
Metabolic, Oxidative and Psychological Stress as Mediators of the Effect of COVID-19 on Male Infertility: A Literature Review



{kind=link}
{kind=link}
Abstract
:1. Introduction
2. SARS-CoV-2 and Male Infertility
2.1. SARS-CoV-2 and Testosterone
2.2. SARS-CoV-2 and Semen
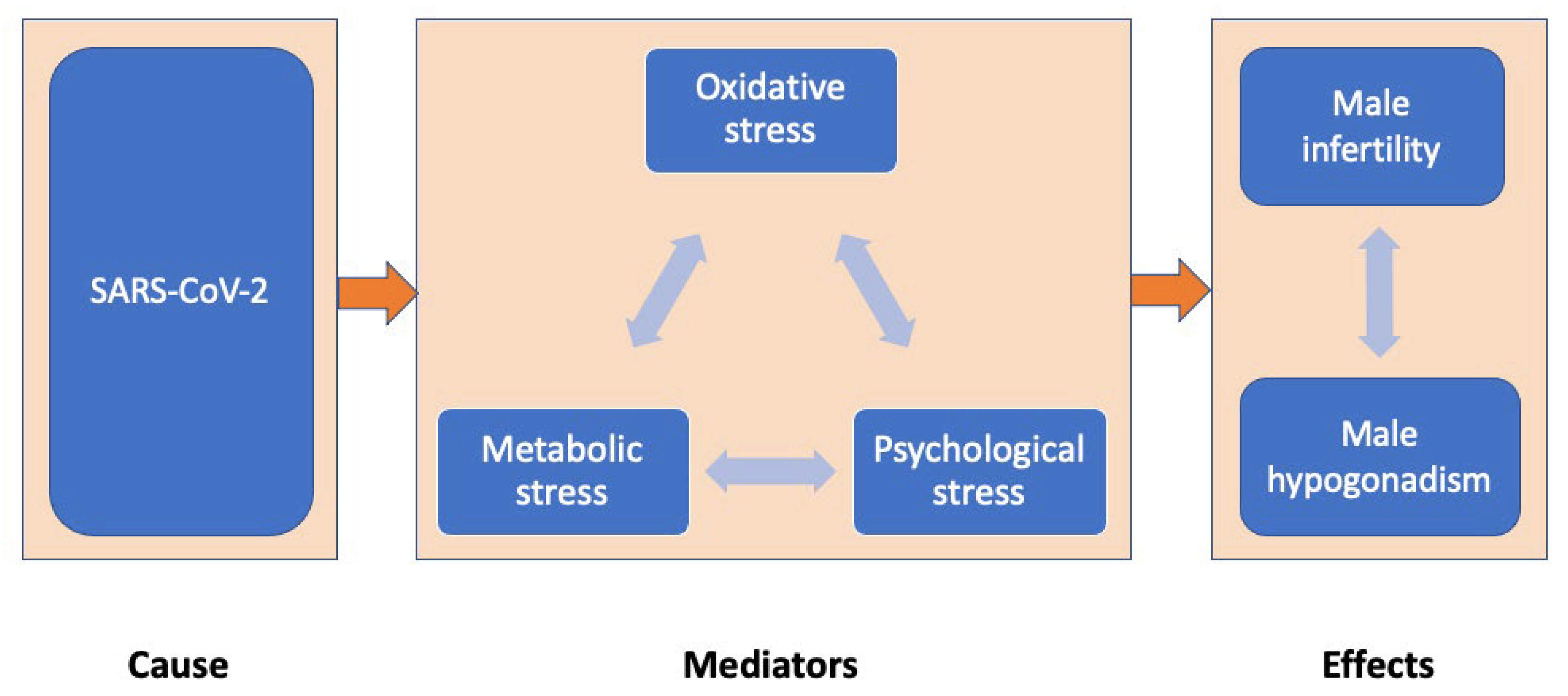
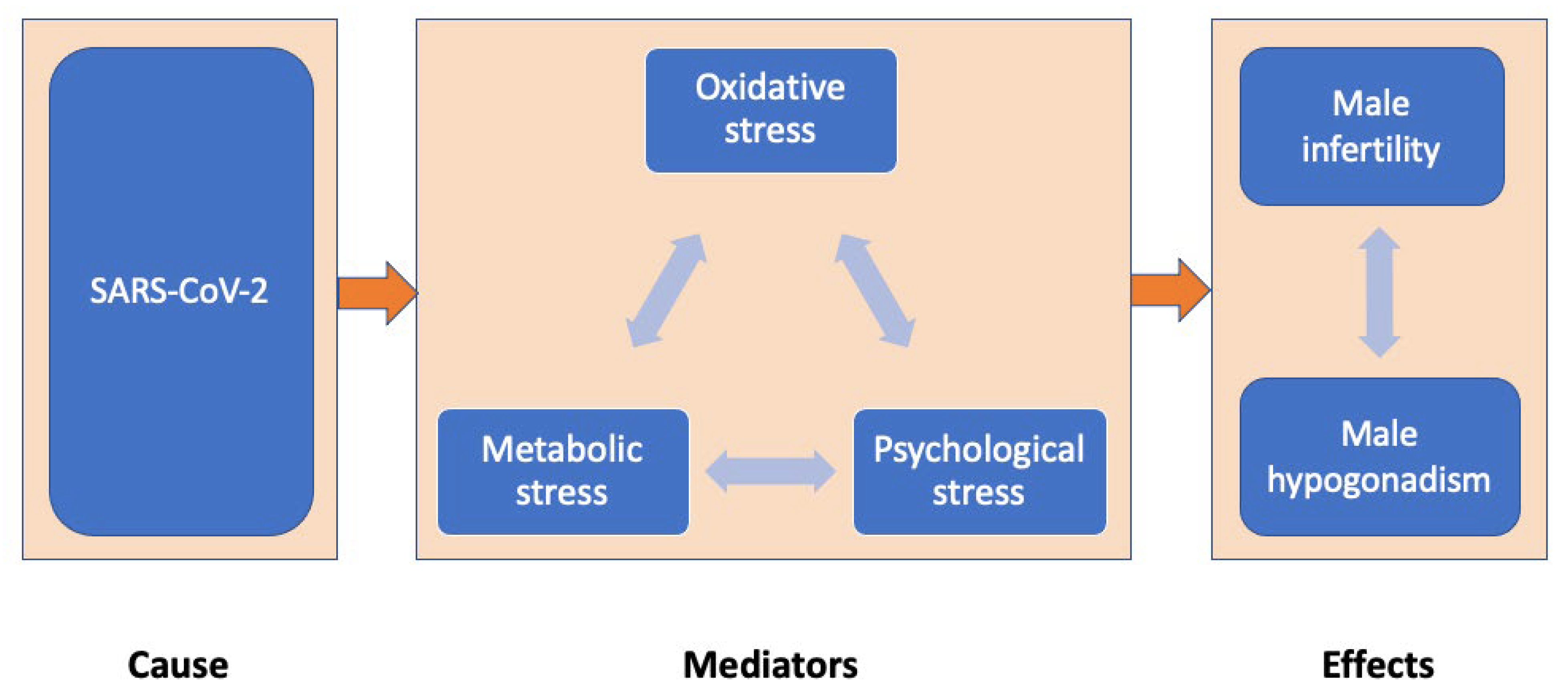
3. Possible Mediators of SARS-CoV-2 Impact on Male Infertility
3.1. Oxidative Stress
3.2. Metabolic Stress
3.3. Psychological Stress
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Tsang, H.F.; Chan, L.W.C.; Cho, W.C.S.; Yu, A.C.S.; Yim, A.K.Y.; Chan, A.K.C.; Ng, L.P.W.; Wong, Y.K.E.; Pei, X.M.; Li, M.J.W.; et al. An update on COVID-19 pandemic: The epidemiology, pathogenesis, prevention and treatment strategies. Expert Rev. Anti-Infect. Ther. 2021, 19, 877–888. [Google Scholar] [CrossRef] [PubMed]
- Max, R. COVID-19 Cases throughout the World. 2022. Available online: https://ourworldindata.org/covid-cases (accessed on 1 March 2022).
- Tabatabaeizadeh, S.A. Airborne transmission of COVID-19 and the role of face mask to prevent it: A systematic review and meta-analysis. Eur. J. Med. Res. 2021, 26, 1. [Google Scholar] [CrossRef] [PubMed]
- Amirfakhryan, H.; Safari, F. Outbreak of SARS-CoV2: Pathogenesis of infection and cardiovascular involvement. Hell. J. Cardiol. 2021, 62, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Umakanthan, S.; Sahu, P.; Ranade, A.V.; Bukelo, M.M.; Rao, J.S.; Abrahao-Machado, L.F.; Dahal, S.; Kumar, H.; Kv, D. Origin, transmission, diagnosis and management of coronavirus disease 2019 (COVID-19). Postgrad. Med. J. 2020, 96, 753–758. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Gallo Marin, B.; Aghagoli, G.; Lavine, K.; Yang, L.; Siff, E.J.; Chiang, S.S.; Salazar-Mather, T.P.; Dumenco, L.; Savaria, M.C.; Aung, S.N.; et al. Predictors of COVID-19 severity: A literature review. Rev. Med. Virol. 2021, 31, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.M.; Bai, P.; He, W.; Wu, F.; Liu, X.F.; Han, D.M.; Liu, S.; Yang, J.K. Gender Differences in Patients With COVID-19: Focus on Severity and Mortality. Front. Public Health 2020, 8, 152. [Google Scholar] [CrossRef]
- Bienvenu, L.A.; Noonan, J.; Wang, X.; Peter, K. Higher mortality of COVID-19 in males: Sex differences in immune response and cardiovascular comorbidities. Cardiovasc. Res. 2020, 116, 2197–2206. [Google Scholar] [CrossRef]
- Nimgaonkar, I.; Valeri, L.; Susser, E.; Hussain, S.; Sunderram, J.; Aviv, A. The age pattern of the male-to-female ratio in mortality from COVID-19 mirrors that of cardiovascular disease in the general population. Aging 2021, 13, 3190–3201. [Google Scholar] [CrossRef]
- Aitken, R.J. COVID-19 and male infertility: An update. Andrology 2022, 10, 8–10. [Google Scholar] [CrossRef]
- Evans, E.P.P.; Scholten, J.T.M.; Mzyk, A.; Reyes-San-Martin, C.; Llumbet, A.E.; Hamoh, T.; Arts, E.G.J.M.; Schirhagl, R.; Cantineau, A.E.P. Male subfertility and oxidative stress. Redox Biol. 2021, 46, 102071. [Google Scholar] [CrossRef]
- Castellini, C.; D’andrea, S.; Cordeschi, G.; Totaro, M.; Parisi, A.; Di Emidio, G.; Tatone, C.; Francavilla, S.; Barbonetti, A. Pathophysiology of mitochondrial dysfunction in human spermatozoa: Focus on energetic metabolism, oxidative stress and apoptosis. Antioxidants 2021, 10, 695. [Google Scholar] [CrossRef]
- Vander Borght, M.; Wyns, C. Fertility and infertility: Definition and epidemiology. Clin. Biochem. 2018, 62, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Perheentupa, A.; Huhtaniemi, I. Aging of the human ovary and testis. Mol. Cell. Endocrinol. 2009, 299, 2–13. [Google Scholar] [CrossRef] [PubMed]
- Heinrich, A.; DeFalco, T. Essential roles of interstitial cells in testicular development and function. Andrology 2020, 8, 903–914. [Google Scholar] [CrossRef] [Green Version]
- Albrecht, M. Insights into the nature of human testicular peritubular cells. Ann. Anat.-Anat. Anz. 2009, 191, 532–540. [Google Scholar] [CrossRef] [PubMed]
- Foster, R.A. CHAP TER 5 Male Genital System. Jubb Kennedy Palmer’s Pathol. Domest. Anim. 2016, 3, 465–510.e1. [Google Scholar] [CrossRef]
- Bräuner, E.V.; Nordkap, L.; Priskorn, L.; Hansen, Å.M.; Bang, A.K.; Holmboe, S.A.; Schmidt, L.; Jensen, T.K.; Jørgensen, N. Psychological stress, stressful life events, male factor infertility, and testicular function: A cross-sectional study. Fertil. Steril. 2020, 113, 865–875. [Google Scholar] [CrossRef]
- Al-kuraishy, H.M.; Al-Gareeb, A.I.; Faidah, H.; Alexiou, A.; Batiha, G.E.S. Testosterone in COVID-19: An Adversary Bane or Comrade Boon. Front. Cell. Infect. Microbiol. 2021, 11, 832. [Google Scholar] [CrossRef]
- Collins, A.B.; Zhao, L.; Zhu, Z.; Givens, N.T.; Bai, Q.; Wakefield, M.R.; Fang, Y. Impact of COVID-19 on Male Fertility. Urology 2022, in press. [Google Scholar] [CrossRef]
- Mohamed, M.S.; Moulin, T.C.; Schiöth, H.B. Sex differences in COVID-19: The role of androgens in disease severity and progression. Endocrine 2021, 71, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Khalili, M.A.; Leisegang, K.; Majzoub, A.; Finelli, R.; Selvam, M.K.P.; Henkel, R.; Mojgan, M.; Agarwal, A. Male fertility and the COVID-19 pandemic: Systematic review of the literature. World J. Men’s Health 2020, 38, 506. [Google Scholar] [CrossRef] [PubMed]
- Salonia, A.; Pontillo, M.; Capogrosso, P.; Gregori, S.; Tassara, M.; Boeri, L.; Carenzi, C.; Abbate, C.; Cignoli, D.; Ferrara, A.M.; et al. Severely low testosterone in males with COVID-19: A case-control study. Andrology 2021, 9, 1043–1052. [Google Scholar] [CrossRef] [PubMed]
- Cinislioglu, A.E.; Cinislioglu, N.; Demirdogen, S.O.; Sam, E.; Akkas, F.; Altay, M.S.; Utlu, M.; Sen, I.A.; Yildirim, F.; Kartal, S.; et al. The relationship of serum testosterone levels with the clinical course and prognosis of COVID-19 disease in male patients: A prospective study. Andrology 2022, 10, 24–33. [Google Scholar] [CrossRef]
- Camici, M.; Zuppi, P.; Lorenzini, P.; Scarnecchia, L.; Pinetti, C.; Cicallini, S.; Nicastry, E.; Petrosillo, N.; Palmieri, F.; D’Offizi, G.; et al. Role of testosterone in SARS-CoV-2 infection: A key pathogenic factor and a biomarker for severe pneumonia. Int. J. Infect. Dis. 2021, 108, 244–251. [Google Scholar] [CrossRef]
- Dhindsa, S.; Zhang, N.; McPhaul, M.J.; Wu, Z.; Ghoshal, A.K.; Erlich, E.C.; Mani, K.; Randolph, G.J.; Edwards, J.R.; Mudd, P.A.; et al. Association of circulating sex hormones with inflammation and disease severity in patients with COVID-19. JAMA Netw. Open 2021, 4, e2111398. [Google Scholar] [CrossRef]
- Lanser, L.; Burkert, F.R.; Thommes, L.; Egger, A.; Hoermann, G.; Kaser, S.; Pinggera, G.M.; Anliker, M.; Griesmacher, A.; Weiss, G.; et al. Testosterone Deficiency Is a Risk Factor for Severe COVID-19. Front. Endocrinol. 2021, 12, 731. [Google Scholar] [CrossRef]
- Rastrelli, G.; Di Stasi, V.; Inglese, F.; Beccaria, M.; Garuti, M.; Di Costanzo, D.; Spreafico, F.; Greco, G.F.; Cervi, G.; Pecoriello, A.; et al. Low testosterone levels predict clinical adverse outcomes in SARS-CoV-2 pneumonia patients. Andrology 2021, 9, 88–98. [Google Scholar] [CrossRef]
- Salonia, A.; Corona, G.; Giwercman, A.; Maggi, M.; Minhas, S.; Nappi, R.E.; Sofikitis, N.; Vignozzi, L. SARS-CoV-2, testosterone and frailty in males (PROTEGGIMI): A multidimensional research project. Andrology 2021, 9, 19–22. [Google Scholar] [CrossRef]
- Al-Lami, R.A.; Urban, R.J.; Volpi, E.; Algburi, A.M.A.; Baillargeon, J. Sex Hormones and Novel Corona Virus Infectious Disease (COVID-19). Mayo Clin. Proc. 2020, 95, 1710–1714. [Google Scholar] [CrossRef]
- Kumar, N.; Zuo, Y.; Yalavarthi, S.; Hunker, K.L.; Knight, J.S.; Kanthi, Y.; Obi, A.T.; Ganesh, S.K. SARS-CoV-2 spike protein s1-mediated endothelial injury and pro-inflammatory state is amplified by dihydrotestosterone and prevented by mineralocorticoid antagonism. Viruses 2021, 13, 2209. [Google Scholar] [CrossRef] [PubMed]
- Swerdloff, R.S.; Dudley, R.E.; Page, S.T.; Wang, C.; Salameh, W.A. Dihydrotestosterone: Biochemistry, physiology, and clinical implications of elevated blood levels. Endocr. Rev. 2017, 38, 220–254. [Google Scholar] [CrossRef] [PubMed]
- Salam, A.P.; Horby, P.W. The breadth of viruses in human semen. Emerg. Infect. Dis. 2017, 23, 1922–1924. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Zhao, S.; Li, W.; Wang, Y.; Li, L.; Jiang, S.; Ren, W.; Yuan, Q.; Zhang, F.; Kong, F.; et al. Absence of SARS-CoV-2 in semen of a COVID-19 patient cohort. Andrology 2021, 9, 42–47. [Google Scholar] [CrossRef]
- Pan, F.; Xiao, X.; Guo, J.; Song, Y.; Li, H.; Patel, D.; Spivak, A.; Alukal, J.; Zhang, X.; Xiong, C.; et al. No evidence of SARS-CoV-2 in semen of males recovering from COVID-19. Fertil Steril 2020, 113, 1135–1139. [Google Scholar] [CrossRef]
- Best, J.C.; Kuchakulla, M.; Khodamoradi, K.; Lima, T.F.N.; Frech, F.S.; Achua, J.; Rosete, O.; Mora, B.; Arora, H.; Ibrahim, E.; et al. Evaluation of SARS-CoV-2 in human semen and effect on total sperm number: A prospective observational study. World J. Men’s Health 2021, 39, 489–495. [Google Scholar] [CrossRef]
- Burke, C.A.; Skytte, A.; Kasiri, S.; Howell, D.; Patel, Z.P.; Trolice, M.P.; Parekattil, S.J.; Michael, S.F.; Paul, L.M. A cohort study of men infected with COVID-19 for presence of SARS-CoV-2 virus in their semen. J. Assist. Reprod. Genet. 2021, 38, 785–789. [Google Scholar] [CrossRef]
- Sharma, A.P.; Sahoo, S.; Goyal, K.; Chandna, A.; Kirubanandhan, S.; Sharma, V.; Grover, S.; Singh, M.P.; Bhalla, A.; Singh, S.K. Absence of SARS-CoV-2 infection in the semen of men recovering from COVID-19 infection: An exploratory study and review of literature. Andrologia 2021, 53, e14136. [Google Scholar] [CrossRef]
- Ruan, Y.; Hu, B.; Liu, Z.; Liu, K.; Jiang, H.; Li, H.; Li, R.; Luan, Y.; Liu, X.; Yu, G.; et al. No detection of SARS-CoV-2 from urine, expressed prostatic secretions, and semen in 74 recovered COVID-19 male patients: A perspective and urogenital evaluation. Andrology 2021, 9, 99–106. [Google Scholar] [CrossRef]
- Li, D.; Jin, M.; Bao, P.; Zhao, W.; Zhang, S. Clinical Characteristics and Results of Semen Tests Among Men With Coronavirus Disease 2019. JAMA Netw. Open 2020, 3, e208292. [Google Scholar] [CrossRef]
- Delaroche, L.; Bertine, M.; Oger, P.; Descamps, D.; Damond, F.; Genauzeau, E.; Meicler, P.; Le Hingrat, Q.; Lamazou, F.; Gschwind, R.; et al. Evaluation of SARS-CoV-2 in semen, seminal plasma, and spermatozoa pellet of COVID-19 patients in the acute stage of infection. PLoS ONE 2021, 16, e0260187. [Google Scholar] [CrossRef] [PubMed]
- Saylam, B.; Uguz, M.; Yarpuzlu, M.; Efesoy, O.; Akbay, E.; Çayan, S. The presence of SARS-CoV-2 virus in semen samples of patients with COVID-19 pneumonia. Andrologia 2021, 53, e14145. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Yuan, X.; Wu, L.; Guo, N.; Yin, L.; Li, Y. COVID-19 and male reproduction: Current research and unknown factors. Andrology 2021, 9, 1027–1037. [Google Scholar] [CrossRef] [PubMed]
- Cai, T.; Mao, G.; Zheng, R.; Fang, M.; Yang, X.; Wang, L.; Qi, C. Testicular injury during SARS-CoV-2 infection may be neglected: An assessment from scRNA-seq profiling and protein detection of angiotensin-converting enzyme II. Exp. Ther. Med. 2021, 22, 1485. [Google Scholar] [CrossRef]
- Yang, M.; Chen, S.; Huang, B.; Jhong, J.M.; Su, H.; Chen, Y.J.; Cao, Q.; Ma, L.; He, J.; Li, X.F.; et al. Pathological Findings in the Testes of COVID-19 Patients: Clinical Implications. Eur. Urol. Focus 2020, 6, 1124–1129. [Google Scholar] [CrossRef]
- Achua, J.K.; Chu, K.Y.; Ibrahim, E.; Khodamoradi, K.; Delma, K.S.; Iakymenko, O.A.; Kryvenko, O.N.; Arora, H.; Ramasamy, R. Histopathology and ultrastructural findings of fatal COVID-19 infections on testis. World J. Men’s Health 2020, 39, 65–74. [Google Scholar] [CrossRef]
- Omolaoye, T.S.; Adeniji, A.A.; Cardona, W.D.; du Plessis, S.S. SARS-CoV-2 (COVID-19) and male fertility: Where are we? Reprod. Toxicol. 2021, 99, 65–70. [Google Scholar] [CrossRef]
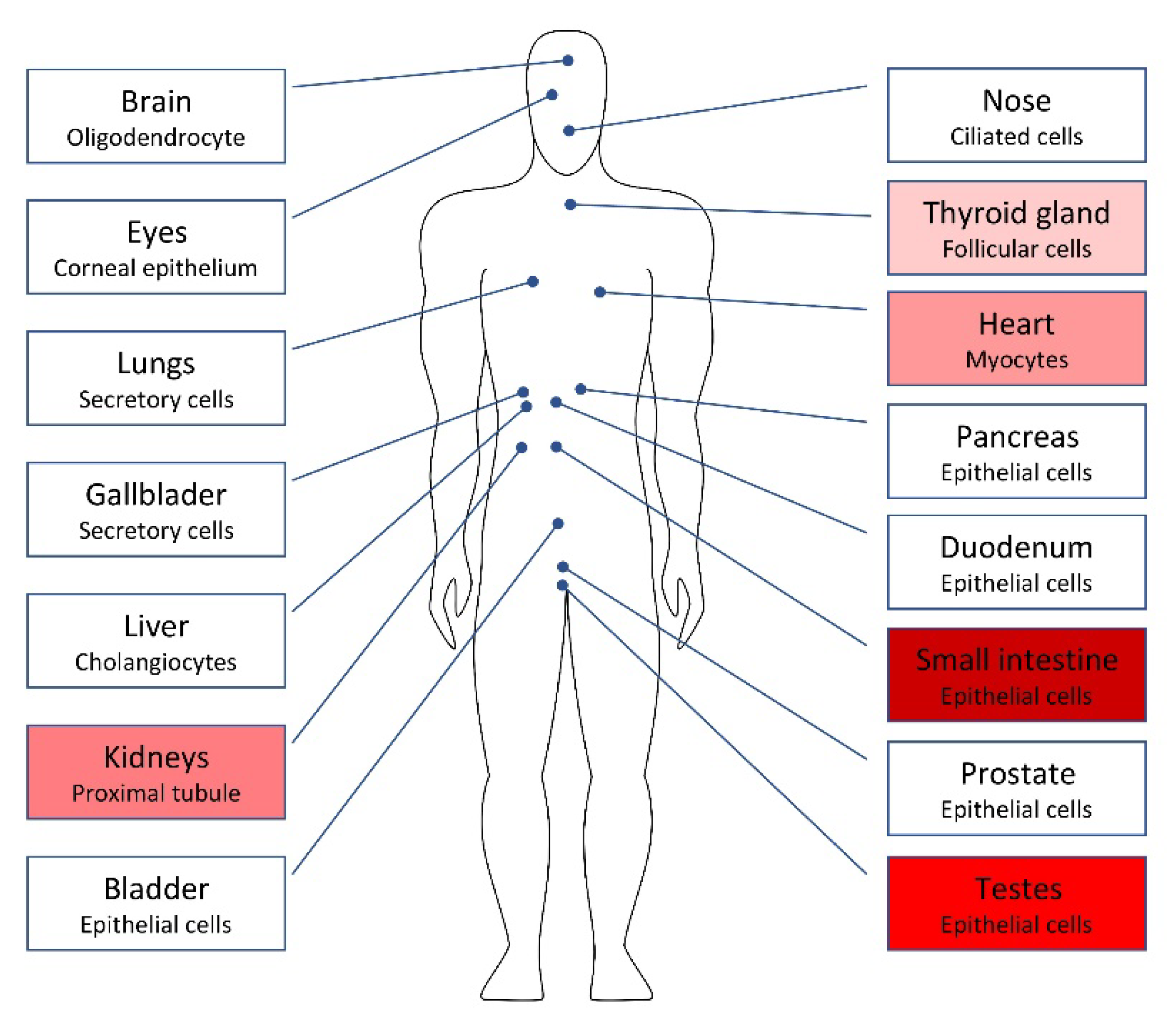
- Radzikowska, U.; Ding, M.; Tan, G.; Zhakparov, D.; Peng, Y.; Wawrzyniak, P.; Wang, M.; Li, S.; Morita, H.; Altunbulakli, C.; et al. Distribution of ACE2, CD147, CD26, and other SARS-CoV-2 associated molecules in tissues and immune cells in health and in asthma, COPD, obesity, hypertension, and COVID-19 risk factors. Allergy 2020, 75, 2829–2845. [Google Scholar] [CrossRef]
- Liu, S.; Han, L.; Li, J.; Li, H. Electrochemical detection of ACE2 as a biomarker for diagnosis of COVID-19 and potential male infertility. Biosens. Bioelectron. 2022, 198, 113788. [Google Scholar] [CrossRef]
- Shen, Q.; Xiao, X.; Aierken, A.; Yue, W.; Wu, X.; Liao, M.; Hua, J. The ACE2 expression in Sertoli cells and germ cells may cause male reproductive disorder after SARS-CoV-2 infection. J. Cell. Mol. Med. 2020, 24, 9472–9477. [Google Scholar] [CrossRef]
- Donders, G.G.; Bosmans, E.; Reumers, J.; Donder, F.; Jonckheere, J.; Salembier, G.; Stern, N.; Jacqyemyn, Y.; Ombelet, W.; Depuydt, C.E. Sperm quality and absence of SARS-CoV-2 RNA in semen after COVID-19 infection: A prospective, observational study and validation of the SpermCOVID test. Fertil Steril 2020, 117, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Gacci, M.; Coppi, M.; Baldi, E.; Sebastianelli, A.; Zaccaro, C.; Morselli, S.; Pecoraro, A.; Manera, A.; Nicoletti, R.; Liaci, A.; et al. Semen impairment and occurrence of SARS-CoV-2 virus in semen after recovery from COVID-19. Hum. Reprod. 2021, 36, 1520–1529. [Google Scholar] [CrossRef] [PubMed]
- Hadi, M.; Abdelhamid, M.; Fellah, A.A.; Elmarghani, A. An Assessment of Men Semen Alterations in SARS-CoV-2: Is Fever the Principal Concern? Reprod. Sci. 2022. Published Online First. [Google Scholar] [CrossRef]
- Hayashi, T.; Miyata, A.; Yamada, T. The impact of commonly prescribed drugs on male fertility. Hum. Fertil 2008, 11, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Hamarat, M.B.; Ozkent, M.S.; Yilmaz, B.; Aksanyar, S.Y.; Karabacak, K. Effect of SARS-CoV-2 infection on semen parameters. Can. Urol. Assoc. J. 2021, 16, 173–177. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Wang, J.; Ren, J.; Zhao, Y.; Chen, J.; Chen, X. Effect of COVID-19 on Male Reproductive System—A Systematic Review. Front. Endocrinol. 2021, 12, 677701. [Google Scholar] [CrossRef] [PubMed]
- Banihani, S.A. Human semen quality as affected by SARS-CoV-2 infection: An up-to-date review. Andrologia 2021, 54, e14295. [Google Scholar] [CrossRef]
- Sengupta, P.; Leisegang, K.; Agarwal, A. The impact of COVID-19 on the male reproductive tract and fertility: A systematic review. Arab J. Urol. 2021, 19, 423–436. [Google Scholar] [CrossRef]
- Corona, G.; Baldi, E.; Isidori, A.M.; Paoli, D.; Pallotti, F.; De Santis, L.; Francavilla, F.; La Vignera, S.; Selice, R.; Caponecchia, L.; et al. SARS-CoV-2 infection, male fertility and sperm cryopreservation: A position statement of the Italian Society of Andrology and Sexual Medicine (SIAMS) (Società Italiana di Andrologia e Medicina della Sessualità). J. Endocrinol. Investig. 2020, 43, 1153–1157. [Google Scholar] [CrossRef]
- Kumar, V.; Kaur, M. COVID-19 Vaccine and Male Fertility. Urol. J. 2021, 18, 6897. [Google Scholar] [CrossRef]
- Reschini, M.; Pagliardini, L.; Boeri, L.; Piazzini, F.; Bandini, V.; Fornelli, G.; Dolci, C.; Cermisoni, G.C.; Viganò, P.; Somigliana, E.; et al. COVID-19 Vaccination Does Not Affect Reproductive Health Parameters in Men. Front. Public Health 2022, 10, 839967. [Google Scholar] [CrossRef]
- Berry, S.D.; Johnson, K.S.; Myles, L.; Herndon, L.; Montoya, A.; Fashaw, S.; Gifford, D. Lessons learned from frontline skilled nursing facility staff regarding COVID-19 vaccine hesitancy. J. Am. Geriatr. Soc. 2021, 69, 1140–1146. [Google Scholar] [CrossRef]
- Lifshitz, D.; Haas, J.; Lebovitz, O.; Raviv, G.; Orvieto, R.; Aizer, A. Does mRNA SARS-CoV-2 vaccine detrimentally affect male fertility, as reflected by semen analysis? Reprod. Biomed. Online 2022, 44, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Dutta, S.; Sengupta, P. SARS-CoV-2 and Male Infertility: Possible Multifaceted Pathology. Reprod. Sci. 2021, 28, 23–26. [Google Scholar] [CrossRef]
- Haghpanah, A.; Masjedi, F.; Alborzi, S.; Hosseinpour, A.; Dehghani, A.; Malekmakan, L.; Roozbeh, J. Potential mechanisms of SARS-CoV-2 action on male gonadal function and fertility: Current status and future prospects. Andrologia 2021, 53, e13883. [Google Scholar] [CrossRef] [PubMed]
- Morselli, S.; Sebastianelli, A.; Liaci, A.; Zaccaro, C.; Pecoraro, A.; Nicoletti, R.; Manera, A.; Bisegna, C.; Campi, R.; Pollini, S.; et al. Male reproductive system inflammation after healing from coronavirus disease 2019. Andrology 2021. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Gu, L.; Ren, X.; Liu, Y.; Qian, K.; Lan, R.; Wang, T.; Jin, L.; Yang, J.; Liu, J. Prediction model for clinical pregnancy for ICSI after surgical sperm retrieval in different types of azoospermia. Hum. Reprod. 2020, 35, 1972–1982. [Google Scholar] [CrossRef]
- Moghimi, N.; Eslami Farsani, B.; Ghadipasha, M.; Mahmoudiasl, G.R.; Piryaei, A.; Aliaghaei, A.; Abdi, S.; Abbaszadeh, H.A.; Abdollahifar, M.A.; Forozesh, M. COVID-19 disrupts spermatogenesis through the oxidative stress pathway following induction of apoptosis. Apoptosis 2021, 26, 415–430. [Google Scholar] [CrossRef]
- Maleki, B.H.; Tartibian, B. COVID-19 and male reproductive function: A prospective, longitudinal cohort study. Reproduction 2021, 161, 319–331. [Google Scholar] [CrossRef]
- Falahieh, F.M.; Zarabadipour, M.; Mirani, M.; Abdiyan, M.; DInparvar, M.; Alizadeh, H.; Paktinat, S.; Hosseinirad, H. Effects of moderate COVID-19 infection on semen oxidative status and parameters 14 and 120 days after diagnosis. Reprod. Fertil Dev. 2021, 33, 683–690. [Google Scholar] [CrossRef]
- Ekholm, M.; Kahan, T. The Impact of the Renin-Angiotensin-Aldosterone System on Inflammation, Coagulation, and Atherothrombotic Complications, and to Aggravated COVID-19. Front. Pharmacol. 2021, 12, 1534. [Google Scholar] [CrossRef] [PubMed]
- Sengupta, P.; Dutta, S. Does SARS-CoV-2 infection cause sperm DNA fragmentation? Possible link with oxidative stress. Eur. J. Contracept. Reprod. Health Care 2020, 25, 405–406. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Li, L.; Zhang, Y.; Wang, X. An Investigation of the Expression of 2019 Novel Coronavirus Cell Receptor Gene ACE2 in a Wide Variety of Human Tissues. Infect. Dis. Poverty 2020, 9, 1–7. [Google Scholar]
- Gadotti, A.C.; Lipinski, A.L.; Vasconcellos, F.T.; Marqueze, L.F.; Cunha, E.B.; Campos, A.C.; Oliveira, C.F.; Amaral, A.N.; Baena, C.P.; Telles, J.P.; et al. Susceptibility of the patients infected with SARS-CoV-2 to oxidative stress and possible interplay with severity of the disease. Free Radic. Biol. Med. 2021, 165, 184–190. [Google Scholar] [CrossRef]
- Silva, N.D.J.; Ribeiro-Silva, R.D.C.; Ferreira, A.J.F.; Teixeira, C.S.S.; Rocha, A.S.; Alves, F.J.O.; Falcão, I.R.; Pinto, E.D.J.; Santos, C.A.D.S.T.; Fiaccone, R.L.; et al. Combined association of obesity and other cardiometabolic diseases with severe COVID-19 outcomes: A nationwide cross-sectional study of 21 773 Brazilian adult and elderly inpatients. BMJ Open 2021, 11, e050739. [Google Scholar] [CrossRef]
- Hayden, M.R. An Immediate and Long-Term Complication of COVID-19 May Be Type 2 Diabetes Mellitus: The Central Role of β-Cell Dysfunction, Apoptosis and Exploration of Possible Mechanisms. Cells 2020, 9, 2475. [Google Scholar] [CrossRef]
- Kahn, B.E.; Brannigan, R.E. Obesity and male infertility. Curr. Opin. Urol. 2017, 27, 441–445. [Google Scholar] [CrossRef]
- Dafallah Albashir, A.A. The potential impacts of obesity on COVID-19. Clin. Med. 2020, 20, E109–E113. [Google Scholar] [CrossRef]
- Lakhan, R.; Agrawal, A.; Sharma, M. Prevalence of Depression, Anxiety, and Stress during COVID-19 Pandemic. J. Neurosci. Rural Pract. 2020, 11, 519–525. [Google Scholar] [CrossRef]
- Abel, K.M.; Carr, M.J.; Ashcroft, D.M.; Chalder, T.; Chew-Graham, C.A.; Hope, H.; Kapur, N.; McManus, S.; Steeg, S.; Webb, R.T.; et al. Association of SARS-CoV-2 Infection with Psychological Distress, Psychotropic Prescribing, Fatigue, and Sleep Problems among UK Primary Care Patients. JAMA Netw. Open 2021, 4, e2134803. [Google Scholar] [CrossRef]
- Stefano, G.B.; Ptacek, R.; Ptackova, H.; Martin, A.; Kream, R.M. Selective neuronal mitochondrial targeting in SARS-CoV-2 infection affects cognitive processes to induce ‘Brain Fog’ and results in behavioral changes that favor viral survival. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2021, 27, e930886-1. [Google Scholar] [CrossRef] [PubMed]
- Gopal, A.B.; Chakraborty, S.; Padhan, P.K.; Barik, A.; Dixit, P.; Chakraborty, D.; Poirah, I.; Samal, S.; Sarkar, A.; Bhattacharyya, A. Silent hypoxia in COVID-19: A gut microbiota connection. Curr. Opin. Physiol. 2021, 23, 100456. [Google Scholar] [CrossRef] [PubMed]
- Kolbasi, B.; Bulbul, M.V.; Karabulut, S.; Altun, C.E.; Cakici, C.; Ulfer, G.; Mudok, T.; Keskin, I. Chronic unpredictable stress disturbs the blood–testis barrier affecting sperm parameters in mice. Reprod. Biomed. Online 2021, 42, 983–995. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Li, Z.; Wang, G.; Wang, H.; Zhou, Y.; Zhao, X.; Cheng, C.Y.; Qiao, Y.; Sun, F. Sperm epigenetic alterations contribute to inter- and transgenerational effects of paternal exposure to long-term psychological stress via evading offspring embryonic reprogramming. Cell Discov. 2021, 7, 101. [Google Scholar] [CrossRef]
- Micelli, E.; Cito, G.; Cocci, A.; Polloni, G.; Russo, G.I.; Minervini, A.; Carini, M.; Natali, A.; Coccia, M.E. Desire for parenthood at the time of COVID-19 pandemic: An insight into the Italian situation. J. Psychosom. Obstet. Gynecol. 2020, 41, 183–190. [Google Scholar] [CrossRef]
- Madjunkov, M.; Dviri, M.; Librach, C. A comprehensive review of the impact of COVID-19 on human reproductive biology, assisted reproduction care and pregnancy: A Canadian perspective. J. Ovarian Res. 2020, 13, 140. [Google Scholar] [CrossRef]
- Masoudi, M.; Maasoumi, R.; Bragazzi, N.L. Effects of the COVID-19 pandemic on sexual functioning and activity: A systematic review and meta-analysis. BMC Public Health 2022, 22, 189. [Google Scholar] [CrossRef]
- Lotti, F.; Maggi, M. Sexual dysfunction and male infertility. Nat. Rev. Urol. 2018, 15, 287–307. [Google Scholar] [CrossRef]
- Gaskins, A.J.; Sundaram, R.; Buck Louis, G.M.; Chavarro, J.E. Predictors of Sexual Intercourse Frequency Among Couples Trying to Conceive. J. Sex. Med. 2018, 15, 519–528. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mintziori, G.; Duntas, L.H.; Veneti, S.; Goulis, D.G. Metabolic, Oxidative and Psychological Stress as Mediators of the Effect of COVID-19 on Male Infertility: A Literature Review. Int. J. Environ. Res. Public Health 2022, 19, 5277. https://doi.org/10.3390/ijerph19095277
Mintziori G, Duntas LH, Veneti S, Goulis DG. Metabolic, Oxidative and Psychological Stress as Mediators of the Effect of COVID-19 on Male Infertility: A Literature Review. International Journal of Environmental Research and Public Health. 2022; 19(9):5277. https://doi.org/10.3390/ijerph19095277
Chicago/Turabian StyleMintziori, Gesthimani, Leonidas H. Duntas, Stavroula Veneti, and Dimitrios G. Goulis. 2022. "Metabolic, Oxidative and Psychological Stress as Mediators of the Effect of COVID-19 on Male Infertility: A Literature Review" International Journal of Environmental Research and Public Health 19, no. 9: 5277. https://doi.org/10.3390/ijerph19095277
APA StyleMintziori, G., Duntas, L. H., Veneti, S., & Goulis, D. G. (2022). Metabolic, Oxidative and Psychological Stress as Mediators of the Effect of COVID-19 on Male Infertility: A Literature Review. International Journal of Environmental Research and Public Health, 19(9), 5277. https://doi.org/10.3390/ijerph19095277