
Effects of Forest-Based Interventions on Mental Health: A Meta-Analysis of Randomized Controlled Trials


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
Criteria for Literature Selection
2.2. Data Collection
2.3. Evaluation of the Quality of Literature
2.4. Data Analysis
2.4.1. Data Coding and Processing
2.4.2. Effect Size
2.4.3. Publication Bias
3. Results
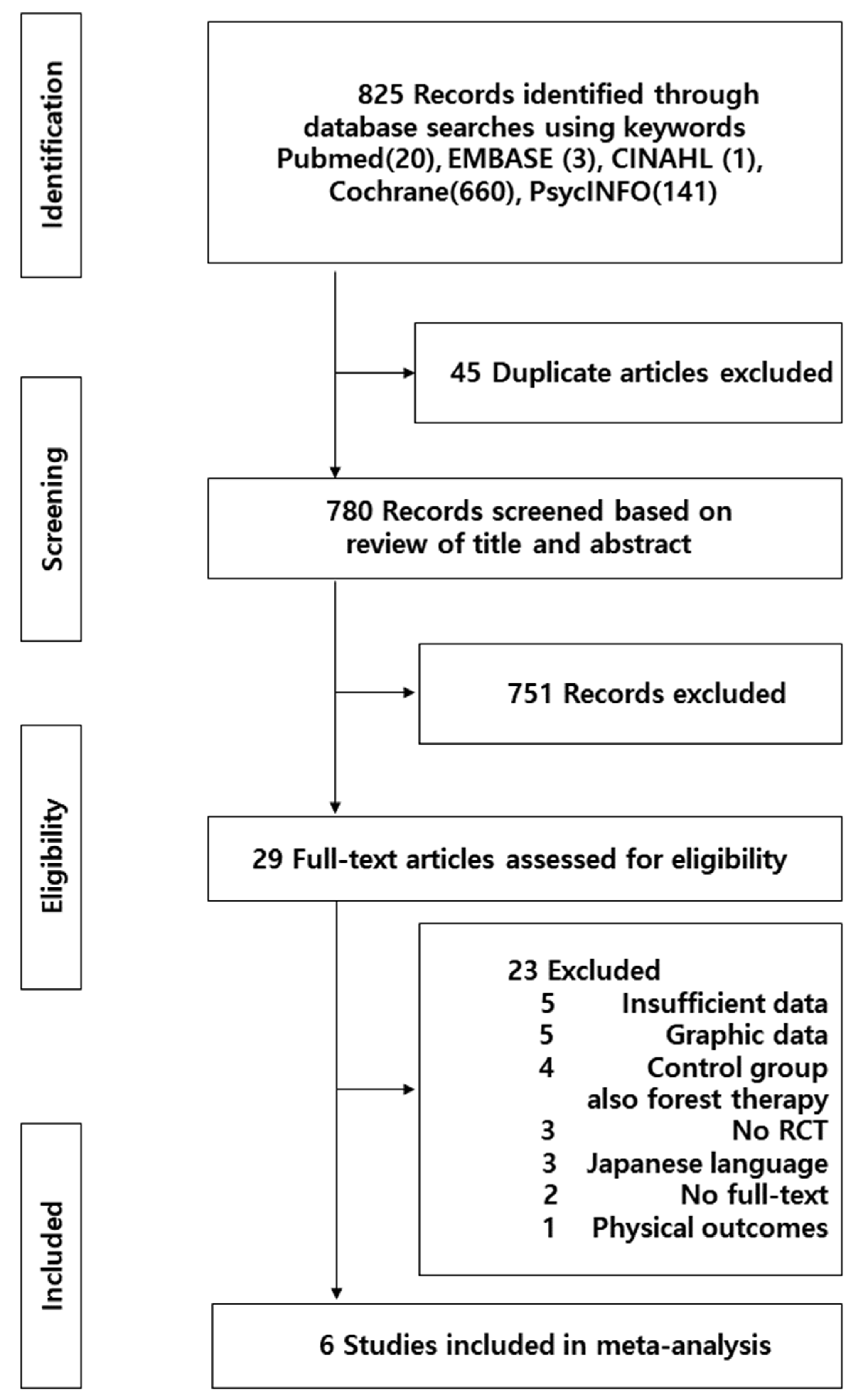
3.1. Selection of Literature
3.2. Evaluation of the Quality of the Literature
3.3. General Characteristics of the Included Studies
3.4. Outcome Variables and the Effect Sizes of Forest Therapy Intervention Studies
3.4.1. Depression
3.4.2. Anxiety
3.4.3. Positive Emotions
3.4.4. Negative Emotions
3.4.5. Testing for Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kabisch, N.; Püffel, C.; Masztalerz, O.; Hemmerling, J.; Kraemer, R. Physiological and psychological effects of visits to different urban green and street environments in older people: A field experiment in a dense inner-city area. Landsc. Urban Plan. 2021, 207, 103998. [Google Scholar] [CrossRef]
- Levin, R.; Zilli Vieira, C.L.; Rosenbaum, M.H.; Bischoff, K.; Mordarski, D.C.; Brown, M.J. The urban lead (Pb) burden in humans, animals and the natural environment. Environ. Res. 2021, 193, 110377. [Google Scholar] [CrossRef] [PubMed]
- Oh, B.; Lee, K.J.; Zaslawski, C.; Yeung, A.; Rosenthal, D.; Larkey, L.; Back, M. Health and well-being benefits of spending time in forests: Systematic review. Environ. Health Prev. Med. 2017, 22, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.; Kim, D.; Lee, K.; Lee, H.; Lee, Y. A study on effect of forest related programs based on the meta-analysis. J. Korean Inst. For. Recreat. 2015, 19, 1–13. [Google Scholar]
- Stier-Jarmer, M.; Throner, V.; Kirschneck, M.; Immich, G.; Frisch, D.; Schuh, A. The psychological and physical effects of forests on human health: A systematic review of systematic reviews and meta-analyses. Int. J. Environ. Res. Public Health 2021, 18, 1770. [Google Scholar] [CrossRef]
- Lee, Y.; Kim, S.M.; Li, N. The effects of forest therapy on medical expenses reduction. J. Women Econ. 2015, 12, 23–44. [Google Scholar]
- Forestry Culture and Recreation Act. Available online: http://www.law.go.kr/main.html (accessed on 27 September 2021).
- Bae, S.-J.; Kim, D.-S.; Kim, S.-J.; Kim, S.-P.; Lee, W.-L.; Ryu, J.-S.; Kim, J.-E.; Park, S. Recognition and demand analysis of agro-healing services by supply types. J. Korean Soc. Rural Plan. 2019, 25, 1–11. [Google Scholar] [CrossRef]
- Kotte, D.; Li, Q.; Shin, W.S.; Michalsen, A. International Handbook of Forest Therapy; Cambridge Scholars Publishing: Cambridge, UK, 2019. [Google Scholar]
- Antonelli, M.; Donelli, D.; Barbieri, G.; Valussi, M.; Maggini, V.; Firenzuoli, F. Forest Volatile Organic Compounds and Their Effects on Human Health: A State-of-the-Art Review. Int. J. Environ. Res. Public Health 2020, 17, 6506. [Google Scholar] [CrossRef]
- Lee, J.Y.; Lee, D.C. Cardiac and pulmonary benefits of forest walking versus city walking in elderly women: A randomised, controlled, open-label trial. Eur. J. Integr. Med. 2014, 6, 5–11. [Google Scholar] [CrossRef]
- Bang, K.S.; Lee, I.S.; Kim, S.J.; Song, M.K.; Park, S.E. The Effects of Urban Forest-walking Program on Health Promotion Behavior, Physical Health, Depression, and Quality of Life: A Randomized Controlled Trial of Office-workers. J. Korean Acad. Nurs. 2016, 46, 140–148. [Google Scholar] [CrossRef] [Green Version]
- Chun, M.H.; Chang, M.C.; Lee, S.J. The effects of forest therapy on depression and anxiety in patients with chronic stroke. Int. J. Neurosci. 2017, 127, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Ye, B.; Lv, X.; Mao, G.; Wang, S.; Chen, Z.; Wang, G. Adjunctive therapeutic effects of cinnamomum camphora forest environment on elderly patients with hypertension. Int. J. Gerontol. 2020, 14, 327–331. [Google Scholar] [CrossRef]
- Kim, J.G.; Khil, T.G.; Lim, Y.; Park, K.; Shin, M.; Shin, W.S. The psychological effects of a campus forest therapy program. Int. J. Environ. Res. Public Health 2020, 17, 3409. [Google Scholar] [CrossRef]
- Lee, I.; Choi, H.; Bang, K.-S.; Kim, S.; Song, M.; Lee, B. Effects of forest therapy on depressive symptoms among adults: A systematic review. Int. J. Environ. Res. Public Health 2017, 14, 321. [Google Scholar] [CrossRef] [PubMed]
- Ameli, R.; Skeath, P.; Abraham, P.A.; Panahi, S.; Kazman, J.B.; Foote, F.; Deuster, P.A.; Ahmad, N.; Berger, A. A nature-based health intervention at a military healthcare center: A randomized, controlled, cross-over study. PeerJ 2021, 9, e10519. [Google Scholar] [CrossRef] [PubMed]
- Bielinis, E.; Simkin, J.; Puttonen, P.; Tyrväinen, L. Effect of viewing video representation of the urban environment and forest environment on mood and level of procrastination. Int. J. Environ. Res. Public Health 2020, 17, 5109. [Google Scholar] [CrossRef] [PubMed]
- Zabini, F.; Albanese, L.; Becheri, F.R.; Gavazzi, G.; Giganti, F.; Giovanelli, F.; Gronchi, G.; Guazzini, A.; Laurino, M.; Li, Q. Comparative study of the restorative effects of forest and urban videos during COVID-19 lockdown: Intrinsic and benchmark values. Int. J. Environ. Res. Public Health 2020, 17, 8011. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Kim, S.; Park, J.; Seo, H.; Lee, Y.; Jang, B.; Son, H.; Suh, H.; Shin, C. NECA’s guidance for undertaking systematic reviews and meta-analyses for intervention. Seoul Natl. Evid.-Based Healthc. Collab. Agency 2011, 25, 129–199. Available online: https://www.neca.re.kr/lay1/bbs/S1T11C102/F/39/view.do?article_seq=5329&cpage=1&rows=10&condition=A.TITLE&keyword=%EC%B2%B4%EA%B3%84%EC%A0%81%20%EB%AC%B8%ED%97%8C%EA%B3%A0%EC%B0%B0&show=&cat= (accessed on 2 August 2021).
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Rothstein, H.R.; Sutton, A.J.; Borenstein, M. Publication Bias in Meta-Analysis: Prevention, Assessment and Adjustments; John Wiley & Sons: Chichester, UK, 2006. [Google Scholar]
- Chae, Y.R.; Lee, S.H. Systematic review of forest therapy program for adult patients with diseases. J. Korean Biol. Nurs. Sci. 2020, 22, 157–171. [Google Scholar] [CrossRef]
- Cuijpers, P. The challenges of improving treatments for depression. JAMA 2018, 320, 2529–2530. [Google Scholar] [CrossRef] [PubMed]
- Stigsdotter, U.K.; Palsdottir, A.M.; Burls, A.; Chermaz, A.; Ferrini, F.; Grahn, P. Nature-based therapeutic interventions. In Forests, Trees and Human Health; Springer: Dordrecht, The Netherlands, 2011; pp. 309–342. [Google Scholar]
- Rosa, C.D.; Larson, L.R.; Collado, S.; Profice, C.C. Forest therapy can prevent and treat depression: Evidence from meta-analyses. Urban For. Urban Green. 2020, 57, 126943. [Google Scholar] [CrossRef]
- Wolf, K.L.; Lam, S.T.; McKeen, J.K.; Richardson, G.R.; van den Bosch, M.; Bardekjian, A.C. Urban trees and human health: A scoping review. Int. J. Environ. Res. Public Health 2020, 17, 4371. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, M.; Barbieri, G.; Donelli, D. Effects of forest bathing (shinrin-yoku) on levels of cortisol as a stress biomarker: A systematic review and meta-analysis. Int. J. Biometeorol. 2019, 63, 1117–1134. [Google Scholar] [CrossRef] [PubMed]
- Song, M.K.; Bang, K.-S. A systematic review of forest therapy programs for elementary school students. Child Health Nurs. Res. 2017, 23, 300–311. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Kim, J.; Ju, H.J.; Jang, B.J.; Wang, T.K.; Kim, Y.I. Effect of forest therapy for menopausal women with insomnia. Int. J. Environ. Res. Public Health 2020, 17, 6548. [Google Scholar] [CrossRef]
- Furuyashiki, A.; Tabuchi, K.; Norikoshi, K.; Kobayashi, T.; Oriyama, S. A comparative study of the physiological and psychological effects of forest bathing (Shinrin-yoku) on working age people with and without depressive tendencies. Environ. Health Prev. Med. 2019, 24, 46. [Google Scholar] [CrossRef]
- Shin, Y.; Baek, J.; Chae, J. Application of Environmental Therapy: Focused on Forest Therapy and Hydrotherapy. Korean J. Stress Res. 2010, 18, 167–179. [Google Scholar]
- Shin, W.S.; Shin, C.S.; Yeoun, P.S. The influence of forest therapy camp on depression in alcoholics. Environ. Health Prev. Med. 2012, 17, 73–76. [Google Scholar] [CrossRef] [Green Version]
- Ochiai, H.; Ikei, H.; Song, C.; Kobayashi, M.; Takamatsu, A.; Miura, T.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M. Physiological and psychological effects of forest therapy on middle-aged males with high-normal blood pressure. Int. J. Environ. Res. Public Health 2015, 12, 2532–2542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.J. Factors Affecting the Mental Health of the Urban Elderly and Psychological Therapeutic Utilization of an Urban Forest. Ph.D. Thesis, Seoul National University, Seoul, Korea, 2019. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| Study | Country | Ex. | Com. | Experimental program | Comparator program | Outcome | D1 | D2 | D3 | D4 | D5 | Overall |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Zabini et al. (2020) | Italy | 41 | 34 | Forest Videos | Urban Videos | SPRAS, STAI |  | |  | | | |
| 2. Wu et al. (2020) | China | 20 | 11 | forest bathing | sit quietly on suburban site | POMS | | | | | | |
| 3. Kim et al. (2020) | Korea | 19 | 19 | forest therapy program (forest dance, forest meditation, forest exercise, walking) | no description | POMS, SRI-MF | | | | | | |
| 4. Bielinis et al. (2020) | Finland | 42 | 42 | Forest Videos | Urban Videos | POMS, ROS, SVS |  | | | | | |
| 5. Chun et al. (2017) | Korea | 30 | 29 | forest therapy program consisted of promoting positive emotion through meditation, experiencing the forest through all five senses and walking in the forest | The urban group stayed in a hotel. The meditation and walking activities were similarly performed in the urban area and the forest | BDI, HAM-D17, STAI | | | | | | |
| 6. Bang et al. (2016) | Korea | 18 | 27 | Forest-walking Program | no treatment | BDI, QOL | | | | | | |
: Low risk, : Some concerns, : High risk. D1: Randomisation process, D2: Deviations from the intended interventions, D3: Missing outcome data, D4: Measurement of the outcome, D5: Selection of the reported result.Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, M.-J.; Kim, H.-S.; Kim, J.-Y. Effects of Forest-Based Interventions on Mental Health: A Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2022, 19, 4884. https://doi.org/10.3390/ijerph19084884
Kang M-J, Kim H-S, Kim J-Y. Effects of Forest-Based Interventions on Mental Health: A Meta-Analysis of Randomized Controlled Trials. International Journal of Environmental Research and Public Health. 2022; 19(8):4884. https://doi.org/10.3390/ijerph19084884
Chicago/Turabian StyleKang, Mi-Jung, Hyun-Sun Kim, and Ji-Yeon Kim. 2022. "Effects of Forest-Based Interventions on Mental Health: A Meta-Analysis of Randomized Controlled Trials" International Journal of Environmental Research and Public Health 19, no. 8: 4884. https://doi.org/10.3390/ijerph19084884
APA StyleKang, M.-J., Kim, H.-S., & Kim, J.-Y. (2022). Effects of Forest-Based Interventions on Mental Health: A Meta-Analysis of Randomized Controlled Trials. International Journal of Environmental Research and Public Health, 19(8), 4884. https://doi.org/10.3390/ijerph19084884