
Madelung’s Disease as an Example of a Metabolic Disease Associated with Alcohol Abuse—Diagnostic Importance of Computed Tomography

 ,
,  and
and
Abstract
:1. Introduction
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Szewc, M.; Sitarz, R.; Moroz, N.; Maciejewski, R.; Wierzbicki, R. Madelung’s disease—Progressive, excessive, and symmetrical deposition of adipose tissue in the subcutaneous layer: Case report and literature review. Diabetes Diabetes Metab. Syndr. Obes. Targets Ther. 2018, 11, 819–825. Available online: https://www.dovepress.com/madelungs-disease-progressive-excessive-and-symmetrical-deposition-of-peer-reviewed-fulltext-article-DMSO#ref6 (accessed on 2 February 2022). [CrossRef] [PubMed] [Green Version]
- Rare Disease Database. Available online: https://rarediseases.org/rare-diseases/madelungs-disease/ (accessed on 2 February 2022).
- Schiltz, D.; Anker, A.; Ortner, C.; Tschernitz, S.; Koller, M.; Klein, S.; Felthaus, O.; Schreml, J.; Schreml, S.; Prantl, L. Multiple Symmetric Lipomatosis: New Classification System Based on the Largest German Patient Cohort. Plast. Reconstr. Surg. Glob. Open 2018, 6, e1722. Available online: https://journals.lww.com/prsgo/Fulltext/2018/04000/Multiple_Symmetric_Lipomatosis__New_Classification.14.aspx (accessed on 2 February 2022). [CrossRef] [PubMed]
- Musialik, K.; Bogdański, P.; Nawrocka, M. Choroba Madelunga—Opis przypadku i przegląd piśmiennictwa. Forum Zaburzeń Metab. 2012, 3, 147–153. [Google Scholar]
- Waniczek, D.; Kamińska, E.; Kamiński, T.; Pilch, J.; Nawrocki, P. Łagodna symetryczna tłuszczakowatość—Choroba metaboliczna o nieznanej etiologii. Ann. Acad. Med. Silesiensis 2012, 66, 85–90. Available online: http://psjd.icm.edu.pl/psjd/element/bwmeta1.element.psjd-44ac6335-27fa-4f9c-8424-fe877d6b2a2d (accessed on 2 February 2022).
- Ouahabi, H.; Doubi, S.; Lahlou, K.; Boujraf, S.; Ajdi, F. Launois-Bensaude Syndrome: A Benign Symmetric Lipomatosis without Alcohol Association. Ann. Afr. Med. 2017, 16, 33–34. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5452705/ (accessed on 2 February 2022).
- Gozzo, C.; Galioto, F.; Palmucci, S.; Signorelli, S.; Basile, A. A non–alcohol-related case of Madelung’s disease: Challenging patient with progressive jugular vein distension. Radiol. Case Rep. 2021, 16, 1183–1187. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7985283/ (accessed on 2 February 2022). [CrossRef] [PubMed]
- Ardeleanu, V.; Chicos, S.; Georgescu, C.; Tutunaru, D. Multiple benign symmetric lipomatosis—A differential diagnosis of obesity. Chirurgia 2013, 108, 580–583. Available online: https://pubmed.ncbi.nlm.nih.gov/23958107/ (accessed on 2 February 2022). [PubMed]
- Chen, C.; Fang, Q.; Wang, X.; Zhang, M.; Zhao, W.; Shi, B.; Wu, L.; Zhang, L.; Tan, W. Madelung’s Disease: Lipectomy or Liposuction? BioMed Res. Int. 2018, 2018, 3975974. Available online: https://www.hindawi.com/journals/bmri/2018/3975974/ (accessed on 2 February 2022). [CrossRef] [PubMed] [Green Version]
- Mlosek, R.; Skrzypek, E.; Migda, B.; Migda, M.; Woźniak, W. The efficacy of high-frequency ultrasound-guided injection lipolysis in reducing fat deposits located on the inside of the knees. J. Ultrason. 2020, 20, e273–e278. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7830143/ (accessed on 2 February 2022). [CrossRef] [PubMed]

{kind=link}
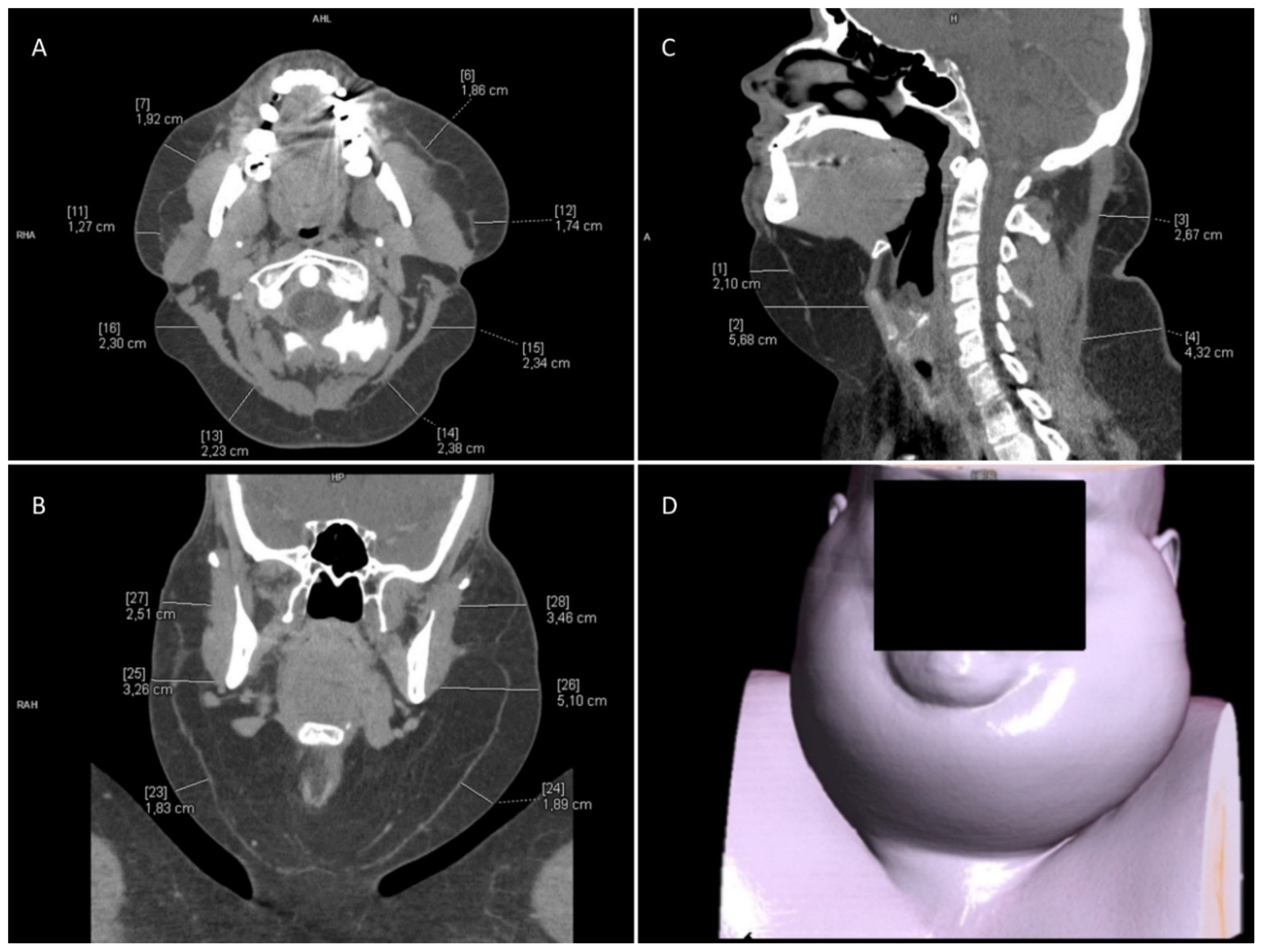
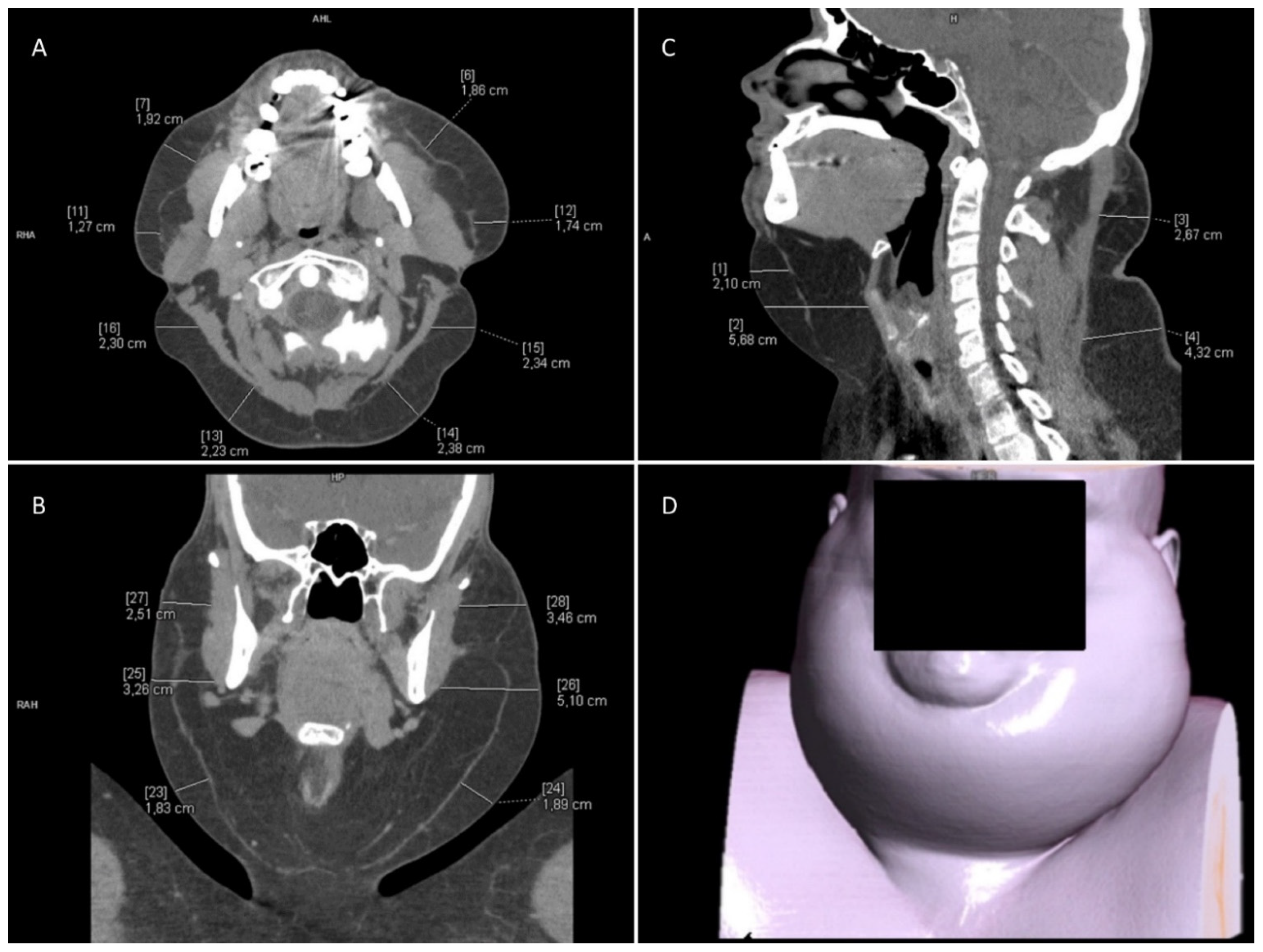
| Neck CT | |
|---|---|
| Exact Location | Fat Layer Thickness [mm] |
| left side of the neck | 50 |
| right side of the neck | 50 |
| chin area | 70 |
| infrahyoid region | 60 |
| right neck triangle | 40 |
| left neck triangle | 30 |
| Chest CT—Anterior Part of the Chest | |||
| Right side | Left side | ||
| Exact location | Fat layer thickness [mm] | Exact location | Fat layer thickness [mm] |
| Upper part | 30 | Upper part | 20 |
| Middle part | 25 | Middle part | 15 |
| Lower part | 20 | Lower part | 15 |
| Chest CT—Lateral Part of the Chest | |||
| Right side | Left side | ||
| Exact location | Fat layer thickness [mm] | Exact location | Fat layer thickness [mm] |
| Upper part | 40 | Upper part | 30 |
| Middle part | 30 | Middle part | 40 |
| Lower part | 28 | Lower part | 30 |
| Chest CT—Posterior Part of the Chest | |||
| Right side | Left side | ||
| Exact location | Fat layer thickness [mm] | Exact location | Fat layer thickness [mm] |
| Upper part | 20 | Upper part | 20 |
| Middle part | 25 | Middle part | 25 |
| Lower part | 30 | Lower part | 35 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jaźwiec, P.; Pawłowska, M.; Czerwińska, K.; Poręba, M.; Gać, P.; Poręba, R. Madelung’s Disease as an Example of a Metabolic Disease Associated with Alcohol Abuse—Diagnostic Importance of Computed Tomography. Int. J. Environ. Res. Public Health 2022, 19, 5168. https://doi.org/10.3390/ijerph19095168
Jaźwiec P, Pawłowska M, Czerwińska K, Poręba M, Gać P, Poręba R. Madelung’s Disease as an Example of a Metabolic Disease Associated with Alcohol Abuse—Diagnostic Importance of Computed Tomography. International Journal of Environmental Research and Public Health. 2022; 19(9):5168. https://doi.org/10.3390/ijerph19095168
Chicago/Turabian StyleJaźwiec, Przemysław, Maria Pawłowska, Karolina Czerwińska, Małgorzata Poręba, Paweł Gać, and Rafał Poręba. 2022. "Madelung’s Disease as an Example of a Metabolic Disease Associated with Alcohol Abuse—Diagnostic Importance of Computed Tomography" International Journal of Environmental Research and Public Health 19, no. 9: 5168. https://doi.org/10.3390/ijerph19095168
APA StyleJaźwiec, P., Pawłowska, M., Czerwińska, K., Poręba, M., Gać, P., & Poręba, R. (2022). Madelung’s Disease as an Example of a Metabolic Disease Associated with Alcohol Abuse—Diagnostic Importance of Computed Tomography. International Journal of Environmental Research and Public Health, 19(9), 5168. https://doi.org/10.3390/ijerph19095168