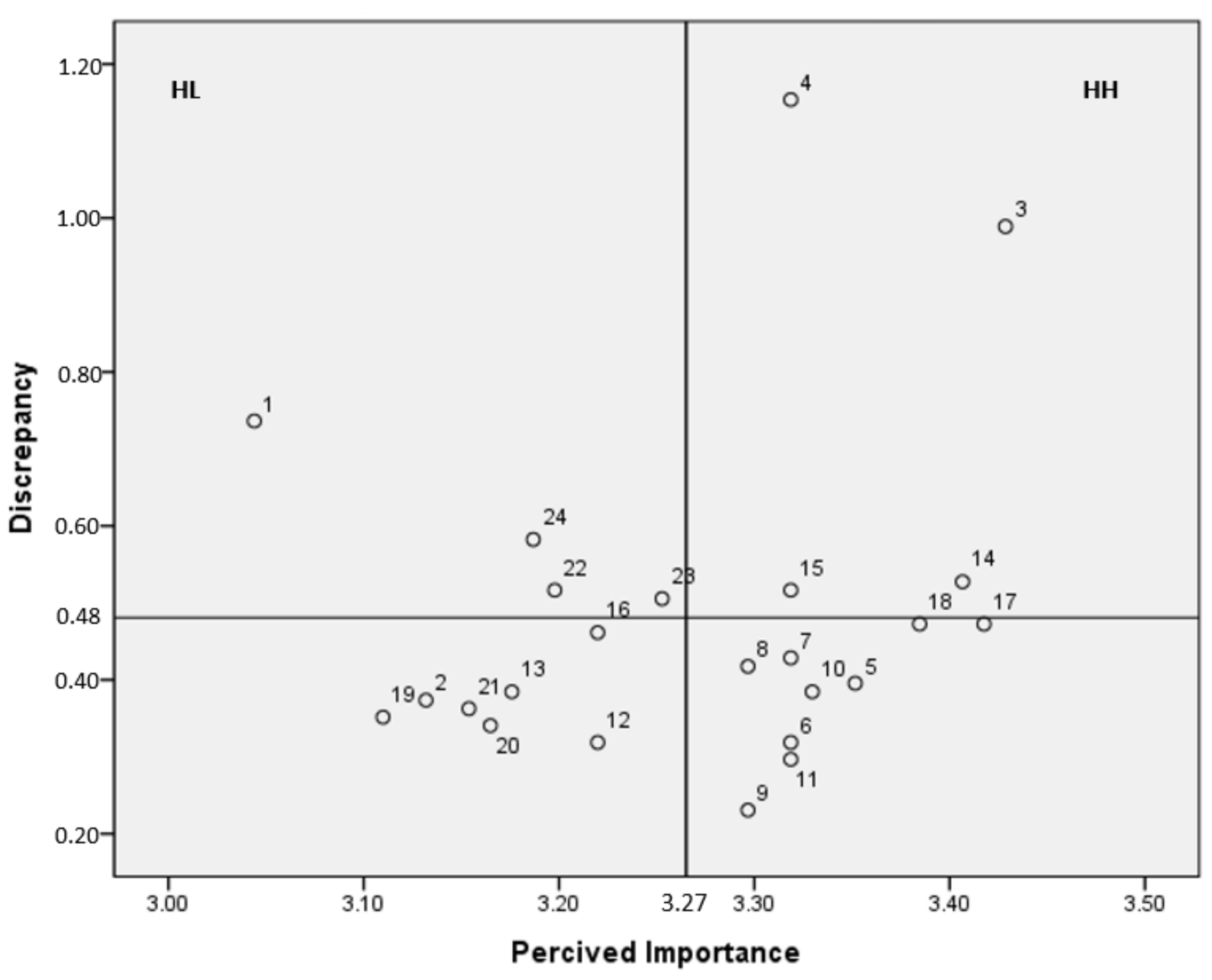
3.5. The Locus for Focus Model of Educational Needs for Forest Healing Programs for Cancer Survivors
3.6. Priority of Educational Needs for Forest Healing Programs for Cancer Survivors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Niedzwiedz, C.L.; Knifton, L.; Robb, K.A.; Katikireddi, S.V.; Smith, D.J. Depression and anxiety among people living with and beyond cancer: A growing clinical and research priority. BMC Cancer 2019, 19, 943. [Google Scholar] [CrossRef] [PubMed]
- Korea Central Cancer Registry. 2019 Annual Report of Korean Central Cancer Registry. Available online: https://ncc.re.kr/cancerStatsList.ncc?sea (accessed on 8 January 2022).
- Baek, S.Y.; Choi, J.Y. A comparative study on the characteristics of cancer patients and cancer survivors. Asian Oncol. Nurs. 2018, 18, 11–20. [Google Scholar] [CrossRef]
- Song, E.A.; Kweon, Y.; Hwang, Y.Y.; An, M. Health-related quality of life and its related factors among cancer survivors and general adults: Focusing on lifestyle behaviors and mental health. Korean J. Adult Nurs. 2020, 32, 385–398. [Google Scholar] [CrossRef]
- Miller, K.D.; Nogueira, L.; Mariotto, A.B.; Rowland, J.H.; Yabroff, K.R.; Alfano, C.M.; Jemal, A.; Kramer, J.L.; Siegel, R.L. Cancer treatment and survivorship statistics, 2019. CA Cancer J. Clin. 2019, 69, 363–385. [Google Scholar] [CrossRef] [PubMed]
- Jean, C.Y.; Syrjala, K.L. Anxiety and depression in cancer survivors. Med. Clin. 2017, 101, 1099–1113. [Google Scholar] [CrossRef]
- Korean Law Information Center Forestry Culture and Recreation Act. Available online: https://www.law.go.kr/ (accessed on 20 January 2022).
- Korea Forest Welfare Institute Forest Welfare. Available online: www.fowi.or.kr (accessed on 10 January 2022).
- Lawton, E.; Brymer, E.; Clough, P.; Denovan, A. The relationship between the physical activity environment, nature relatedness, anxiety, and the psychological well-being benefits of regular exercisers. Front. Psychol. 2017, 8, 1058. [Google Scholar] [CrossRef] [PubMed]
- Martyn, P.; Brymer, E. The relationship between nature relatedness and anxiety. J. Health Psychol. 2016, 21, 1436–1445. [Google Scholar] [CrossRef]
- Mayer, F.S.; Frantz, C.M.; Bruehlman-Senecal, E.; Dolliver, K. Why is nature beneficial? The role of connectedness to nature. Environ. Behav. 2009, 41, 607–643. [Google Scholar] [CrossRef]
- Lee, I.; Choi, H.; Bang, K.-S.; Kim, S.; Song, M.; Lee, B. Effects of forest therapy on depressive symptoms among adults: A systematic review. Int. J. Environ. Res. Public Health 2017, 14, 321. [Google Scholar] [CrossRef]
- Yi, Y.; An, J. Meta-analysis of the effects of forest therapy on depression among adult in Korea. J. Korean Inst. For. Recreat. 2021, 25, 91–106. [Google Scholar] [CrossRef]
- Chae, Y.R.; Lee, S.H. Systematic review of forest therapy program for adult patients with diseases. J. Korean Biol. Nurs. Sci. 2020, 22, 157–171. [Google Scholar] [CrossRef]
- Kim, K. Influence of forest healing programs on health care of cancer patients—Mainly about physiological characteristics and psychological traits. J. Humanit. Soc. Sci. 2020, 11, 13–26. [Google Scholar] [CrossRef]
- Lee, S. A Study on the Improvement of Training Program on the Forest Healing Instructor. Master’s Thesis, Kangwon University, Chuncheon, Korea, 2016. [Google Scholar]
- Lee, J.H.; Yoo, R.-H.; Lee, J.W. Analysis on visitors of healing forest for improvement of forest healing program. J. Korean Inst. For. Recreat. 2016, 20, 73–80. [Google Scholar] [CrossRef][Green Version]
- Park, S.-H.; Koo, C.-D. Needs analysis for the development of forest therapy program utilizing the urban forest: Focused on the Visitors of Incheon Grand Park. J. Korean Inst. For. Recreat. 2018, 22, 11–24. [Google Scholar] [CrossRef]
- Lee, J.E. A Study on the Subjectivity of the Forest Therapy in Forest Therapy Instructor Q Methodological Approach. Master’s Thesis, Chungbuk National Universi, Cheongju, Korea, 2020. [Google Scholar]
- Kim, J.-Y.; Shin, W.S.; Park, S.-H. The relationship between forest healing instructor’s job choice motivation and their job satisfaction. J. Korean Inst. For. Recreat. 2021, 25, 39–49. [Google Scholar] [CrossRef]
- Borich, G.D. A needs assessment model for conducting follow-up studies. J. Teach. Educ. 1980, 31, 39–42. [Google Scholar] [CrossRef]
- Mink, O.; Shultz, J.; Mink, B.; AB, F. Developing and Managing Open Organizations: A Model and Method for Maximizing Organizational Potential, 2nd ed.; Somerset Consulting Group: Austin, TX, USA, 1991. [Google Scholar]
- Shin, D.-A.; Bang, K.-S. Analysis of the educational needs of nurses in the neonatal intensive care unit for developmental supportive care. J. Korean Acad. Soc. Nurs. Educ. 2021, 27, 261–273. [Google Scholar] [CrossRef]
- Jang, J.; Lee, Y. An analysis of empowerment perception and needs according to individual characteristics of forest interpreters. J. People Plants Environ. 2018, 21, 167–183. [Google Scholar] [CrossRef]
- Kim, J.-S.; Kang, Y.-M.; Lee, S.-Y. A needs analysis oral health education contents for teachers and parents using Borich priority formula and the Locus for Focus Model. J. Dent. Hyg. Sci. 2018, 18, 252–264. [Google Scholar] [CrossRef]
- Jiang, S.; Hong, Y.A. Mobile-based patient-provider communication in cancer survivors: The roles of health literacy and patient activation. Psycho-Oncol. 2018, 27, 886–891. [Google Scholar] [CrossRef]
- Lee, M.S.; Baek, T.S.; Shin, H.S.; Lee, W.L.; Park, S.J.; Park, C.W.; Yeo, S.H.; Lee, S.J. Integrated medical perspective view on forest healing instructor training program and curriculum development. J. Digit. Converg. 2013, 11, 227–234. [Google Scholar] [CrossRef]
- Fujisawa, D.; Umezawa, S.; Fujimori, M.; Miyashita, M. Prevalence and associated factors of perceived cancer-related stigma in Japanese cancer survivors. Jpn. J. Clin. Oncol. 2020, 50, 1325–1329. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.; Kim, S.; Bang, K.S.; Yi, Y.; Lee, S.; Kim, D.; Jang, S.Y. Job analysis and curriculum development for forest healing instructor in charge of forest taegyo based on DACUM. J. Korean Inst. For. Recreat. 2020, 24, 37–46. [Google Scholar] [CrossRef]
- Lee, M.-M.; Park, B.-J. Effects of forest healing program on depression, stress and cortisol changes of cancer patients. J. People Plants Environ. 2020, 23, 245–254. [Google Scholar] [CrossRef]
- Park, L.; Jun, S.; Lee, J.A. Quality of life and associated factor among cancer survivors in Korea. Korean J. Health Promot. 2018, 18, 7–14. [Google Scholar] [CrossRef]
- Warmoth, K.; Wong, C.C.; Chen, L.; Ivy, S.; Lu, Q. The role of acculturation in the relationship between self-stigma and psychological distress among Chinese American breast cancer survivors. Psychol. Health Med. 2020, 25, 1278–1292. [Google Scholar] [CrossRef]
- Choi, K.H.; Oh, S.H. The effects of forest therapy program on job stress and self-esteem of the intellectually disabled. J. Learn. Cent. Curric. Instr. 2022, 22, 885–902. [Google Scholar] [CrossRef]
- Lee, M.-M.; Lee, D.-G.; Park, B.-J. A needs analysis for the development of forest healing programs: Focusing on cancer patients. J. People Plants Environ. 2020, 23, 683–694. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Categories | n (%) M ± SD | t (p) |
|---|---|---|---|
| Age | 55.7 ± 8.1 | ||
| Gender | Female | 62 (68.1) | |
| Male | 29 (31.9) | ||
| Education level | High school or university graduate | 43 (47.3) | |
| ≥Graduate school | 48 (52.7) | ||
| Major | Forest-related fields | 45 (49.5) | |
| Nursing/Health Science/Medicine | 23 (25.3) | ||
| Others | 23 (25.3) | ||
| Working period (month) | 30.7 ± 25.0 | ||
| Currently active | Yes | 56 (61.5) | |
| No | 35 (38.5) | ||
| Currently active facility | Natural recreation forest | 8 (14.3) | |
| Healing forest | 20 (35.7) | ||
| Urban forest/park | 22 (39.3) | ||
| Others | 6 (10.7) | ||
| Program operation experience for cancer survivors | Yes | 38 (41.8) | |
| No | 53 (58.2) | ||
| Degree of difficulty in program operation | Had experience | 2.05 ± 0.70 | −4.57 (<0.001) |
| No experience | 2.74 ± 0.71 | ||
| Difficulty reason 1 (Had experience) | Fear of an emergency | 13 (26.0) | |
| Fear that the participant is sensitive | 19 (38.0) | ||
| Fear that the participant’s health may deteriorate | 3 (6.0) | ||
| Hard to talk | 2 (4.0) | ||
| Lack of knowledge | 12 (24.0) | ||
| Others | 1 (2.0) | ||
| Difficulty reason 1 (No experience) | Fear of an emergency | 29 (33.3) | |
| Fear that the participant is sensitive | 27 (31.0) | ||
| Fear that the participant’s health may deteriorate | 8 (9.2) | ||
| Hard to talk | 1 (1.1) | ||
| Lack of knowledge | 21 (24.1) | ||
| Others | 1 (1.1) | ||
| Intention to participate in education | Yes | 90 (98.9) | |
| No | 1 (1.1) |
| Variables | Categories | Knowledge Level | Perceived Importance | ||
|---|---|---|---|---|---|
| M ± SD | T, F (p) | M ± SD | T, F (p) | ||
| Gender | Female | 2.78 ± 0.43 | −0.21 (0.837) | 3.31 ± 0.37 | 1.28 (0.205) |
| Male | 2.80 ± 0.53 | 3.18 ± 0.57 | |||
| Education level | High school or university graduate | 2.69 ± 0.50 | −1.89 (0.062) | 3.19 ± 0.49 | −1.54 (0.128) |
| ≥Graduate school | 2.87 ± 0.40 | 3.33 ± 0.40 | |||
| Major | Forest-related fields | 2.80 ± 0.51 | 1.40 (0.252) | 3.28 ± 0.52 | 0.78 (0.463) |
| Nursing/Public Health/Medicine | 2.87 ± 0.33 | 3.33 ± 0.39 | |||
| Others | 2.66 ± 0.44 | 3.17 ± 0.32 | |||
| Currently active | Yes | 2.85 ± 0.46 | 1.75 (0.084) | 3.27 ± 0.37 | 0.11 (0.909) |
| No | 2.68 ± 0.44 | 3.26 ± 0.55 | |||
| Currently active facility | Natural recreation forest | 2.89 ± 0.53 | 0.47 (0.707) | 3.21 ± 0.30 | 1.03 (0.388) |
| Healing forest | 2.76 ± 0.54 | 3.21 ± 0.35 | |||
| Urban forest/park | 2.92 ± 0.39 | 3.38 ± 0.41 | |||
| Others | 2.82 ± 0.33 | 3.15 ± 0.39 | |||
| Program operation experience for cancer survivors | Yes | 2.70 ± 0.51 | −1.49 (0.140) | 3.24 ± 0.53 | −0.47 (0.639) |
| No | 2.84 ± 0.41 | 3.28 ± 0.38 | |||
| Domain | Items | Knowledge Level M ± SD | Perceived Importance M ± SD | Mean Difference M ± SD | T (p) | Borich Needs Assessment | Ranks |
|---|---|---|---|---|---|---|---|
| 1. Cancer survivors’ overview | 2.42 ± 0.60 | 3.23 ± 0.54 | 0.81 ± 0.68 | 11.47 (<0.001) | 2.62 | 1 | |
| 1. Status for cancer survivors | 2.31 ± 0.78 | 3.04 ± 0.54 | 0.74 ± 0.89 | 7.87 (<0.001) | 2.24 | 3 | |
| 2. Cancer treatment (surgery, chemotherapy, radiation therapy, etc.) | 2.76 ± 0.74 | 3.13 ± 0.60 | 0.37 ± 0.80 | 4.47 (<0.001) | 1.17 | 17 | |
| 3. Effective communication with cancer survivors | 2.44 ± 0.73 | 3.43 ± 0.67 | 0.99 ± 0.86 | 10.94 (<0.001) | 3.39 | 2 | |
| 4. Health status screening method | 2.16 ± 0.69 | 3.32 ± 0.66 | 1.15 ± 0.91 | 12.15 (<0.001) | 3.83 | 1 | |
| 2. Emotional problems | 2.93 ± 0.44 | 3.32 ± 0.52 | 0.39 ± 0.58 | 6.44 (<0.001) | 1.29 | 4 | |
| 5. Depression/sadness | 2.96 ± 0.47 | 3.35 ± 0.57 | 0.40 ± 0.61 | 6.16 (<0.001) | 1.33 | 14 | |
| 6. Fear/worry | 3.00 ± 0.47 | 3.32 ± 0.53 | 0.32 ± 0.58 | 5.29 (<0.001) | 1.06 | 21 | |
| 7. Nervousness/irritability | 2.89 ± 0.53 | 3.32 ± 0.56 | 0.43 ± 0.72 | 5.70 (<0.001) | 1.42 | 12 | |
| 8. Loss of motivation | 2.88 ± 0.51 | 3.30 ± 0.55 | 0.42 ± 0.65 | 6.12 (<0.001) | 1.38 | 13 | |
| 3. Physical problems | 2.90 ± 0.51 | 3.29 ± 0.48 | 0.39 ± 0.61 | 6.12 (<0.001) | 1.28 | 5 | |
| 9. Change in appearance (hair loss, skin color) | 3.07 ± 0.49 | 3.30 ± 0.53 | 0.23 ± 0.60 | 3.68 (<0.001) | 0.76 | 24 | |
| 10. Diet (weight/intake change) | 2.95 ± 0.54 | 3.33 ± 0.56 | 0.38 ± 0.68 | 5.40 (<0.001) | 1.28 | 15 | |
| 11. Fatigue | 3.02 ± 0.52 | 3.32 ± 0.53 | 0.30 ± 0.59 | 4.82 (<0.001) | 0.98 | 23 | |
| 12. Indigestion (nausea) | 2.90 ± 0.60 | 3.22 ± 0.55 | 0.32 ± 0.70 | 4.36 (<0.001) | 1.03 | 22 | |
| 13. Memory/reduced concentration | 2.79 ± 0.68 | 3.18 ± 0.51 | 0.38 ± 0.76 | 4.85 (<0.001) | 1.22 | 16 | |
| 14. Pain | 2.88 ± 0.70 | 3.41 ± 0.56 | 0.53 ± 0.85 | 5.94 (<0.001) | 1.80 | 5 | |
| 15. Sleep disorder | 2.80 ± 0.64 | 3.32 ± 0.53 | 0.52 ± 0.78 | 6.32 (<0.001) | 1.71 | 6 | |
| 16. Numbness of limbs | 2.76 ± 0.69 | 3.22 ± 0.49 | 0.46 ± 0.76 | 5.76 (<0.001) | 1.49 | 11 | |
| 4. Spiritual problems | 2.93 ± 0.57 | 3.40 ± 0.56 | 0.47 ± 0.71 | 6.33 (<0.001) | 1.60 | 3 | |
| 17. Anxiety about recurrence/death | 2.95 ± 0.60 | 3.42 ± 0.58 | 0.47 ± 0.75 | 6.01 (<0.001) | 1.61 | 9 | |
| 18. Worries about the meaning of life | 2.91 ± 0.61 | 3.38 ± 0.57 | 0.47 ± 0.75 | 6.01 (<0.001) | 1.60 | 10 | |
| 5. Functional problems | 2.79 ± 0.62 | 3.14 ± 0.54 | 0.35 ± 0.69 | 4.87 (<0.001) | 1.10 | 6 | |
| 19. Raising children | 2.76 ± 0.64 | 3.11 ± 0.55 | 0.35 ± 0.72 | 4.65 (<0.001) | 1.09 | 19 | |
| 20. Economic problems | 2.82 ± 0.66 | 3.16 ± 0.54 | 0.34 ± 0.76 | 4.26 (<0.001) | 1.08 | 20 | |
| 21. Work/school | 2.79 ± 0.66 | 3.15 ± 0.61 | 0.36 ± 0.75 | 4.59 (<0.001) | 1.14 | 18 | |
| 6. Family problems | 2.68 ± 0.68 | 3.21 ± 0.52 | 0.53 ± 0.79 | 6.42 (<0.001) | 1.70 | 2 | |
| 22. Problems with children | 2.68 ± 0.68 | 3.20 ± 0.52 | 0.52 ± 0.81 | 6.10 (<0.001) | 1.65 | 7 | |
| 23. Relationship with spouse | 2.75 ± 0.74 | 3.25 ± 0.57 | 0.51 ± 0.86 | 5.60 (<0.001) | 1.64 | 8 | |
| 24. Relationship with parents | 2.60 ± 0.71 | 3.19 ± 0.54 | 0.58 ± 0.84 | 6.58 (<0.001) | 1.86 | 4 | |
| Total | 2.78 ± 0.46 | 3.27 ± 0.45 | 0.48 ± 0.53 | 8.69 (<0.001) | 1.49 | ||
| Domain | Contents | Rank (Borich Needs Assessment) | Quadrant (Locus for Focus Model) | High Priority |
|---|---|---|---|---|
| 1 | 4. Health status screening method | 1 | Ⅰ | 1 |
| 1 | 3. Effective communication with cancer survivors | 2 | Ⅰ | 1 |
| 1 | 1. Status for cancer survivors | 3 | Ⅱ | 2 |
| 6 | 24. Relationship with parents | 4 | Ⅱ | 2 |
| 3 | 14. Pain | 5 | Ⅰ | 2 |
| 3 | 15. Sleep disorder | 6 | Ⅰ | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, K.-H.; Song, M.K. Priority Analysis of Educational Needs of Forest Healing Instructors Related to Programs for Cancer Survivors: Using Borich Needs Assessment and the Locus for Focus Model. Int. J. Environ. Res. Public Health 2022, 19, 5376. https://doi.org/10.3390/ijerph19095376
Park K-H, Song MK. Priority Analysis of Educational Needs of Forest Healing Instructors Related to Programs for Cancer Survivors: Using Borich Needs Assessment and the Locus for Focus Model. International Journal of Environmental Research and Public Health. 2022; 19(9):5376. https://doi.org/10.3390/ijerph19095376
Chicago/Turabian StylePark, Kwang-Hi, and Min Kyung Song. 2022. "Priority Analysis of Educational Needs of Forest Healing Instructors Related to Programs for Cancer Survivors: Using Borich Needs Assessment and the Locus for Focus Model" International Journal of Environmental Research and Public Health 19, no. 9: 5376. https://doi.org/10.3390/ijerph19095376
APA StylePark, K.-H., & Song, M. K. (2022). Priority Analysis of Educational Needs of Forest Healing Instructors Related to Programs for Cancer Survivors: Using Borich Needs Assessment and the Locus for Focus Model. International Journal of Environmental Research and Public Health, 19(9), 5376. https://doi.org/10.3390/ijerph19095376