
Analysis of Posture Parameters in Patients with Idiopathic Scoliosis with the Use of 3D Ultrasound Diagnostics—Preliminary Results




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
- -
- Current X-ray scan of the pelvic girdle, diagnosed double-curve idiopathic scoliosis of Types I and II according to the King–Moe classification, with the Cobb angle between 25 and 50 degrees of primary scoliosis;
- -
- Girls aged 10–16 years;
- -
- Unfinished ossification with Risser sign < 5;
- -
- No contraindications to the therapy from other systems;
- -
- Consent to examination procedures.
- -
- Scoliosis of other than idiopathic origin;
- -
- Coexisting diseases of other organs that prevent participation in the rehabilitation program;
- -
- Lack of consent of the patient and the guardian to examinations and participation in the program.
2.2. Study Protocol
2.3. Data Analysis
3. Results
3.1. Participant Characteristics
3.2. The Shapiro–Wilk Test
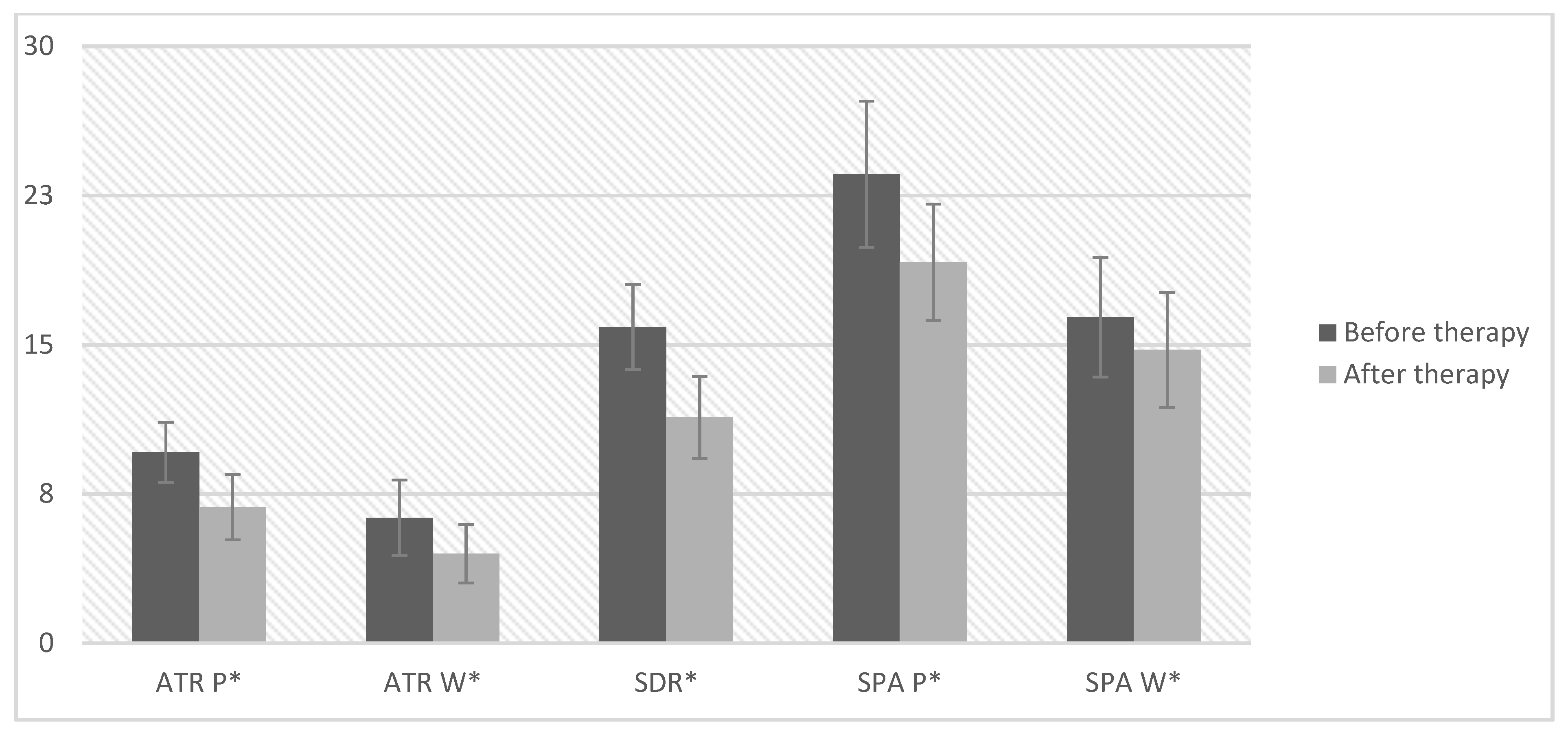
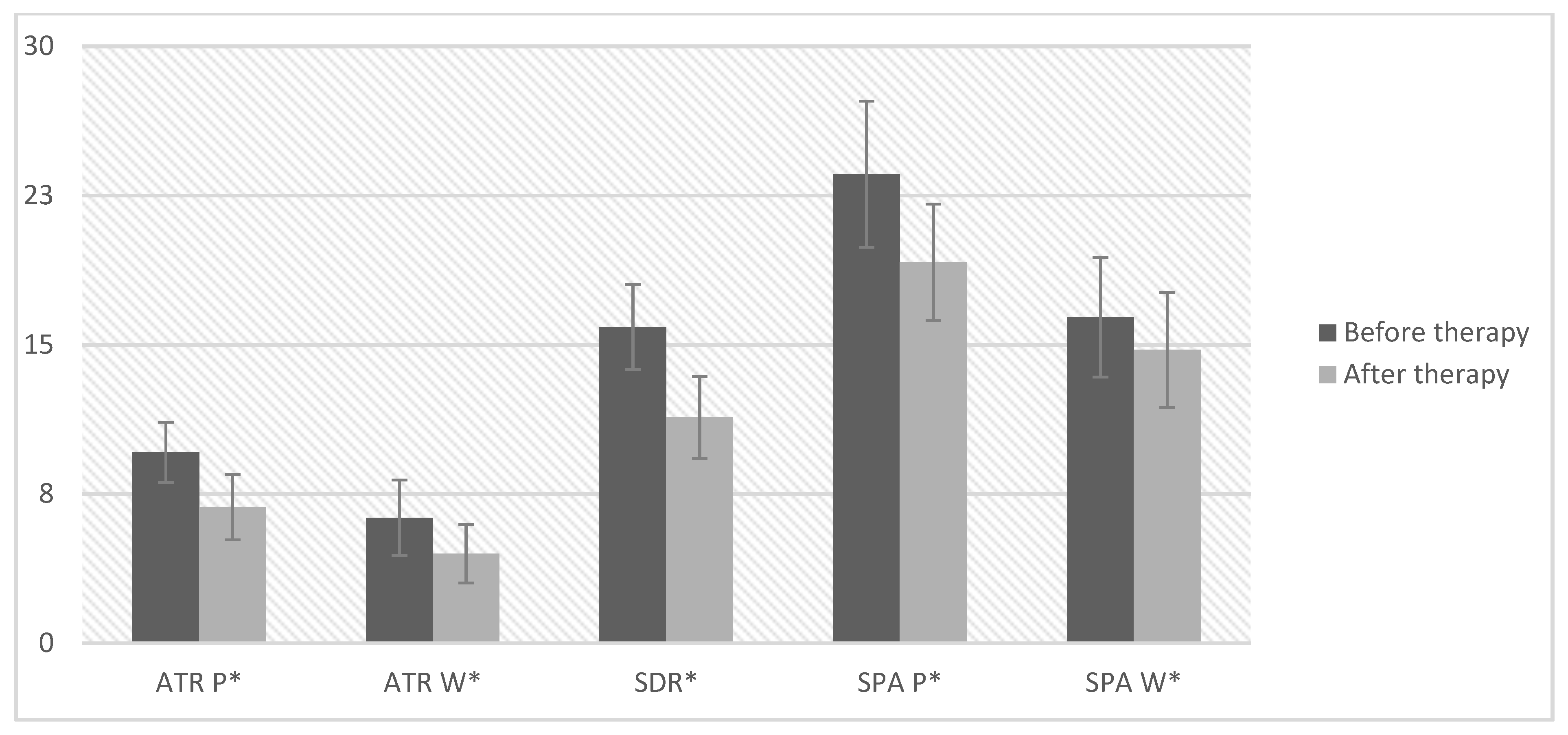
3.3. Comparison of the Values of Rotation and Curvature Angles
3.4. Correlations between Parameters Measured with X-ray, Scoliometer, and Scolioscan
4. Discussion
5. Conclusions
- The application of therapy that takes into account summing parameters may prevent the deterioration of the secondary curve when treating patients with idiopathic scoliosis.
- The observed correlations between the parameters of the radiological examination, the scoliometer and the scolioscan, prove the possibility of their interchangeable application in the assessment of effects of the therapy.
- Three-dimensional ultrasound diagnostics may become an alternative to radiological examination in assessing the treatment effects of patients with idiopathic scoliosis.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Trobisch, P.; Suess, O.; Schwab, F. Idiopathic Scoliosis. Dtsch. Arztebl. Int. 2010, 107, 875–884. [Google Scholar] [CrossRef]
- Yaman, O.; Dalbayrak, S. Idiopathic scoliosis. Turk. Neurosurg. 2014, 24, 646–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burton, M.S. Diagnosis and Treatment of Adolescent Idiopathic Scoliosis. Pediatr. Ann. 2013, 42, e233–e237. [Google Scholar] [CrossRef] [PubMed]
- Liang, J.; Zhou, X.; Chen, N.; Li, X.; Yu, H.; Yang, Y.; Song, Y.; Du, Q. Efficacy of three-dimensionally integrated exercise for scoliosis in patients with adolescent idiopathic scoliosis: Study protocol for a randomized controlled trial. Trials 2018, 19, 485. [Google Scholar] [CrossRef] [PubMed]
- Reamy, B.V.; Slakey, J.B. Adolescent idiopathic scoliosis: Review and current concepts. Am. Fam. Physician 2001, 64, 111. [Google Scholar]
- Kuznia, A.L.; Hernandez, A.K.; Lee, L.U. Adolescent Idiopathic Scoliosis: Common Questions and Answers. Am. Fam. Physician 2020, 101, 19–23. [Google Scholar]
- Kokabu, T.; Kawakami, N.; Uno, K.; Kotani, T.; Suzuki, T.; Abe, Y.; Maeda, K.; Inage, F.; Ito, Y.M.; Iwasaki, N.; et al. Three-dimensional depth sensor imaging to identify adolescent idiopathic scoliosis: A prospective multicenter cohort study. Sci. Rep. 2019, 9, 9678. [Google Scholar] [CrossRef]
- Weinstein, S.L.; Dolan, L.; Cheng, J.; Danielsson, A.; Morcuende, J.A. Adolescent idiopathic scoliosis. Lancet 2008, 371, 1527–1537. [Google Scholar] [CrossRef] [Green Version]
- Oakley, P.A.; Ehsani, N.N.; Harrison, D.E. The Scoliosis Quandary: Are Radiation Exposures from Repeated X-Rays Harmful? Dose-Response 2019, 17, 1559325819852810. [Google Scholar] [CrossRef]
- Kotwicki, T.; Kinel, E.; Chowańska, J.; Bodnar-Nanuś, A. POTSI, Hump Sum and Sum of Rotation—New surface topography parameters for evaluation of scoliotic deformity of the trunk. Fizjoter. Pol. 2008, 8, 231–240. [Google Scholar]
- Zheng, Y.-P.; Lee, T.T.-Y.; Lai, K.K.-L.; Yip, B.H.K.; Zhou, G.; Jiang, W.-W.; Cheung, C.W.J.; Wong, M.; Ng, B.K.-W.; Cheng, J.; et al. A reliability and validity study for Scolioscan: A radiation-free scoliosis assessment system using 3D ultrasound imaging. Scoliosis Spinal Disord. 2016, 11, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caciulan, E.; Stanca, D.; Marin, D. Study on the fed method application in thoracolum-bar scoliosis eficienţa metodei fed în recuperare a scoliozei toraco-lombare. Rev. Romana Kinetoterapie 2011, 17, 10–18. [Google Scholar]
- Trzcińska, S.; Kiebzak, W.; Wiecheć, M.; Śliwiński, Z. Compensation Mechanism in Treatment of Idiopathic Scoliosis with the FED Method Preliminary Results. Fizjoter. Pol. 2017, 17, 6–14. [Google Scholar]
- Trzcińska, S.; Koszela, K.; Kuszewski, M. Effectiveness of the FED Method in the Treatment of Idiopathic Scoliosis of Girls Aged 11–15 Years. Int. J. Environ. Res. Public Health 2021, 19, 65. [Google Scholar] [CrossRef]
- Czaprowski, D.; Kotwicki, T.; Durmała, J.; Stoliński, Ł. Fizjoterapia w leczeniu skoliozy idiopatycznej—Aktualne rekomendacje oparte o zalecenia SOSORT 2011 (Society Scoliosis Orthopedic and Rehabilitation Treatment). Post Rehab 2014, 1, 23–29. [Google Scholar]
- Białek, M.; Kotwicki, T.; M’hango, A.; Szulc, A. Angle of trunk rotation in primary and compensatory scoliotic curve in children after individual rehabilitation with FITS method. Ann. Acad. Med. Siles. 2007, 61, 45–48. [Google Scholar]
- Kotwicki, T.; Kinel, E.; Stryla, W.; Szulc, A. Discrepancy in clinical versus radiological parameters describing deformity due to brace treatment for moderate idiopathic scoliosis. Scoliosis 2007, 2, 18. [Google Scholar] [CrossRef] [Green Version]
- Oakley, P.A.; Ehsani, N.N.; Harrison, D.E. 5 Reasons Why Scoliosis X-Rays Are Not Harmful. Dose-Response 2020, 18, 155932582095779. [Google Scholar] [CrossRef]
- Brink, R.C.; Wijdicks, S.P.J.; Tromp, I.N.; Schlösser, T.P.C.; Kruyt, M.C.; Beek, F.J.A.; Castelein, R.M. A reliability and validity study for different coronal angles using ultrasound imaging in adolescent idiopathic scoliosis. Spine J. 2018, 18, 979–985. [Google Scholar] [CrossRef]
- Cheung, C.W.J.; Zhou, G.; Law, S.-Y.; Lai, K.-L.; Jiang, W.-W.; Zheng, Y.-P. Freehand three-dimensional ultrasound system for assessment of scoliosis. J. Orthop. Transl. 2015, 3, 123–133. [Google Scholar] [CrossRef] [Green Version]
- Cheung, C.W.; Law, S.Y.; Zheng, Y.P. Development of 3-D ultrasound system for assessment of adolescent idiopathic scoliosis(AIS): And system validation. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 6474–6477. [Google Scholar]
- Jiang, W.W.; Cheng, C.L.K.; Cheung, J.P.Y.; Samartzis, D.; Lai, K.K.L.; To, M.K.T.; Zheng, Y.-P. Patterns of coronal curve changes in forward bending posture: A 3D ultrasound study of adolescent idiopathic scoliosis patients. Eur. Spine J. 2018, 27, 2139–2147. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.T.-Y.; Jiang, W.W.; Cheng, C.L.K.; Lai, K.K.-L.; To, M.K.T.; Castelein, R.M.; Cheung, J.P.Y.; Zheng, Y.-P. A Novel Method to Measure the Sagittal Curvature in Spinal Deformities: The Reliability and Feasibility of 3-D Ultrasound Imaging. Ultrasound Med. Biol. 2019, 45, 2725–2735. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| ± SD | Min | Max | |
|---|---|---|---|
| Age (years) | 14.05 ± 1.64 | 10.00 | 16.00 |
| Weight (kg) | 52.50 ± 9.45 | 36.00 | 73.00 |
| Hight (cm) | 163.40 ± 7.16 | 143.00 | 174.00 |
| BMI | 19.58 ± 2.69 | 15.79 | 25.86 |
| Cobb angle of the primary curve (°) Cobb P | 32.45 ± 6.53 | 25.00 | 50.00 |
| Cobb angle of the secondary curve (°) Cobb W | 21.85 ± 7.91 | 11.00 | 41.00 |
| Risser test (points) | 2.50 ± 1.67 | 0.00 | 4.00 |
| King–Moe Classification | n | % of Total |
|---|---|---|
| Type I | 3 | 15.0 |
| Type II | 17 | 85.0 |
| Total | 20 | 100.0 |
| ± SD | Me | Kurt | Min | Max | W | p | |
|---|---|---|---|---|---|---|---|
| Before therapy (n = 20) | |||||||
| Cobb angle of the primary curve (°) Cobb P | 32.45 ± 6.53 | 31.50 | 2.01 | 25.00 | 50.00 | 0.87 | 0.011 * |
| Cobb angle of the secondary curve (°) Cobb W | 21.85 ± 7.91 | 22.50 | 0.45 | 11.00 | 41.00 | 0.95 | 0.343 |
| The trunk rotation angle primary curve (°) ATR P | 9.6 ± 3.45 | 9.00 | 1.61 | 5.00 | 19.00 | 0.92 | 0.121 |
| The trunk rotation angle secondary curve (°) ATR W | 6.3 ± 4.34 | 6.00 | −0.19 | 0.00 | 16.00 | 0.95 | 0.378 |
| Sum of two rotations (°) SDR | 15.9 ± 4.88 | 15.00 | −0.60 | 9.00 | 26.00 | 0.95 | 0.316 |
| Angle of scoliotic curvature of the primary curve (°) SPA P | 23.58 ± 8.37 | 20.45 | −1.14 | 12.00 | 38.60 | 0.93 | 0.158 |
| Angle of scoliotic curvature of the secondary curve (°) SPA W | 16.39 ± 6.86 | 17.85 | 1.97 | 0.00 | 33.50 | 0.93 | 0.177 |
| After therapy (n = 20) | |||||||
| The trunk rotation angle primary curve (°) ATR P | 6.85 ± 3.76 | 6.00 | 2.96 | 2.00 | 18.00 | 0.86 | 0.009 * |
| The trunk rotation angle secondary curve (°) ATR W | 4.5 ± 3.35 | 4.00 | −0.73 | 0.00 | 11.00 | 0.94 | 0.212 |
| Sum of two rotations(°) SDR | 11.35 ± 4.69 | 11.50 | 0.04 | 5.00 | 22.00 | 0.92 | 0.113 |
| Angle of scoliotic curvature of the primary curve (°) SPA P | 19.15 ± 6.67 | 19.10 | −1.14 | 9.20 | 30.40 | 0.95 | 0.371 |
| Angle of scoliotic curvature of the secondary curve (°) SPA W | 14.74 ± 6.62 | 15.80 | −0.28 | 0.00 | 25.00 | 0.97 | 0.766 |
| Before Therapy (n = 20) | After Therapy (n = 20) | Average Difference | t | p | 95% CI | d Cohena | ||
|---|---|---|---|---|---|---|---|---|
| ± SD | ± SD | LL | UL | |||||
| The trunk rotation angle primary curve(°) ATR P | 9.6 ± 3.45 | 6.85 ± 3.76 | 2.75 | 8.10 | <0.001 * | 2.04 | 3.46 | 1.81 |
| The trunk rotation angle secondary curve(°) ATR W | 6.3 ± 4.34 | 4.5 ± 3.35 | 1.80 | 3.45 | 0.002 * | 0.71 | 2.89 | 0.77 |
| Sum of two rotations (°) SDR | 15.9 ± 4.88 | 11.35 ± 4.69 | 4.55 | 7.42 | <0.001 * | 3.27 | 5.83 | 1.66 |
| Angle of scoliotic curvature of the primary curve(°) SPA P | 23.58 ± 8.37 | 19.15 ± 6.67 | 4.43 | 3.64 | 0.001 * | 1.88 | 6.98 | 0.81 |
| Angle of scoliotic curvature of the secondary curve(°) SPA W | 16.39 ± 6.86 | 14.74 ± 6.62 | 1.65 | 2.00 | 0.059 * | −0.07 | 3.37 | 0.45 |
| Compared Methods | Compared Variables | Before Therapy | After Therapy | ||
|---|---|---|---|---|---|
| X-ray—Skoliometr | Cobb angle of the primary curve (°) Cobb P | The trunk rotation angle primary curve (°) ATR P | r Pearson | 0.54 | - |
| p | 0.014 * | - | |||
| Cobb angle of the secondary curve (°) Cobb W | The trunk rotation angle secondary curve (°) ATR W | r Pearson | 0.48 | - | |
| p | 0.031 * | - | |||
| X-ray—Skolioscan | Cobb angle of the primary curve (°) Cobb P | Angle of scoliotic curvature of the primary curve (°) SPA P | r Pearson | 0.7 | - |
| p | 0.001 * | - | |||
| Cobb angle of the secondary curve (°) Cobb W | Angle of scoliotic curvature of the secondary curve (°) SPA W | r Pearson | 0.62 | - | |
| p | 0.003 * | - | |||
| Skoliometr—Scolioscan | The trunk rotation angle primary curve (°) ATR P | Angle of scoliotic curvature of the primary curve (°) SPA P | r Pearson | 0.44 | 0.35 |
| p | 0.054 * | 0.132 | |||
| The trunk rotation angle secondary curve (°) ATR W | Angle of scoliotic curvature of the secondary curve (°) SPA W | r Pearson | 0.47 | 0.44 | |
| p | 0.036 * | 0.050 * | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trzcińska, S.; Kuszewski, M.; Koszela, K. Analysis of Posture Parameters in Patients with Idiopathic Scoliosis with the Use of 3D Ultrasound Diagnostics—Preliminary Results. Int. J. Environ. Res. Public Health 2022, 19, 4750. https://doi.org/10.3390/ijerph19084750
Trzcińska S, Kuszewski M, Koszela K. Analysis of Posture Parameters in Patients with Idiopathic Scoliosis with the Use of 3D Ultrasound Diagnostics—Preliminary Results. International Journal of Environmental Research and Public Health. 2022; 19(8):4750. https://doi.org/10.3390/ijerph19084750
Chicago/Turabian StyleTrzcińska, Sandra, Michał Kuszewski, and Kamil Koszela. 2022. "Analysis of Posture Parameters in Patients with Idiopathic Scoliosis with the Use of 3D Ultrasound Diagnostics—Preliminary Results" International Journal of Environmental Research and Public Health 19, no. 8: 4750. https://doi.org/10.3390/ijerph19084750
APA StyleTrzcińska, S., Kuszewski, M., & Koszela, K. (2022). Analysis of Posture Parameters in Patients with Idiopathic Scoliosis with the Use of 3D Ultrasound Diagnostics—Preliminary Results. International Journal of Environmental Research and Public Health, 19(8), 4750. https://doi.org/10.3390/ijerph19084750