
Pediatric Cancer as a Factor of Changes in the Family



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group
2.2. Research Methods
2.3. Statistical Analysis
3. Results
4. Discussion
Limitations
- (1)
- The survey questionnaires were completed only by volunteers from one region of the country (Lower Silesia, Poland). Therefore, the results cannot be extrapolated to the whole population.
- (2)
- The survey questionnaires were completed electronically without the assistance of health care professionals. As a result, neither the diagnosis nor the current health status of children was verified, which may have affected the level of resilience.
- (3)
- Only one parent per family was enrolled in the study. We did not evaluate dyadic or intrafamily resilience. We did not include data on parent–child or parent-to-parent relationships, which limits conclusions for the whole family.
- (4)
- We did not include an analysis of resilience in relation to socio-economic factors. We did not consider time elapsed since the diagnosis or treatment time in the study group. We lacked power and sample diversity to conduct relevant subgroup analyses.
- (5)
- We did not include information on whether the parents received psychological support or other psychotherapeutic interventions that could have influenced the results.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Potrykowska, A.; Strzelecki, Z.; Szymborski, J.; Witkowski, J. Cancer Incidence and Mortality versus the Demographic Situation of Poland; Governmental Population Council: Warszawa, Poland, 2014; pp. 117–146. (In Polish)
- Hunger, S.P.; Mullighan, C.G. Acute Lymphoblastic Leukemia in Children. N. Engl. J. Med. 2015, 373, 1541–1552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mousavi, S.M.; Pourfeizi, A. Dastgiri, S. Childhood Cancer in Iran. J. Pediatr. Hematol. Oncol. 2010, 32, 376–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arestedt, L.; Benzein, E.; Persson, C. Families living with chronic illness: Beliefs about illness, family, and healthcare. J. Fam. Nurs. 2015, 21, 206–231. [Google Scholar] [CrossRef] [PubMed]
- Kędziora, S. The impact of a child’s chronic illness on family life. Naucz. I Szkoła 2007, 3–4, 57–66. (In Polish) [Google Scholar]
- Van Schoors, M.; Caes, L.; Verhofstadt, L.L.; Gouber, L.; Alderfer, M.A. Systematic review: Family resilience after pediatric cancer diagnosis. J. Pediatr. Psychol. 2015, 40, 856–868. [Google Scholar] [CrossRef] [Green Version]
- Da Silva, F.M.; Jacob, E.; Nascimento, L.C. Impact of childhood cancer on parents’ relationships: An integrative review. J. Nurs. Scholarsh. 2010, 42, 250–261. [Google Scholar]
- Long, K.A.; Marsland, A.L. Family adjustment to childhood cancer: A systematic review. Clin. Child Fam. Psychol. Rev. 2011, 14, 57–88. [Google Scholar] [CrossRef]
- Nóia, T.D.C.; Sant’Ana, R.S.E.; Santos, A.D.S.D.; Oliveira, S.D.C.; Bastos Veras, S.M.C.; Lopes-Júnior, L.C. Coping with the diagnosis and hospitalization of a child with childhood cancer. Investig. Y Educ. En Enfermería 2015, 33, 465–472. [Google Scholar] [CrossRef] [Green Version]
- Van Schoors, M.; De Paepe, A.L.; Lemiere, J.; Morez, A.; Norga, K.; Lambrecht, K.; Goubert, L.; Verhofstadt, L.L. Family Adjustment When Facing Pediatric Cancer: The Role of Parental Psychological Flexibility, Dyadic Coping, and Network Support. Front. Psychol. 2019, 10, 2740. [Google Scholar] [CrossRef]
- Seiler, A.; Jenewein, J. Resilience of Cancer Patients. Front. Psychiatry 2019, 10, 208. [Google Scholar] [CrossRef] [Green Version]
- Rosenberg, A.R.; Wolfe, J.; Bradford, M.C.; Shaffer, M.L.; Yi-Frazier, J.P.; Curtis, R.; Syrjala, K.L.; Baker, K.S. Resilience and psychosocial outcomes in parents of children with cancer. Pediatr. Blood Cancer 2014, 61, 552–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosoda, T. The Impact of Childhood Cancer on Family Functioning: A Review. Grad. Stud. J. Psychol. 2014, 15, 18–30. [Google Scholar]
- Ogińska-Bulik, N.; Juczyński, Z. The Resilience Measurement Scale. Now Psychol. 2008, 3, 39–56. (In Polish) [Google Scholar]
- Molina, Y.; Yi, J.C.; Martinez-Gutierrez, J.; Reding, K.W.; Yi-Frazier, J.P.; Rosenberg, A.R. Resilience among Patients Across the Cancer Continuum: Diverse Perspectives. Clin. J. Oncol. Nurs. 2014, 18, 93–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, Y.H.; Li, W.H.C.; Cheung, A.T.; Ho, L.K.K.; Xia, W.; He, X.L.; Zhang, J.P.; Chung, J.O.K. Relationships between resilience and quality of life in parents of children with cancer. J. Health Psychol. 2021, 27, 1048–1056. [Google Scholar] [CrossRef]
- Van Warmerdam, J.; Zabih, V.; Kurdyak, P.; Sutradhar, R.; Nathan, P.C.; Gupta, S. Prevalence of anxiety, depression, and posttraumatic stress disorder in parents of children with cancer: A meta-analysis. Pediatr. Blood Cancer 2019, 66, e27677. [Google Scholar] [CrossRef]
- Eilertsen, M.E.; Hjemdal, O.; Le, T.T.; Diseth, T.H.; Reinfjell, T. Resilience factors play an important role in the mental health of parents when children survive acute lymphoblastic leukaemia. Acta Paediatr. 2015, 105, 30–34. [Google Scholar] [CrossRef]
- Ye, Z.J.; Guan, H.J.; Wu, L.H.; Xiao, M.Y.; Luo, D.M.; Quan, X.M. Resilience and Psychosocial Function Among Mainland Chinese Parents of Children with Cancer. Cancer Nurs. 2015, 38, 466–474. [Google Scholar] [CrossRef]
- Oginska-Bulik, N. Resiliency and satisfaction with life in alcohol-dependent persons. Alkohol. I Narkom. 2014, 27, 319–324. (In Polish) [Google Scholar]
- Bruce, M. A systematic and conceptual review of posttraumatic stress in childhood cancer survivors and their parents. Clin. Psychol. Rev. 2006, 26, 233–256. [Google Scholar] [CrossRef]
- Mouw, T.; Koster, A.; Wright, M.E.; Blank, M.M.; Moore, S.C.; Hollenbeck, A.; Schatzkin, A. Education and Risk of Cancer in a Large Cohort of Men and Women in the United States. PLoS ONE 2008, 3, e3639. [Google Scholar] [CrossRef] [PubMed]
- Oliver, M.A.; Lajaunie, C.h.; Webster, R.; Muir, K.R.; Mann, J.R. Estimating the Risk of Childhood Cancer. In Geostatistics Troia’92; Springer: Dordrecht, The Netherlands, 1993; pp. 899–910. [Google Scholar]
- Delavar, A.; Johnson, K.J. Place of residence and childhood cancer survival. Oncotarget 2019, 10, 1864–1865. [Google Scholar] [CrossRef]
- Youlden, D.R.; Baade, P.D.; Valery, P.C.; Ward, L.J.; Green, A.C.; Aitken, J.F. Differentials in Survival for Childhood Cancer in Australia by Remoteness of Residence and Area Disadvantage. Cancer Epidemiol. Prev. Biomark. 2011, 20, 1649–1656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bona, K.; Dussel, V.; Orellana, L.; Kang, T.; Geyer, R.; Feudtner, C.h.; Wolfe, J. Economic Impact of Advanced Pediatric Cancer on Families. J. Pain Symptom Manag. 2014, 47, 594–603. [Google Scholar] [CrossRef] [PubMed]
- Lau, S.; Lu, X.; Balsamo, L.; Devidas, M.; Winick, N.; Hunger, S.P.; Kadan-Lottick, N. Family life events in the first year of acute lymphoblastic leukemia therapy: A children’s oncology group report. Pediatr. Blood Cancer 2014, 61, 2277–2284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peikert, M.L.; Inhestern, L.; Krauth, K.A.; Escherich, G.; Rutkowski, S.; Kandels, D.; Bergelt, C. Returning to daily life: A qualitative interview study on parents of childhood cancer survivors in Germany. BMJ Open 2020, 10, e033730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baruch, A. Child cancer as a factor causing changes in family functioning—Selected aspects. Przegląd Pedagog. 2013, 2, 133–148. (In Polish) [Google Scholar]
- Brody, A.C.; Simmons, L.A. Family Resiliency during Childhood Cancer: The Father’s Perspective. J. Pediatr. Oncol. Nurs. 2007, 24, 152–165. [Google Scholar] [CrossRef]
- Carlsson, T.; Kukkola, L.; Ljungman, L.; Hovén, E.; Von Essen, L. Psychological distress in parents of children treated for cancer: An explorative study. PLoS ONE 2019, 14, e0218860. [Google Scholar] [CrossRef] [Green Version]
- Jones, B.L.; Pelletier, W.; Decker, C.; Barczyk, A.; Dungan, S.S. Fathers of children with cancer: A descriptive synthesis of the literature. Soc. Work. Health Care 2010, 49, 458–493. [Google Scholar] [CrossRef]
- Wakefield, C.E.; McLoone, J.K.; Butow, P.; Lenthen, K.; Cohn, R.J. Parental adjustment to the completion of their child’s cancer treatment. Pediatr. Blood Cancer 2011, 56, 524–531. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | Total (N = 339) | Study Group (N = 153) | Control Group (N = 186) | Chi-Squared Test | Study Group vs. Control Group p |
|---|---|---|---|---|---|
| Place of residence | <0.001 * | ||||
| Village | 73 | 54 | 19 | ||
| Town (<50,000) | 75 | 26 | 49 | ||
| City (50,000–100,000) | 34 | 25 | 9 | 60.2 | |
| Large city (>100,000) | 157 | 48 | 109 | ||
| Education | <0.001 * | ||||
| Primary/vocational | 17 | 14 | 3 | ||
| Secondary | 68 | 43 | 25 | ||
| Higher (Bachelor’s degree) | 48 | 24 | 24 | 28.28 | |
| Higher (Master’s degree) | 206 | 72 | 134 | ||
| Financial situation | <0.001 * | ||||
| Satisfactory | 300 | 145 | 155 | ||
| Unsatisfactory | 32 | 2 | 30 | 227.64 | |
| Poor | 7 | 6 | 1 | ||
| Employment structure | <0.001 * | ||||
| The parent does not work | 108 | 96 | 12 | ||
| One spouse does not work | 28 | 18 | 10 | 156.24 | |
| Both parents work | 203 | 39 | 164 | ||
| Upbringing of the child | 0.2 | ||||
| by both parents | 313 | 144 | 169 | 3.21 | |
| by one parent | 19 | 8 | 11 | ||
| with a partner who is not the child’s parent | 7 | 1 | 6 |
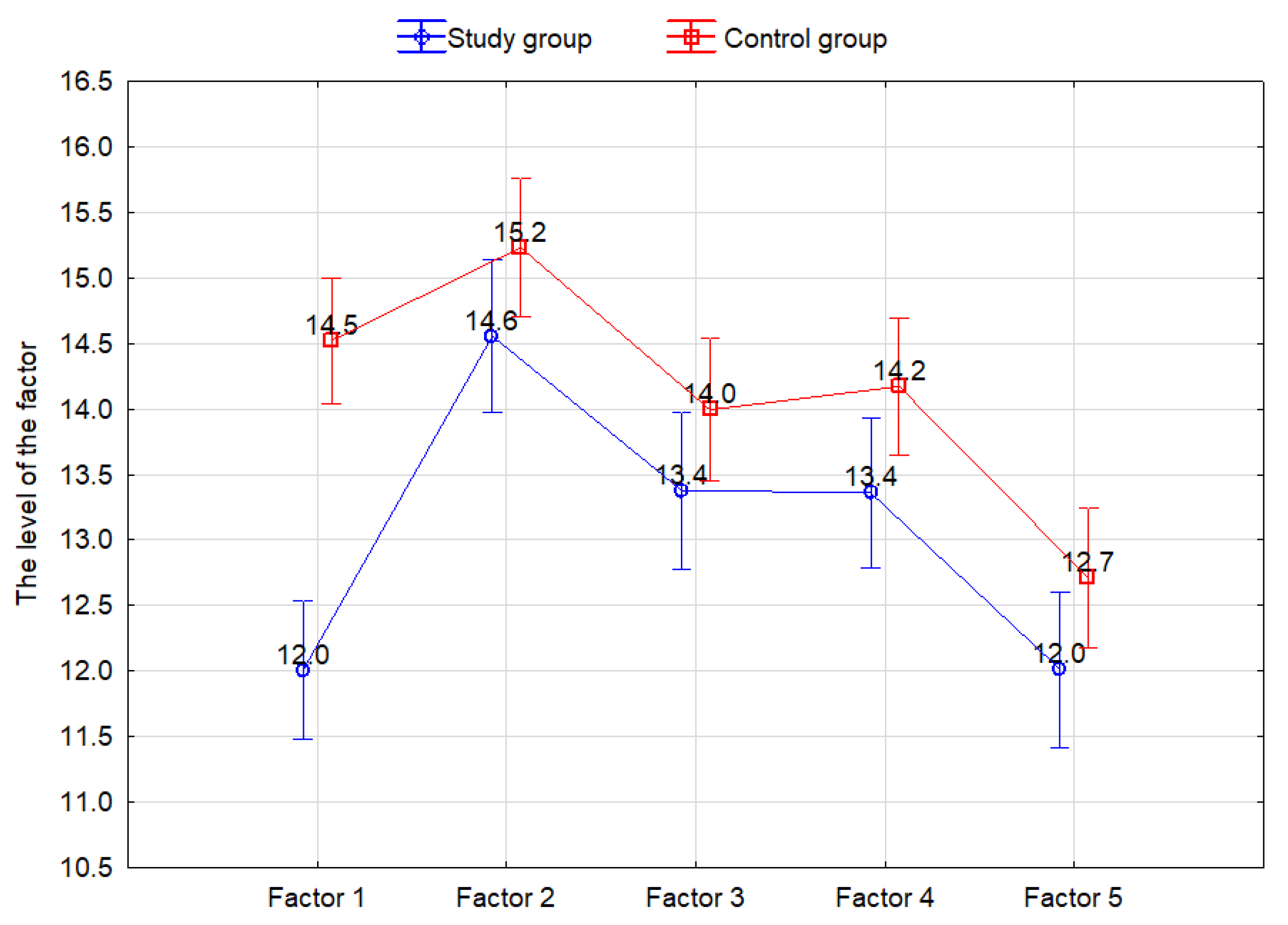
| Effect | F | p |
|---|---|---|
| Group | 8.867 | 0.003 * |
| FACTOR | 92.699 | <0.001 * |
| FACTOR × Group | 18.344 | <0.001 * |
| FACTOR | 1 13.25 | 2 14.9 | 3 13.7 | 4 13.8 | 5 12.35 |
|---|---|---|---|---|---|
| 1 | <0.001 * | 0.13 | 0.02 * | <0.001 * | |
| 2 | <0.001 * | <0.001 * | <0.001 * | <0.001 * | |
| 3 | 0.13 | <0.001 * | 1.00 | <0.001 * | |
| 4 | 0.02 * | <0.001 * | 1.00 | <0.001 * | |
| 5 | <0.001 * | <0.001 * | <0.001 * | <0.001 * |
| FACTOR | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Study group vs. control group | <0.001 * | 0.09 | 0.13 | 0.04 * | 0.08 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dąbrowska, A.; Malicka, I. Pediatric Cancer as a Factor of Changes in the Family. Int. J. Environ. Res. Public Health 2022, 19, 5002. https://doi.org/10.3390/ijerph19095002
Dąbrowska A, Malicka I. Pediatric Cancer as a Factor of Changes in the Family. International Journal of Environmental Research and Public Health. 2022; 19(9):5002. https://doi.org/10.3390/ijerph19095002
Chicago/Turabian StyleDąbrowska, Aleksandra, and Iwona Malicka. 2022. "Pediatric Cancer as a Factor of Changes in the Family" International Journal of Environmental Research and Public Health 19, no. 9: 5002. https://doi.org/10.3390/ijerph19095002
APA StyleDąbrowska, A., & Malicka, I. (2022). Pediatric Cancer as a Factor of Changes in the Family. International Journal of Environmental Research and Public Health, 19(9), 5002. https://doi.org/10.3390/ijerph19095002