
Inequality in the Utilization of Breast Cancer Screening between Women with and without Disabilities in Taiwan: A Propensity-Score-Matched Nationwide Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
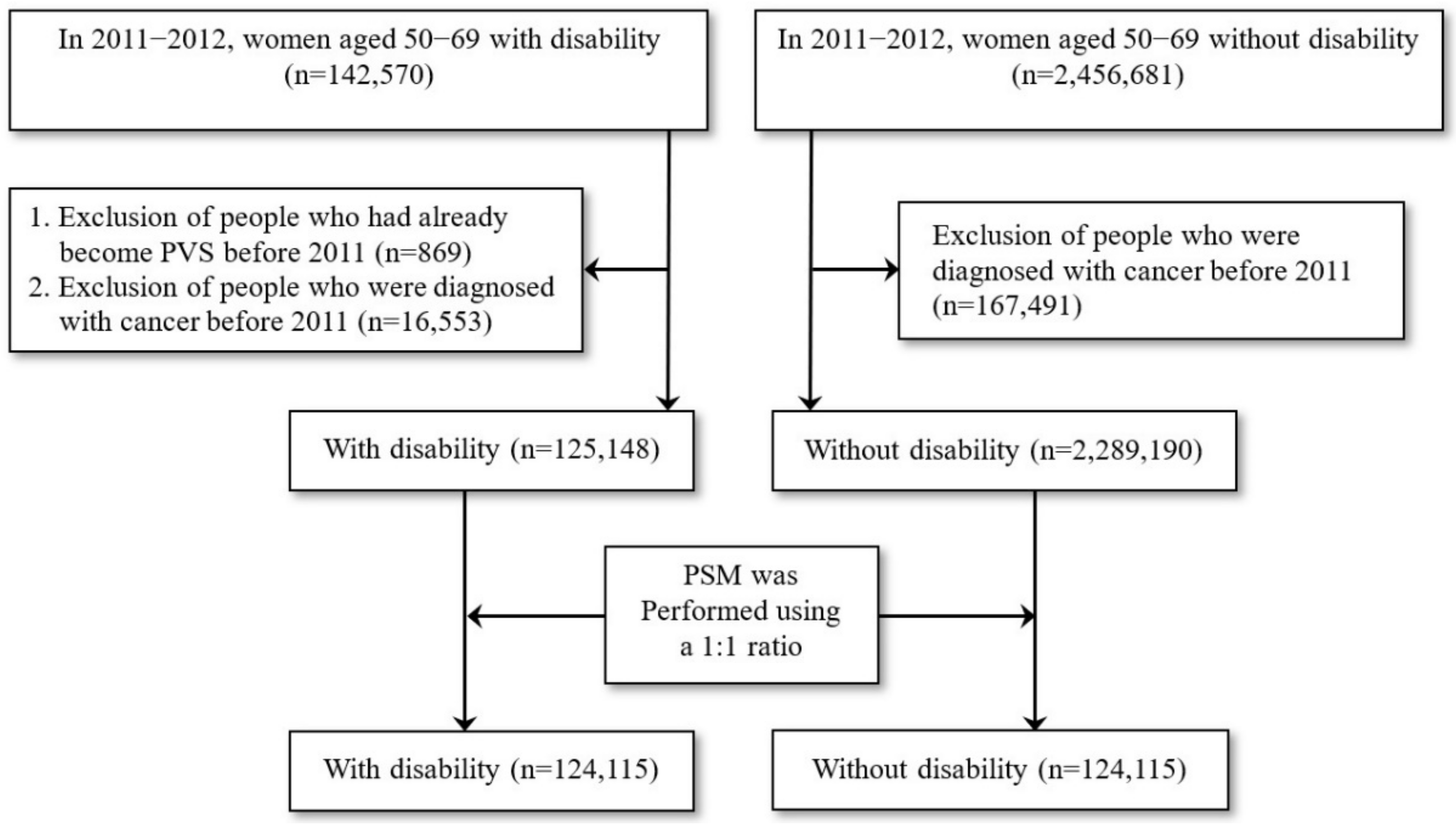
2.2. Study Design and Study Population
2.3. Variable Descriptions and Definitions
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Global Burden of Disease Cancer Collaboration. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived with Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2017: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2019, 5, 1749–1768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Cancer Research Fund/American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective. Available online: https://www.wcrf.org/sites/default/files/Breast-cancer-report.pdf (accessed on 5 August 2021).
- Ministry of Health and Welfare. Statistics on The Causes of Death of Taiwanese. Available online: https://www.mohw.gov.tw/cp-16-54482-1.html (accessed on 10 August 2021).
- Health Promotion Administration. The Cancer Registry Report in Taiwan in 2014. Available online: https://www.hpa.gov.tw/Pages/ashx/File.ashx?FilePath=∼/File/Attach/7308/File_6785.pdf (accessed on 25 August 2021).
- Gøtzsche, P.C.; Jørgensen, K.J. Screening for Breast Cancer with Mammography. Cochrane Database Syst Rev. 2013, 156, CD001877. [Google Scholar] [CrossRef] [PubMed]
- Health Promotion Administration. 2016 National Health Agency Annual Report. Available online: https://www.hpa.gov.tw/Pages/List.aspx?nodeid=1249 (accessed on 25 August 2021).
- Sakellariou, D.; Rotarou, E.S. Access to Healthcare for Men and Women with Disabilities in the UK: Secondary Analysis of Cross-Sectional Data. BMJ Open 2017, 7, e016614. [Google Scholar] [CrossRef] [PubMed]
- Courtney-Long, E.; Armour, B.; Frammartino, B.; Miller, J. Factors Associated with Self-Reported Mammography Use for Women with and Women Without a Disability. J. Women’s Health 2011, 20, 1279–1286. [Google Scholar] [CrossRef]
- Shin, D.W.; Yu, J.; Cho, J.; Lee, S.K.; Jung, J.H.; Han, K.; Kim, S.Y.; Yoo, J.E.; Yeob, K.E.; Kim, Y.Y.; et al. Breast Cancer Screening Disparities Between Women with and without Disabilities: A National Database Study in South Korea. Cancer 2020, 126, 1522–1529. [Google Scholar] [CrossRef]
- Ministry of Health and Welfare. 2017 Taiwan Health and Welfare Report. Available online: https://www.mohw.gov.tw/dl-44682-2644622d-3e42-495a-bbdc-ebb6e6d55092.html (accessed on 29 August 2021).
- Yankaskas, B.C.; Dickens, P.; Bowling, J.M.; Jarman, M.P.; Luken, K.; Salisbury, K.; Halladay, J.; Lorenz, C.E. Barriers to Adherence to Screening Mammography among Women with Disabilities. Am. J. Public Health 2010, 100, 947–953. [Google Scholar] [CrossRef]
- Groß, S.E.; Pfaff, H.; Swora, M.; Ansmann, L.; Albert, U.S.; Groß-Kunkel, A. Health Disparities among Breast Cancer Patients With/Without Disabilities in Germany. Disabil. Health J. 2020, 13, 100873. [Google Scholar] [CrossRef]
- Floud, S.; Barnes, I.; Verfürden, M.; Kuper, H.; Gathani, T.; Blanks, R.G.; Alison, R.; Patnick, J.; Beral, V.; Green, J.; et al. Disability and Participation in Breast and Bowel Cancer Screening in England: A Large Prospective Study. Br. J. Cancer 2017, 117, 1711–1714. [Google Scholar] [CrossRef] [Green Version]
- National Health Insurance Research Database, Taiwan. Available online: http://nhird.nhri.org.tw/en/index.htm (accessed on 18 August 2021).
- National Health Insurance Administration. Copayment. Available online: https://www.nhi.gov.tw/english/Content_List.aspx?n=E5509C8FE29950EA&topn=1D1ECC54F86E9050#:~:text=When%20local%20residents%20covered%20under,insured%20that%20medical%20resources%20are (accessed on 12 April 2022).
- Ban, L.K.; Tseng, A.H.; Hsing, H.C.; Lee, H.H. Improving Colorectal, Oral, Breast, and Cervical Cancer Screening Rates using an Inreach Approach. J. Cancer Res. Pract. 2019, 6, 26–29. [Google Scholar] [CrossRef]
- Health Promotion Administration. Taiwan Breast Cancer, Oral Cancer, and Colorectal Cancer Screening Programs. Available online: https://www.hpa.gov.tw/EngPages/Detail.aspx?nodeid=1051&pid=5957 (accessed on 3 September 2021).
- Chiu, W.T.; Yen, C.F.; Teng, S.W.; Liao, H.F.; Chang, K.H.; Chi, W.C.; Wang, Y.H.; Liou, T.H. Implementing Disability Evaluation and Welfare Services Based on the Framework of the International Classification of Functioning, Disability and Health: Experiences in Taiwan. BMC Health Serv. Res. 2013, 13, 416. [Google Scholar] [CrossRef] [Green Version]
- Kung, P.T.; Tsai, W.C.; Li, Y.H. Determining Factors for Utilization of Preventive Health Services among Adults with Disabilities in Taiwan. Res. Dev. Disabil. 2012, 33, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Division of Welfare Services for the Disabled. Services. Department of Social Welfare. Available online: https://english.dosw.gov.taipei/News_Content.aspx?n=78DCE46BFF7721CF&sms=85FBABE70858A8D4&s=8EC812B46B867994 (accessed on 30 December 2020).
- Morgan, C.J. Reducing Bias Using Propensity Score Matching. J. Nucl. Cardiol. 2018, 25, 404–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, C.Y.; Hung, H.Y.; Chuang, Y.L.; Chen, Y.J.; Weng, W.S.; Liu, J.S.; Liang, K.Y. Incorporating Development Stratification of Taiwan Townships into Sampling Design of Large Scale Health Interview Survey. J. Health Manag. 2006, 4, 1–22. [Google Scholar] [CrossRef]
- Deyo, R.A.; Cherkin, D.C.; Ciol, M.A. Adapting a Clinical Comorbidity Index for Use with ICD-9-CM Administrative Databases. J. Clin. Epidemiol. 1992, 45, 613–619. [Google Scholar] [CrossRef]
- Ramjan, L.; Cotton, A.; Algoso, M.; Peters, K. Barriers to Breast and Cervical Cancer Screening for Women with Physical Disability: A Review. Women Health 2016, 56, 141–156. [Google Scholar] [CrossRef] [PubMed]
- Horner-Johnson, W.; Dobbertin, K.; Andresen, E.M.; Iezzoni, L.I. Breast and Cervical Cancer Screening Disparities Associated with Disability Severity. Women’s Health Issues 2014, 24, e147–e153. [Google Scholar] [CrossRef] [PubMed]
- Law, M.; Dhillon, S.; Herrmann, N.; Farah, F.; Dey, A.K.; Li, A.; Ayala, A.P.; Lenton, E.; Edwards, J.D.; Swardfager, W. Rates of Screening for Breast, Colorectal, and Cervical Cancers in Older People with Cognitive Impairment or Dementia: A Meta-Analysis. Gerontol. Geriatr. Med. 2018, 4, 2333721418799446. [Google Scholar] [CrossRef] [Green Version]
- Mehta, K.M.; Fung, K.Z.; Kistler, C.E.; Chang, A.; Walter, L.C. Impact of Cognitive Impairment on Screening Mammography Use in Older US Women. Am. J. Public Health 2010, 100, 1917–1923. [Google Scholar] [CrossRef] [PubMed]
- Walter, L.C.; Eng, C.; Covinsky, K.E. Screening Mammography for Frail Older Women: What Are the Burdens? J. Gen. Intern. Med. 2001, 16, 779–784. [Google Scholar] [CrossRef]
- Sachs, G.A.; Carter, R.; Holtz, L.R.; Smith, F.; Stump, T.E.; Tu, W.; Callahan, C.M. Cognitive Impairment: An Independent Predictor of Excess Mortality: A Cohort Study. Ann. Intern. Med. 2011, 155, 300–308. [Google Scholar] [CrossRef]
- Waring, S.C.; Doody, R.S.; Pavlik, V.N.; Massman, P.J.; Chan, W. Survival among Patients with Dementia from a Large Multi-Ethnic Population. Alzheimer Dis. Assoc. Disord. 2005, 19, 178–183. [Google Scholar] [CrossRef] [PubMed]
- CassCel, C.K. Breast Cancer Screening in Older Women: Ethical Issues. J. Gerontol. 1992, 47, 126–130. [Google Scholar]
- Todd, A.; Stuifbergen, A. Barriers and Facilitators to Breast Cancer Screening: A Qualitative Study of Women with Multiple Sclerosis. Int. J. MS Care 2011, 13, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Angus, J.; Seto, L.; Barry, N.; Cechetto, N.; Chandani, S.; Devaney, J.; Fernando, S.; Muraca, L.; Odette, F. Access to Cancer Screening for Women with Mobility Disabilities. J. Cancer Educ. 2012, 27, 75–82. [Google Scholar] [CrossRef]
- NHS. Overview: Multiple Sclerosis. Available online: https://www.nhs.uk/conditions/multiple-sclerosis/ (accessed on 17 September 2021).
- Department of Health. Implementation Regulations for NHI Preventive Care. Available online: http://www.nhi.gov.tw/webdata/webdata.aspx?menu=&menu_id=&wd_id=&webdata_id=2432 (accessed on 1 October 2021).
- Guilcher, S.J.; Lofters, A.; Glazier, R.H.; Jaglal, S.B.; Voth, J.; Bayoumi, A.M. Level of Disability, Multi-Morbidity and Breast Cancer Screening: Does Severity Matter? Prev. Med. 2014, 67, 193–198. [Google Scholar] [CrossRef]
- Tsai, W.C.; Kung, P.T.; Wang, J.Y. Disparities in the Use of Preventive Health Care among Children with Disabilities in Taiwan. Res. Dev. Disabil. 2012, 33, 324–333. [Google Scholar] [CrossRef]
- Sun, J.K.; Smith, J. Self-Perceptions of Aging and Perceived Barriers to Care: Reasons for Health Care Delay. Gerontologist 2017, 57, S216–S226. [Google Scholar] [CrossRef]
- Bayliss, E.A.; Ellis, J.L.; Steiner, J.F. Barriers to Self-Management and Quality-of-Life Outcomes in Seniors with Multimorbidities. Ann. Fam. Med. 2007, 5, 395–402. [Google Scholar] [CrossRef]
- Fisher, E.B.; Fitzgibbon, M.L.; Glasgow, R.E.; Haire-Joshu, D.; Hayman, L.L.; Kaplan, R.M.; Nanney, M.S.; Ockene, J.K. Behavior Matters. Am. J. Prev. Med. 2011, 40, e15–e30. [Google Scholar] [CrossRef]
- Kasl, S.V.; Cobb, S. Health Behavior, Illness Behavior, and Sick-Role Behavior. II. Sick-Role Behavior. Arch. Environ. Health 1966, 12, 531–541. [Google Scholar] [CrossRef]
- Yom Din, G.; Zugman, Z.; Khashper, A. The Impact of Preventive Health Behaviour and Social Factors on Visits to The Doctor. Isr. J. Health Policy Res. 2014, 3, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorant, V.; Boland, B.; Humblet, P.; Deliège, D. Equity in Prevention and Health Care. J. Epidemiol. Community Health 2002, 56, 510–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jusot, F.; Or, Z.; Sirven, N. Variations in Preventive Care Utilisation in Europe. Eur. J. Ageing 2012, 9, 15–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harkins, C.; Shaw, R.; Gillies, M.; Sloan, H.; Macuntyre, K.; Scoular, A.; Morrison, C.; Mackay, F.; Cunningham, H.; Docherty, P. Overcoming Barriers to Engaging Socio-Economically Disadvantaged Populations in CHD Primary Prevention: A Qualitative Study. BMC Public Health 2010, 10, 391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soskolne, V. Preventive Health Behaviors and Physician Visits: Relevance to Health Inequality. Isr. J. Health Policy Res. 2015, 4, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eurostat Statistics Explained. Archive: Breast Cancer Screening Statistics. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Archive:Breast_cancer_screening_statistics (accessed on 8 April 2022).
- Chan, H.P.; Samala, R.K.; Hadjiiski, L.M. CAD and AI for Breast Cancer-Recent Development and Challenges. Br. J. Radiol. 2020, 93, 20190580. [Google Scholar] [CrossRef]
- United Nations Department of Economic and Social Affairs. Sustainable Development Goals (SDGs) and Disability. Available online: https://www.un.org/development/desa/disabilities/about-us/sustainable-development-goals-sdgs-and-disability.html (accessed on 15 October 2021).
- WHO. A New Landmark Resolution on Disability Adopted at the 74th World Health Assembly. Available online: https://www.who.int/news/item/27-05-2021-a-new-landmark-resolution-on-disability-adopted-at-the-74th-world-health-assembly (accessed on 15 October 2021).
- Jagger, C. Educational Disparities in Adult Disability: Person, Place, Policies, and Family. Am. J. Public Health 2017, 107, 1021–1022. [Google Scholar] [CrossRef]
- Maryland Population Research Center. People with Disabilities Less Likely to Get Married. Available online: https://www.popcenter.umd.edu/news/news_1483634158302 (accessed on 11 April 2022).
- WHO. Disability and Health. Available online: https://www.who.int/en/news-room/fact-sheets/detail/disability-and-health (accessed on 11 April 2022).

{kind=link}
| Variables | Women without Disabilities | Women with Disabilities | |||||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | p-Value a | |
| Total | 248,230 | 100.00 | 124,115 | 50.00 | 124,115 | 50.00 | |
| Age | 0.827 | ||||||
| 50–59 years | 137,555 | 55.41 | 68,750 | 49.98 | 68,805 | 50.02 | |
| 60–69years | 110,675 | 44.59 | 55,365 | 50.02 | 55,310 | 49.98 | |
| Monthly salary (NT$) | 0.976 | ||||||
| Low-income households | 6856 | 2.76 | 3397 | 49.55 | 3459 | 50.45 | |
| ≦17,280 | 14,642 | 5.90 | 7352 | 50.21 | 7290 | 49.79 | |
| 17,281–22,800 | 109,430 | 44.08 | 54,715 | 50.00 | 54,715 | 50.00 | |
| 22,801–28,800 | 50,570 | 20.37 | 25,285 | 50.00 | 25,285 | 50.00 | |
| 28,801–36,300 | 33,484 | 13.49 | 16,742 | 50.00 | 16,742 | 50.00 | |
| ≧36,301 | 33,248 | 13.39 | 16,624 | 50.00 | 16,624 | 50.00 | |
| Urbanization level | 1.000 | ||||||
| 1 | 50,986 | 20.54 | 25,493 | 50.00 | 25,493 | 50.00 | |
| 2 | 75,233 | 30.31 | 37,644 | 50.04 | 37,589 | 49.96 | |
| 3 | 37,336 | 15.04 | 18,668 | 50.00 | 18,668 | 50.00 | |
| 4 | 45,329 | 18.26 | 22,637 | 49.94 | 22,692 | 50.06 | |
| 5 | 8400 | 3.38 | 4200 | 50.00 | 4200 | 50.00 | |
| 6 | 16,311 | 6.57 | 8151 | 49.97 | 8160 | 50.03 | |
| 7 | 14,635 | 5.90 | 7322 | 50.03 | 7313 | 49.97 | |
| CCI b | 0.990 | ||||||
| 0 | 105,748 | 42.60 | 52,843 | 49.97 | 52,905 | 50.03 | |
| 1 | 53,160 | 21.42 | 26,580 | 50.00 | 26,580 | 50.00 | |
| 2 | 38,196 | 15.39 | 19,098 | 50.00 | 19,098 | 50.00 | |
| ≧3 | 51,126 | 20.60 | 25,594 | 50.06 | 25,532 | 49.94 | |
| Variables | Total | Women without Disabilities | Women with Disabilities | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| No Mammography | Mammography | No Mammography | Mammography | ||||||||
| N | % | N | % | N | % | N | % | N | % | p-Value a | |
| Total | 248,230 | 100.00 | 92,438 | 74.48 | 31,677 | 25.52 | 101,367 | 81.67 | 22,748 | 18.33 | <0.001 |
| Disability type | |||||||||||
| Without disability | 124,115 | 50.00 | 92,438 | 74.48 | 31,677 | 25.52 | |||||
| Moving functional limitation | 55,296 | 22.28 | 44,446 | 80.38 | 10,850 | 19.62 | |||||
| Visual impairment | 8201 | 3.30 | 6745 | 82.25 | 1456 | 17.75 | |||||
| Hearing impairment | 11,980 | 4.83 | 9025 | 75.33 | 2955 | 24.67 | |||||
| Speech disorder | 919 | 0.37 | 741 | 80.63 | 178 | 19.37 | |||||
| Intellectual disability | 4245 | 1.71 | 3676 | 86.60 | 569 | 13.40 | |||||
| Multiple disabilities | 9438 | 3.80 | 8449 | 89.52 | 989 | 10.48 | |||||
| Dysfunction of primary organs | 18,956 | 7.64 | 16,417 | 86.61 | 2539 | 13.39 | |||||
| Facial impairment | 214 | 0.09 | 149 | 69.63 | 65 | 30.37 | |||||
| Dementia | 1642 | 0.66 | 1529 | 93.12 | 113 | 6.88 | |||||
| Congenital disorders | 24 | 0.01 | 14 | 58.33 | 10 | 41.67 | |||||
| Chronic mental health conditions | 12,667 | 5.10 | 9761 | 77.06 | 2906 | 22.94 | |||||
| Balance disorder | 322 | 0.13 | 271 | 84.16 | 51 | 15.84 | |||||
| Intractable epilepsy | 151 | 0.06 | 96 | 63.58 | 55 | 36.42 | |||||
| Rare diseases | 42 | 0.02 | 33 | 78.57 | 9 | 21.43 | |||||
| Other b | 18 | 0.01 | 15 | 83.33 | 3 | 16.67 | |||||
| Severity of disability | |||||||||||
| Without disability | 124,115 | 50.00 | 92,438 | 74.48 | 31,677 | 25.52 | |||||
| Mild | 45,336 | 18.26 | 33,781 | 74.51 | 11,555 | 25.49 | |||||
| Moderate | 39,179 | 15.78 | 31,988 | 81.65 | 7191 | 18.35 | |||||
| Severe | 19,915 | 8.02 | 17,774 | 89.25 | 2141 | 10.75 | |||||
| Very severe | 19,685 | 7.93 | 17,824 | 90.55 | 1861 | 9.45 | |||||
| Age | |||||||||||
| 50–59 years | 137,555 | 55.41 | 44,142 | 64.21 | 24,608 | 35.79 | 50,326 | 73.14 | 18,479 | 26.86 | <0.001 |
| 60–69 years | 110,675 | 44.59 | 48,296 | 87.23 | 7069 | 12.77 | 51,041 | 92.28 | 4269 | 7.72 | <0.001 |
| Monthly salary (NT$) | |||||||||||
| Low-income households | 6856 | 2.76 | 2676 | 78.78 | 721 | 21.22 | 2978 | 86.09 | 481 | 13.91 | <0.001 |
| ≦17,280 | 14,642 | 5.90 | 5656 | 76.93 | 1696 | 23.07 | 6216 | 85.27 | 1074 | 14.73 | <0.001 |
| 17,281–22,800 | 109,430 | 44.08 | 41,645 | 76.11 | 13,070 | 23.89 | 45,427 | 83.02 | 9288 | 16.98 | <0.001 |
| 22,801–28,800 | 50,570 | 20.37 | 18,791 | 74.32 | 6494 | 25.68 | 20,770 | 82.14 | 4515 | 17.86 | <0.001 |
| 28,801–36,300 | 33,484 | 13.49 | 12,070 | 72.09 | 4672 | 27.91 | 13,295 | 79.41 | 3447 | 20.59 | <0.001 |
| ≧36,301 | 33,248 | 13.39 | 11,600 | 69.78 | 5024 | 30.22 | 12,681 | 76.28 | 3943 | 23.72 | <0.001 |
| Urbanization level | |||||||||||
| 1 | 50,986 | 20.54 | 19,070 | 74.80 | 6423 | 25.20 | 20,967 | 82.25 | 4526 | 17.75 | <0.001 |
| 2 | 75,233 | 30.31 | 27,837 | 73.95 | 9807 | 26.05 | 30,163 | 80.24 | 7426 | 19.76 | <0.001 |
| 3 | 37,336 | 15.04 | 14,119 | 75.63 | 4549 | 24.37 | 15,662 | 83.90 | 3006 | 16.10 | <0.001 |
| 4 | 45,329 | 18.26 | 16,927 | 74.78 | 5710 | 25.22 | 18,630 | 82.10 | 4062 | 17.90 | <0.001 |
| 5 | 8400 | 3.38 | 3117 | 74.21 | 1083 | 25.79 | 3342 | 79.57 | 858 | 20.43 | <0.001 |
| 6 | 16,311 | 6.57 | 5954 | 73.05 | 2197 | 26.95 | 6583 | 80.67 | 1577 | 19.33 | <0.001 |
| 7 | 14,635 | 5.90 | 5414 | 73.94 | 1908 | 26.06 | 6020 | 82.32 | 1293 | 17.68 | <0.001 |
| CCI c | |||||||||||
| 0 | 105,748 | 42.60 | 39,484 | 74.72 | 13,359 | 25.28 | 41,459 | 78.36 | 11,446 | 21.64 | <0.001 |
| 1 | 53,160 | 21.42 | 19,293 | 72.58 | 7287 | 27.42 | 20,957 | 78.84 | 5623 | 21.16 | <0.001 |
| 2 | 38,196 | 15.39 | 13,997 | 73.29 | 5101 | 26.71 | 15,879 | 83.14 | 3219 | 16.86 | <0.001 |
| ≧3 | 51,126 | 20.60 | 19,664 | 76.83 | 5930 | 23.17 | 23,072 | 90.37 | 2460 | 9.63 | <0.001 |
| Adults’ preventive care service | |||||||||||
| No | 161,286 | 64.97 | 57,994 | 78.73 | 15,668 | 21.27 | 75,515 | 86.18 | 12,109 | 13.82 | <0.001 |
| Yes | 86,944 | 35.03 | 34,444 | 68.27 | 16,009 | 31.73 | 25,852 | 70.84 | 10,639 | 29.16 | <0.001 |
| Variables | Model A | Model B | Model C | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | ||||
| Disability status | ||||||||||||
| No (reference) | 1.00 | – | – | – | ||||||||
| Yes | 0.72 | 0.71 | 0.74 | <0.001 | ||||||||
| Disability type | ||||||||||||
| Without disability (reference) | 1.00 | – | – | – | ||||||||
| Moving functional limitation | 0.73 | 0.68 | 0.78 | <0.001 | ||||||||
| Visual impairment | 1.00 | 0.95 | 1.06 | 0.884 | ||||||||
| Hearing impairment | 0.71 | 0.59 | 0.87 | 0.001 | ||||||||
| Speech disorder | 0.77 | 0.74 | 0.79 | <0.001 | ||||||||
| Intellectual disability | 0.45 | 0.41 | 0.50 | <0.001 | ||||||||
| Multiple disabilities | 0.43 | 0.40 | 0.47 | <0.001 | ||||||||
| Dysfunction of primary organs | 0.59 | 0.56 | 0.62 | <0.001 | ||||||||
| Facial impairment | 0.97 | 0.68 | 1.39 | 0.857 | ||||||||
| Dementia | 0.34 | 0.28 | 0.43 | <0.001 | ||||||||
| Congenital disorders | 1.95 | 0.61 | 6.26 | 0.263 | ||||||||
| Chronic mental health conditions | 0.82 | 0.78 | 0.86 | <0.001 | ||||||||
| Balance disorder | 0.63 | 0.45 | 0.89 | 0.008 | ||||||||
| Intractable epilepsy | 1.33 | 0.90 | 1.97 | 0.154 | ||||||||
| Rare diseases | 0.65 | 0.28 | 1.53 | 0.322 | ||||||||
| Other a | 0.38 | 0.09 | 1.56 | 0.181 | ||||||||
| Severity of disability | ||||||||||||
| Without disability (reference) | 1.00 | – | – | – | ||||||||
| Mild | 1.00 | 0.97 | 1.03 | 0.906 | ||||||||
| Moderate | 0.73 | 0.71 | 0.76 | <0.001 | ||||||||
| Severe | 0.42 | 0.40 | 0.45 | <0.001 | ||||||||
| Very severe | 0.39 | 0.37 | 0.41 | <0.001 | ||||||||
| Age | ||||||||||||
| 50–59 years (reference) | 1.00 | – | – | – | 1.00 | – | – | – | 1.00 | – | – | – |
| 60–69 years | 0.27 | 0.26 | 0.28 | <0.001 | 0.27 | 0.26 | 0.28 | <0.001 | 0.27 | 0.26 | 0.28 | <0.001 |
| Monthly salary (NT$) | ||||||||||||
| Low-income households (reference) | 1.00 | – | – | – | 1.00 | – | – | – | 1.00 | – | – | – |
| ≦17,280 | 1.27 | 1.11 | 1.45 | 0.001 | 1.25 | 1.09 | 1.43 | 0.001 | 1.19 | 1.04 | 1.36 | 0.011 |
| 17,281–22,800 | 1.35 | 1.21 | 1.51 | <0.001 | 1.32 | 1.18 | 1.48 | <0.001 | 1.25 | 1.12 | 1.40 | <0.001 |
| 22,801–28,800 | 1.32 | 1.17 | 1.48 | <0.001 | 1.30 | 1.15 | 1.46 | <0.001 | 1.23 | 1.10 | 1.39 | 0.001 |
| 28,801–36,300 | 1.33 | 1.18 | 1.50 | <0.001 | 1.32 | 1.17 | 1.49 | <0.001 | 1.26 | 1.11 | 1.42 | <0.001 |
| ≧36,301 | 1.51 | 1.34 | 1.71 | <0.001 | 1.48 | 1.31 | 1.67 | <0.001 | 1.40 | 1.24 | 1.58 | <0.001 |
| Urbanization level | ||||||||||||
| 1 (reference) | 1.00 | – | – | – | 1.00 | – | – | – | 1.00 | – | – | – |
| 2 | 1.22 | 1.17 | 1.27 | <0.001 | 1.22 | 1.17 | 1.27 | <0.001 | 1.21 | 1.16 | 1.26 | <0.001 |
| 3 | 1.07 | 1.02 | 1.13 | 0.006 | 1.08 | 1.03 | 1.13 | 0.003 | 1.08 | 1.03 | 1.13 | 0.004 |
| 4 | 1.32 | 1.26 | 1.39 | <0.001 | 1.33 | 1.26 | 1.39 | <0.001 | 1.31 | 1.25 | 1.37 | <0.001 |
| 5 | 1.73 | 1.56 | 1.91 | <0.001 | 1.72 | 1.56 | 1.91 | <0.001 | 1.69 | 1.53 | 1.87 | <0.001 |
| 6 | 1.77 | 1.64 | 1.91 | <0.001 | 1.77 | 1.64 | 1.91 | <0.001 | 1.74 | 1.61 | 1.87 | <0.001 |
| 7 | 1.55 | 1.43 | 1.68 | <0.001 | 1.56 | 1.44 | 1.69 | <0.001 | 1.51 | 1.40 | 1.63 | <0.001 |
| CCI b | ||||||||||||
| 0 (reference) | 1.00 | – | – | – | 1.00 | – | – | – | 1.00 | – | – | – |
| 1 | 1.36 | 1.30 | 1.42 | <0.001 | 1.37 | 1.31 | 1.44 | <0.001 | 1.35 | 1.29 | 1.41 | <0.001 |
| 2 | 1.39 | 1.31 | 1.49 | <0.001 | 1.45 | 1.36 | 1.55 | <0.001 | 1.48 | 1.38 | 1.58 | <0.001 |
| ≧3 | 1.17 | 1.09 | 1.25 | <0.001 | 1.24 | 1.16 | 1.33 | <0.001 | 1.29 | 1.21 | 1.38 | <0.001 |
| Adults’ preventive care service | ||||||||||||
| No (reference) | 1.00 | – | – | – | 1.00 | – | – | – | 1.00 | – | – | – |
| Yes | 2.61 | 2.55 | 2.68 | <0.001 | 2.56 | 2.49 | 2.62 | <0.001 | 2.49 | 2.43 | 2.56 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inchai, P.; Tsai, W.-C.; Chiu, L.-T.; Kung, P.-T. Inequality in the Utilization of Breast Cancer Screening between Women with and without Disabilities in Taiwan: A Propensity-Score-Matched Nationwide Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 5280. https://doi.org/10.3390/ijerph19095280
Inchai P, Tsai W-C, Chiu L-T, Kung P-T. Inequality in the Utilization of Breast Cancer Screening between Women with and without Disabilities in Taiwan: A Propensity-Score-Matched Nationwide Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(9):5280. https://doi.org/10.3390/ijerph19095280
Chicago/Turabian StyleInchai, Puchong, Wen-Chen Tsai, Li-Ting Chiu, and Pei-Tseng Kung. 2022. "Inequality in the Utilization of Breast Cancer Screening between Women with and without Disabilities in Taiwan: A Propensity-Score-Matched Nationwide Cohort Study" International Journal of Environmental Research and Public Health 19, no. 9: 5280. https://doi.org/10.3390/ijerph19095280
APA StyleInchai, P., Tsai, W.-C., Chiu, L.-T., & Kung, P.-T. (2022). Inequality in the Utilization of Breast Cancer Screening between Women with and without Disabilities in Taiwan: A Propensity-Score-Matched Nationwide Cohort Study. International Journal of Environmental Research and Public Health, 19(9), 5280. https://doi.org/10.3390/ijerph19095280