
Assessment of Subjective Well-Being in a Cohort of University Students and Staff Members: Association with Physical Activity and Outdoor Leisure Time during the COVID-19 Pandemic

 ,
,  ,
,  ,
, 
 ,
,  ,
,  ,
,  ,
, 
 , , and
, , and 
Abstract
:1. Introduction
- the simultaneous use of multiple complementary measurement tools to comparatively assess the mental health perceptions of an Italian subpopulation of young university students versus a subpopulation of adult university employees during a specific period of the pandemic COVID-19;
- the assessment of the levels of PA, leisure activity and perception of energy levels in the two subpopulations during the same period;
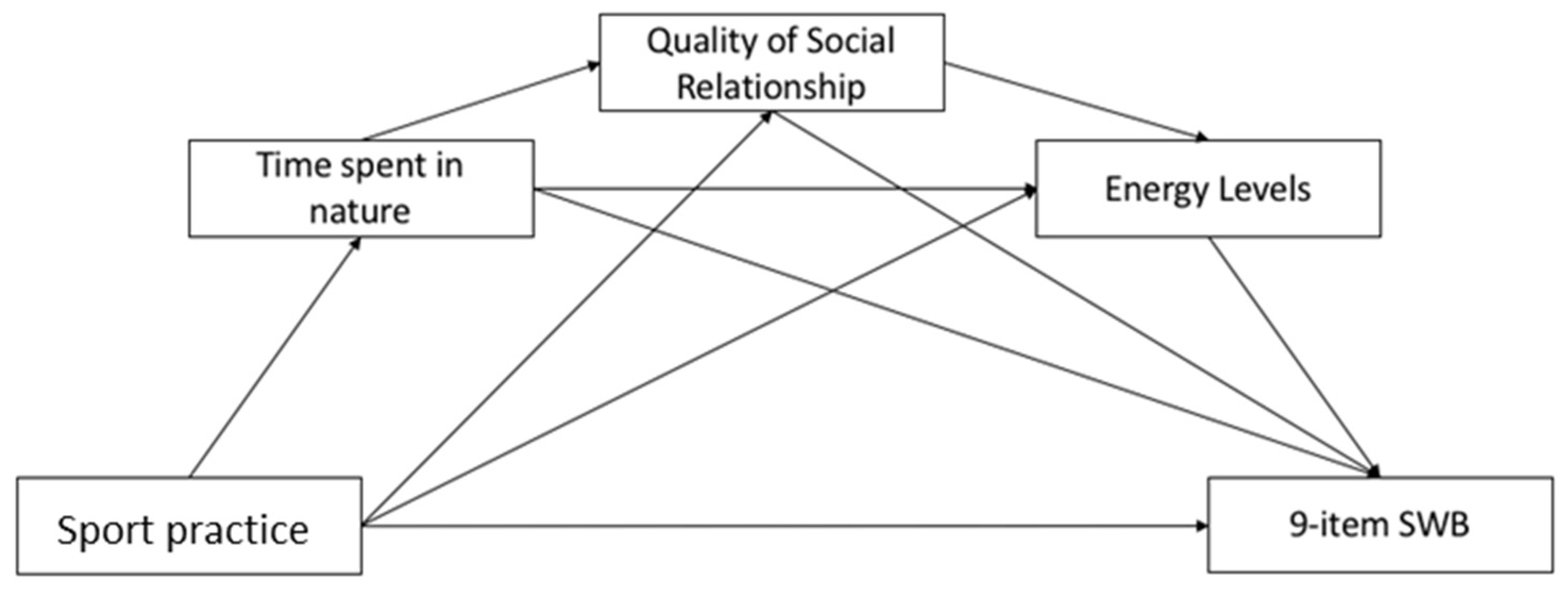
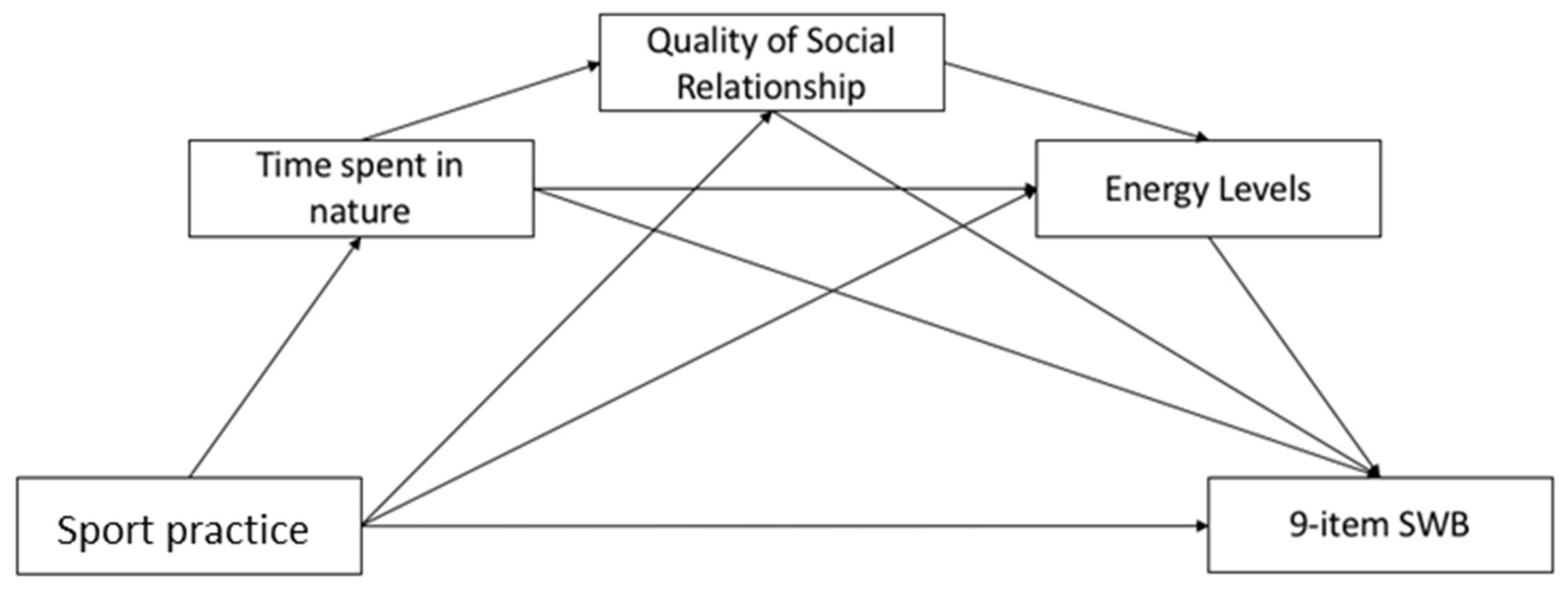
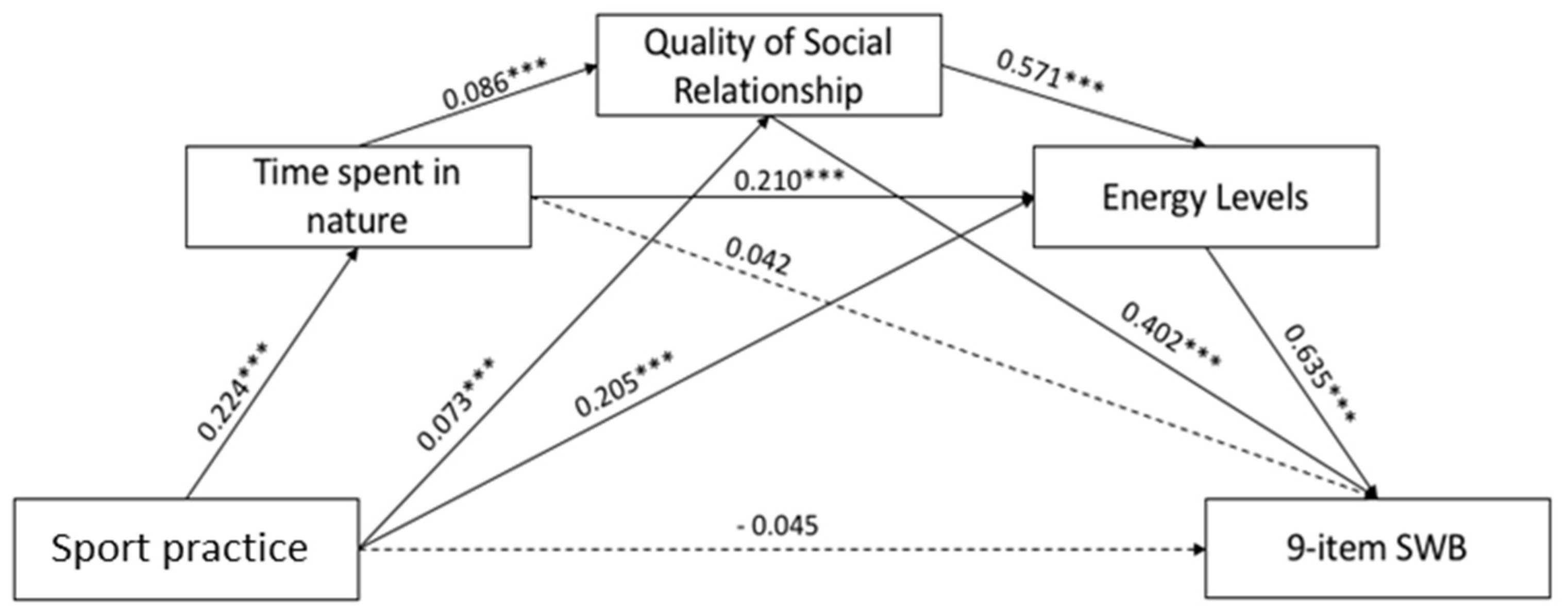
- evaluating the association between (1) and (2) through correlation analyses and a mediation model, which combine the role of time spent in nature, perceived individual energy level, and social relationships on the relationship between PA and subjective well-being.
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Procedure and Measures
- Socio-demographic characteristics (age, sex, nationality, marital status, cohousing conditions, total household income per month, employment status);
- Body health status (based on the reported weight and height by the participants and the estimation of the body mass index (BMI), as well as by the self-reported declaration of any recent diagnosed disease (yes/no);
- Comprehensive evaluation of the mental health perception. We applied three independent psychological tools.
- 4.
- Energy levels. The evaluation of energy levels was computed on three items adapted from the Lee’s Fatigue scale [51]: (1) Last week, how energetic did you normally feel in the middle of the day?; (2) Last week, how tired did you normally feel in the middle of the day?; and (3) Last week, how efficient did you normally feel in the middle of the day?. Total score was calculated as the average of all three items (Table 1).
- 5.
- Physical activity habits. The evaluation of the levels of PA of the participants was conducted by administering the following ad hoc question: If you practice sport, on average, last month, how frequently did you practice exercise? The answer was given according to the 4-point Likert scale and pass through points 0 = Never; 1 = Occasionally, but not regularly; 2 = Regularly, less than 150 min per week; 3 = Regularly, 150 min or more per week. The cut-off points were: low (never or occasionally) and moderate/high (regularly).
2.3. Covariates
2.4. Data Analysis
3. Results
3.1. Participants Sociodemographic Characteristics and Body Health Status
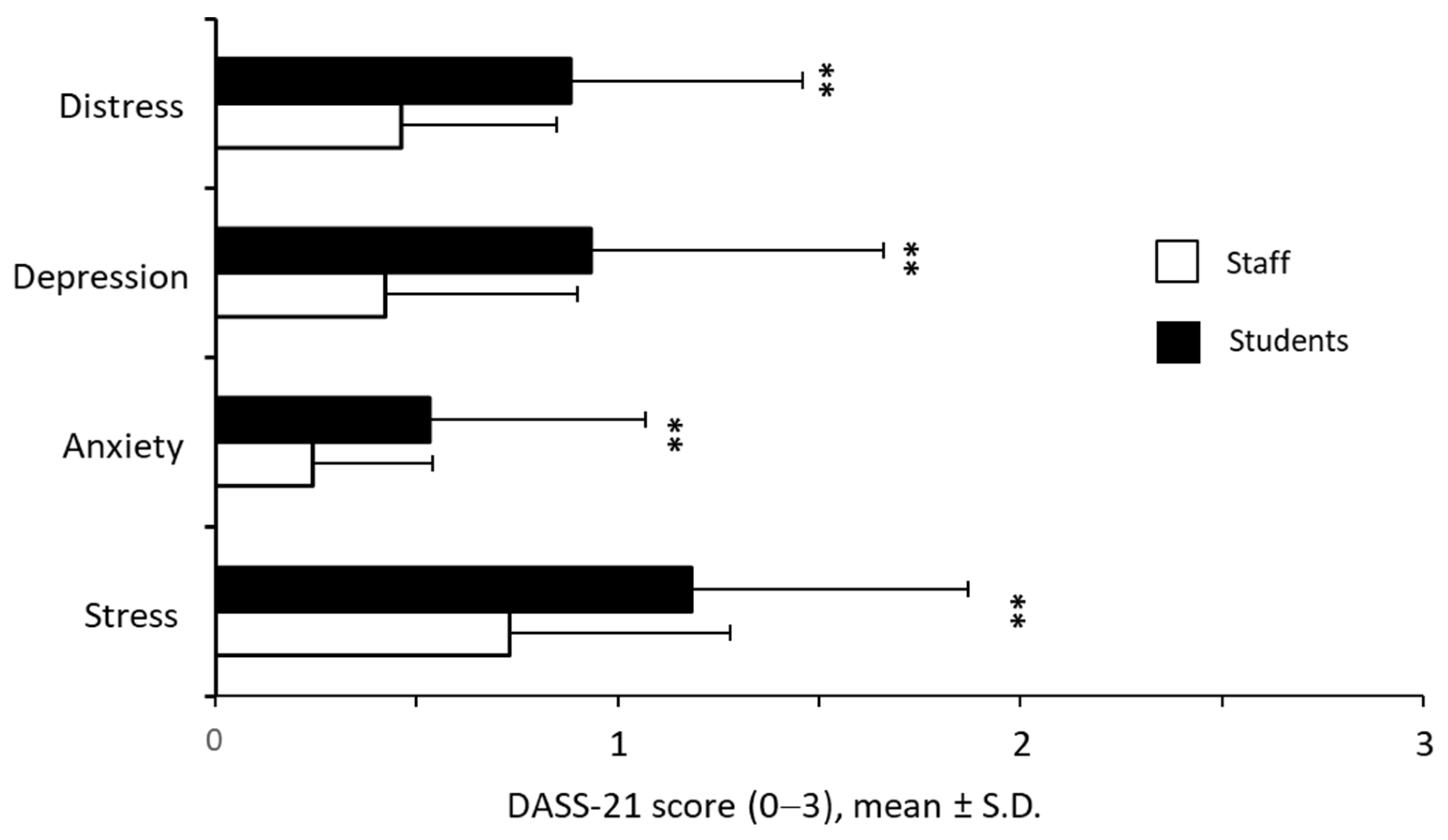
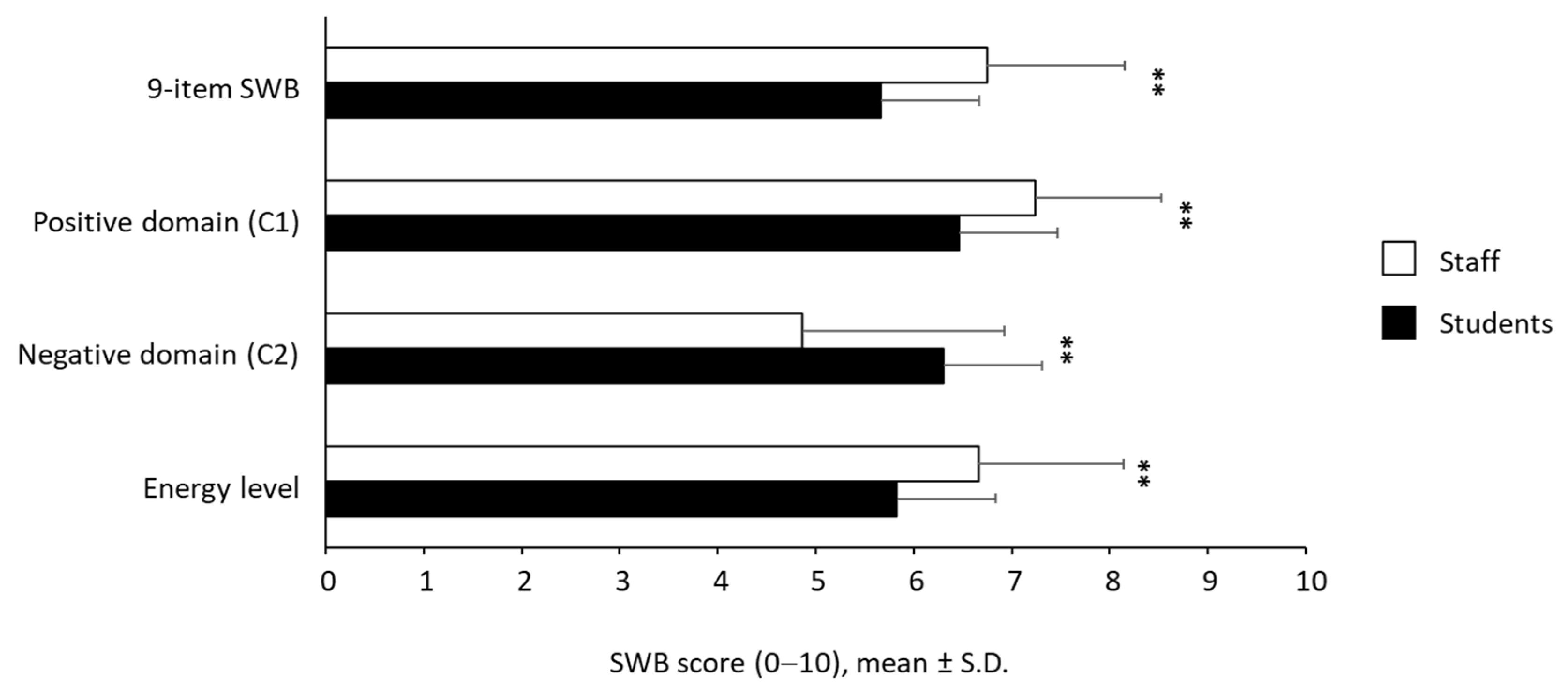
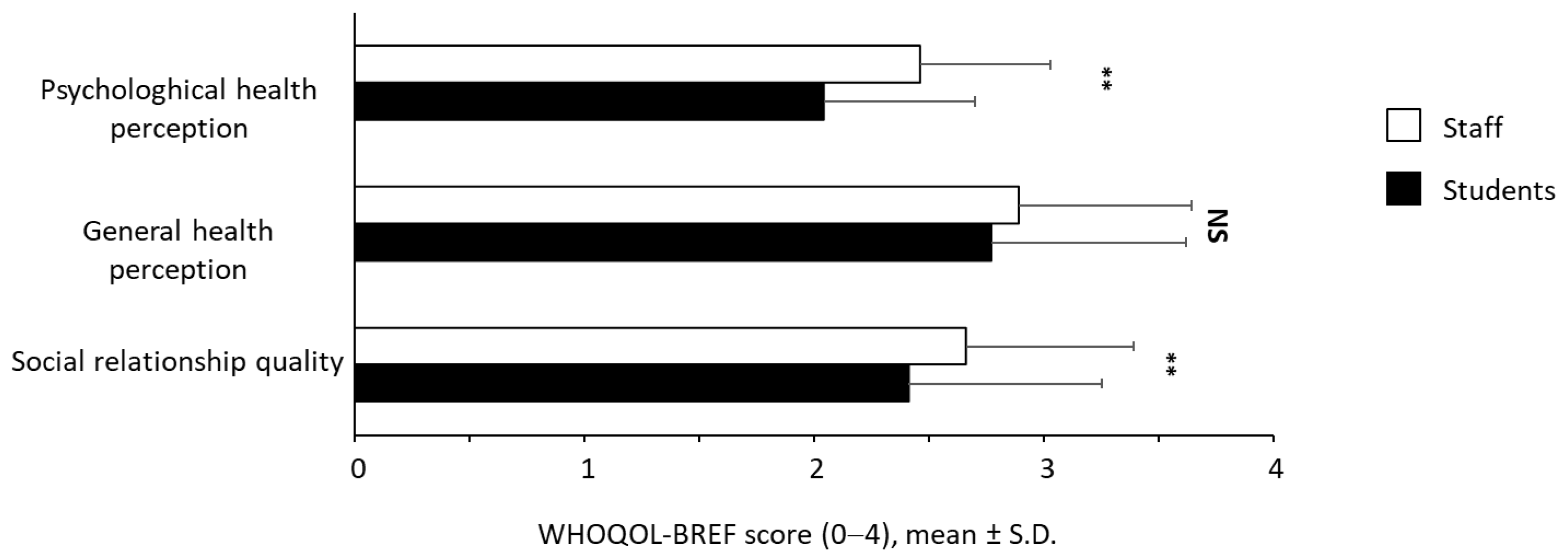
3.2. Evaluation of Distress and Subjective Well-Being in the Student and Staff Member Subpopulations
3.3. Validation of the 9-Item SWB Index with the Two Subdomains
3.4. Distribution of PA Levels among Students and Staff Members
3.5. Association between Distress, SWB, Physical Activities Levels and Time Spent in Nature
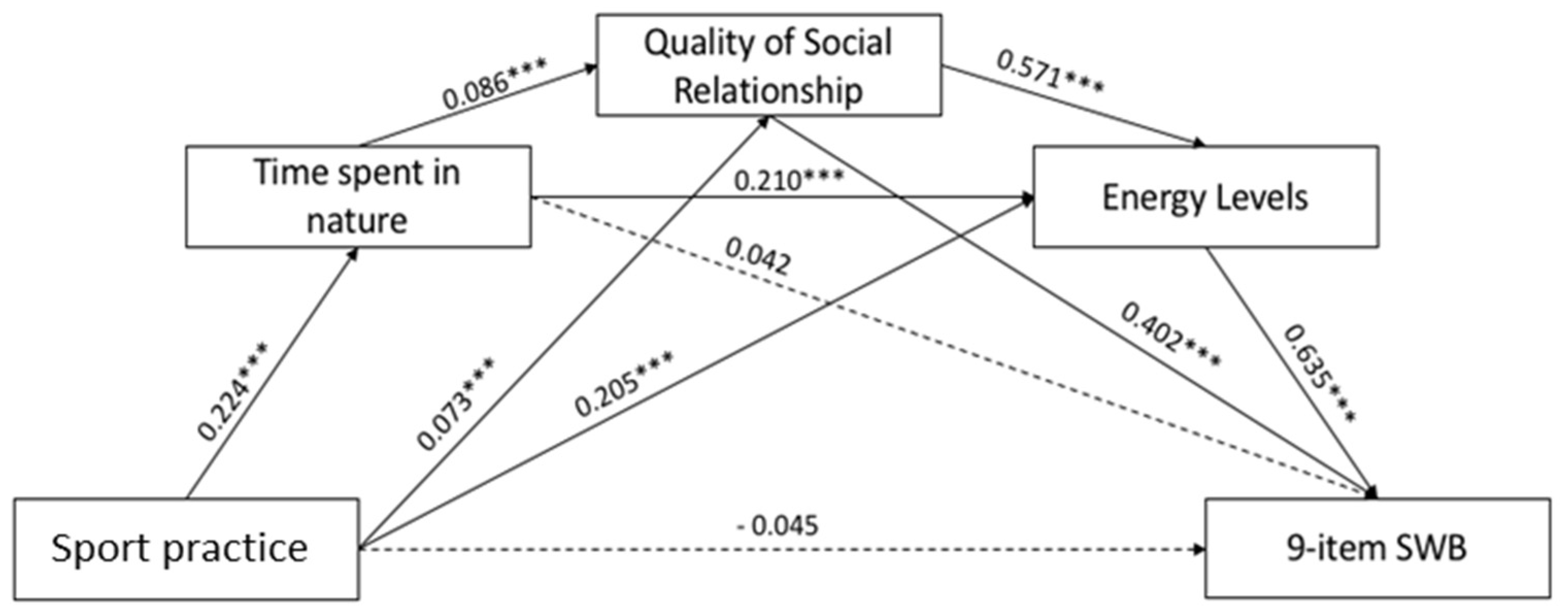
3.6. Mediation Models
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. The WHO Special Initiative for Mental Health (2019–2023): Universal Health Coverage for Mental Health; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Henry, J.D.; Crawford, J.R. The short-form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in a large non-clinical sample. Br. J. Clin. Psychol. 2005, 44, 227–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vignola, R.C.; Tucci, A.M. Adaptation and validation of the depression, anxiety and stress scale (DASS) to Brazilian Portuguese. J. Affect. Disord. 2014, 155, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Seligman, M.E.P.; Csikszentmihalyi, M. Positive psychology: An introduction. Am. Psychol. 2000, 55, 5–14. [Google Scholar] [CrossRef]
- OECD. OECD Guidelines on Measuring Subjective Well-Being; OECD: Paris, France, 2013. [Google Scholar]
- Andrade, V.; Quarta, S.; Tagarro, M.; Miloseva, L.; Massaro, M.; Chervenkov, M.; Ivanova, T.; Jorge, R.; Maksimova, V.; Smilkov, K.; et al. Exploring hedonic and eudaimonic items of well-being in Mediterranean and non-Mediterranean countries: Influence of sociodemographic and lifestyle factors. Int. J. Environ. Res. Public Health 2022, 19, 1715. [Google Scholar] [CrossRef] [PubMed]
- Abbott, R.A.; Ploubidis, G.B.; Huppert, F.A.; Kuh, D.; Wadsworth, M.E.; Croudace, T.J. Psychometric evaluation and predictive validity of Ryff’s psychological well-being items in a UK birth cohort sample of women. Health Qual. Life Outcomes 2006, 4, 76. [Google Scholar] [CrossRef] [Green Version]
- Beekman, A.T.; Penninx, B.W.; Deeg, D.J.; De Beurs, E.; Geerling, S.W.; Van Tilburg, W. The impact of depression on the well-being, disability and use of services in older adults: A longitudinal perspective. Acta Psychiatr. Scand. 2002, 105, 20–27. [Google Scholar] [CrossRef]
- Spijker, J.; Graaf, R.; Bijl, R.V.; Beekman, A.T.; Ormel, J.; Nolen, W.A. Functional disability and depression in the general population. Results from the Netherlands Mental Health Survey and Incidence Study (NEMESIS). Acta Psychiatr. Scand. 2004, 110, 208–214. [Google Scholar] [CrossRef]
- Bani, M.; Zorzi, F.; Corrias, D.; Strepparava, M. Reducing psychological distress and improving students well-being and academic self-efficacy: The effectiveness of a cognitive university counselling service for clinical and non-clinical situations. Br. J. Guid. Couns. 2020, 1–11. [Google Scholar] [CrossRef]
- Bernaras Iturrioz, E.; Insúa Cerretani, P.; Bully Garay, P. Prevalence and severity of psychological problems in university students. Br. J. Guid. Couns. 2018, 46, 418–428. [Google Scholar] [CrossRef]
- Eisenberg, D.; Hunt, J.; Speer, N.; Zivin, K. Mental health service utilization among college students in the United States. J. Nerv. Ment. Dis. 2011, 199, 301–308. [Google Scholar] [CrossRef] [PubMed]
- McLafferty, M.; Lapsley, C.R.; Ennis, E.; Armour, C.; Murphy, S.; Bunting, B.P.; Bjourson, A.J.; Murray, E.K.; O’Neill, S.M. Mental health, behavioural problems and treatment seeking among students commencing university in Northern Ireland. PLoS ONE 2017, 12, e0188785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharp, J.; Theiler, S. A Review of Psychological Distress Among University Students: Pervasiveness, Implications and Potential Points of Intervention. Int. J. Adv. Couns. 2018, 40, 193–212. [Google Scholar] [CrossRef]
- Davies, G.A.; Strader, C.; Chibbar, R.; Papatheodorou, S.; Dmytriw, A.A. The relationship between physical activity and lymphoma: A systematic review and meta analysis. BMC Cancer 2020, 20, 962. [Google Scholar] [CrossRef]
- Kolnes, K.J.; Petersen, M.H.; Lien-Iversen, T.; Højlund, K.; Jensen, J. Effect of Exercise Training on Fat Loss-Energetic Perspectives and the Role of Improved Adipose Tissue Function and Body Fat Distribution. Front. Physiol. 2021, 12, 737709. [Google Scholar] [CrossRef]
- Murtagh, E.M.; Nichols, L.; Mohammed, M.A.; Holder, R.; Nevill, A.M.; Murphy, M.H. The effect of walking on risk factors for cardiovascular disease: An updated systematic review and meta-analysis of randomised control trials. Prev. Med. 2015, 72, 34–43. [Google Scholar] [CrossRef] [Green Version]
- Soares, C.M.; Teixeira, A.M.; Sarmento, H.; Silva, F.M.; Rusenhack, M.C.; Furmann, M.; Nobre, P.R.; Fachada, M.A.; Urbano, A.M.; Ferreira, J.P. Effect of exercise-conditioned human serum on the viability of cancer cell cultures: A systematic review and meta-analysis. Exerc. Immunol. Rev. 2021, 27, 24–41. [Google Scholar]
- Xie, F.; You, Y.; Huang, J.; Guan, C.; Chen, Z.; Fang, M.; Yao, F.; Han, J. Association between physical activity and digestive-system cancer: An updated systematic review and meta-analysis. J. Sport Health Sci. 2021, 10, 4–13. [Google Scholar] [CrossRef]
- Zhao, X.; He, Q.; Zeng, Y.; Cheng, L. Effectiveness of combined exercise in people with type 2 diabetes and concurrent overweight/obesity: A systematic review and meta-analysis. BMJ Open 2021, 11, e046252. [Google Scholar] [CrossRef]
- Zubala, A.; MacGillivray, S.; Frost, H.; Kroll, T.; Skelton, D.A.; Gavine, A.; Gray, N.M.; Toma, M.; Morris, J. Promotion of physical activity interventions for community dwelling older adults: A systematic review of reviews. PLoS ONE 2017, 12, e0180902. [Google Scholar] [CrossRef]
- Penedo, F.J.; Dahn, J.R. Exercise and well-being: A review of mental and physical health benefits associated with physical activity. Curr. Opin. Psychiatry 2005, 18, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Windle, G.; Hughes, D.; Linck, P.; Russell, I.; Woods, B. Is exercise effective in promoting mental well-being in older age? A systematic review. Aging Ment. Health 2010, 14, 652–669. [Google Scholar] [CrossRef] [PubMed]
- Dale, L.P.; Vanderloo, L.; Moore, S.; Faulkner, G. Physical activity and depression, anxiety, and self-esteem in children and youth: An umbrella systematic review. Ment. Health Phys. Act. 2019, 16, 66–79. [Google Scholar] [CrossRef]
- Mandolesi, L.; Polverino, A.; Montuori, S.; Foti, F.; Ferraioli, G.; Sorrentino, P.; Sorrentino, G. Effects of Physical Exercise on Cognitive Functioning and Wellbeing: Biological and Psychological Benefits. Front. Psychol. 2018, 9, 509. [Google Scholar] [CrossRef]
- Bhui, K.; Fletcher, A. Common mood and anxiety states: Gender differences in the protective effect of physical activity. Soc. Psychiatry Psychiatr. Epidemiol. 2000, 35, 28–35. [Google Scholar] [CrossRef]
- Felez-Nobrega, M.; Bort-Roig, J.; Ma, R.; Romano, E.; Faires, M.; Stubbs, B.; Stamatakis, E.; Olaya, B.; Haro, J.M.; Smith, L.; et al. Light-intensity physical activity and mental ill health: A systematic review of observational studies in the general population. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 123. [Google Scholar] [CrossRef]
- Biddle, S.J.; Asare, M. Physical activity and mental health in children and adolescents: A review of reviews. Br. J. Sports Med. 2011, 45, 886–895. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Ayllon, M.; Cadenas-Sanchez, C.; Estevez-Lopez, F.; Munoz, N.E.; Mora-Gonzalez, J.; Migueles, J.H.; Molina-Garcia, P.; Henriksson, H.; Mena-Molina, A.; Martinez-Vizcaino, V.; et al. Role of Physical Activity and Sedentary Behavior in the Mental Health of Preschoolers, Children and Adolescents: A Systematic Review and Meta-Analysis. Sports Med. 2019, 49, 1383–1410. [Google Scholar] [CrossRef]
- Wei, Y.; McGrath, P.J.; Hayden, J.; Kutcher, S. Measurement properties of tools measuring mental health knowledge: A systematic review. BMC Psychiatry 2016, 16, 297. [Google Scholar] [CrossRef] [Green Version]
- Kleppang, A.L.; Hartz, I.; Thurston, M.; Hagquist, C. The association between physical activity and symptoms of depression in different contexts-a cross-sectional study of Norwegian adolescents. BMC Public Health 2018, 18, 1368. [Google Scholar] [CrossRef]
- Hartig, T.; Mitchell, R.; Vries, S.d.; Frumkin, H. Nature and Health. Annu. Rev. Public Health 2014, 35, 207–228. [Google Scholar] [CrossRef] [Green Version]
- WHO. Urban Green Spaces and Health; World Health Organization: Geneva, Switzerland; Regional Office for Europe: Copenhagen, Denmark, 2016. [Google Scholar]
- Belanger, M.; Gallant, F.; Dore, I.; O’Loughlin, J.L.; Sylvestre, M.P.; Abi Nader, P.; Larouche, R.; Gunnell, K.; Sabiston, C.M. Physical activity mediates the relationship between outdoor time and mental health. Prev. Med. Rep. 2019, 16, 101006. [Google Scholar] [CrossRef] [PubMed]
- Kerr, J.; Marshall, S.; Godbole, S.; Neukam, S.; Crist, K.; Wasilenko, K.; Golshan, S.; Buchner, D. The relationship between outdoor activity and health in older adults using GPS. Int. J. Environ. Res. Public Health 2012, 9, 4615–4625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coventry, P.A.; Brown, J.E.; Pervin, J.; Brabyn, S.; Pateman, R.; Breedvelt, J.; Gilbody, S.; Stancliffe, R.; McEachan, R.; White, P.L. Nature-based outdoor activities for mental and physical health: Systematic review and meta-analysis. SSM Popul. Health 2021, 16, 100934. [Google Scholar] [CrossRef] [PubMed]
- Thompson Coon, J.; Boddy, K.; Stein, K.; Whear, R.; Barton, J.; Depledge, M.H. Does participating in physical activity in outdoor natural environments have a greater effect on physical and mental wellbeing than physical activity indoors? A systematic review. Environ. Sci. Technol. 2011, 45, 1761–1772. [Google Scholar] [CrossRef]
- Olff, M.; Primasari, I.; Qing, Y.; Coimbra, B.M.; Hovnanyan, A.; Grace, E.; Williamson, R.E.; Hoeboer, C.M. Mental health responses to COVID-19 around the world. Eur. J. Psychotraumatol. 2021, 12, 1929754. [Google Scholar] [CrossRef]
- Petrocchi, S.; Levante, A.; Bianco, F.; Castelli, I.; Lecciso, F. Maternal Distress/Coping and Children’s Adaptive Behaviors During the COVID-19 Lockdown: Mediation Through Children’s Emotional Experience. Front. Public Health 2020, 8, 587833. [Google Scholar] [CrossRef]
- Tommasi, M.; Toro, F.; Arno, S.; Carrieri, A.; Conte, M.M.; Devastato, M.D.; Picconi, L.; Sergi, M.R.; Saggino, A. Physical and Psychological Impact of the Phase One Lockdown for COVID-19 on Italians. Front. Psychol. 2020, 11, 563722. [Google Scholar] [CrossRef]
- Galle, F.; Sabella, E.A.; Ferracuti, S.; De Giglio, O.; Caggiano, G.; Protano, C.; Valeriani, F.; Parisi, E.A.; Valerio, G.; Liguori, G.; et al. Sedentary Behaviors and Physical Activity of Italian Undergraduate Students during Lockdown at the Time of COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6171. [Google Scholar] [CrossRef]
- Maugeri, G.; Castrogiovanni, P.; Battaglia, G.; Pippi, R.; D’Agata, V.; Palma, A.; Di Rosa, M.; Musumeci, G. The impact of physical activity on psychological health during COVID-19 pandemic in Italy. Heliyon 2020, 6, e04315. [Google Scholar] [CrossRef]
- Orgilés, M.; Morales, A.; Delvecchio, E.; Mazzeschi, C.; Espada, J.P. Immediate Psychological Effects of the COVID-19 Quarantine in Youth From Italy and Spain. Front. Psychol. 2020, 11, 579038. [Google Scholar] [CrossRef] [PubMed]
- Villani, L.; Pastorino, R.; Molinari, E.; Anelli, F.; Ricciardi, W.; Graffigna, G.; Boccia, S. Impact of the COVID-19 pandemic on psychological well-being of students in an Italian university: A web-based cross-sectional survey. Glob. Health 2021, 17, 39. [Google Scholar] [CrossRef] [PubMed]
- Benjet, C.; Borges, G.; Méndez, E.; Albor, Y.; Casanova, L.; Orozco, R.; Curiel, T.; Fleiz, C.; Medina-Mora, M.E. Eight-year incidence of psychiatric disorders and service use from adolescence to early adulthood: Longitudinal follow-up of the Mexican Adolescent Mental Health Survey. Eur. Child. Adolesc. Psychiatry 2016, 25, 163–173. [Google Scholar] [CrossRef]
- Keyes, C.L.; Dhingra, S.S.; Simoes, E.J. Change in level of positive mental health as a predictor of future risk of mental illness. Am. J. Public Health 2010, 100, 2366–2371. [Google Scholar] [CrossRef]
- Bottesi, G.; Ghisi, M.; Altoe, G.; Conforti, E.; Melli, G.; Sica, C. The Italian version of the Depression Anxiety Stress Scales-21: Factor structure and psychometric properties on community and clinical samples. Compr. Psychiatry 2015, 60, 170–181. [Google Scholar] [CrossRef] [PubMed]
- Girolamo, G.D.; Rucci, P.; Scocco, P.; Becchi, A.; Coppa, F.; D’Addario, A.; Daru, E.; Leo, D.D.; Galassi, L.; Mangelli, L.; et al. Quality of life assessment: Validation of the Italian version of the WHOQOL-Brief. Epidemiol. E Psichiatr. Soc. 2000, 9, 45–55. [Google Scholar] [CrossRef]
- Orpana, H.; Vachon, J.; Pearson, C.; Elliott, K.; Smith, M.; Branchard, B. Correlates of well-being among Canadians with mood and/or anxiety disorders. Health Promot. Chronic Dis. Prev. Can. 2016, 36, 302–313. [Google Scholar] [CrossRef] [Green Version]
- Mondo, M.; Sechi, C.; Cabras, C. Psychometric evaluation of three versions of the Italian Perceived Stress Scale. Curr. Psychol. 2021, 40, 1884–1892. [Google Scholar] [CrossRef]
- Manzoni, G.M.; Rossi, A.; Marazzi, N.; Agosti, F.; De Col, A.; Pietrabissa, G.; Castelnuovo, G.; Molinari, E.; Sartorio, A. Feasibility, Validity, and Reliability of the Italian Pediatric Quality of Life Inventory Multidimensional Fatigue Scale for Adults in Inpatients with Severe Obesity. Obes. Facts 2018, 11, 25–36. [Google Scholar] [CrossRef]
- Fritz, C.O.; Morris, P.E.; Richler, J.J. Effect size estimates: Current use, calculations, and interpretation. J. Exp. Psychol. Gen. 2012, 141, 2–18. [Google Scholar] [CrossRef] [Green Version]
- Courrieu, P.; Brand-D’abrescia, M.; Peereman, R.; Spieler, D.; Rey, A. Validated intraclass correlation statistics to test item performance models. Behav. Res. Methods 2011, 43, 37–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Obesity: Preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ. Tech. Rep. Ser. 2000, 894, 1–253. [Google Scholar]
- WHO. The European Health Report 2015: Targets and Beyond–Reaching New Frontiers in Evidence; World Health Organization: Geneva, Switzerland; Regional Office for Europe: Copenhagen, Demark, 2015. [Google Scholar]
- Dodd, R.H.; Dadaczynski, K.; Okan, O.; McCaffery, K.J.; Pickles, K. Psychological Wellbeing and Academic Experience of University Students in Australia during COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 866. [Google Scholar] [CrossRef]
- Fornili, M.; Petri, D.; Berrocal, C.; Fiorentino, G.; Ricceri, F.; Macciotta, A.; Bruno, A.; Farinella, D.; Baccini, M.; Severi, G.; et al. Psychological distress in the academic population and its association with socio-demographic and lifestyle characteristics during COVID-19 pandemic lockdown: Results from a large multicenter Italian study. PLoS ONE 2021, 16, e0248370. [Google Scholar] [CrossRef] [PubMed]
- Eurostat. 7.2% of People in the EU Suffer from Chronic Depression. Available online: https://ec.europa.eu/eurostat/web/products-eurostat-news/-/edn-20210910-1 (accessed on 12 March 2022).
- Gigantesco, A.; Masocco, M.; Minardi, V.; Contoli, M.; Medda, E.; Fagnani, C. L’epidemiologia per la Sanità Pubblica. Aspetti Epidemiologici in Italia. Available online: https://www.epicentro.iss.it/mentale/epidemiologia-italia (accessed on 12 March 2022).
- Volpe, U.; Ventriglio, A.; Bellomo, A.; Kadhum, M.; Lewis, T.; Molodynski, A.; Sampogna, G.; Fiorillo, A. Mental health and wellbeing among Italian medical students: A descriptive study. Int. Rev. Psychiatry 2019, 31, 569–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ammar, A.; Mueller, P.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Brach, M.; Schmicker, M.; Bentlage, E.; et al. Psychological consequences of COVID-19 home confinement: The ECLB-COVID19 multicenter study. PLoS ONE 2020, 15, e0240204. [Google Scholar] [CrossRef] [PubMed]
- Sibley, C.G.; Greaves, L.M.; Satherley, N.; Wilson, M.S.; Overall, N.C.; Lee, C.H.J.; Milojev, P.; Bulbulia, J.; Osborne, D.; Milfont, T.L.; et al. Effects of the COVID-19 pandemic and nationwide lockdown on trust, attitudes toward government, and well-being. Am. Psychol. 2020, 75, 618–630. [Google Scholar] [CrossRef]
- Odriozola-Gonzalez, P.; Planchuelo-Gomez, A.; Irurtia, M.J.; De Luis-Garcia, R. Psychological effects of the COVID-19 outbreak and lockdown among students and workers of a Spanish university. Psychiatry Res. 2020, 290, 113108. [Google Scholar] [CrossRef]
- Wathelet, M.; Duhem, S.; Vaiva, G.; Baubet, T.; Habran, E.; Veerapa, E.; Debien, C.; Molenda, S.; Horn, M.; Grandgenevre, P.; et al. Factors Associated With Mental Health Disorders Among University Students in France Confined During the COVID-19 Pandemic. JAMA Netw. Open 2020, 3, e2025591. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Roberts, R.E. The power of positive emotions: It’s a matter of life or death—Subjective well-being and longevity over 28 years in a general population. Health Psychol. 2010, 29, 9–19. [Google Scholar] [CrossRef] [Green Version]
- Boehm, J.K.; Peterson, C.; Kivimaki, M.; Kubzansky, L. A prospective study of positive psychological well-being and coronary heart disease. Health Psychol. 2011, 30, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Bailey, T.H.; Phillips, L.J. The influence of motivation and adaptation on students’ subjective well-being, meaning in life and academic performance. High. Educ. Res. Dev. 2016, 35, 201–216. [Google Scholar] [CrossRef]
- Denovan, A.; Macaskill, A. Stress and Subjective Well-Being Among First Year UK Undergraduate Students. J. Happiness Stud. 2017, 18, 505–525. [Google Scholar] [CrossRef]
- Yu, L.; Shek, D.T.L.; Zhu, X. The Influence of Personal Well-Being on Learning Achievement in University Students Over Time: Mediating or Moderating Effects of Internal and External University Engagement. Front. Psychol. 2017, 8, 2287. [Google Scholar] [CrossRef] [Green Version]
- Delmastro, M.; Zamariola, G. Depressive symptoms in response to COVID-19 and lockdown: A cross-sectional study on the Italian population. Sci. Rep. 2020, 10, 22457. [Google Scholar] [CrossRef]
- Scully, D.; Kremer, J.; Meade, M.M.; Graham, R.; Dudgeon, K. Physical exercise and psychological well being: A critical review. Br. J. Sports Med. 1998, 32, 111–120. [Google Scholar] [CrossRef] [Green Version]
- Scully, D.; Kremer, J.; Meade, M.M.; Graham, R.; Dudgeon, K. Physical activity and psychological benefits: A position statement from the international society of sport psychology. J. Appl. Sports Psychol. 1992, 4, 94–98. [Google Scholar] [CrossRef]
- Richardson, C.; Faulkner, G.; McDevitt, J.; Skrinar, G.; Hutchinson, D.; Piette, D. Integrating Physical Activity Into Mental Health Services for Persons With Serious Mental Illness. Psychiatr. Serv. 2005, 56, 324–331. [Google Scholar] [CrossRef]
- WHO. Guidelines on Physical Activity and Sedentary Behaviour; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Fluetsch, N.; Levy, C.; Tallon, L. The relationship of physical activity to mental health: A 2015 behavioral risk factor surveillance system data analysis. J. Affect. Disord. 2019, 253, 96–101. [Google Scholar] [CrossRef]
- Silva, L.R.B.; Seguro, C.S.; De Oliveira, C.G.A.; Santos, P.O.S.; De Oliveira, J.C.M.; De Souza Filho, L.F.M.; De Paula Júnior, C.A.; Gentil, P.; Rebelo, A.C.S. Physical Inactivity Is Associated With Increased Levels of Anxiety, Depression, and Stress in Brazilians During the COVID-19 Pandemic: A Cross-Sectional Study. Front. Psychiatry 2020, 11, 565291. [Google Scholar] [CrossRef] [PubMed]
- Conn, V.S. Depressive symptom outcomes of physical activity interventions: Meta-analysis findings. Ann. Behav. Med. 2010, 39, 128–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuch, F.B.; Stubbs, B.; Meyer, J.; Heissel, A.; Zech, P.; Vancampfort, D.; Rosenbaum, S.; Deenik, J.; Firth, J.; Ward, P.B.; et al. Physical activity protects from incident anxiety: A meta-analysis of prospective cohort studies. Depress. Anxiety 2019, 36, 846–858. [Google Scholar] [CrossRef] [PubMed]
- Wessely, S.; Hotopf, M.; Sharpe, M. Chronic Fatigue and Its Syndromes; Oxford University Press: Oxford, UK, 1998. [Google Scholar]
- Bonner, A.; Wellard, S.; Caltabiano, M. Levels of fatigue in people with ESRD living in far North Queensland. J. Clin. Nurs. 2008, 17, 90–98. [Google Scholar] [CrossRef]
- Prescott, E.; Holst, C.; Gronbaek, M.; Schnohr, P.; Jensen, G.; Barefoot, J. Vital exhaustion as a risk factor for ischaemic heart disease and all-cause mortality in a community sample. A prospective study of 4084 men and 5479 women in the Copenhagen City Heart Study. Int. J. Epidemiol. 2003, 32, 990–997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demyttenaere, K.; De Fruyt, J.; Stahl, S.M. The many faces of fatigue in major depressive disorder. Int. J. Neuropsychopharmacol. 2005, 8, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Colucci, E.; Nadeau, S.; Higgins, J.; Kehayia, E.; Poldma, T.; Saj, A.; De Guise, E. COVID-19 lockdowns’ effects on the quality of life, perceived health and well-being of healthy elderly individuals: A longitudinal comparison of pre-lockdown and lockdown states of well-being. Arch. Gerontol. Geriatr. 2021, 99, 104606. [Google Scholar] [CrossRef]
- Ellingson, L.D.; Kuffel, A.E.; Vack, N.J.; Cook, D.B. Active and sedentary behaviors influence feelings of energy and fatigue in women. Med. Sci. Sports Exerc. 2014, 46, 192–200. [Google Scholar] [CrossRef]
- Morales-Vives, F.; Duenas, J.M.; Vigil-Colet, A.; Camarero-Figuerola, M. Psychological Variables Related to Adaptation to the COVID-19 Lockdown in Spain. Front. Psychol. 2020, 11, 565634. [Google Scholar] [CrossRef]
- Puetz, T.W. Physical activity and feelings of energy and fatigue: Epidemiological evidence. Sports Med. 2006, 36, 767–780. [Google Scholar] [CrossRef]
- Eigenschenk, B.; Thomann, A.; McClure, M.; Davies, L.; Gregory, M.; Dettweiler, U.; Ingles, E. Benefits of Outdoor Sports for Society. A Systematic Literature Review and Reflections on Evidence. Int. J. Environ. Res. Public Health 2019, 16, 937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMahon, E.M.; Corcoran, P.; O’Regan, G.; Keeley, H.; Cannon, M.; Carli, V.; Wasserman, C.; Hadlaczky, G.; Sarchiapone, M.; Apter, A.; et al. Physical activity in European adolescents and associations with anxiety, depression and well-being. Eur. Child Adolesc. Psychiatry 2017, 26, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Frumkin, H.; Bratman, G.N.; Breslow, S.J.; Cochran, B.; Kahn, P.H., Jr.; Lawler, J.J.; Levin, P.S.; Tandon, P.S.; Varanasi, U.; Wolf, K.L.; et al. Nature Contact and Human Health: A Research Agenda. Environ. Health Perspect. 2017, 125, 075001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, M.P.; Alcock, I.; Grellier, J.; Wheeler, B.W.; Hartig, T.; Warber, S.L.; Bone, A.; Depledge, M.H.; Fleming, L.E. Spending at least 120 minutes a week in nature is associated with good health and wellbeing. Sci. Rep. 2019, 9, 7730. [Google Scholar] [CrossRef] [Green Version]
- Robinson, J.M.; Brindley, P.; Cameron, R.; MacCarthy, D.; Jorgensen, A. Nature’s Role in Supporting Health during the COVID-19 Pandemic: A Geospatial and Socioecological Study. Int. J. Environ. Res. Public Health 2021, 18, 2227. [Google Scholar] [CrossRef]
- Klesges, R.C.; Eck, L.H.; Mellon, M.W.; Fulliton, W.; Somes, G.W.; Hanson, C.L. The accuracy of self-reports of physical activity. Med. Sci. Sports Exerc. 1990, 22, 690–697. [Google Scholar] [CrossRef]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.H.; Stewart, S.M. Validity of the International Physical Activity Questionnaire Short Form (IPAQ-SF): A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 115. [Google Scholar] [CrossRef] [Green Version]
- Hill, A.B. The enviroment and disease: Association or causation? Proc. R Soc. Med. 1965, 58, 295–300. [Google Scholar]
- Antunes, H.K.; Leite, G.S.; Lee, K.S.; Barreto, A.T.; Santos, R.V.; De Sá Souza, H.; Tufik, S.; De Mello, M.T. Exercise deprivation increases negative mood in exercise-addicted subjects and modifies their biochemical markers. Physiol. Behav. 2016, 156, 182–190. [Google Scholar] [CrossRef]
- Almeida, D.L.; Moreira, V.M.; Cardoso, L.E.; Junior, M.D.F.; Pavanelo, A.; Ribeiro, T.A.; Da Silva Franco, C.C.; Tófolo, L.P.; Peres, M.N.C.; Ribeiro, M.V.G.; et al. Lean in one way, in obesity another: Effects of moderate exercise in brown adipose tissue of early overfed male Wistar rats. Int. J. Obes. 2021, 46, 137–143. [Google Scholar] [CrossRef]
- Mikkelsen, K.; Stojanovska, L.; Polenakovic, M.; Bosevski, M.; Apostolopoulos, V. Exercise and mental health. Maturitas 2017, 106, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Wipfli, B.; Landers, D.; Nagoshi, C.; Ringenbach, S. An examination of serotonin and psychological variables in the relationship between exercise and mental health. Scand. J. Med. Sci. Sports 2011, 21, 474–481. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| What Measure | Original Items Number | ||
|---|---|---|---|
| DASS-21 | Distress | Depression | 3. I could not seem to experience any positive feeling at all; |
| 5. I found it difficult to work up the initiative to do things; | |||
| 10. I felt that I had nothing to look forward to; | |||
| 13. I felt down-hearted and blue; | |||
| 16. I was unable to become enthusiastic about anything | |||
| 17. I felt I was not worth much as a person; | |||
| 21. I felt that life was meaningless; | |||
| Anxiety | 2. I was aware of dryness of my mouth; | ||
| 4. I experienced breathing difficulty (e.g., excessively rapid breathing, breathlessness in the absence of physical exertion); | |||
| 7. I experienced trembling (e.g., in the hands) | |||
| 9. I was worried about situations in which I might panic and make a fool of myself; | |||
| 15. I felt I was close to panic; | |||
| 19. I was aware of the action of my heart in the absence of physical exertion (e.g., sense of heart rate increase, heart missing a beat); | |||
| 20. I felt scared without any good reason; | |||
| Stress | 1. I found it hard to wind down; | ||
| 6. I tended to over-react to situations; | |||
| 8. I felt that I was using a lot of nervous energy; | |||
| 11. I found myself getting agitated; | |||
| 12. I found it difficult to relax; | |||
| 14. I was intolerant of anything that kept me from getting on with what I was doing; | |||
| 18. I felt that I was rather touchy; | |||
| WHOQoL Brief | Psychological health (PH) | 5. How much do you enjoy your life?; | |
| 6. To what extent do you feel your life is meaningful?; | |||
| 7. How well can you concentrate?; | |||
| 11. Can you accept your physical appearance?; | |||
| 19. How satisfied are you with yourself?; | |||
| 26. How often do you have negative feelings such as bad mood, despair, anxiety, depression?; | |||
| Social relationships (SR) | 20. How satisfied are you with your personal relationships?; | ||
| 21. How satisfied are you with your sex life?; | |||
| 22. How satisfied are you with the support you get from your friends? | |||
| General health (GH) | How satisfied are you with your health? | ||
| Subjective well-being (SWB) | 9-item SWB | C1 (positive domain) | 1.How satisfied are you with your life as a whole these days? |
| 2. To what extent do you feel that the things you do in life are worthwhile?; | |||
| 3. How happy did you feel during the last week?; | |||
| 8.Last week, how energetic did you normally feel in the middle of the day? | |||
| 9. Last week, how efficient did you normally feel in the middle of the day? | |||
| C2 (negative domain) | 4. How worried did you feel during the last week? | ||
| 5. Did you feel depressed during the last week? | |||
| 6. During last week, how often did you feel nervous and stressed? | |||
| 7. During last week, how often did you feel that you were unable to cope with all the thing you had | |||
| Energy level | 8.Last week, how energetic did you normally feel in the middle of the day? | ||
| 9. Last week, how efficient did you normally feel in the middle of the day? | |||
| 10. Last week, how tired did you normally feel in the middle of the day? | |||
| Students | Staff | p-Value | |
|---|---|---|---|
| N (%) | 939 | 238 | <0.001 |
| Sex distribution, N (%): | |||
| Male | 235 (25.0) | 109 (45.8) | |
| Female | 704 (75.0) | 129 (54.2) | |
| Age distribution (years), N (%) | <0.001 | ||
| 18–24 y | 586 (62.4) | 0 (0) | |
| 25–34 y | 274 (29.2) | 8 (3.4) | |
| 35–44 y | 47 (5.0) | 38 (16.0) | |
| 45–54 y | 26 (2.8) | 96 (40.3) | |
| 55–64 y | 5 (0.5) | 86 (36.1) | |
| >65 y | 1 (0.1) | 10 (4.2) | |
| Marital status, N (%) | <0.001 | ||
| Single | 676 (71.9) | 58 (24.3) | |
| Married or analogous relationship | 263 (28.0) | 180 (75.6) | |
| Having children N (%) | <0.001 | ||
| No | 886 (94.4) | 75 (31.5) | |
| Yes | 53 (5.6) | 163 (68.5) | |
| Cohabitants | <0.001 | ||
| Median (IQR) | 4.00 (1.00) | 3.00 (2.00) | |
| Mean ± SD | 3.69 ± 0.99 | 2.92 ± 1.17 | |
| Family income N (%) | <0.001 | ||
| <500€ | 51 (5.4) | 0 (0) | |
| 500–1000€ | 143 (15.2) | 1 (0.4) | |
| 1000–1500€ | 272 (29.0) | 28 (11.8) | |
| 1500–2000€ | 215 (22.9) | 45 (18.9) | |
| 2000–2500€ | 143 (15.2) | 44 (18.5) | |
| >2500€ | 115 (12.2) | 120 (50.4) | |
| BMI (Kg/m2) | <0.001 | ||
| Median (IQR) | 22.48 (5.00) | 24.22 (4.00) | |
| Mean ± SD | 23.14 ± 4.21 | 24.88 ± 4.00 | |
| BMI distribution 1, N (%) | 0.002 | ||
| Underweight | 72 (7.7) | 1 (0.4) | |
| Normal weight | 633 (67.4) | 137 (57.6) | |
| Overweight | 183 (19.5) | 77 (32.4) | |
| Obese | 51 (5.4) | 23 (9.7) | |
| Diagnosed pathologies, N (%) | 0.002 | ||
| No | 816 (86.9) | 188 (79.0) | |
| Yes | 123 (13.1) | 50 (21.0) |
| Students | Staff | ||||
|---|---|---|---|---|---|
| Severity | (N) | % | N | % | p Value |
| DASS—Depression | |||||
| Normal (range: 0–9) | 405 | 43.2 | 184 | 77.3 | <0.001 |
| Mild (range: 10–12) | 126 | 13.4 | 23 | 9.7 | 0.127 |
| Moderate (range: 13–20) | 213 | 22.7 | 21 | 8.8 | <0.001 |
| Severe (range: 21–27) | 95 | 10.1 | 5 | 2.1 | <0.001 |
| Extremely severe (range: 28–42) | 100 | 10.6 | 5 | 2.1 | <0.001 |
| DASS—Anxiety | |||||
| Normal (range: 0–6) | 571 | 60.8 | 206 | 86.7 | <0.001 |
| Mild (range: 7–9) | 78 | 8.3 | 12 | 5 | 0.09 |
| Moderate (range: 10–14) | 152 | 16.2 | 13 | 5.5 | <0.001 |
| Severe (range: 15–19) | 58 | 6.2 | 3 | 1.3 | 0.001 |
| Extremely severe (range: 20–42) | 80 | 8.5 | 4 | 1.7 | <0.001 |
| DASS—Stress | |||||
| Normal (range: 0–10) | 469 | 49.9 | 187 | 78.6 | <0.001 |
| Mild (range: 11–18) | 64 | 6.8 | 14 | 5.9 | 0.605 |
| Moderate (range: 19–26) | 215 | 23 | 23 | 9.7 | <0.001 |
| Severe (range: 27–34) | 128 | 13.6 | 12 | 5 | <0.001 |
| Extremely severe (range: 35–42) | 63 | 6.7 | 2 | 0.8 | <0.001 |
| N 1 (Valid Population) | Comparison Tool | Correlation 2 (r, p Value) | ICC 3 (95% CI, p Value) |
|---|---|---|---|
| 9-item SWB index | |||
| Students (939) | WHOQoL psychological health domain | 0.762, <0.001 Strong positive correlation | 0.713 (0.673, 0.747; <0.001) Moderate |
| DASS-21 distress | −0.801, <0.001 Strong negative correlation | not calculable | |
| Staff (238) | WHOQoL psychological health domain | 0.734, <0.001 Strong positive correlation | 0.678 (0.585, 0.751; <0.001) Moderate |
| DASS-21 distress | −0.784, <0.001 Strong negative correlation | not calculable | |
| C1 (positive) | |||
| Students (939) | WHOQoL psychological health domain | 0.753, <0.001 Strong positive correlation | 0.715 (0.676, 0.750; <0.001) Moderate |
| Staff (238) | WHOQoL psychological health domain | 0.712, <0.001 Strong positive correlation | 0.695 (0.606, 0.764; <0.001) Moderate |
| C2 (negative) | |||
| Students (939) | DASS-21 distress | 0.740, <0.001 Strong positive correlation | 0.557 (0.496, 0.610; <0.001) Moderate |
| DASS-21 depression | 0.663, <0.001 Moderate positive correlation | 0.586 (0.529, 0.636; <0.001) Moderate | |
| DASS-21 stress | 0.745, <0.001 Strong positive correlation | 0.620 (0.568, 0.666; <0.001) Moderate | |
| DASS-21 anxiety | 0.543, <0.001 Moderate positive correlation | 0.420 (0.341, 0.490; <0.001) Poor | |
| Staff (238) | DASS-21 distress | 0.762, <0.001 Strong positive correlation | 0.442 (0.279, 0.568; <0.001) Poor |
| DASS-21 depression | 0.676, <0.001 Moderate positive correlation | 0.463 (0.307, 0.584; <0.001) Poor | |
| DASS-21 stress | 0.760, <0.001 Strong positive correlation | 0.551 (0.421, 0.652; <0.001) Moderate | |
| DASS-21 anxiety | 0.524, <0.001 Moderate positive correlation | 0.265 (0.052, 0.431; 0.009) Poor | |
| Students | Staff | p-Value | |
|---|---|---|---|
| Sport practising, N (%) | 0.003 | ||
| Never | 270 (28.8) | 97 (40.8) | |
| Occasionally | 297 (31.6) | 57 (23.9) | |
| Regularly (<150 min per week) | 158 (16.8) | 31 (13.0) | |
| Regularly (>150 min per week) | 214 (22.8) | 53 (22.3) | |
| Leisure activity, N (%) | 0.006 | ||
| Activities that do not require physical activity | 301 (32.1) | 62 (26.1) | |
| Relaxing activities sometimes per week | 311 (33.1) | 105 (44.1) | |
| Sport or intense physical activity | 327 (34.8) | 71 (29.8) | |
| Time spent in nature, N (%) | 0.06 | ||
| Never | 131 (14.0) | 34 (14.2) | |
| Occasionally | 276 (29.4) | 48 (20.2) | |
| Sometimes | 290 (30.9) | 84 (35.3) | |
| Frequently | 171 (18.2) | 54 (22.7) | |
| Almost all the time | 71 (7.6) | 18 (7.6) |
| Sport Practice | Physical Activity in Leisure Time | Time Spent in Nature | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Low | Moderate/High | p Value | Effect Size (r) | Low | Moderate/High | p Value | Effect Size (r) | Low | Moderate/High | p Value | Effect Size (r) | |
| Students | ||||||||||||
| DASS—Depression | ||||||||||||
| N (%) Mean ± SD | 567 (60.4) 1.00 ± 0.73 | 372 (39.6) 0.81 ± 0.69 | <0.001 | 0.14 Small | 612 (65.2) 0.98 ± 0.73 | 327 (34.8) 0.82 ± 0.70 | 0.001 | 0.12 Small | 407 (43.3) 1.04 ± 0.74 | 532 (56.7) 0.84 ± 0.71 | <0.001 | 0.14 Small |
| DASS—Anxiety | ||||||||||||
| N (%) Mean ± SD | 567 (60.4) 0.60 ± 0.57 | 372 (39.6) 0.42 ± 0.47 | <0.001 | 0.16 Small | 612 (65.2) 0.59 ± 0.57 | 327 (34.8) 0.41 ± 0.46 | <0.001 | 0.16 Small | 407 (43.3) 0.63 ± 0.58 | 532 (56.7) 0.45 ± 0.49 | <0.001 | 0.17 Small |
| DASS—Stress | ||||||||||||
| N (%) Mean ± SD | 567 (60.4) 1.24 ± 0.70 | 372 (39.6) 1.07 ± 0.67 | <0.001 | 0.12 Small | 612 (65.2) 1.23 ± 0.70 | 327 (34.8) 1.08 ± 0.68 | 0.003 | 0.10 Small | 407 (43.3) 1.32 ± 0.68 | 532 (56.7) 1.07 ± 0.68 | <0.001 | 0.18 Small |
| 9-item SWB index | ||||||||||||
| N (%) Mean ± SD | 567 (60.4) 5.45 ± 1.53 | 372 (39.6) 6.01 ± 1.52 | <0.001 | 0.19 Small | 612 (65.2) 5.53 ± 1.54 | 327 (34.8) 5.93 ± 1.52 | <0.001 | 0.14 Small | 407 (43.3) 5.34 ± 1.52 | 532 (56.7) 5.93 ± 1.52 | <0.001 | 0.19 Small |
| Staff | ||||||||||||
| DASS—Depression | ||||||||||||
| N (%) Mean ± SD | 154 (64.7) 0.45 ± 0.48 | 84 (35.3) 0.37 ± 0.49 | 0.282 | 0.07 NS | 167 (70.2) 0.46 ± 0.52 | 71 (29.8) 0.32 ± 0.36 | 0.014 | 0.12 Small | 82 (34.5) 0.49 ± 0.53 | 156 (65.5) 0.38 ± 0.45 | 0.119 | 0.11 NS |
| DASS—Anxiety | ||||||||||||
| N (%) Mean ± SD | 154 (64.7) 0.24 ± 0.29 | 84 (35.3) 0.23 ± 0.33 | 0.797 | 0.04 NS | 167 (70.2) 0.26 ± 0.32 | 71 (29.8) 0.19 ± 0.27 | 0.089 | 0.10 NS | 82 (34.5) 0.28 ± 0.36 | 156 (65.5) 0.22 ± 0.27 | 0.161 | 0.007 NS |
| DASS—Stress | ||||||||||||
| N (%) Mean ± SD | 154 (64.7) 0.75 ± 0.55 | 84 (35.3) 0.69 ± 0.54 | 0.449 | 0.05 NS | 167 (70.2) 0.74 ± 0.56 | 71 (29.8) 0.71 ± 0.53 | 0.685 | 0.002 NS | 82 (34.5) 0.82 ± 0.57 | 156 (65.5) 0.68 ± 0.54 | 0.068 | 0.12 NS |
| 9-item SWB index | ||||||||||||
| N (%) Mean ± SD | 154 (64.7) 6.60 ± 1.35 | 84 (35.3) 7.03 ± 1.49 | 0.031 | 0.14 Small | 167 (70.2) 6.62 ± 1.43 | 71 (29.8) 7.06 ± 1.33 | 0.023 | 0.13 Small | 82 (34.5) 6.51 ± 1.33 | 156 (65.5) 6.88 ± 1.44 | 0.055 | 0.10 NS |
| Parameters | Sport Practice (Spearman ρ/p Values) (1) | PA in Leisure Time * (Spearman ρ/p Values) (1) | Time Spent in Nature (Spearman ρ/p Values) (1) | |||
|---|---|---|---|---|---|---|
| Students | Staff | Students | Staff | Students | Staff | |
| SWB | ||||||
| 9-item SWB | 0.102/0.002 | 0.135/0.041 | 0.083/0.012 | 0.147/0.026 | 0.163/<0.001 | 0.097/0.143 |
| C1 (positive) | 0.133/<0.001 | 0.116/0.080 | 0.115/<0.001 | 0.086/0.191 | 0.163/<0.001 | 0.98/0.138 |
| C2 (negative) | −0.045/0.172 | −0.102/0.125 | −0.025/0.443 | −0.130/0.049 | −0.121/<0.001 | −0.075/0.257 |
| Energy level | 0.187/<0.001 | 0.184/0.005 | 0.194/<0.001 | 0.170/0.010 | 0.187/<0.001 | 0.198/0.003 |
| WHOQoL-Brief | ||||||
| Psychological health | 0.072/0.028 | 0.243/<0.001 | 0.049/0.131 | 0.208/0.001 | 0.106/0.001 | 0.142/0.032 |
| General health | 0.374/<0.001 | 0.396/<0.001 | 0.351/<0.001 | 0.360/<0.000 | 0.160/<0.001 | 0.209/0.001 |
| DASS-21 | ||||||
| Stress | −0.039/0.235 | −0.082/0.218 | −0.051/0.118 | −0.036/0.592 | −0.116/<0.001 | −0.096/0.148 |
| Anxiety | −0.111/<0.001 | −0.075/0.257 | −0.119/<0.001 | −0.061/0.356 | −0.134/<0.001 | −0.036/0.586 |
| Depression | −0.067/0.042 | −0.080/0.228 | −0.070/0.036 | −0.069/0.297 | 0.097/0.003 | −0.124/0.060 |
| Distress | −0.081/0.014 | −0.097/0.143 | −0.087/0.008 | −0.061/0.355 | −0.134/<0.001 | −0.107/0.107 |
| Path | β | SE | p | 95%CI | ||
|---|---|---|---|---|---|---|
| Boot_LLCI | Boot_ULCI | |||||
| Sport practice→ | 9-item SWB | 0.045 | 0.26 | 0.083 | −0.094 | 0.007 |
| Time spent in nature | 0.224 | 0.029 | <0.000 | 0.168 | 0.281 | |
| Quality of social relationship | 0.073 | 0.021 | <0.001 | 0.031 | 0.115 | |
| Energy levels | 0.205 | 0.039 | <0.000 | 0.128 | 0.282 | |
| Time spent in nature→ | 9-item SWB | 0.042 | 0.026 | 0.101 | −0.007 | 0.089 |
| Quality of social relationship | 0.086 | 0.021 | <0.001 | 0.044 | 0.128 | |
| Energy levels | 0.210 | 0.038 | <0.001 | 0.133 | 0.286 | |
| Quality of social relationship→ | 9-item SWB | 0.402 | 0.037 | <0.001 | 0.324 | 0.481 |
| Energy levels | 0.571 | 0.054 | <0.001 | 0.455 | 0.689 | |
| Energy levels→ | 9-item SWB | 0.635 | 0.019 | <0.001 | 0.595 | 0.673 |
| Indirect paths | ||||||
| Sport practice→Time spent in nature→9-item SWB | 0.007 | 0.004 | / | −0.001 | 0.015 | |
| Sport practice→Quality of social relationship→9-item SWB | 0.021 | 0.006 | / | 0.009 | 0.034 | |
| Sport practice→Energy levels→9-item SWB | 0.093 | 0.018 | / | 0.058 | 0.129 | |
| Sport practice→Time spent in nature→quality of social relationship→9-item SWB | 0.006 | 0.002 | / | 0.003 | 0.009 | |
| Sport practice→Time spent in nature→Energy levels→9-item SWB | 0.021 | 0.005 | / | 0.013 | 0.032 | |
| Sport practice→Quality of social relationship→Energy levels→9-item SWB | 0.019 | 0.006 | / | 0.008 | 0.031 | |
| Sport practice→Time spent in nature→Quality of social relationship→Energy levels→9-item SWB | 0.005 | 0.001 | / | 0.002 | 0.008 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quarta, S.; Levante, A.; García-Conesa, M.-T.; Lecciso, F.; Scoditti, E.; Carluccio, M.A.; Calabriso, N.; Damiano, F.; Santarpino, G.; Verri, T.; et al. Assessment of Subjective Well-Being in a Cohort of University Students and Staff Members: Association with Physical Activity and Outdoor Leisure Time during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 4787. https://doi.org/10.3390/ijerph19084787
Quarta S, Levante A, García-Conesa M-T, Lecciso F, Scoditti E, Carluccio MA, Calabriso N, Damiano F, Santarpino G, Verri T, et al. Assessment of Subjective Well-Being in a Cohort of University Students and Staff Members: Association with Physical Activity and Outdoor Leisure Time during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(8):4787. https://doi.org/10.3390/ijerph19084787
Chicago/Turabian StyleQuarta, Stefano, Annalisa Levante, María-Teresa García-Conesa, Flavia Lecciso, Egeria Scoditti, Maria Annunziata Carluccio, Nadia Calabriso, Fabrizio Damiano, Giuseppe Santarpino, Tiziano Verri, and et al. 2022. "Assessment of Subjective Well-Being in a Cohort of University Students and Staff Members: Association with Physical Activity and Outdoor Leisure Time during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 8: 4787. https://doi.org/10.3390/ijerph19084787
APA StyleQuarta, S., Levante, A., García-Conesa, M.-T., Lecciso, F., Scoditti, E., Carluccio, M. A., Calabriso, N., Damiano, F., Santarpino, G., Verri, T., Pinto, P., Siculella, L., & Massaro, M. (2022). Assessment of Subjective Well-Being in a Cohort of University Students and Staff Members: Association with Physical Activity and Outdoor Leisure Time during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 19(8), 4787. https://doi.org/10.3390/ijerph19084787