
Correlation Analysis between Urban Elements and COVID-19 Transmission Using Social Media Data




Abstract
:1. Introduction
2. Study Area and Data
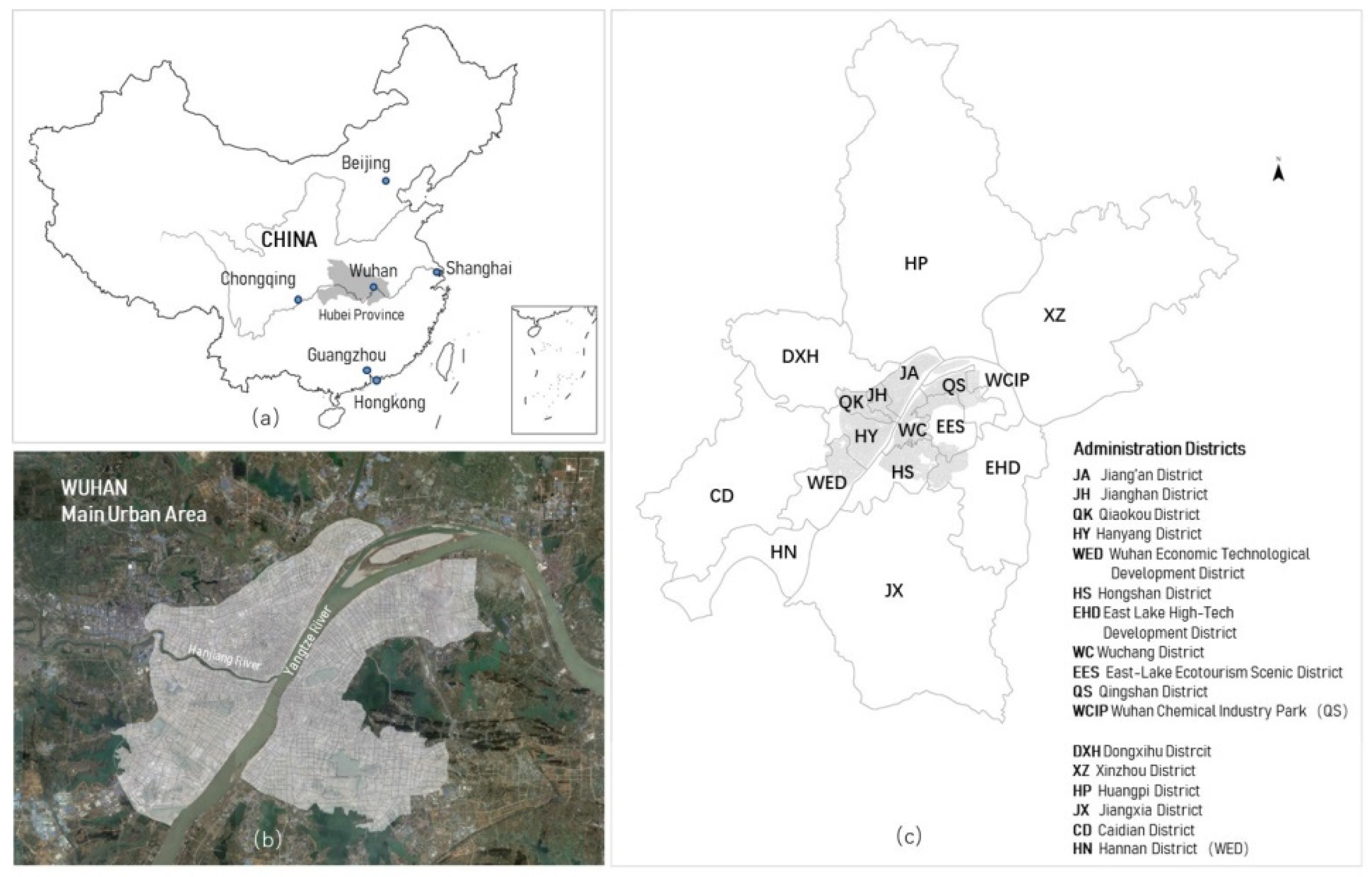
2.1. Study Area
2.2. Weibo COVID-19 Cases
2.3. Explanatory Variables
3. Methods
3.1. Kernel Density Analysis
3.2. Inverse Distance Weighted (IDW)
3.3. Multiple Linear Regression
4. Results
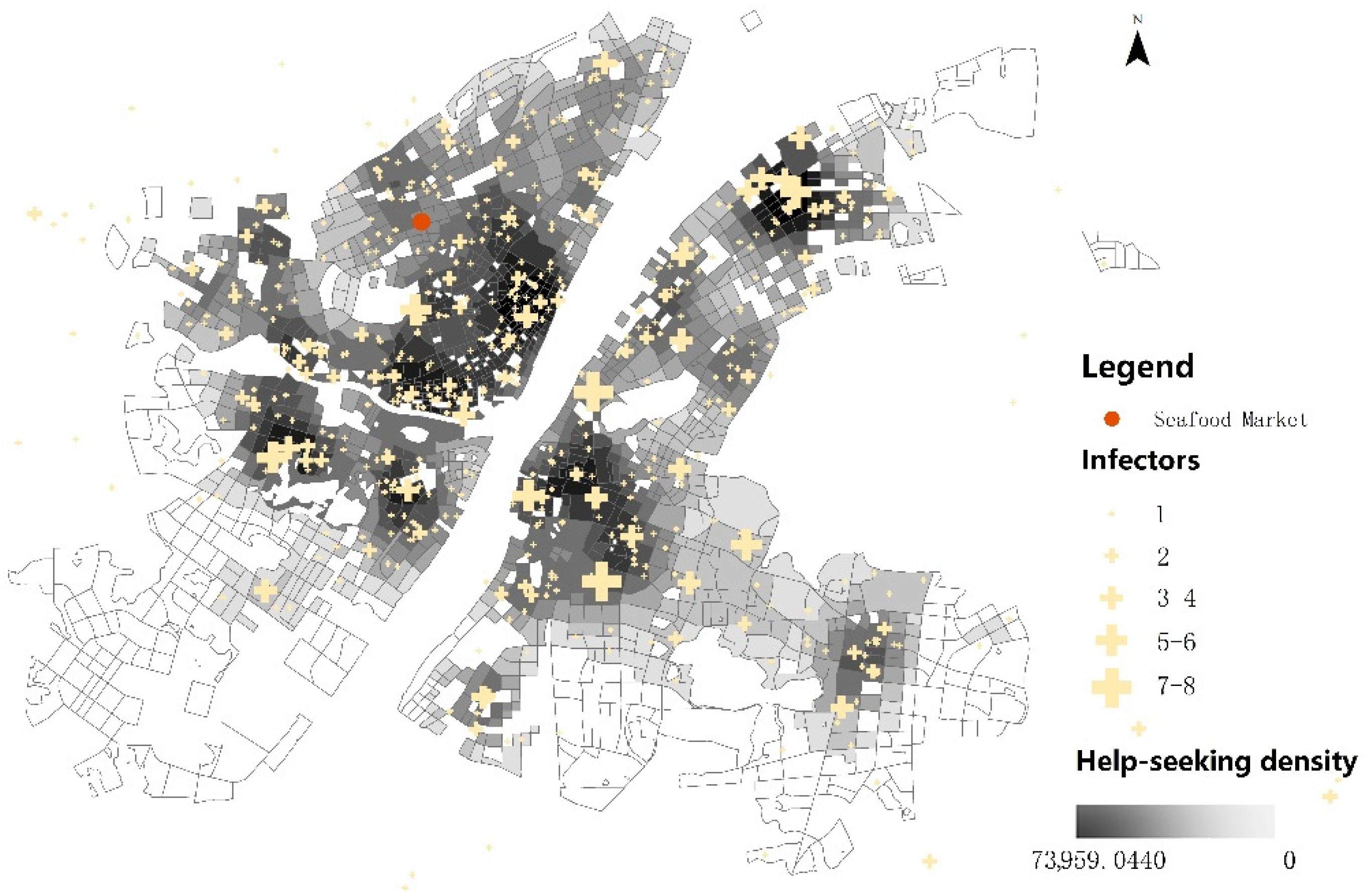
4.1. Spatial Variations of Weibo COVID-19 Cases
4.2. Correlation Analysis
4.3. Multiple Regression Model
5. Discussion
5.1. Impacts of Urban Factors on COVID-19 Transmission
5.2. Policy Recommendations for Urban Development
5.3. Future Research and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Wang, Y.; Ye, D.; Liu, Q. Review of the 2019 novel coronavirus (SARS-CoV-2) based on current evidence. Int. J. Antimicrob. Agent 2020, 55, 105948. [Google Scholar] [CrossRef]
- Lai, K.Y.; Webster, C.; Kumari, S.; Sarkar, C. The nature of cities and the COVID-19 pandemic. Curr. Opin. Environ. Sustain. 2020, 46, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Alirol, E.; Getaz, L.; Stoll, B.; Chappuis, F.; Loutan, L. Urbanisation and infectious diseases in a globalised world. Lancet Infect. Dis. 2011, 11, 131–141. [Google Scholar] [CrossRef]
- Matthew, R.A.; McDonald, B. Cities under Siege: Urban Planning and the Threat of Infectious Disease. J. Am. Plan. Assoc. 2007, 72, 109–117. [Google Scholar] [CrossRef]
- You, H.; Wu, X.; Guo, X. Distribution of COVID-19 Morbidity Rate in Association with Social and Economic Factors in Wuhan, China: Implications for Urban Development. Int. J. Environ. Res. Public Health 2020, 17, 3417. [Google Scholar] [CrossRef]
- Lai, S.; Leone, F.; Zoppi, C. COVID-19 and spatial planning. TeMA J. Land Use Mob. Environ. 2020, 231–246. [Google Scholar] [CrossRef]
- Peng, Z.; Wang, R.; Liu, L.; Wu, H. Exploring urban spatial features of COVID-19 transmission in Wuhan based on social media data. ISPRS Int. J. Geo-Inf. 2020, 9, 402. [Google Scholar] [CrossRef]
- Jin, X.; Leng, Y.; Gong, E.; Xiong, S.; Yao, Y.; Vedanthan, R.; Yang, Z.; Chen, K.; Wu, C.; Yan, L. Neighborhood-Level Public Facilities and COVID-19 Transmission: A Nationwide Geospatial Study In China. Medrxiv 2020. [Google Scholar] [CrossRef]
- Im Kampe, E.O.; Lehfeld, A.-S.; Buda, S.; Buchholz, U.; Haas, W. Surveillance of COVID-19 school outbreaks, Germany, March to August 2020. Eurosurveillance 2020, 25, 2001645. [Google Scholar] [CrossRef]
- Patel, A.; Shah, P. Rethinking slums, cities, and urban planning: Lessons from the COVID-19 pandemic. Cities Health 2020, 1–3. [Google Scholar] [CrossRef]
- Schomaker, R.M.; Bauer, M.W. What Drives Successful Administrative Performance during Crises? Lessons from Refugee Migration and the COVID-19 Pandemic. Public Admin. Rev. 2020, 80, 845–850. [Google Scholar] [CrossRef]
- Hu, R. Reinventing community in COVID-19: A case in Canberra, Australia. Soc.-Ecol. Pract. Res. 2020, 2, 237–241. [Google Scholar] [CrossRef]
- Berkowitz, R.L.; Gao, X.; Michaels, E.K.; Mujahid, M.S. Structurally vulnerable neighbourhood environments and racial/ethnic COVID-19 inequities. Cities Health 2020, 1–4. [Google Scholar] [CrossRef]
- Hu, M.; Roberts, J.D.; Azevedo, G.P.; Milner, D. The role of built and social environmental factors in COVID-19 transmission: A look at America’s capital city. Sustain. Cities Soc. 2021, 65, 102580. [Google Scholar] [CrossRef]
- Bashir, M.F.; Ma, B.; Komal, B.; Bashir, M.A.; Tan, D.; Bashir, M. Correlation between climate indicators and COVID-19 pandemic in New York, USA. Sci. Total Environ. 2020, 728, 138835. [Google Scholar] [CrossRef]
- Wu, X.; Nethery, R.C.; Sabath, B.M.; Braun, D.; Dominici, F. Air pollution and COVID-19 mortality in the United States: Strengths and limitations of an ecological regression analysis. Sci. Adv. 2020, 6, eabd4049. [Google Scholar] [CrossRef]
- Doğan, B.; Jebli, M.B.; Shahzad, K.; Farooq, T.H.; Shahzad, U. Investigating the effects of meteorological parameters on COVID-19: Case study of New Jersey, United States. Environ. Res. 2020, 191, 110148. [Google Scholar] [CrossRef]
- Kleinschroth, F.; Kowarik, I. COVID-19 crisis demonstrates the urgent need for urban greenspaces. Front. Ecol. Environ. 2020, 18, 318–319. [Google Scholar] [CrossRef]
- Pandit, N. COVID-19: Urban Density’s Poetic Justice. Ecol. Econ. Soc. INSEE J. 2020, 3, 13–18. [Google Scholar] [CrossRef]
- Global Humanitarian Response Plan COVID-19. OCHA Geneva. Available online: https://reliefweb.int/sites/reliefweb.int/files/resources/Global%20Humanitarian%20Response%20Plan%20COVID-19.pdf (accessed on 1 July 2020).
- Ma, Y.; Zhao, Y.; Liu, J.; He, X.; Wang, B.; Fu, S.; Yan, J.; Niu, J.; Zhou, J.; Luo, B. Effects of temperature variation and humidity on the death of COVID-19 in Wuhan, China. Sci. Total Environ. 2020, 724, 138226. [Google Scholar] [CrossRef] [PubMed]
- Pan, A.; Liu, L.; Wang, C.; Guo, H.; Hao, X.; Wang, Q.; Huang, J.; He, N.; Yu, H.; Lin, X.; et al. Association of Public Health Interventions with the Epidemiology of the COVID-19 Outbreak in Wuhan, China. JAMA 2020, 323, 1915–1923. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Wang, Y.; Xue, J.; Zhao, N.; Zhu, T. The impact of COVID-19 epidemic declaration on psychological consequences: A study on active Weibo users. Int. J. Environ. Res. Public Health 2020, 17, 2032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Y.; Xu, H. Chinese public attention to COVID-19 epidemic: Based on social media. medRxiv 2020, 22, e18825. [Google Scholar]
- Li, L.; Zhang, Q.; Wang, X.; Zhang, J.; Wang, T.; Gao, T.-L.; Duan, W.; Tsoi, K.K.-F.; Wang, F.-Y. Characterizing the propagation of situational information in social media during COVID-19 epidemic: A case study on weibo. IEEE Trans. Comput. Soc. Syst. 2020, 7, 556–562. [Google Scholar] [CrossRef]
- Jahanbin, K.; Rahmanian, V. Using Twitter and web news mining to predict COVID-19 outbreak. Asian Pac. J. Trop. Med. 2020, 13, 378. [Google Scholar]
- Prabhakar Kaila, D.; Prasad, D.A. Informational flow on Twitter–Corona virus outbreak–topic modelling approach. Int. J. Adv. Res. Eng. Technol. 2020, 11, 128–134. [Google Scholar]
- Tisdell, C.A. Economic, social and political issues raised by the COVID-19 pandemic. Econ. Anal. Policy 2020, 68, 17–28. [Google Scholar] [CrossRef]
- Li, B.; Peng, Y.; He, H.; Wang, M.; Feng, T. Built environment and early infection of COVID-19 in urban districts: A case study of Huangzhou. Sustain. Cities Soc. 2021, 66, 102685. [Google Scholar] [CrossRef]
- Li, S.; Ma, S.; Zhang, J. Association of built environment attributes with the spread of COVID-19 at its initial stage in China. Sustain. Cities Soc. 2021, 67, 102752. [Google Scholar] [CrossRef] [PubMed]
- Jenks, M.; Jones, C. Dimensions of the Sustainable City; Springer: Berlin/Heidelberg, Germany, 2009. [Google Scholar]
- Peng, Z.; Wang, R.; Liu, L.; Wu, H. Fine-Scale Dasymetric Population Mapping With Mobile Phone and Building Use Data Based on Grid Voronoi Method. ISPRS Int. J. Geo-Inf. 2020, 9, 344. [Google Scholar] [CrossRef]
- Zhang, Y.; Pan, Y.; Zhao, X.; Shi, W.; Chen, Z.; Zhang, S.; Liu, P.; Xiao, J.; Tan, W.; Wang, D. Genomic characterization of SARS-CoV-2 identified in a reemerging COVID-19 outbreak in Beijing’s Xinfadi market in 2020. Biosaf. Health 2020, 2, 202–205. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Wang, Q.; Ding, P.; Cha, Y.e.; Mao, Y.; Ding, C.; Gu, W.; Wang, Y.; Ying, B.; Zhao, X. Risk factors and on-site simulation of environmental transmission of SARS-CoV-2 in the largest wholesale market of Beijing, China. Sci. Total Environ. 2021, 778, 146040. [Google Scholar] [CrossRef]
- Zhong, N. Management and prevention of SARS in China. Philos. Trans. R. Soc. Lond. Ser. B Biol. Sci. 2004, 359, 1115–1116. [Google Scholar] [CrossRef]
- Bowman, A.W.; Azzalini, A. Applied Smoothing Techniques for Data Analysis: The Kernel Approach with S-Plus Illustrations; OUP Oxford: Oxford, UK, 1997; Volume 18. [Google Scholar]
- Silverman, B.W. Density Estimation for Statistics and Data Analysis; Routledge: London, UK, 2018. [Google Scholar]
- Porta, S.; Strano, E.; Iacoviello, V.; Messora, R.; Latora, V.; Cardillo, A.; Wang, F.; Scellato, S. Street centrality and densities of retail and services in Bologna, Italy. Environ. Plan. Plan. Des. 2009, 36, 450–465. [Google Scholar] [CrossRef] [Green Version]
- Rybnikova, N.; Stevens, R.G.; Gregorio, D.I.; Samociuk, H.; Portnov, B.A. Kernel density analysis reveals a halo pattern of breast cancer incidence in Connecticut. Spat. Spatio-Temp. Epidemiol. 2018, 26, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Zhu, J.; Sun, Y.; Zhao, J. Delimitating urban commercial central districts by combining kernel density estimation and road intersections: A case study in nanjing city, china. ISPRS Int. J. Geo-Inf. 2019, 8, 93. [Google Scholar] [CrossRef] [Green Version]
- Prasannakumar, V.; Vijith, H.; Charutha, R.; Geetha, N. Spatio-temporal clustering of road accidents: GIS based analysis and assessment. Proc. Soc. Behav. Sci. 2011, 21, 317–325. [Google Scholar] [CrossRef] [Green Version]
- Nicholl, J.; West, J.; Goodacre, S.; Turner, J. The relationship between distance to hospital and patient mortality in emergencies: An observational study. Emerg. Med. J. 2007, 24, 665–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coombes, E.; Jones, A.P.; Hillsdon, M. The relationship of physical activity and overweight to objectively measured green space accessibility and use. Soc. Sci. Med. 2010, 70, 816–822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shukla, K.; Kumar, P.; Mann, G.S.; Khare, M. Mapping spatial distribution of particulate matter using Kriging and Inverse Distance Weighting at supersites of megacity Delhi. Sustain. Cities Soc. 2020, 54, 101997. [Google Scholar] [CrossRef]
- Jha, D.K.; Sabesan, M.; Das, A.; Vinithkumar, N.; Kirubagaran, R. Evaluation of Interpolation Technique for Air Quality Parameters in Port Blair, India. Univ. J. Environ. Res. Technol. 2011, 1, 301–310. [Google Scholar]
- Ma, J.; Ding, Y.; Gan, V.J.; Lin, C.; Wan, Z. Spatiotemporal prediction of PM2.5 concentrations at different time granularities using IDW-BLSTM. IEEE Access 2019, 7, 107897–107907. [Google Scholar] [CrossRef]
- Chen, F.-W.; Liu, C.-W. Estimation of the spatial rainfall distribution using inverse distance weighting (IDW) in the middle of Taiwan. Pad. Water Environ. 2012, 10, 209–222. [Google Scholar] [CrossRef]
- Yang, W.; Zhao, Y.; Wang, D.; Wu, H.; Lin, A.; He, L. Using principal components analysis and IDW interpolation to determine spatial and temporal changes of surface water quality of Xin’anjiang river in Huangshan, China. Int. J. Environ. Res. Public Health 2020, 17, 2942. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.; Su, X. Linear Regression Analysis: Theory and Computing; World Scientific: Singapore, 2009. [Google Scholar]
- Seber, G.A.; Lee, A.J. Linear Regression Analysis; John Wiley & Sons: Hoboken, NJ, USA, 2012; Volume 329. [Google Scholar]
- Montgomery, D.C.; Peck, E.A.; Vining, G.G. Introduction to Linear Regression Analysis; John Wiley & Sons: Hoboken, NJ, USA, 2021. [Google Scholar]
- Hamidi, S.; Sabouri, S.; Ewing, R. Does Density Aggravate the COVID-19 Pandemic? J. Am. Plan. Assoc. 2020, 86, 495–509. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Epidemiology Working Group for NCIP Epidemic Response, Chinese Center for Disease Control and Prevention. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Zhonghua Liuxingbingxue Zazhi 2020, 41, 145. [Google Scholar]
- Guida, C.; Carpentieri, G. Quality of life in the urban environment and primary health services for the elderly during the COVID-19 pandemic: An application to the city of Milan (Italy). Cities 2021, 110, 103038. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Geary, R.S.; Wheeler, B.; Lovell, R.; Jepson, R.; Hunter, R.; Rodgers, S. A call to action: Improving urban green spaces to reduce health inequalities exacerbated by COVID-19. Prevent. Med. 2021, 145, 106425. [Google Scholar] [CrossRef] [PubMed]
- Bereitschaft, B.; Scheller, D. How Might the COVID-19 Pandemic Affect 21st Century Urban Design, Planning, and Development? Urban Sci. 2020, 4, 56. [Google Scholar] [CrossRef]
- Kapoor, A.; Guha, S.; Das, M.K.; Goswami, K.C.; Yadav, R. Digital healthcare: The only solution for better healthcare during COVID-19 pandemic? Ind. Heart J. 2020, 72, 61–64. [Google Scholar] [CrossRef] [PubMed]
- Swiggy Plans to Serve 5 Lakh Meals Daily to the Needy Amid Coronavirus Lockdown. Available online: https://www.deccanherald.com/business/business-news/swiggy-plans-to-serve-5-lakh-meals-daily-to-the-needy-amid-coronavirus-lockdown-820599.html (accessed on 1 July 2020).
- Awad-Núñez, S.; Julio, R.; Gomez, J.; Moya-Gómez, B.; González, J.S. Post-COVID-19 travel behaviour patterns: Impact on the willingness to pay of users of public transport and shared mobility services in Spain. Eur. Trans. Res. Rev. 2021, 13, 1–18. [Google Scholar] [CrossRef]
- Gang, F. Harmonious coexistence of university and city-on the planning and design of clustered open campus. New Arch. 2009, 5, 4–9. [Google Scholar]
- Haaland, C.; van Den Bosch, C.K. Challenges and strategies for urban green-space planning in cities undergoing densification: A review. Urban Forest. Urban Green. 2015, 14, 760–771. [Google Scholar] [CrossRef]
- Boulton, C.; Dedekorkut-Howes, A.; Byrne, J. Factors shaping urban greenspace provision: A systematic review of the literature. Landsc. Urban Plan. 2018, 178, 82–101. [Google Scholar] [CrossRef]
- Gray, S.; Kellas, A. COVID-19 Has Highlighted the Inadequate, and Unequal, Access to High Quality Green Spaces; BMJ Publishing Group: London, UK, 2020; p. 3. [Google Scholar]
- Zhu, J.; Xu, C. Sina microblog sentiment in Beijing city parks as measure of demand for urban green space during the COVID-19. Urban Forest. Urban Green. 2021, 58, 126913. [Google Scholar] [CrossRef]
- Kondo, M.C.; Fluehr, J.M.; McKeon, T.; Branas, C.C. Urban green space and its impact on human health. Int. J. Environ. Res. Public Health 2018, 15, 445. [Google Scholar] [CrossRef] [Green Version]
- Markevych, I.; Schoierer, J.; Hartig, T.; Chudnovsky, A.; Hystad, P.; Dzhambov, A.M.; De Vries, S.; Triguero-Mas, M.; Brauer, M.; Nieuwenhuijsen, M.J. Exploring pathways linking greenspace to health: Theoretical and methodological guidance. Environ. Res. 2017, 158, 301–317. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Districts | Cumulative Confirmed Case | Proportion |
|---|---|---|
| Jiang’an (MUA) | 6563 | 12.987% |
| Jianghan (MUA) | 5242 | 10.373% |
| Qiaokou (MUA) | 6854 | 13.562% |
| Hanyang (MUA) | 4691 | 9.282% |
| Wuchang (MUA) | 7551 | 14.942% |
| Qingshan (MUA) | 2804 | 5.548% |
| Hongshan (MUA) | 4720 | 9.340% |
| Dongxihu | 2637 | 5.218% |
| Caidian | 1424 | 2.818% |
| Jiangxia | 875 | 1.731% |
| Huangpi | 2117 | 4.189% |
| Xinzhou | 1071 | 2.119% |
| East Lake Ecotourism Scenic District | 483 | 0.956% |
| East Lake High-Tech Development District | 2174 | 4.302% |
| Wuhan Economic Technological Development District | 1108 | 2.192% |
| Other places | 223 | 0.441% |
| Total | 50,537 | 100.00% |
| Date of Illness | Number of Weibo Help Information |
|---|---|
| 20–30 Novenmber 2019 | 3 |
| 1–31 Januaru 2020 | 558 |
| 1–6 February 2020 | 154 |
| 7–10 February 2020 | 14 |
| Districts | Infections in Weibo Information | Cumulative Confirmed Case | the Participation Rate |
|---|---|---|---|
| Jianghan (MUA) | 75 | 5137 | 1.46% |
| Qiaokou (MUA) | 128 | 6789 | 1.89% |
| Wuchang (MUA) | 135 | 7431 | 1.82% |
| Jiang’an (MUA) | 145 | 6521 | 2.22% |
| Hanyang (MUA) | 116 | 4661 | 2.49% |
| Hongshan (MUA) | 87 | 4652 | 1.87% |
| Qingshan (MUA) | 64 | 2773 | 2.31% |
| Dimension | Variables | Definitions |
|---|---|---|
| Dependent variable | Weibo help case density (Weibo) | The average KDE 1 value of COVID-19 infectors in each unit |
| Population density | Population density (Population) | The average KDE 1 value of the population in each unit |
| The elderly population density (Elderly) | The average KDE 1 value of the elderly population in each unit | |
| Distance to the third ring road (Ring3) | The average ED 2 value from units to the third ring road | |
| Distance to rivers (River) | The average ED 2 value from units to rivers | |
| Human mobility | Distance to markets (Market) | The average ED 2 value from units to markets |
| Distance to third-class hospitals (Hospital) | The average ED 2 value from units to hospitals | |
| Middle school density (M_school) | The average KDE 1 value of middle schools in each unit | |
| University density (University) | The average KDE 1 value of universities in each unit | |
| Business density (Business) | The average KDE 1 value of business facilities in each unit | |
| Administration density (Administration) | The average KDE 1 value of administration facilities in each unit | |
| Bus stop density (Bus) | The average KDE 1 value of bus stop in each unit | |
| Metro station density (Metro) | The average KDE 1 value of metro station in each unit | |
| Environmental quality | Housing price (Price) | The average house price in each unit |
| Age of buildings (Year) | The average age of buildings in each unit | |
| Air quality index (AQI) | The average IDW 3 value of air quality index in each unit | |
| Distance to green spaces (Green) | The average ED 2 value from units to green spaces | |
| water density (water) | The average KDE 1 value values of waters in each unit |
| Variable Name | Number | Minimum | Maximum | Mean | Std. Deviation |
|---|---|---|---|---|---|
| Weibo help density (Weibo) | 1681 | 0.0000 | 73,959.0440 | 28,405.5334 | 17,269.6339 |
| Population density (Population) | 1681 | 2.5756 | 31,293.7673 | 8199.1254 | 5694.6717 |
| The elderly population density (Elderly) | 1681 | 1.9645 | 2052.2024 | 653.7139 | 464.9645 |
| Distance to the third ring road (Ring3) | 1681 | –6662.0000 | 10,621.0000 | 4499.3998 | 3162.0162 |
| Distance to rivers (River) | 1681 | 70.0000 | 16,329.0000 | 3259.2570 | 3170.4919 |
| Distance to markets (Market) | 1681 | 11.2599 | 4087.3986 | 410.5552 | 421.3228 |
| Distance to third-class hospitals (Hospital) | 1681 | 23.0000 | 9432.0000 | 1913.4747 | 1535.0498 |
| Middle school density (M_school) | 1681 | 1.0000 | 59.1887 | 15.1634 | 13.7686 |
| University density (University) | 1681 | 1.0000 | 58.6333 | 3.6523 | 5.2843 |
| Business density (Business) | 1681 | 1.0000 | 54.7805 | 3.2398 | 5.1925 |
| Administration density (Administration) | 1681 | 1.0000 | 58.9231 | 4.2478 | 7.3873 |
| Bus stop density (Bus) | 1681 | 1.4563 | 59.6098 | 27.6569 | 13.4843 |
| Metro station density (Metro) | 1681 | 1.0000 | 57.6180 | 17.0827 | 14.5484 |
| Housing price (Price) | 1681 | 7975.0000 | 40,989.0000 | 18,447.5544 | 3879.5026 |
| Age of buildings (Year) | 1681 | 2.6891 | 28.0737 | 15.9859 | 4.5786 |
| Air quality index (AQI) | 1681 | 80.3393 | 93.3462 | 86.6823 | 2.1607 |
| Distance to green spaces (Green) | 1681 | 0.0000 | 6727.0000 | 662.9863 | 633.4966 |
| water density (water) | 1681 | 1.0000 | 32.4762 | 9.8986 | 7.4350 |
| Model | Unstandardized Coefficients | Standardized Coefficients | t-Value | Significance | Collinearity Statistics | ||
|---|---|---|---|---|---|---|---|
| Beta | Std. Error | Beta | Tolerance | VIF | |||
| (Constant) | −70,623.886 | 10,753.331 | −6.568 | 0.000 | |||
| Population | −0.475 | 0.083 | −0.157 | −5.725 | 0.000 | 0.164 | 6.113 |
| Elderly | 16.697 | 1.28 | 0.450 | 13.041 | 0.000 | 0.103 | 9.714 |
| Ring3 | 1.539 | 0.115 | 0.282 | 13.379 | 0.000 | 0.276 | 3.625 |
| River | −0.781 | 0.088 | −0.143 | −8.914 | 0.000 | 0.473 | 2.114 |
| Market | −2.144 | 0.607 | −0.052 | −3.531 | 0.000 | 0.558 | 1.794 |
| Hospital | −0.923 | 0.186 | −0.082 | −4.978 | 0.000 | 0.45 | 2.223 |
| M_school | 151.174 | 21.843 | 0.121 | 6.921 | 0.000 | 0.403 | 2.479 |
| University | −156.239 | 44.016 | −0.048 | −3.55 | 0.000 | 0.674 | 1.483 |
| Business | −18.321 | 43.511 | −0.006 | −0.421 | 0.674 | 0.715 | 1.399 |
| Administration | 25.647 | 35.631 | 0.011 | 0.72 | 0.472 | 0.527 | 1.899 |
| Bus | 417.361 | 29.146 | 0.326 | 14.32 | 0.000 | 0.236 | 4.234 |
| Metro | 142.755 | 21.209 | 0.120 | 6.731 | 0.000 | 0.383 | 2.610 |
| Price | −0.886 | 0.079 | −0.199 | −11.268 | 0.000 | 0.392 | 2.552 |
| Year | −426.759 | 67.602 | −0.113 | −6.313 | 0.000 | 0.381 | 2.626 |
| AQI | 1132.903 | 119.915 | 0.142 | 9.448 | 0.000 | 0.543 | 1.840 |
| Green | 1.032 | 0.369 | 0.038 | 2.796 | 0.005 | 0.667 | 1.499 |
| Water | −120.487 | 34.619 | −0.052 | −3.48 | 0.001 | 0.551 | 1.816 |
| R: 0.893 | R Square: 0.797 | Adjusted R Square: 0.794 | |||||
| Std. Error of the Estimate: 7831.238353 | |||||||
| Model | Unstandardized Coefficients | Standardized Coefficients | t-Value | Significance | Collinearity Statistics | ||
|---|---|---|---|---|---|---|---|
| Beta | Std. Error | Beta | Tolerance | VIF | |||
| (Constant) | −80,667.568 | 10,629.470 | −7.589 | 0.000 | |||
| Elderly | 11.599 | 0.867 | 0.312 | 13.371 | 0.000 | 0.229 | 4.364 |
| Ring3 | 1.457 | 0.114 | 0.267 | 12.750 | 0.000 | 0.286 | 3.501 |
| River | −0.945 | 0.083 | −0.174 | −11.403 | 0.000 | 0.540 | 1.853 |
| Market | −1.868 | 0.608 | −0.046 | −3.070 | 0.002 | 0.568 | 1.762 |
| Hospital | −0.870 | 0.186 | −0.077 | −4.673 | 0.000 | 0.456 | 2.194 |
| M_school | 144.758 | 22.042 | 0.115 | 6.567 | 0.000 | 0.405 | 2.471 |
| University | −193.204 | 43.907 | −0.059 | −4.400 | 0.000 | 0.692 | 1.444 |
| Bus | 411.545 | 29.433 | 0.321 | 13.983 | 0.000 | 0.237 | 4.226 |
| Metro | 144.609 | 21.162 | 0.122 | 6.833 | 0.000 | 0.393 | 2.543 |
| Price | −0.793 | 0.069 | −0.178 | −11.471 | 0.000 | 0.519 | 1.928 |
| Year | −378.367 | 66.530 | −0.100 | −5.687 | 0.000 | 0.402 | 2.490 |
| AQI | 1229.175 | 117.094 | 0.154 | 10.497 | 0.000 | 0.582 | 1.717 |
| Green | 0.942 | 0.373 | 0.035 | 2.527 | 0.012 | 0.668 | 1.496 |
| Water | −140.884 | 34.832 | −0.061 | −4.045 | 0.000 | 0.556 | 1.799 |
| R: 0.890 | R Square: 0.792 | Adjusted R Square: 0.790 | |||||
| Std. Error of the Estimate: 7915.456643 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, R.; Liu, L.; Wu, H.; Peng, Z. Correlation Analysis between Urban Elements and COVID-19 Transmission Using Social Media Data. Int. J. Environ. Res. Public Health 2022, 19, 5208. https://doi.org/10.3390/ijerph19095208
Wang R, Liu L, Wu H, Peng Z. Correlation Analysis between Urban Elements and COVID-19 Transmission Using Social Media Data. International Journal of Environmental Research and Public Health. 2022; 19(9):5208. https://doi.org/10.3390/ijerph19095208
Chicago/Turabian StyleWang, Ru, Lingbo Liu, Hao Wu, and Zhenghong Peng. 2022. "Correlation Analysis between Urban Elements and COVID-19 Transmission Using Social Media Data" International Journal of Environmental Research and Public Health 19, no. 9: 5208. https://doi.org/10.3390/ijerph19095208
APA StyleWang, R., Liu, L., Wu, H., & Peng, Z. (2022). Correlation Analysis between Urban Elements and COVID-19 Transmission Using Social Media Data. International Journal of Environmental Research and Public Health, 19(9), 5208. https://doi.org/10.3390/ijerph19095208