
Personality Effects on Chinese Public Preference for the COVID-19 Vaccination: Discrete Choice Experiment and Latent Profile Analysis Study

 ,
,  , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Discrete Choice Experiment (DCE)
2.2.1. DCE Overview
2.2.2. Selection of Attributes and Levels
2.2.3. DCE Instrument Design
2.3. Data Collection
2.4. Questionnaire Composition
2.4.1. Demographic Characteristics and Vaccination Acceptance
2.4.2. The 10-Item Big Five Inventory (BFI-10)
2.4.3. DCE Scenarios
2.5. Statistical Analysis
2.5.1. Latent Profile Analysis
2.5.2. Conditional Logit Model
2.5.3. Willingness to Pay
3. Results
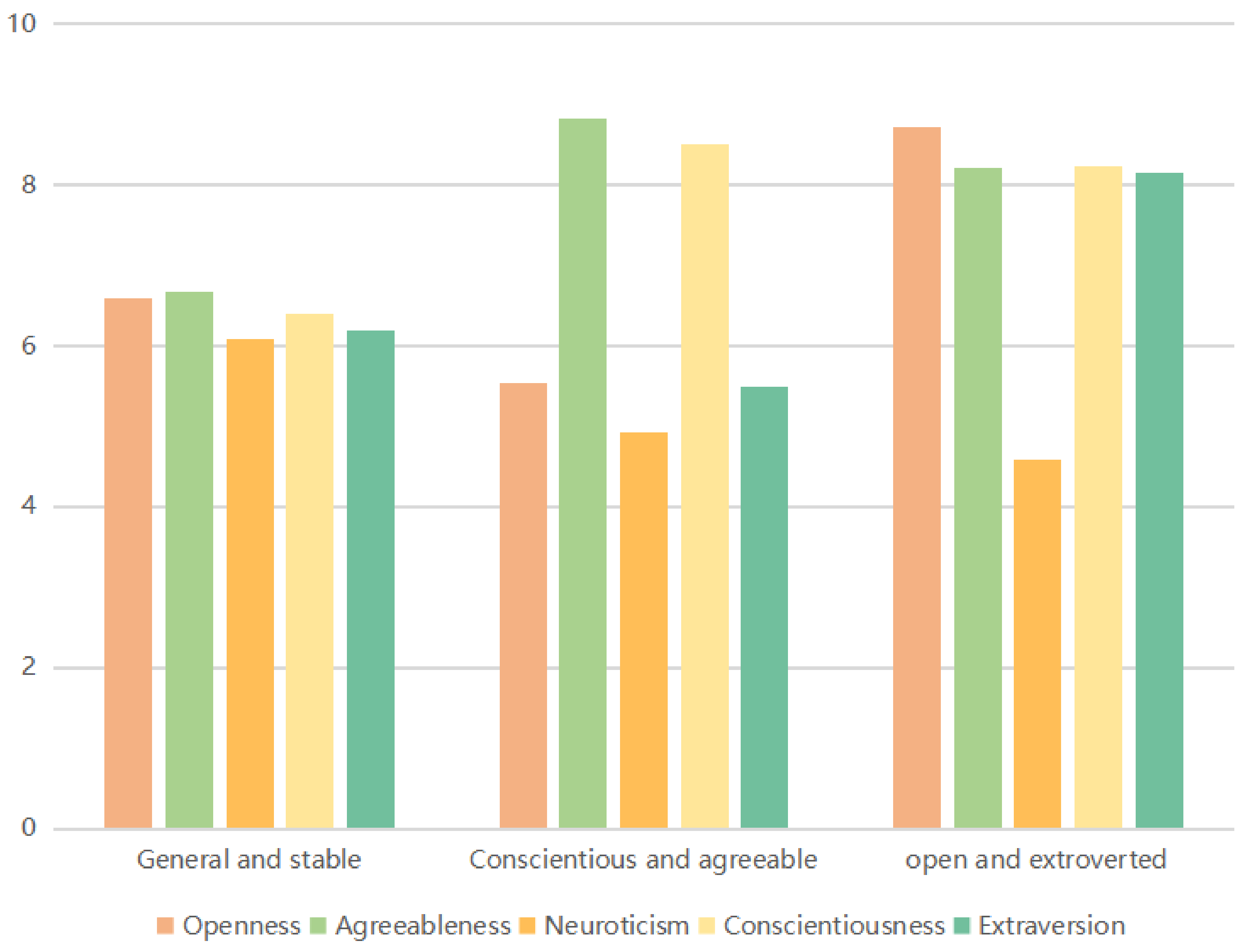
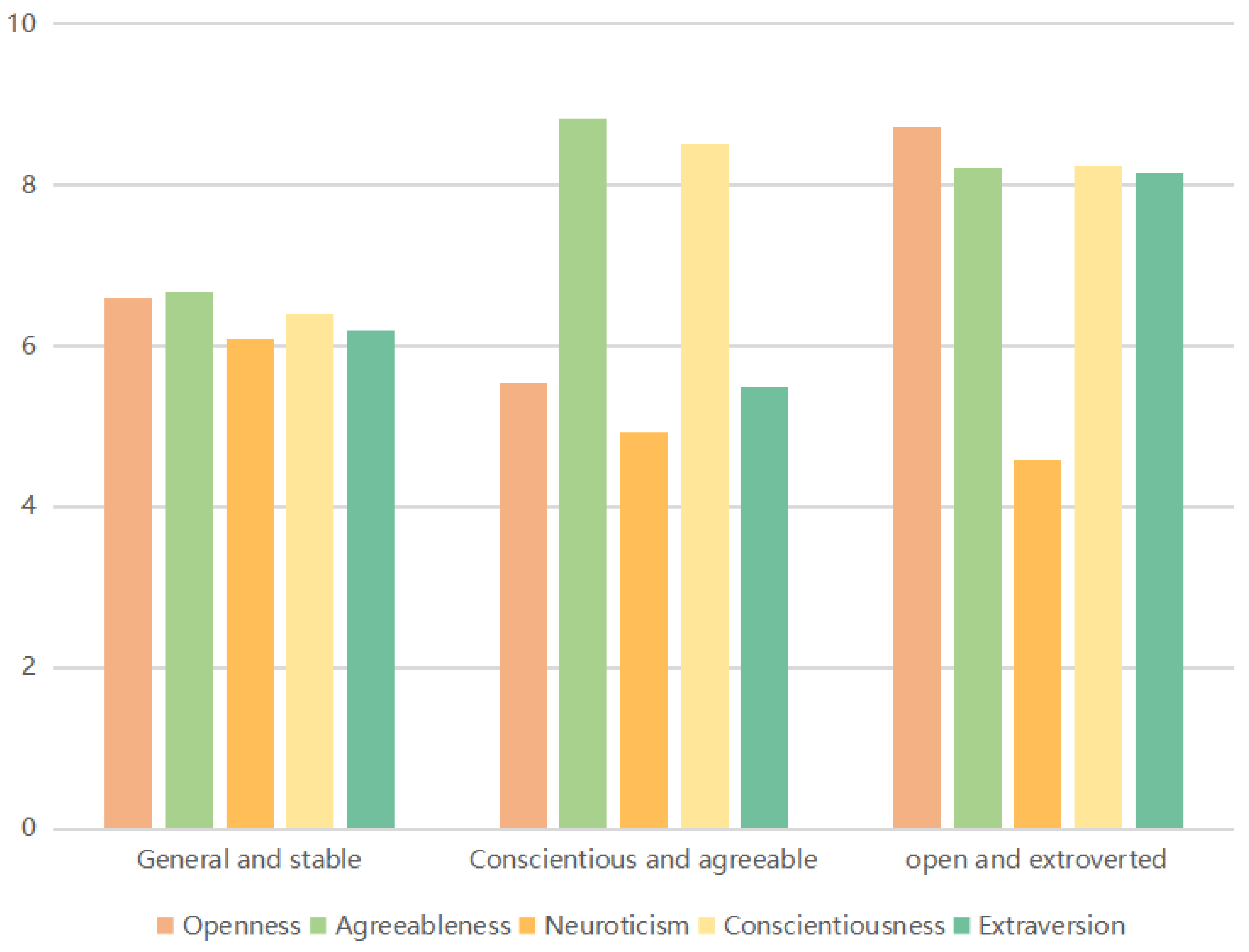
3.1. General Information and Latent Profile Analysis
3.2. DCE Results
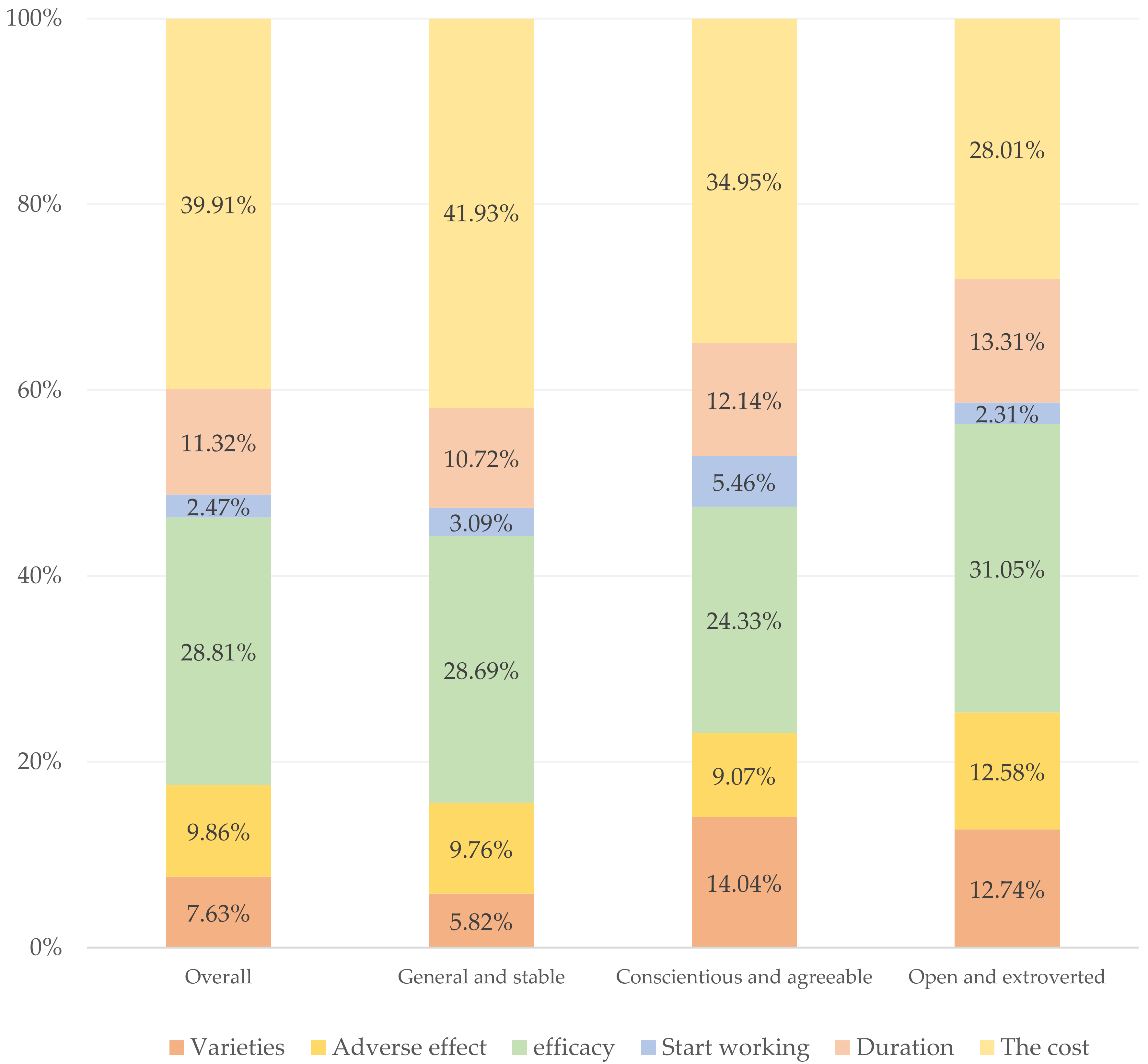
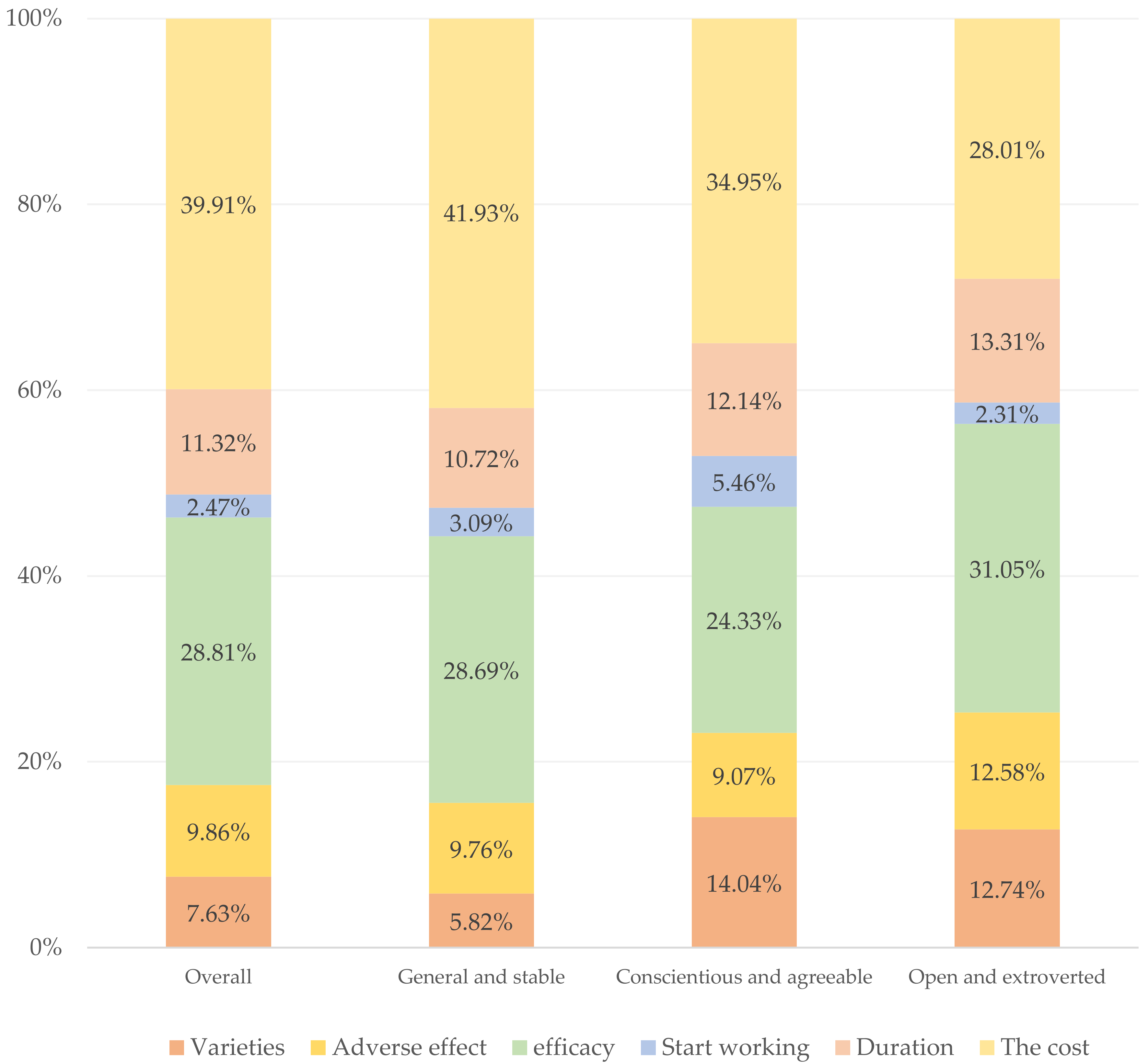
3.3. Overall WTP
4. Discussion
4.1. Principal Results
4.2. Suggestion
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 1 December 2021).
- DeRoo, S.S.; Pudalov, N.J.; Fu, L.Y.J.J. Planning for a COVID-19 vaccination program. J. Am. Med. Assoc. 2020, 323, 2458–2459. [Google Scholar] [CrossRef] [PubMed]
- Mills, M.; Rahal, C.; Brazel, D.; Yan, J.; Gieysztor, S. COVID-19 Vaccine Deployment: Behaviour, Ethics, Misinformation and Policy Strategies; The Royal Society & The British Academy: London, UK, 2020. [Google Scholar]
- Randolph, H.; Barreiro, L. Herd immunity: Understanding COVID-19. Immunity 2020, 52, 737–741. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.M.; Vegvari, C.; Truscott, J.; Collyer, B.S. Challenges in creating herd immunity to SARS-CoV-2 infection by mass vaccination. Lancet 2020, 396, 1614–1616. [Google Scholar] [CrossRef]
- Li, Q.; Wang, J.; Tang, Y.; Lu, H.Z. Next-generation COVID-19 vaccines: Opportunities for vaccine development and challenges in tackling COVID-19. Drug Discov. Ther. 2021, 15, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Different COVID-19 Vaccines. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines.html (accessed on 1 December 2021).
- Rawat, K.; Kumari, P.; Saha, L. COVID-19 vaccine: A recent update in pipeline vaccines, their design and development strategies. Eur. J. Pharm. 2021, 892, 173751. [Google Scholar] [CrossRef]
- Leilei, J. Domestic Vaccines Account for More Than 95% of the Country’s Actual Vaccination. Economic Daily, 7 June 2018. Available online: http://news.cctv.com/2018/06/07/ARTIIuehDvxFl4UACvwtljiy180607.shtml(accessed on 20 March 2022). (In Chinese)
- Shi, Z.W.; Huang, J.; Wei, S. Evaluation, challenges and countermeasures of current domestic COVID-19 vaccines. New Med. 2022, 32, 53–57. [Google Scholar]
- Huang, Z.; Fu, Z.; Wang, J. Review on drug regulatory science promoting COVID-19 vaccine development in China. Engineering 2022. [Google Scholar] [CrossRef]
- He, Q.; Mao, Q.; Zhang, J.; Bian, L.; Gao, F.; Wang, J. COVID-19 vaccines: Current understanding on immunogenicity, safety, and further considerations. Front. Immunol. 2021, 12, 669339. [Google Scholar] [CrossRef]
- World Health Organization. The COVID-19 Vaccines within WHO EUL/PQ Evaluation Process; World Health Organization: Geneva, Switzerland, 2021; Available online: https://extranet.who.int/pqweb/sites/default/fifiles/documents/Status_COVID_VAX_20Oct2021.pdf (accessed on 29 December 2021).
- People’s Daily Online. Two Sessions: 2.1 Billion Doses! The Responsibility of a Responsible Big Country. 3 March 2022. Available online: http://opinion.people.com.cn/n1/2022/0303/c1003-32365450.html (accessed on 20 March 2021).
- Pormohammad, A.; Zarei, M.; Ghorbani, S.; Mohammadi, M.; Razizadeh, M.H.; Turner, D.L.; Turner, R.J. Efficacy and Safety of COVID-19 Vaccines: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Vaccines 2021, 9, 467. [Google Scholar] [CrossRef]
- Torjesen, I. COVID-19: Norway investigates 23 deaths in frail elderly patients after vaccination. BMJ 2021, 372, n149. [Google Scholar] [CrossRef]
- Karim, S.S.A.; Karim, Q.A. Omicron SARS-CoV-2 variant: A new chapter in the COVID-19 pandemic. Lancet 2021, 398, 2126–2128. [Google Scholar] [CrossRef]
- Iacobucci, G. COVID-19: Single vaccine dose is 33% effective against variant from India, data show. Br. Med. J. 2021, 373, 2. [Google Scholar] [CrossRef] [PubMed]
- Lin, F.Y.; Wang, C.H. Personality and individual attitudes toward vaccination: A nationally representative survey in the United States. BMC Public Health 2020, 20, 1–8. [Google Scholar] [CrossRef] [PubMed]
- McCrae, R.R.; Costa, P. Personality Trait Structure as a Human Universal. Am. Psychol. 1997, 52, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Krupic, D.; Zuro, B.; Krupic, D. Big Five traits, approach-avoidance motivation, concerns and adherence with COVID-19 prevention guidelines during the peak of pandemic in Croatia. Personal. Individ. Differ. 2021, 179, 110913. [Google Scholar] [CrossRef]
- Garbe, L.; Rau, R.; Toppe, T. Influence of perceived threat of COVID-19 and HEXACO personality traits on toilet paper stockpiling. PLoS ONE 2020, 15, e0234232. [Google Scholar] [CrossRef]
- Asselmann, E.; Borghans, L.; Montizaan, R.; Seegers, P. The role of personality in the thoughts, feelings, and behaviors of students in Germany during the first weeks of the COVID-19 pandemic. PLoS ONE 2020, 15, 14. [Google Scholar] [CrossRef]
- Li, H.; Cao, Y. Your pain, my gain: The relationship between self-report and behavioral measures of everyday sadism and COVID-19 vaccination intention. Curr. Psychol. 2022, 1–8. [Google Scholar] [CrossRef]
- Clark, M.D.; Determann, D.; Petrou, S.; Moro, D.; de Bekker-Grob, E.W. Discrete Choice Experiments in Health Economics: A Review of the Literature. Pharmacoeconomics 2014, 32, 883–902. [Google Scholar] [CrossRef]
- Milte, R.; Ratcliffe, J.; Chen, G.; Lancsar, E.; Miller, M.; Crotty, M. Cognitive overload? an exploration of the potential impact of cognitive functioning in discrete choice experiments with older people in health care. Value Health 2014, 17, 655–659. [Google Scholar] [CrossRef]
- Bridges, J.F.P.; Hauber, A.B.; Marshall, D.; Lloyd, A.; Prosser, L.A.; Regier, D.A.; Johnson, F.R.; Mauskopf, J. Conjoint Analysis Applications in Health-a Checklist: A Report of the ISPOR Good Research Practices for Conjoint Analysis Task Force. Value Health 2011, 14, 403–413. [Google Scholar] [CrossRef] [PubMed]
- Fry, T.R.L. Stated choice methods analysis and application. Econ. Rec. 2001, 77, 312–314. [Google Scholar]
- Soekhai, V.; de Bekker-Grob, E.W.; Ellis, A.R.; Vass, C.M. Discrete choice experiments in health economics: Past, present and future. Pharmacoeconomics 2019, 37, 201–226. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.R.; He, Z.L.; Huang, J.; Yan, N.; Chen, Q.; Huang, F.Q.; Zhang, Y.J.; Akinwunmi, O.M.; Akinwunmi, B.O.; Zhang, C.J.P.; et al. A Comparison of Vaccine Hesitancy of COVID-19 Vaccination in China and the United States. Vaccines 2021, 9, 649. [Google Scholar] [CrossRef] [PubMed]
- Jones, I.; Roy, P.; Sputnik, V. COVID-19 vaccine candidate appears safe and effective. Lancet 2021, 397, 642–643. [Google Scholar] [CrossRef]
- Remmel, A. COVID vaccines and safety: What the research says. Nature 2021, 590, 538–540. [Google Scholar] [CrossRef]
- Tregoning, J.S.; Flight, K.E.; Higham, S.L.; Wang, Z.; Pierce, B.F. Progress of the COVID-19 vaccine effort: Viruses, vaccines and variants versus efficacy, effectiveness and escape. Nat. Rev. Immunol. 2021, 21, 626–636. [Google Scholar] [CrossRef]
- Kim, J.H.; Marks, F.; Clemens, J.D. Looking beyond COVID-19 vaccine phase 3 trials. Nat. Med. 2021, 27, 205–211. [Google Scholar] [CrossRef]
- Global Times. Sinovac’s COVID-19 Vaccine 78% Effective in Phase 3 Trial in Brazil. 2021. Available online: https://www.globaltimes.cn/page/202101/1212201.shtml (accessed on 12 March 2021).
- Zhang, Y.; Zeng, G.; Pan, H.; Li, C.; Hu, Y.; Chu, K.; Han, W.; Chen, Z.; Tang, R.; Yin, W.; et al. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine in healthy adults aged 18–59 years: A randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet Infect. Dis. 2021, 21, 181–192. [Google Scholar] [CrossRef]
- Wouters, O.; Shadlen, K.; Salcher-Konrad, M.; Pollard, A.; Larson, H.; Teerawattananon, Y.; Jit, M. Challenges in Ensuring Global Access To COVID-19 Vaccines: Production, Affordability, Allocation, And Deployment. Lancet 2021, 397, 1023–1034. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Effificacy of The BNT162b2 mRNA COVID-19 Vaccine. Engl. J. Med. 2021, 384, 1576–1578. [Google Scholar]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and Effificacy of The Chadox1 Ncov-19 Vaccine (AZD1222) Against SARS-CoV-2: An Interim Analysis of Four Randomised Controlled Trials in Brazil, South Africa, And The UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Gunst, R.F.; Mason, R.L. Fractional factorial design. Wiley Interdiscip. Rev. Comput. Stat. 2009, 1, 234–244. [Google Scholar] [CrossRef]
- Bailey, R.A. Balance, orthogonality and efficiency factors in factorial design. J. R. Stat. Soc. Ser. B-Methodol. 1985, 47, 453–458. [Google Scholar] [CrossRef]
- de Bekker-Grob, E.W.; Donkers, B.; Jonker, M.F.; Stolk, E.A. Sample Size Requirements for Discrete-Choice Experiments in Healthcare: A Practical Guide. Patient 2015, 8, 373–384. [Google Scholar] [CrossRef]
- Rammstedt, B.; John, O.P. Measuring personality in one minute or less: A 10-item short version of the Big Five Inventory in English and German. J. Res. Personal. 2007, 41, 203–212. [Google Scholar] [CrossRef]
- Yu, Y.; Zhou, M.; Guo, X.; He, Q.; Zhang, J. The Effect of Work-family Balance on Work Engagement and Job Satisfaction: The Moderating of Personality. Chin. J. Clin. Psychol. 2016, 24, 504. [Google Scholar]
- Carciofo, R.; Yang, J.Y.; Song, N.; Du, F.; Zhang, K. Psychometric Evaluation of Chinese-Language 44-Item and 10-Item Big Five Personality Inventories, Including Correlations with Chronotype, Mindfulness and Mind Wandering. PLoS ONE 2016, 11, e0149963. [Google Scholar] [CrossRef]
- Nylund, K.L.; Asparoutiov, T.; Muthen, B.O. Deciding on the number of classes in latent class analysis and growth mixture modeling: A Monte Carlo simulation study. Struct. Equ. Modeling Multidiscip. J. 2007, 14, 535–569. [Google Scholar] [CrossRef]
- Mangham, L.J.; Hanson, K. Employment preferences of public sector nurses in Malawi: Results from a discrete choice experiment. Trop. Med. Int. Health 2008, 13, 1433–1441. [Google Scholar] [CrossRef]
- Kolstad, J.R. How to make rural jobs more attractive to health workers: Findings from a discrete choice experiment in Tanzania. Health Econ. 2011, 20, 196–211. [Google Scholar] [CrossRef] [PubMed]
- McFadden, D. Conditional logit analysis of qualitative choice behavior. In Frontiers in Econometrics; Zarembka, P., Ed.; Academic Press: New York, NY, USA, 1974; pp. 105–142. [Google Scholar]
- Hauber, A.B.; González, J.M.; Groothuis-Oudshoorn, C.G.; Prior, T.; Marshall, D.A.; Cunningham, C. Statistical methods for the analysis of discrete choice experiments: A report of the ISPOR conjoint analysis good research practices task force. Value Health 2016, 19, 300–315. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Mogasale, V.; Lim, J.K.; Carabali, M.; Sirivichayakul, C.; Anh, D.D.; Lee, K.S.; Thiem, V.D.; Limkittikul, K.; Tho, L.H.; et al. A multi-country study of the household willingness-to-pay for dengue vaccines: Household surveys in Vietnam, Thailand, and Colombia. PLoS Negl. Trop. Dis. 2015, 9, e0003810. [Google Scholar] [CrossRef] [PubMed]
- McNeil, S.A.; Shinde, V.; Andrew, M.; Hatchette, T.F.; Leblanc, J.; Ambrose, A.; Boivin, G.; Bowie, W.R.; Diaz-Mitoma, F.; ElSherif, M.; et al. Interim estimates of 2013/14 influenza clinical severity and vaccine effectiveness in the prevention of laboratory-confirmed influenza-related hospitalisation, Canada, February 2014. Euro. Surveill. 2014, 19, 20729. [Google Scholar] [CrossRef]
- Hou, Z.; Chang, J.; Yue, D.; Fang, H.; Meng, Q.; Zhang, Y. Determinants of willingness to pay for self-paid vaccines in China. Vaccine 2014, 32, 4471–4477. [Google Scholar] [CrossRef]
- Berghea, F.; Berghea, C.E.; Abobului, M.; Vlad, V.M. Willingness to Pay for a for a Potential Vaccine Against SARS-CoV-2/COVID-19 Among Adult Persons. Value Health Reg. Issues 2020, 18–25. [Google Scholar] [CrossRef]
- Leng, A.L.; Maitland, E.; Wang, S.Y.; Nicholas, S.; Liu, R.G.; Wang, J. Individual preferences for COVID-19 vaccination in China. Vaccine 2021, 39, 247–254. [Google Scholar] [CrossRef]
- Carpio, C.E.; Sarasty, O.; Hudson, D.; Macharia, A.; Shibia, M. The demand for a COVID-19 vaccine in ecuador. Vaccine 2020, 38, 8090–8098. [Google Scholar]
- Catma, S.; Reindl, D. Parents’ willingness to pay for a COVID-19 vaccine for themselves and their children in the United States. Hum. Vaccin. Immunother. 2021, 17, 2919–2925. [Google Scholar] [CrossRef]
- McCrae, R.R.; Costa, P.T., Jr. The Five-Factor Theory of Personality. In Handbook of Personality: Theory and Research, 3rd ed.; John, O.P., Robins, R.W., Pervin, L.A., Eds.; The Guilford Press: New York, NY, USA, 2008; pp. 159–181. [Google Scholar]
- Sallam, M. COVID-19 vaccine hesitancy worldwide: A concise systematic review of vaccine acceptance rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Schwaba, T.; Luhmann, M.; Denissen, J.J.A.; Chung, J.M.; Bleidorn, W. Openness to Experience and Culture-Openness Transactions Across the Lifespan. J. Personal. Soc. Psychol. 2018, 115, 118–136. [Google Scholar] [CrossRef] [PubMed]
- Schwaba, T.; Robins, R.W.; Grijalva, E.; Bleidorn, W. Does openness to experience matter in love and work? Domain, facet, and developmental evidence from a 24-year longitudinal study. J. Personal. 2019, 87, 1074–1092. [Google Scholar] [CrossRef] [PubMed]
- Soto, C.J.; John, O.P. The Next Big Five Inventory (BFI-2): Developing and assessing a hierarchical model with 15 facets to enhance bandwidth, fidelity, and predictive power. J. Personal. Soc. Psychol. 2017, 113, 117–143. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, L.D.F.; Pianowski, G.; Gonçalves, A.P. Personality differences and COVID-19: Are extroversion and conscientiousness personality traits associated with engagement with containment measures? Trends Psychiatry Psychother. 2020, 42, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Roberts, B.W.; Lejuez, C.; Krueger, R.F.; Richards, J.M.; Hill, P.L. What is conscientiousness and how can it be assessed? Dev. Psychol. 2014, 50, 1315. [Google Scholar] [CrossRef]
- Aschwanden, D.; Strickhouser, J.E.; Sesker, A.A.; Lee, J.H.; Luchetti, M.; Stephan, Y.; Sutin, A.R.; Terracciano, A. Psychological and Behavioural Responses to Coronavirus Disease 2019: The Role of Personality. Eur. J. Personal. 2021, 35, 51–66. [Google Scholar] [CrossRef]
- Bogg, T.; Roberts, B.W. Conscientiousness and health-related behaviors: A meta-analysis of the leading behavioral contributors to mortality. Psychol. Bull. 2004, 130, 887–919. [Google Scholar] [CrossRef]
- Chang, J.H.; Han, D.; Wang, D. Comparison of Mental Health Status and Behaviour of Chinese Medical and Non-Medical College Students During the Coronavirus Disease 2019 (COVID-19) Pandemic. Psychosom. Med. Res. 2021, 3, 42–52. [Google Scholar]
- Bogg, T.; Milad, E. Slowing the Spread of COVID-19: Demographic, Personality, and Social Cognition Predictors of Guideline Adherence in a Representative U.S. Sample. PsyArXiv 2020, 10, yc2gq. [Google Scholar] [CrossRef]
- Dai, L.P.; Gao, G.F. Viral targets for vaccines against COVID-19. Nat. Rev. Immunol. 2021, 21, 73–82. [Google Scholar] [CrossRef]
- Rojas-Perez-Ezquerra, P.; Quiros, J.C.; Molina, P.T.; de Ocariz, M.; Ortuno, J.M.Z. Safety of New mRNA Vaccines Against COVID-19 in Severely Allergic Patients. J. Investig. Allergol. Clin. Immunol. 2021, 31, 180–181. [Google Scholar] [CrossRef] [PubMed]
- Hajek, A.; Enzenbach, C.; Stengler, K.; Glaesmer, H.; Hinz, A.; Rohr, S.; Stein, J.; Riedel-Heller, S.G.; Konig, H.H. Determinants of Willingness to Pay for Health Insurance in Germany-Results of the Population-Based Health Study of the Leipzig Research Centre for Civilization Diseases (LIFE-Adult-Study). Front. Public Health 2020, 8, 456. [Google Scholar] [CrossRef] [PubMed]
- Qian, K.; Yahara, T. Mentality and behavior in COVID-19 emergency status in Japan: Influence of personality, morality and ideology. PLoS ONE 2020, 15, e0235883. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 29. [Google Scholar] [CrossRef]
- Wu, Y.B.; Liu, S.T.; He, X.Z.; Yu, C.; Huang, X.D.; Shi, L.L.; Tang, Q. The public and medical staff understanding of COVID-19: A large sample, multi-center, cross-sectional study. J. Emerg. Manag. Disaster Commun. 2020, 1, 21–31. [Google Scholar] [CrossRef]
- World Health Organization. Report of the SAGE Working Group on Vaccine Hesitancy; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Xinhua Net. China to Make COVID-19 Vaccine Global Public Good. 2020. Available online: http://www.xinhuanet.com/english/2020-06/07/c_139121278.htm (accessed on 1 December 2021).

{kind=link}
{kind=link}
| Attributes | Levels of Attributes | Explain |
|---|---|---|
| Vaccine varieties | mRNA vaccine | Several common vaccines are produced by countries at present. |
| Adenovirus vector vaccine | ||
| Inactivated vaccine | ||
| Adverse effect | Very mild | The extent of possible side effects of vaccination with COVID-19. |
| mild | ||
| Moderate | ||
| Efficacy | 55% | Effectiveness of vaccination against infection with COVID-19 |
| 65% | ||
| 75% | ||
| 85% | ||
| 95% | ||
| Time for the vaccine to start working | 5 days | Time from the time the COVID-19 vaccine is administered until the time the vaccine begins to work in the body. |
| 10 days | ||
| 15 days | ||
| 20 days | ||
| The duration of vaccine works | 5 months | Duration of time that a COVID-19 vaccine takes effect in the body until it ceases to be effective. |
| 10 months | ||
| 15 months | ||
| 20 months | ||
| The cost of vaccination | $0 | The total cost of vaccinating COVID-19 |
| $50 | ||
| $100 | ||
| $150 | ||
| $200 |
| Attributes | Vaccine A | Vaccine B | Neither |
|---|---|---|---|
| Vaccine varieties | Inactivated vaccine | mRNA vaccine | Neither |
| Adverse effect | mild | Very mild | |
| Efficacy | 95% | 55% | |
| Time for the vaccine to start working | 20 days | 10 days | |
| The duration of vaccine works | 5 months | 20 months | |
| The cost of vaccination | $0 | $0 |
| Number of Profiles | AIC | BIC | ABIC | Entropy | p-Value of LMRT |
|---|---|---|---|---|---|
| 1 | 21,759.116 | 21,810.017 | 21,778.253 | ||
| 2 | 21,535.778 | 21,617.22 | 21,566.397 | 0.677 | 0.6492 |
| 3 | 21,439.248 | 21,551.23 | 21,481.349 | 0.722 | 0.0215 |
| 4 | 21,405.553 | 21,548.076 | 21,459.137 | 0.708 | 0.1956 |
| 5 | 21,359.904 | 21,532.967 | 21,424.97 | 0.719 | 0.1031 |
| Demographic Items | General and Stable Type (n = 956) | Conscientious and Agreeable Type (n = 114) | Open and Extroverted Type (n = 130) | F Value | p-Value |
|---|---|---|---|---|---|
| Gender (%) | 2.149 | 0.117 | |||
| Male | 408 (56.1%) | 37 (32.5) | 50 (38.5%) | ||
| Female | 544 (33.3%) | 77 (67.5) | 80 (61.5%) | ||
| Other | 4 (7.9%) | 0 (0%) | 0 (0%) | ||
| Age interval in years (%) | 2.164 | 0.115 | |||
| 18–40 | 592 (61.9%) | 54 (47.4) | 87 (66.9%) | ||
| 41–60 | 225 (23.5%) | 48 (42.1) | 29 (22.3%) | ||
| Above 60 | 139 (14.5%) | 12 (10.5) | 14 (10.8%) | ||
| Highest educational level (%) | 2.376 | 0.093 | |||
| Pre-primary education or primary school education | 77 (8.1%) | 12 (10.5%) | 4 (3.1%) | ||
| Middle school education | 127 (13.3%) | 11 (9.6%) | 12 (9.2%) | ||
| High school education | 159 (16.6%) | 11 (9.6%) | 25 (19.2%) | ||
| Vocational school education | 164 (17.2%) | 33 (28.9%) | 16 (12.3%) | ||
| Bachelor’s degree | 360 (37.7%) | 41 (36%) | 66 (50.8%) | ||
| Master’s degree | 56 (5.9%) | 4 (3.5%) | 6 (4.6%) | ||
| Ph.D. degree | 13 (1.4%) | 2 (1.8%) | 1 (0.8%) | ||
| Annual salary level (%) | 1.447 | 0.236 | |||
| Under USD 10,000 | 619 (64.7%) | 64 (56.1%) | 86 (66.2%) | ||
| USD 10,001–30,000 | 261 (27.3%) | 38 (33.3%) | 34 (26.2%) | ||
| USD 30,001–50,000 | 52 (5.4%) | 9 (7.9%) | 8 (6.2%) | ||
| Above USD 50,000 | 24 (2.5%) | 3 (2.6%) | 2 (1.5%) | ||
| Acceptance of vaccination (totally unwilling, 0–totally willing, 10) | 4.669 | 0.01 | |||
| Average | 8.96 | 9.18 | 9.45 | ||
| Attributes and Levels | Overall, n = 1200 (100%) | General and Stable Type, | Conscientious and Agreeable Type, n = 114 (9.5%) | Open and Extroverted Type, n = 135 (10.7%) | ||||
|---|---|---|---|---|---|---|---|---|
| n = 956 (79.7%) | ||||||||
| Coefficient | Odds Ratio (95%CI) | Coefficient | Odds Ratio (95%CI) | Coefficient | Odds Ratio (95%CI) | Coefficient | Odds Ratio (95%CI) | |
| Varieties | ||||||||
| mRNA vaccines | −0.081 *** | REF | −0.064 ** | REF | −0.183 * | REF | −0.126 | REF |
| Adenovirus vector vaccines | −0.117 *** | 0.964 (0.925–1.006) | −0.085 *** | 0.979 (0.934–1.026) | −0.255 *** | 0.930 (0.810–1.069) | −0.236 *** | 0.896 (0.788–1.020) |
| Inactivated vaccines | 0.198 *** | 1.32 (1.267–1.376) | 0.149 *** | 1.237 (1.181–1.296) | 0.437 *** | 1.859 (1.624–2.128) | 0.362 *** | 1.629 (1.436–1.848) |
| Adverse effect | ||||||||
| very mild | 0.153 *** | REF | 0.156 *** | REF | 0.165 * | REF | 0.129 * | REF |
| mild | 0.099 *** | 0.947 (0.909–0.988) | 0.080 ** | 0.926 (0.884–0.971) | 0.118 | 0.954 (0.833–1.093) | 0.231 *** | 1.108 (0.977–1.256) |
| moderate | −0.253 *** | 0.666 (0.639–0.695) | −0.236 *** | 0.676 (0.644–0.709) | −0.283 *** | 0.639 (0.554–0.737) | −0.359 *** | 0.614 (0.538–0.700) |
| Efficacy | ||||||||
| 55% | −0.601 *** | REF | −0.574 *** | REF | −0.726 *** | REF | −0.700 *** | REF |
| 65% | −0.282 *** | 1.375 (1.292–1.464) | −0.289 *** | 1.330 (1.239–1.428) | −0.155 | 1.770 (1.444–2.169) | −0.387 *** | 1.367 (1.129–1.656) |
| 75% | 0.008 | 1.839 (1.731–1.953) | −0.028 | 1.726 (1.612–1.848) | 0.165 | 2.438 (2.006–2.962) | 0.150 | 2.340 (1.947–2.811) |
| 85% | 0.289 *** | 2.435 (2.295–2.583) | 0.312 *** | 2.426 (2.270–2.592) | 0.244 * | 2.638 (2.166–3.213) | 0.180 | 2.410 (2.010–2.888) |
| 95% | 0.585 *** | 3.273 (3.086–3.473) | 0.579 *** | 3.166 (2.963–3.383) | 0.473 *** | 3.318 (2.725–4.040) | 0.756 *** | 4.289 (3.578–5.140) |
| Start working | ||||||||
| 5 days | −0.017 | REF | −0.010 | REF | −0.160 | REF | 0.049 | REF |
| 10 days | 0.021 | 1.039 (0.987–1.095) | 0.013 | 1.024 (0.966–1.085) | 0.109 | 1.309 (1.104–1.552) | 0.002 | 0.954 (0.815–1.116) |
| 15 days | 0.049 | 1.069 (1.015–1.125) | 0.060 * | 1.073 (1.012–1.138) | 0.020 | 1.197 (1.007–1.424) | 0.009 | 0.961 (0.822–1.124) |
| 20 days | −0.053 * | 0.965 (0.916–1.017) | −0.064 * | 0.948 (0.894–1.006) | 0.030 | 1.210 (1.017–1.438) | −0.059 | 0.897 (0.767–1.049) |
| Duration | ||||||||
| 5 months | −0.282 *** | REF | −0.274 *** | REF | −0.332 *** | REF | −0.317 *** | REF |
| 10 months | −0.005 | 1.319 (1.252–1.389) | 0.002 | 1.318 (1.244–1.398) | −0.024 | 1.361 (1.145–1.618) | −0.012 | 1.356 (1.160–1.585) |
| 15 months | 0.104 *** | 1.471 (1.397–1.549) | 0.115 *** | 1.476 (1.393–1.564) | 0.089 | 1.523 (1.283–1.807) | 0.021 | 1.402 (1.199–1.640) |
| 20 months | 0.184 *** | 1.593 (1.514–1.677) | 0.157 *** | 1.538 (1.452–1.630) | 0.267 ** | 1.819 (1.538–2.152) | 0.308 *** | 1.867 (1.600–2.178) |
| The cost | ||||||||
| $0 | 0.924 *** | REF | 0.948 *** | REF | 0.974 *** | REF | 0.751 *** | REF |
| $50 | 0.217 *** | 0.493 (0.465–0.523) | 0.232 *** | 0.489 (0.458–0.522) | 0.160 | 0.443 (0.365–0.538) | 0.157 | 0.522 (0.461–0.661) |
| $100 | −0.128 *** | 0.349 (0.329–0.371) | −0.151 *** | 0.333 (0.311–0.357) | −0.126 | 0.333 (0.272–0.407) | 0.032 | 0.487 (0.406–0.585) |
| $150 | −0.294 *** | 0.296 (0.278–0.315) | −0.292 *** | 0.290 (0.270–0.311) | −0.258 * | 0.292 (0.238–0.358) | −0.378 *** | 0.323 (0.267–0.391) |
| $200 | −0.719 *** | 0.193 (0.181–0.207) | −0.737 *** | 0.186 (0.172–0.200) | −0.749 *** | 0.179 (0.143–0.224) | −0.562 *** | 0.269 (0.221–0.328) |
| Attributes and Levels | Overall (n = 1200) (USD) | General and Stable Type (n = 951) (USD) | Conscientious and Agreeable Type (n = 114) (USD) | Open and Extroverted Type (n = 135) (USD) |
|---|---|---|---|---|
| Varieties | ||||
| Adenovirus vector vaccines | REF | REF | REF | REF |
| mRNA vaccines | 1.84 | 0.08 | 8.03 | 3.96 |
| Inactivated vaccines | 26.25 | 34.45 | 59.18 | 75.10 |
| Adverse effect | ||||
| moderate | REF | REF | REF | REF |
| very mild | 30.55 | 55.96 | 50.00 | 44.80 |
| mild | 20.00 | 38.04 | 48.54 | 63.57 |
| Efficacy | ||||
| 55% | REF | REF | REF | REF |
| 65% | 9.35 | 17.55 | 25.15 | 21.09 |
| 75% | 16.58 | 31.51 | 40.75 | 84.28 |
| 85% | 66.38 | 73.83 | 62.61 | 88.28 |
| 95% | 222.36 | 115.53 | 94.86 | 162.34 |
| Start working | ||||
| 5 days | REF | REF | REF | REF |
| 10 days | −0.38 | −3.87 | 30.18 | 3.81 |
| 15 days | 0.20 | −0.48 | 23.98 | −1.46 |
| 20 days | −3.38 | −6.50 | 18.75 | 0.59 |
| Duration | ||||
| 5 months | REF | REF | REF | REF |
| 10 months | 19.22 | 37.23 | 7.68 | 37.01 |
| 15 months | 33.28 | 68.80 | 31.98 | 50.29 |
| 20 months | 62.28 | 75.39 | 61.72 | 80.79 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, J.; Ge, P.; Li, X.; Yin, M.; Wang, Y.; Ming, W.; Li, J.; Li, P.; Sun, X.; Wu, Y. Personality Effects on Chinese Public Preference for the COVID-19 Vaccination: Discrete Choice Experiment and Latent Profile Analysis Study. Int. J. Environ. Res. Public Health 2022, 19, 4842. https://doi.org/10.3390/ijerph19084842
Zhang J, Ge P, Li X, Yin M, Wang Y, Ming W, Li J, Li P, Sun X, Wu Y. Personality Effects on Chinese Public Preference for the COVID-19 Vaccination: Discrete Choice Experiment and Latent Profile Analysis Study. International Journal of Environmental Research and Public Health. 2022; 19(8):4842. https://doi.org/10.3390/ijerph19084842
Chicago/Turabian StyleZhang, Jinzi, Pu Ge, Xialei Li, Mei Yin, Yujia Wang, Waikit Ming, Jinhui Li, Pei Li, Xinying Sun, and Yibo Wu. 2022. "Personality Effects on Chinese Public Preference for the COVID-19 Vaccination: Discrete Choice Experiment and Latent Profile Analysis Study" International Journal of Environmental Research and Public Health 19, no. 8: 4842. https://doi.org/10.3390/ijerph19084842
APA StyleZhang, J., Ge, P., Li, X., Yin, M., Wang, Y., Ming, W., Li, J., Li, P., Sun, X., & Wu, Y. (2022). Personality Effects on Chinese Public Preference for the COVID-19 Vaccination: Discrete Choice Experiment and Latent Profile Analysis Study. International Journal of Environmental Research and Public Health, 19(8), 4842. https://doi.org/10.3390/ijerph19084842