
Physical Examination Tool for Swollen and Tender Lower Limb Joints in Juvenile Idiopathic Arthritis: A Pilot Diagnostic Accuracy Study

 , , and
, , and
Abstract
1. Introduction
1.1. Objective
1.2. Hypotheses
- -
- A lower limb PE tool will display moderate correlation (validity) with MRI in the detection of active joint disease;
- -
- Podiatrist and PR clinical examination of lower limb joints will display moderate to high percentage agreements (inter-rater reliability);
- -
- Independent radiologist examinations of lower limb MRI scans will display moderate to high percentage agreements (inter-rater reliability);
- -
- Podiatrist intra-observer PE of lower limb joints will display high percentage agreements (intra-rater reliability).
2. Methods
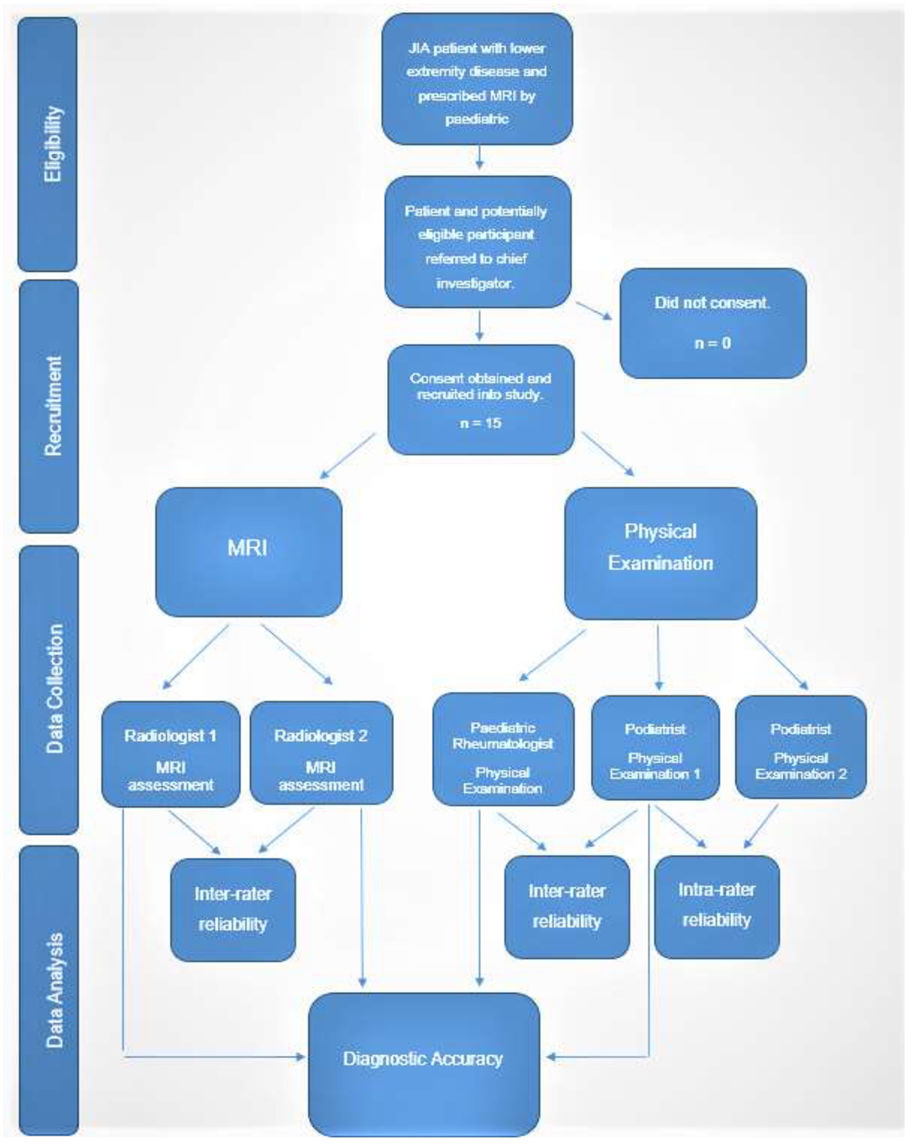
2.1. Study Design
2.2. Participants
2.3. Diagnostic Tools
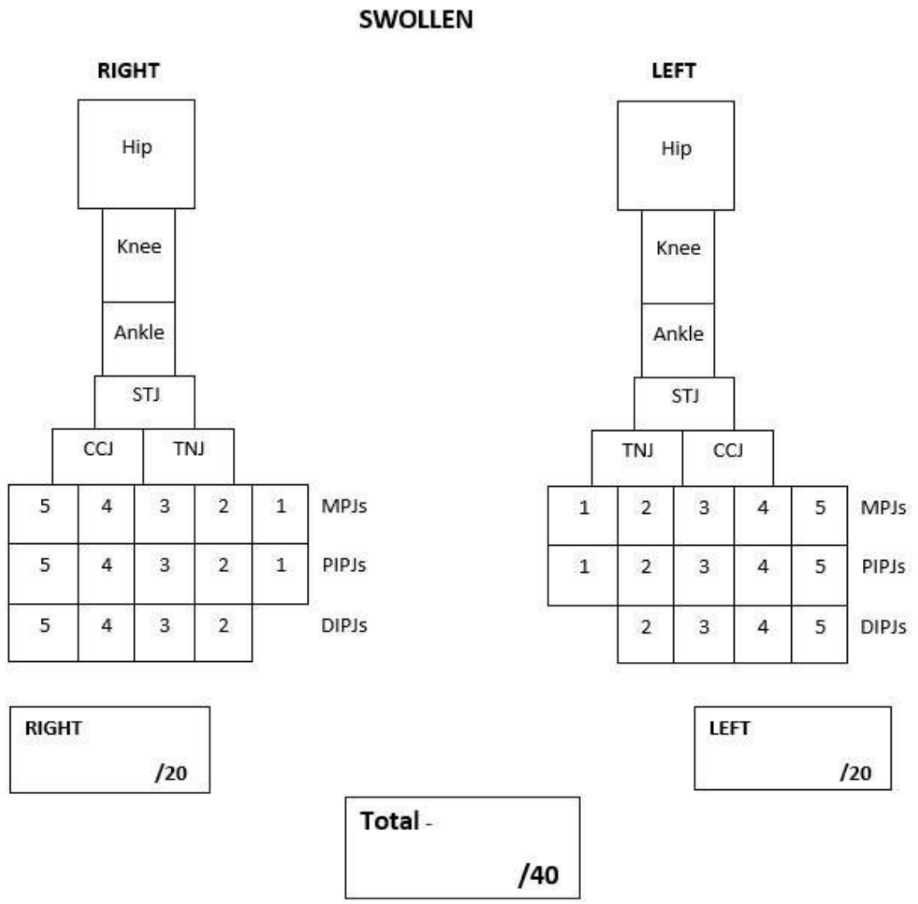
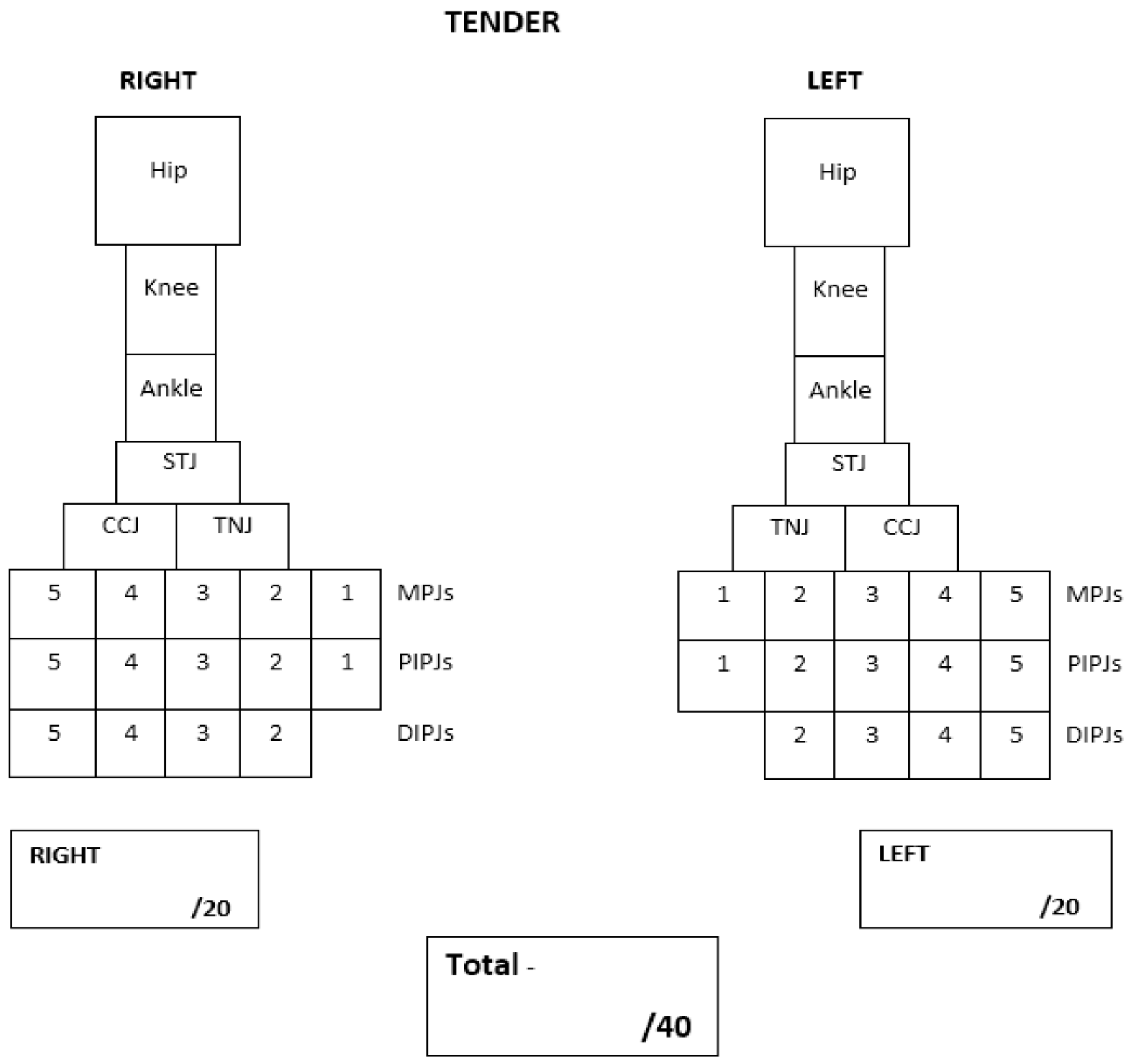
2.3.1. Physical Examination Tool
2.3.2. Physical Examination
2.4. Sample Size
2.5. Statistical Analysis
3. Results
3.1. MRI Scans
3.2. Physical Examination
3.3. Diagnostic Accuracy
3.4. Joint Effusion versus Physical Examination
3.5. Joint Synovitis versus Physical Examination
3.6. Inter-Rater Agreement between Paediatric Rheumatologist and Podiatrist
3.7. Intra-Rater Agreement of Podiatrist
3.8. Inter-Rater Agreement between Radiologists
3.9. Positive and Negative Agreement
4. Discussion
4.1. Limitations
4.2. Clinical Implications and Directions for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| JIA | Juvenile idiopathic arthritis |
| MRI | magnetic resonance imaging |
| PE | physical examination |
| AHPs | allied health professionals |
| PR | paediatric rheumatologist |
| SD | standard deviations |
References
- Ravelli, A.; Martini, A. Juvenile idiopathic arthritis. Lancet 2007, 369, 767–778. [Google Scholar] [CrossRef]
- Foster, H.; Rapley, T.; May, C. Juvenile idiopathic arthritis: Improved outcome requires improved access to care. Rheumatology 2010, 49, 401–403. [Google Scholar] [CrossRef] [PubMed]
- Bourdier, P.; Saidi, O.; Rochette, E.; Ratel, S.; Merlin, E.; Pereira, B.; Duché, P. Physical activity and sedentary levels in children with juvenile idiopathic arthritis and inflammatory bowel disease. A systematic review and meta-analysis. Pediatr. Res. 2019, 86, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Fellas, A.; Hawke, F.; Santos, D.; Coda, A. Prevalence, presentation and treatment of lower limb pathologies in juvenile idiopathic arthritis: A narrative review. J. Paediatr. Child Health 2017, 53, 836–840. [Google Scholar] [CrossRef] [PubMed]
- Hendry, G.; Gardner-Medwin, J.; Watt, G.F.; Woodburn, J. A survey of foot problems in juvenile idiopathic arthritis. Musculoskelet. Care 2008, 6, 221–232. [Google Scholar] [CrossRef]
- Spraul, G.; Koenning, G. A descriptive study of foot problems in children with juvenile rheumatoid arthritis (JRA). Arthritis Care Res. 1994, 7, 144–150. [Google Scholar] [CrossRef]
- Ferrari, J. A review of the foot deformities seen in juvenile chronic arthritis. Foot 1998, 8, 193–196. [Google Scholar] [CrossRef]
- Jousse-Joulin, S.; Breton, S.; Cangemi, C.; Fenoll, B.; Bressolette, L.; De Parscau, L.; Saraux, A.; Devauchelle-Pensec, V. Ultrasonography for detecting enthesitis in juvenile idiopathic arthritis. Arthritis Care Res. 2011, 63, 849–855. [Google Scholar] [CrossRef]
- Hendry, G.J.; Gardner-Medwin, J.; Steultjens, M.P.M.; Woodburn, J.; Sturrock, R.D.; Turner, D.E. Frequent discordance between clinical and musculoskeletal ultrasound examinations of foot disease in juvenile idiopathic arthritis. Arthritis Care Res. 2012, 64, 441–447. [Google Scholar] [CrossRef]
- Magni-Manzoni, S.; Epis, O.; Ravelli, A.; Klersy, C.; Veisconti, C.; Lanni, S.; Muratore, V.; Scirè, C.A.; Rossi, S.; Montecucco, C. Comparison of clinical versus ultrasound-determined synovitis in juvenile idiopathic arthritis. Arthritis Care Res. 2009, 61, 1497–1504. [Google Scholar] [CrossRef]
- Dekker, M.; Hoeksma, A.F.; Dekker, J.H.M.; Rossum, M.A.J.V.; Dolman, K.M.; Beckerman, H.; Roorda, L.D. Strong relationships between disease activity, foot-related impairments, activity limitations and participation restrictions in children with juvenile idiopathic arthritis. Clin. Exp. Rheumatol. 2010, 28, 905–911. [Google Scholar] [PubMed]
- Davies, K.; Cleary, G.; Foster, H.; Hutchinson, E.; Baildam, E. BSPAR Standards of Care for children and young people with juvenile idiopathic arthritis. Rheumatology 2010, 49, 1406–1408. [Google Scholar] [CrossRef] [PubMed]
- The Royal Australian College of General Practitioners. Clinical Guideline for the Diagnosis and Management of Juvenile Idiopathic Arthritis. 2009. Available online: http://www.racgp.org.au/your-practice/guidelines/musculoskeletal/juvenileidiopathicarthritis/ (accessed on 25 September 2019).
- Fellas, A.; Singh-Grewal, D.; Santos, D.; Coda, A. Physical Examination Tools Used to Identify Swollen and Tender Lower Limb Joints in Juvenile Idiopathic Arthritis: A Scoping Review. Arthritis 2018, 2018, 3408162. [Google Scholar] [CrossRef]
- Helliwell, P. The Foot and Ankle in Rheumatoid Arthritis: A Comprehensive Guide; Elsevier Health Sciences: Amsterdam, The Netherlands, 2007. [Google Scholar]
- Cameron-Fiddes, V.; Santos, D. The use of ‘off-the-shelf’ foot orthoses in the reduction of foot symptoms in patients with early rheumatoid arthritis. Foot 2013, 23, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Johnson, K. Imaging of juvenile idiopathic arthritis. Pediatr. Radiol. 2006, 36, 743–758. [Google Scholar] [CrossRef]
- Miller, E.; Uleryk, E.; Doria, A.S. Evidence-based outcomes of studies addressing diagnostic accuracy of MRI of juvenile idiopathic arthritis. Am. J. Roentgenol. 2009, 192, 1209–1218. [Google Scholar] [CrossRef]
- Mazzoni, M.; Pistorio, A.; Magnaguagno, F.; Viola, S.; Urru, A.; Magnano, G.M.; Ravelli, A.; Malattia, C. Predictive value of MRI in patients with juvenile idiopathic arthritis in clinical remission. Arthritis Care Res. 2021. [Google Scholar] [CrossRef]
- Hemke, R.; Maas, M.; van Veenendaal, M.; Dolman, K.M.; van Rossum, M.A.; van den Berg, J.M.; Kuijpers, T.W. Contrast-enhanced MRI compared with the physical examination in the evaluation of disease activity in juvenile idiopathic arthritis. Eur. Radiol. 2014, 24, 327–334. [Google Scholar] [CrossRef]
- Nusman, C.M.; Hemke, R.; Benninga, M.A.; Schonenberg-Meinema, D.; Kindermann, A.; van Rossum, M.A.; van den Berg, J.M.; Maas, M.; Kuijpers, T.W. Contrast-enhanced MRI of the knee in children unaffected by clinical arthritis compared to clinically active juvenile idiopathic arthritis patients. Eur. Radiol. 2016, 26, 1141–1148. [Google Scholar] [CrossRef][Green Version]
- Javadi, S.; Kan, J.H.; Orth, R.C.; DeGuzman, M. Wrist and ankle MRI of patients with juvenile idiopathic arthritis: Identification of unsuspected multicompartmental tenosynovitis and arthritis. AJR Am. J. Roentgenol. 2014, 202, 413–417. [Google Scholar] [CrossRef]
- Pascoli, L.; Wright, S.; McAllister, C.; Rooney, M. Prospective evaluation of clinical and ultrasound findings in ankle disease in juvenile idiopathic arthritis: Importance of ankle ultrasound. J. Rheumatol. 2010, 37, 2409–2414. [Google Scholar] [CrossRef] [PubMed]
- Hemke, R.; van Rossum, M.A.; van Veenendaal, M.; Terra, M.P.; Deurloo, E.E.; de Jonge, M.C.; van den Berg, J.M.; Dolman, K.M.; Kuijpers, T.W.; Maas, M. Reliability and responsiveness of the Juvenile Arthritis MRI Scoring (JAMRIS) system for the knee. Eur. Radiol. 2013, 23, 1075–1083. [Google Scholar] [CrossRef] [PubMed]
- Nusman, C.M.; Hemke, R.; Schonenberg, D.; Dolman, K.M.; van Rossum, M.A.; van den Berg, J.M.; Kuijpers, T.W.; Maas, M. Distribution pattern of MRI abnormalities within the knee and wrist of juvenile idiopathic arthritis patients: Signature of disease activity. Am. J. Roentgenol. 2014, 202, W439–W446. [Google Scholar] [CrossRef] [PubMed]
- Nusman, C.M.; Hemke, R.; Schonenberg, D.; Dolman, K.; van Rossum, M.; van den Berg, M.; Maas, M.; Kuijpers, T. Joint inflammation assessed by physical examination and MRI of the knee in juvenile idiopathic arthritis: Low predictive value for synovitis. Pediatr. Rheumatol. 2014, 12, P2. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Participants n = 15 |
|---|---|
| Demographics | |
| Age, years, median (IQR) | 11 (6) |
| Male/female, n | 5/10 |
| Health Status | |
| VAS child reported pain, median (range) | 48 (3–81) |
| PedsQL child reported QoL, median (range) | 62.50 (35.22–87.5) |
| Duration of disease, years median (IQR) | 3 (3) |
| Drug Therapies | |
| NSAIDS, n (%) | 2 (13) |
| Methotrexate, n (%) | 11 (73) |
| Etanercept, n (%) | 1 (7) |
| Adalimumab, n (%) | 3 (23) |
| Tofacitinib, n (%) | 1 (7) |
| Prednisone, n (%) | 1 (7) |
| Tocilizumab, n (%) | 2 (13) |
| Leflunomide, n (%) | 1 (7) |
| Combination Therapy—NSAID and Methotrexate and/or Biologic, n (%) | 1 (7) |
| Combination Therapy—DMARD and Biologic, n (%) | 3 (23) |
| ILAR Subtypes | |
| Persistent Oligoarticular, n (%) | 1 (7) |
| Extended Oligoarticular, n (%) | 3 (23) |
| Polyarticular RF −ve, n (%) | 7 (47) |
| Polyarticular RF +ve, n (%) | 3 (9) |
| Psoriatic, n (%) | 0 (0) |
| Systemic, n (%) | 1 (7) |
| Enthesitis-Related, n (%) | 3 (23) |
| Undifferentiated, n (%) | 0 (0) |
| Imaging and Clinical Findings | Present, n (%) | Absent, n (%) |
|---|---|---|
| MRI—Joint Effusion (n = 195) | ||
| Radiologist 1 | 114 (58.46) | 81 (41.54) |
| Radiologist 2 | 17 (8.72) | 178 (91.28) |
| PR joint swelling | 25 (12.82) | 170 (87.18) |
| Pod joint swelling | 27 (13.85) | 168 (86.15) |
| PR joint tender | 37 (18.97) | 158 (81.03) |
| Pod joint tender | 40 (20.51) | 155 (79.49) |
| MRI—Joint Synovitis (n = 141) | ||
| Radiologist 1 | 83 (58.87) | 58 (41.13) |
| Radiologist 2 | 20 (14.18) | 121 (85.82) |
| PR joint swelling | 18 (12.77) | 123 (87.23) |
| Pod joint swelling | 21 (14.89) | 120 (85.11) |
| PR joint tender | 24 (17.14) | 116 (82.86) |
| Pod joint tender | 24 (17.14) | 116 (82.86) |
| Physical Examination—Joint Swelling (n = 600) | ||
| PR | 41 (6.83) | 559 (93.17) |
| Pod | 44 (7.33) | 556 (92.67) |
| Physical Examination—Joint Tenderness (n = 600) | ||
| PR | 68 (11.33) | 532 (88.67) |
| Pod | 81 (13.50) | 519 (86.50) |
| Comparison | Observed Agreement (%) | Positive Agreement (%) | Negative Agreement (%) | Kappa | 95% Confidence Interval |
|---|---|---|---|---|---|
| Joint Effusion (MRI) vs. Swelling (PE) | |||||
| R1 vs. PR | 50.3 | 30 | 61 | 0.12 | 0.04, 0.19 |
| R1 vs. Pod | 52.3 | 34 | 63 | 0.15 | 0.07, 0.23 |
| R2 vs. PR | 87 | 38 | 48 | 0.31 | 0.11, 0.51 |
| R2 vs. Pod | 85.6 | 36 | 92 | 0.29 | 0.09, 0.48 |
| Joint Effusion (MRI) vs. Tenderness (PE) | |||||
| R1 vs. PR | 50.3 | 26 | 59 | 0.10 | 0.01, 0.19 |
| R1 vs. Pod | 51.8 | 39 | 60 | 0.12 | 0.03, 0.22 |
| R2 vs. PR | 79 | 26 | 88 | 0.16 | −0.002, 0.32 |
| R2 vs. Pod | 80.0 | 32 | 88 | 0.22 | 0.06, 0.38 |
| Joint Synovitis (MRI) vs. Swelling (PE) | |||||
| R1 vs. PR | 46.8 | 26 | 37 | 0.06 | −0.03, 0.15 |
| R1 vs. Pod | 50.4 | 33 | 61 | 0.12 | 0.02, 0.21 |
| R2 vs. PR | 84 | 42 | 91 | 0.11 | 0.11, 0.55 |
| R2 vs. Pod | 86.5 | 54 | 92 | 0.46 | 0.25, 0.66 |
| Joint Synovitis (MRI) vs. Tenderness (PE) | |||||
| R1 vs. PR | 53.2 | 39 | 62 | 0.16 | 0.06, 0.26 |
| R1 vs. Pod | 51.1 | 36 | 61 | 0.12 | 0.02, 0.23 |
| R2 vs. PR | 87 | 59 | 92 | 0.52 | 0.32, 0.71 |
| R2 vs. Pod | 87.1 | 59 | 92 | 0.52 | 0.32, 0.71 |
| Physical Examination Pod vs. PR | |||||
| Swelling | 96.5 | 75 | 98 | 0.73 | 0.63, 0.84 |
| Tenderness | 91.5 | 66 | 95 | 0.61 | 0.51, 0.71 |
| Physical Examination Pod Intra-rater | |||||
| Swelling | 100 | 100 | 100 | 1 | |
| Tenderness | 98.5 | 95 | 99 | 0.93 | 0.89, 0.98 |
| MRI Examination R1 vs. R2 | |||||
| Effusion | 50.3 | 26 | 63 | 0.13 | 0.07, 0.19 |
| Synovitis | 49.7 | 31 | 60 | 0.11 | 0.01, 0.20 |
| Comparison | Joints | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ankle | STJ | CCJ | TNJ | |||||||||
| OA (%) | PA (%) | NA (%) | OA (%) | PA (%) | NA (%) | OA (%) | PA (%) | NA (%) | OA (%) | PA (%) | NA (%) | |
| Joint Effusion (MRI) vs. Swelling (PE) | ||||||||||||
| R1 vs. R2 | 80 | 82.4 | 76.9 | 35.7 | 18.2 | 47.1 | 43.8 | 40 | 47.1 | 37.5 | 28.6 | 44.4 |
| R1 vs. Pod | 73.3 | 77.8 | 66.7 | 64.2 | 70.6 | 54.5 | 37.5 | 37.5 | 37.5 | 68.8 | 73.7 | 61.5 |
| R1 vs. PR | 60 | 70 | 40 | 57.1 | 62.5 | 50 | 56.3 | 58.8 | 53.3 | 50 | 50 | 50 |
| R2 vs. Pod | 80 | 80 | 80 | 42.9 | 0 | 60 | 68.8 | 28.6 | 80 | 56.3 | 22.2 | 69.6 |
| R2 vs. PR | 66.7 | 70.6 | 61.5 | 50 | 0 | 66.7 | 62.5 | 25 | 75 | 75 | 33.3 | 84.6 |
| Joint Synovitis (MRI) vs. Swelling (PE) | ||||||||||||
| R1 vs. R2 | 60 | 66.7 | 50 | 50 | 54.5 | 44.4 | 50 | 54.5 | 44.4 | 60 | 71.4 | 33.3 |
| R1 vs. Pod | 50 | 61.2 | 28.6 | 30 | 46.2 | 0 | 60 | 66.7 | 50 | 60 | 71.4 | 33.3 |
| R1 vs. PR | 70 | 80 | 40 | 20 | 33.3 | 0 | 40 | 40 | 40 | 40 | 50 | 25 |
| R2 vs. Pod | 70 | 72.7 | 66.7 | 60 | 50 | 66.7 | 50 | 28.6 | 61.5 | 60 | 60 | 60 |
| R2 vs. PR | 50 | 61.5 | 28.6 | 70 | 57.1 | 76.9 | 70 | 40 | 80 | 40 | 25 | 50 |
| Swelling (PE) | ||||||||||||
| Pod vs. PR | 86.7 | 84.6 | 88.2 | 93.3 | 87.5 | 95.5 | 76.7 | 46.2 | 85.1 | 86.7 | 75 | 90.9 |
| Tenderness (PE) | ||||||||||||
| Pod vs. PR | 63.3 | 64.5 | 62.1 | 76.7 | 63.2 | 82.9 | 86.7 | 81.2 | 89.5 | 86.7 | 83.3 | 88.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fellas, A.; Singh-Grewal, D.; Chaitow, J.; Warner, D.; Onikul, E.; Santos, D.; Clapham, M.; Coda, A. Physical Examination Tool for Swollen and Tender Lower Limb Joints in Juvenile Idiopathic Arthritis: A Pilot Diagnostic Accuracy Study. Int. J. Environ. Res. Public Health 2022, 19, 4517. https://doi.org/10.3390/ijerph19084517
Fellas A, Singh-Grewal D, Chaitow J, Warner D, Onikul E, Santos D, Clapham M, Coda A. Physical Examination Tool for Swollen and Tender Lower Limb Joints in Juvenile Idiopathic Arthritis: A Pilot Diagnostic Accuracy Study. International Journal of Environmental Research and Public Health. 2022; 19(8):4517. https://doi.org/10.3390/ijerph19084517
Chicago/Turabian StyleFellas, Antoni, Davinder Singh-Grewal, Jeffrey Chaitow, Denise Warner, Ella Onikul, Derek Santos, Matthew Clapham, and Andrea Coda. 2022. "Physical Examination Tool for Swollen and Tender Lower Limb Joints in Juvenile Idiopathic Arthritis: A Pilot Diagnostic Accuracy Study" International Journal of Environmental Research and Public Health 19, no. 8: 4517. https://doi.org/10.3390/ijerph19084517
APA StyleFellas, A., Singh-Grewal, D., Chaitow, J., Warner, D., Onikul, E., Santos, D., Clapham, M., & Coda, A. (2022). Physical Examination Tool for Swollen and Tender Lower Limb Joints in Juvenile Idiopathic Arthritis: A Pilot Diagnostic Accuracy Study. International Journal of Environmental Research and Public Health, 19(8), 4517. https://doi.org/10.3390/ijerph19084517