
Knowledge, Attitudes, Beliefs, and Practices Regarding Dengue in La Réunion Island, France

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sites and Population
2.2. Study Design
3. Results
3.1. Results of the Quantitative Study
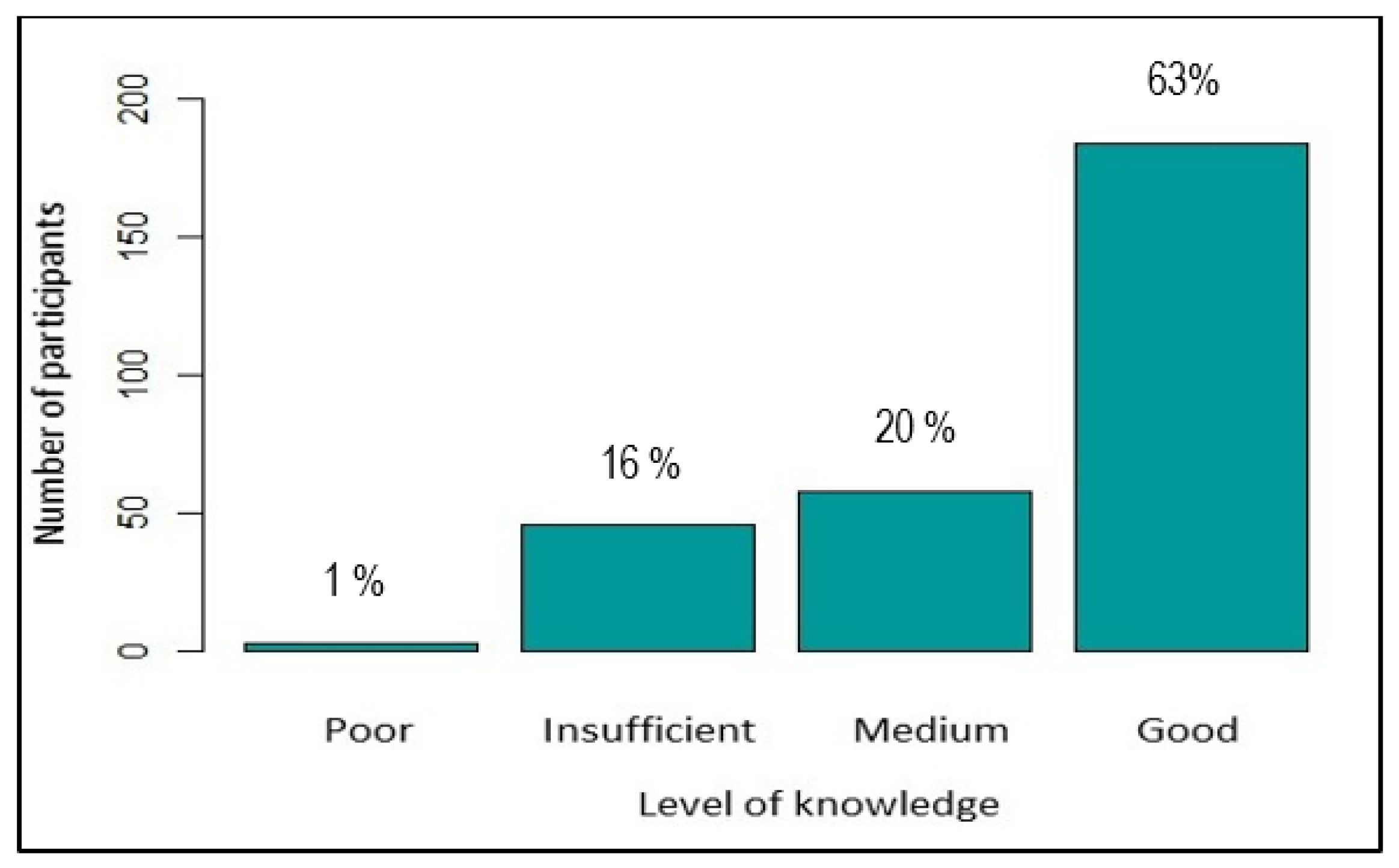
3.1.1. Level of Knowledge about Dengue
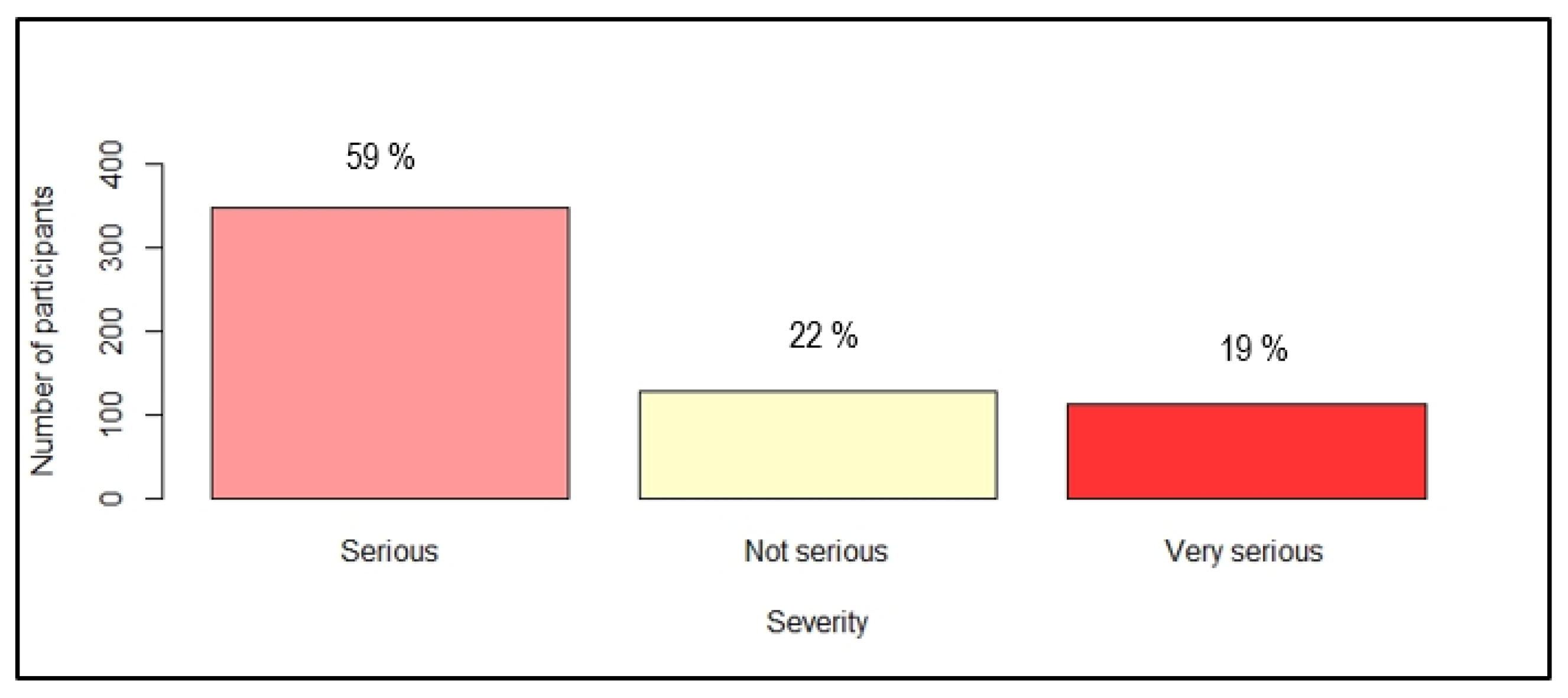
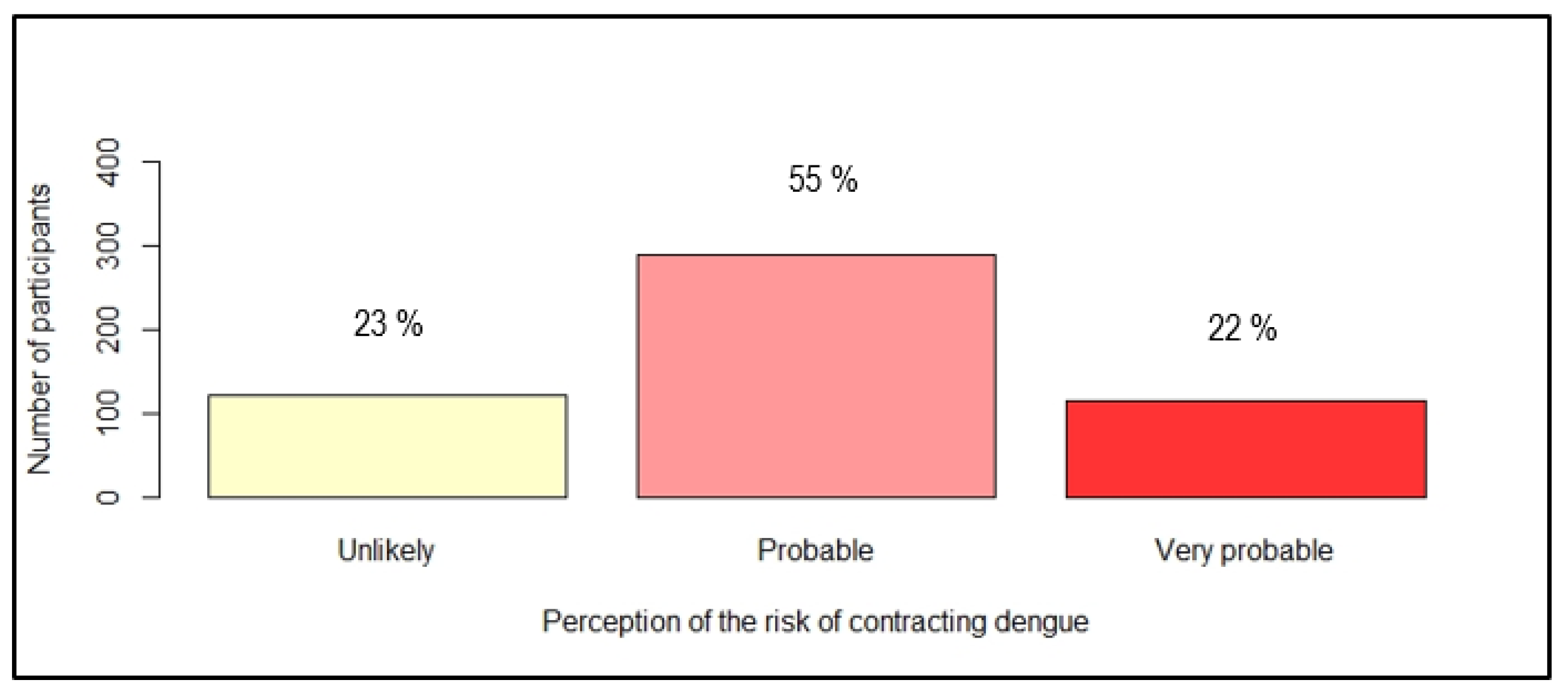
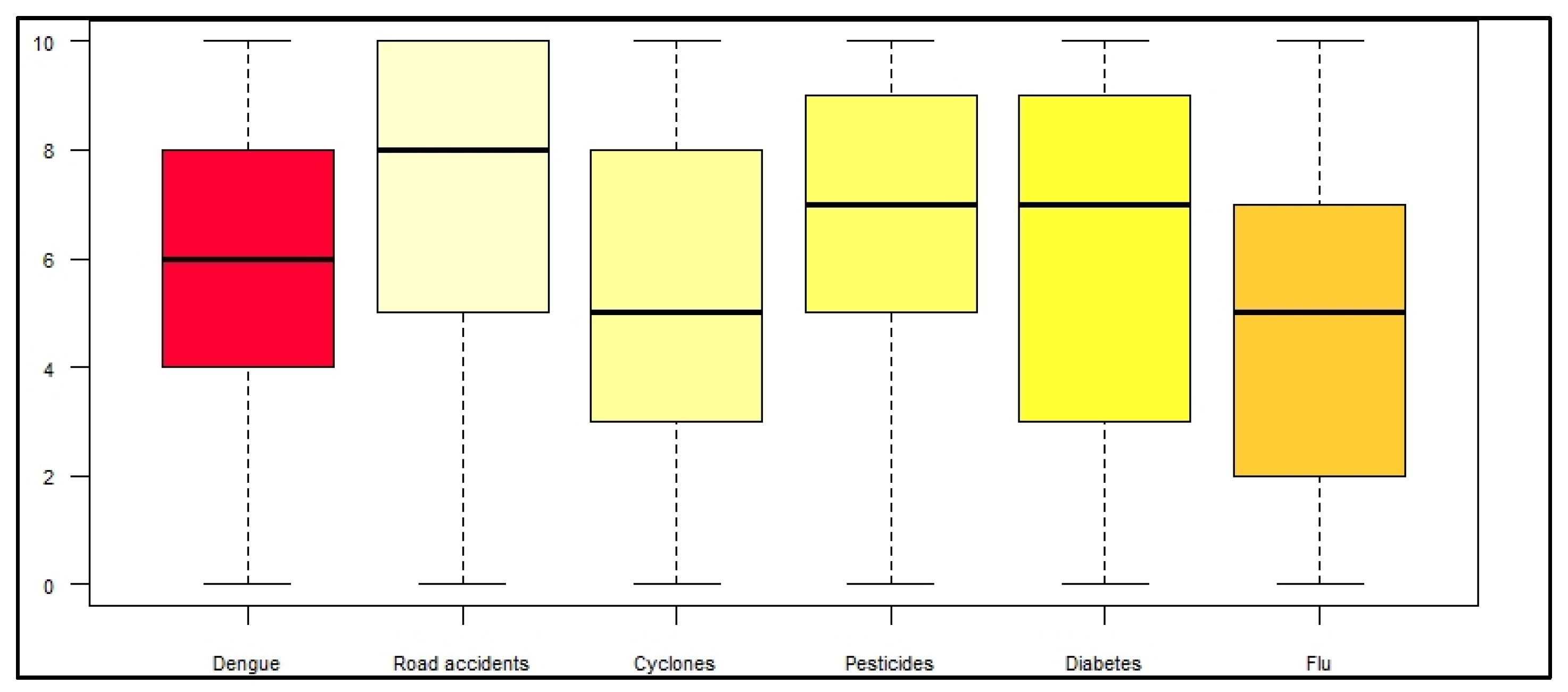
3.1.2. Perception of Danger Related to Dengue
3.1.3. Use of protective Measures against Mosquito Bites
3.2. Results of the Qualitative Study
3.2.1. Knowledge and Beliefs about Dengue
3.2.2. Perception of Danger
3.2.3. Perception of Local Ecology
3.2.4. Responsibility for Prevention
3.2.5. Individual Beliefs: A Barrier to Prevention?
3.2.6. Motivation and Confidence in Public Authorities
3.2.7. Vision of the Future
4. Discussion
Strengths and Limits
- (i)
- Quantitative recruitment bias: field recruitment took place during the week, in normal working hours. Indeed, the sample showed a high proportion of retired people, who were more available at this time slot.
- (ii)
- Information biases: with certain variables being declarative, it is relevant to think that estimates are over or underestimated. For example, the frequency of use of protective measures may have been overestimated, as participants were able to respond by compliance with the obligations conveyed in prevention campaigns.
- (iii)
- Confounding factors: the variable “type of environment” was not used to conclude on the results of the study. Indeed, this data cannot be used as such and should be subjected to additional analysis relating to the social level with additional data that were not available.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bhatt, S.; Gething, P.W.; Brady, O.J.; Messina, J.P.; Farlow, A.W.; Moyes, C.L.; Drake, J.M.; Brownstein, J.S.; Hoen, A.G.; Sankoh, O.; et al. The global distribution and burden of dengue. Nature 2013, 496, 504–507. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Dengue: Guidelines for Diagnosis, Treatment, Prevention, and Control, 1st ed.; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Raharimalala, F.N.; Ravaomanarivo, L.H.; Ravelonandro, P.; Rafarasoa, L.S.; Zouache, K.; Tran-Van, V.; Mousson, L.; Failloux, A.-B.; Hellard, E.; Moro, C.V.; et al. Biogeography of the two major arbovirus mosquito vectors, Aedes aegypti and Aedes albopictus (Diptera, Culicidae), in Madagascar. Parasit Vectors 2012, 5, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Ortenzio, E.; Balleydier, E.; Baville, M.; Filleul, L.; Renault, P. Dengue à la Réunion et dans les îles du sud-ouest de l’océan Indien. Médecine Mal. Infect. 2011, 41, 475–479. [Google Scholar] [CrossRef]
- ANSES. Avis Révisé Relatif à L’analyse de la Stratégie de Lutte Anti-Vectorielle (LAV) Mise en Oeuvre à La Réunion Depuis 2017; Agence Nationale de Sécurité Sanitaire de L’alimentation, de L’environnement et du Travail: Maisons-Alfort, France, 2018. [Google Scholar]
- Santé Publique France. Surveillance de la Dengue à La Réunion. Point au 9 aout 2021. Available online: https://www.santepubliquefrance.fr/regions/ocean-indien/documents/bulletin-regional/2021/surveillance-de-la-dengue-a-la-reunion.-point-au-9-aout-2021 (accessed on 23 November 2021).
- Setbon, M.; Raude, J. Le chikungunya à la Réunion: Facteurs sociaux, environnementaux et comportementaux en situation épidémique. Population 2008, 63, 555–583. [Google Scholar] [CrossRef] [Green Version]
- Setbon, M.; Raude, J. Perceptions et comportements de prévention face à la dengue en Martinique. Med. Mal. Infect. 2008, 38, S78–S81. [Google Scholar] [CrossRef]
- Harapan, H.; Rajamoorthy, Y.; Anwar, S.; Bustamam, A.; Radiansyah, A.; Angraini, P.; Fasli, R.; Salwiyadi, S.; Bastian, R.A.; Oktiviyari, A.; et al. Knowledge, attitude, and practice regarding dengue virus infection among inhabitants of Aceh, Indonesia: A cross-sectional study. BMC Infect. Dis. 2018, 18, 96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benítez Díaz, L.; Diaz-Quijano, F.; Martínez-Vega, R. Experience and perception of risk associated with knowledge, attitudes and practices regarding dengue in Riohacha, Colombia. Ciência Saúde Coletiva 2020, 25, 1137–1146. [Google Scholar] [PubMed]
- Wong, L.P.; Shakir, S.M.M.; Atefi, N.; Abubakar, S. Factors affecting dengue prevention practices: Nationwide survey of the Malaysian public. PLoS ONE 2015, 10, e0122890. [Google Scholar] [CrossRef] [PubMed]
- Suwanbamrung, C.; Saengsuwan, B.; Sangmanee, T.; Thrikaew, N.; Srimoung, P.; Maneerattanasak, S. Knowledge, attitudes, and practices towards dengue prevention among primary school children with and without experience of previous dengue infection in southern Thailand. One Health 2021, 13, 100275. [Google Scholar] [CrossRef] [PubMed]
- Rami, A.; Zuharah, W.F. School-based health education for dengue control in Kelantan, Malaysia: Impact on knowledge, attitude and practice. PLOS Negl. Trop. Dis. 2020, 14, e0008075. [Google Scholar]
- Ghebreab, L.; Zainuddin, H. Factors associated with knowledge and attitude on prevention of dengue fever among international postgraduate students in a malaysian university. Int. J. Public Health Clin. Sci. 2018, 5, 2289–7577. [Google Scholar]
- Ibrahim, A. Effect of Health Education on Dengue Fever: A Comparison of Knowledge, Attitude, and Practices in Public and Private High School Children of Jeddah. Cureus 2018, 10, e3809. [Google Scholar]
- World Health Organization. Action Mondiale Pour Lutter Contre Les Vecteurs 2017–2030; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Social and Environmental Determinants of Aedes Aegypti Infestation in Central Havana: Results of a Case–Control Study Nested in an Integrated Dengue Surveillance Programme in Cuba-Spiegel-2007-Tropical Medicine and International Health-Wiley Online Library. Available online: https://onlinelibrary-wiley-com.docelec.u-bordeaux.fr/doi/full/10.1111/j.1365-3156.2007.01818.x (accessed on 18 August 2020).
- Adalja, A.A.; Sell, T.K.; Bouri, N.; Franco, C. Lessons Learned during Dengue Outbreaks in the United States, 2001–2011. Emerg. Infect. Dis. 2012, 18, 608–614. [Google Scholar] [CrossRef] [PubMed]
- Santé Publique France. Connaissances, attitudes et pratiques de la population en vue de l’amélioration des actions de prévention de l’épidémie de Zika en Guadeloupe. BVS 2017, 41, 36–39. [Google Scholar]
- Dupé, S. Séparer les Moustiques des Humains à La Réunion. Co-Production d’un Nouvel Ordre Socio-Naturel en Contexte Post-Colonial. Ph.D. Thesis, Université de la Réunion, Saint-Denis, France, 2015. Available online: https://tel.archives-ouvertes.fr/tel-01391435 (accessed on 9 June 2020).
- Thuilliez, J.; Bellia, C.; Dehecq, J.-S.; Reilhes, O. Household-Level Expenditure on Protective Measures Against Mosquitoes on the Island of La Réunion, France. PLoS Negl. Trop. Dis. 2014, 8, e2609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmerman, M.A.; Israel, B.A.; Schulz, A.; Checkoway, B. Further explorations in empowerment theory: An empirical analysis of psychological empowerment. Am. J. Community Psychol. 1992, 20, 707–727. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| LEVEL OF KNOWLEDGE | |||||||
|---|---|---|---|---|---|---|---|
| Poor or insufficient | Medium | Good | p | ||||
| n | % | n | % | n | % | ||
| GENDER | 0.2 | ||||||
| Female | 33 | 18 | 29 | 16 | 118 | 66 | |
| Male | 16 | 14 | 29 | 26 | 66 | 60 | |
| AGE | <0.005 | ||||||
| Mean | 61 | 52 | 49 | ||||
| IC95% | 57—66 | 48—57 | 47—51 | ||||
| LEVEL OF EDUCATION | <0.005 | ||||||
| None or primary | 24 | 46 | 14 | 26 | 15 | 28 | |
| Secondary 1 | 20 | 21 | 25 | 27 | 49 | 52 | |
| Secondary 2 | 3 | 6 | 12 | 23 | 37 | 71 | |
| Bac + 2 | 1 | 4 | 3 | 11 | 22 | 85 | |
| Bac > +2 | 1 | 2 | 4 | 6 | 61 | 92 | |
| SOCIOPROFESSIONNAL CATEGORY | <0.005 | ||||||
| Schoolchild or student | 0 | 0 | 3 | 18 | 14 | 82 | |
| Housewife | 5 | 17 | 7 | 24 | 17 | 59 | |
| State employee | 4 | 10 | 4 | 10 | 32 | 80 | |
| Private employee | 3 | 7 | 6 | 13 | 37 | 80 | |
| Independant | 1 | 4 | 7 | 25 | 20 | 71 | |
| Unemployed | 12 | 24 | 17 | 35 | 20 | 41 | |
| Retired | 24 | 30 | 14 | 18 | 41 | 52 | |
| USE OF PROTECTIVE MEASURE | 0.5 | ||||||
| Yes | 32 | 15 | 44 | 21 | 134 | 64 | |
| No | 17 | 21 | 14 | 17 | 50 | 62 | |
| PERCEPTION OF SEVERITY | |||||||
|---|---|---|---|---|---|---|---|
| Not serious | Serious | Very serious | p | ||||
| n | % | n | % | n | % | ||
| GENDER | 0.01 | ||||||
| Female | 59 | 17 | 210 | 62 | 69 | 20 | |
| Male | 68 | 27 | 138 | 56 | 42 | 17 | |
| AGE | 0.01 | ||||||
| Mean | 46 | 49 | 50 | ||||
| IC95% | 42—49 | 47—51 | 57—54 | ||||
| LEVEL OF EDUCATION | 0.02 | ||||||
| None or primary | 15 | 15 | 68 | 67 | 19 | 19 | |
| Secondary 1 | 32 | 18 | 112 | 62 | 36 | 20 | |
| Secondary 2 | 23 | 18 | 76 | 60 | 27 | 21 | |
| Bac + 2 | 14 | 27 | 29 | 58 | 9 | 17 | |
| Bac > +2 | 42 | 34 | 61 | 50 | 20 | 16 | |
| SOCIOPROFESSIONNAL CATEGORY | 0.004 | ||||||
| Schoolchild or student | 16 | 21 | 51 | 67 | 9 | 12 | |
| Housewife | 10 | 17 | 38 | 64 | 11 | 19 | |
| State employee | 21 | 27 | 36 | 46 | 21 | 27 | |
| Private employee | 23 | 29 | 47 | 59 | 10 | 13 | |
| Independant | 20 | 37 | 21 | 39 | 13 | 24 | |
| Unemployed | 12 | 16 | 48 | 65 | 14 | 19 | |
| Retired | 23 | 15 | 101 | 65 | 31 | 20 | |
| ANTECEDENT OF DENGUE-LIKE SYNDROM | 0.6 | ||||||
| Yes | 51 | 24 | 126 | 59 | 38 | 18 | |
| No | 76 | 20 | 221 | 60 | 74 | 20 | |
| FEELING OF BEING BITTEN BY MOSQUITOES | 0.6 | ||||||
| Often | 49 | 22 | 130 | 58 | 47 | 21 | |
| Occasionnaly | 37 | 26 | 78 | 56 | 25 | 18 | |
| Rarely | 29 | 17 | 107 | 64 | 31 | 19 | |
| Never | 12 | 23 | 32 | 60 | 9 | 17 | |
| LEVEL OF KNOWLEDGE ABOUT DENGUE | 0.3 | ||||||
| Poor or insufficient | 32 | 27 | 65 | 55 | 22 | 18 | |
| Medium | 61 | 21 | 174 | 61 | 51 | 18 | |
| Good | 22 | 19 | 63 | 56 | 28 | 25 | |
| PERCEPTION OF RISK | |||||||
|---|---|---|---|---|---|---|---|
| Unlikely | Probable | Very probable | p | ||||
| n | % | n | % | n | % | ||
| GENDER | 0.2 | ||||||
| Female | 59 | 19 | 175 | 58 | 69 | 23 | |
| Male | 62 | 28 | 113 | 51 | 46 | 21 | |
| AGE | 0.4 | ||||||
| Mean | 42 | 49 | 46 | ||||
| IC95% | 43—51 | 47—51 | 43—49 | ||||
| LEVEL OF EDUCATION | 0.2 | ||||||
| None or primary | 21 | 27 | 38 | 49 | 19 | 24 | |
| Secondary 1 | 35 | 23 | 93 | 60 | 26 | 17 | |
| Secondary 2 | 29 | 25 | 65 | 57 | 21 | 18 | |
| Bac + 2 | 10 | 20 | 29 | 59 | 10 | 20 | |
| Bac > +2 | 24 | 19 | 62 | 50 | 39 | 31 | |
| SOCIOPROFESSIONNAL CATEGORY | 0.0006 | ||||||
| Schoolchild or student | 25 | 40 | 28 | 45 | 9 | 15 | |
| Housewife | 12 | 22 | 29 | 54 | 13 | 24 | |
| State employee | 10 | 13 | 41 | 53 | 27 | 35 | |
| Private employee | 11 | 14 | 46 | 61 | 19 | 25 | |
| Independant | 6 | 13 | 26 | 54 | 16 | 33 | |
| Unemployed | 16 | 25 | 37 | 57 | 12 | 18 | |
| Retired | 38 | 29 | 75 | 57 | 19 | 14 | |
| ANTECEDENT OF DENGUE-LIKE SYNDROM | 0.006 | ||||||
| Yes | 30 | 16 | 108 | 57 | 51 | 27 | |
| No | 90 | 27 | 181 | 54 | 64 | 19 | |
| FEELING OF BEING BITTEN BY MOSQUITOES | 0.0002 | ||||||
| Often | 35 | 17 | 109 | 53 | 60 | 30 | |
| Occasionnaly | 24 | 19 | 79 | 62 | 24 | 19 | |
| Rarely | 44 | 30 | 76 | 51 | 28 | 19 | |
| Never | 18 | 40 | 25 | 56 | 2 | 4 | |
| LEVEL OF KNOWLEDGE ABOUT DENGUE | 0.01 | ||||||
| Poor or insufficient | 9 | 25 | 20 | 56 | 7 | 19 | |
| Medium | 15 | 28 | 32 | 61 | 6 | 11 | |
| Good | 22 | 13 | 101 | 58 | 51 | 29 | |
| USE OF PROTECTIVE MEASURES AGAINST MOSQUITO’BITES | |||||
|---|---|---|---|---|---|
| Yes | No | p | |||
| n | % | n | % | ||
| GENDER | 0.003 | ||||
| Female | 268 | 75 | 87 | 25 | |
| Male | 170 | 64 | 94 | 36 | |
| AGE | 0.0002 | ||||
| Mean | 49 | 42 | |||
| IC95% | 48—51 | 36—49 | |||
| LEVEL OF EDUCATION | 0.05 | ||||
| None or primary | 79 | 64 | 45 | 36 | |
| Secondary 1 | 133 | 73 | 49 | 27 | |
| Secondary 2 | 83 | 65 | 45 | 35 | |
| Bac + 2 | 41 | 77 | 12 | 23 | |
| Bac > +2 | 99 | 77 | 29 | 23 | |
| SOCIOPROFESSIONNAL CATEGORY | 0.001 | ||||
| Schoolchild or student | 50 | 52 | 46 | 48 | |
| Housewife | 45 | 76 | 14 | 24 | |
| State employee | 64 | 79 | 17 | 21 | |
| Private employee | 59 | 73 | 22 | 27 | |
| Independant | 40 | 74 | 14 | 26 | |
| Unemployed | 52 | 68 | 25 | 32 | |
| Retired | 121 | 76 | 39 | 24 | |
| ANTECEDENT OF DENGUE-LIKE SYNDROM | 0.1 | ||||
| Yes | 166 | 74 | 57 | 26 | |
| No | 271 | 68 | 125 | 32 | |
| FEELING OF BEING BITTEN BY MOSQUITOES | 0.004 | ||||
| Often | 175 | 75 | 57 | 25 | |
| Occasionnaly | 113 | 75 | 38 | 25 | |
| Rarely | 118 | 67 | 58 | 33 | |
| Never | 31 | 53 | 27 | 47 | |
| PERCEPTION OF SEVERITY | 0.2 | ||||
| Not serious | 83 | 65 | 44 | 35 | |
| Serious | 255 | 73 | 93 | 27 | |
| Very serious | 84 | 75 | 28 | 25 | |
| PERCEPTION OF RISK | 0.1 | ||||
| Unlikely | 86 | 71 | 35 | 29 | |
| Probable | 206 | 68 | 83 | 32 | |
| Very probable | 93 | 73 | 22 | 27 | |
| LEVEL OF KNOWLEDGE ABOUT DENGUE | 0.4 | ||||
| Poor or insufficient | 32 | 65 | 17 | 35 | |
| Medium | 44 | 76 | 14 | 24 | |
| Good | 134 | 73 | 50 | 27 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lamaurt, F.; De Santis, O.; Ramis, J.; Schultz, C.; Rivadeneyra, A.; Waelli, M.; Flahault, A. Knowledge, Attitudes, Beliefs, and Practices Regarding Dengue in La Réunion Island, France. Int. J. Environ. Res. Public Health 2022, 19, 4390. https://doi.org/10.3390/ijerph19074390
Lamaurt F, De Santis O, Ramis J, Schultz C, Rivadeneyra A, Waelli M, Flahault A. Knowledge, Attitudes, Beliefs, and Practices Regarding Dengue in La Réunion Island, France. International Journal of Environmental Research and Public Health. 2022; 19(7):4390. https://doi.org/10.3390/ijerph19074390
Chicago/Turabian StyleLamaurt, Florence, Olga De Santis, Julie Ramis, Cédric Schultz, Ana Rivadeneyra, Mathias Waelli, and Antoine Flahault. 2022. "Knowledge, Attitudes, Beliefs, and Practices Regarding Dengue in La Réunion Island, France" International Journal of Environmental Research and Public Health 19, no. 7: 4390. https://doi.org/10.3390/ijerph19074390
APA StyleLamaurt, F., De Santis, O., Ramis, J., Schultz, C., Rivadeneyra, A., Waelli, M., & Flahault, A. (2022). Knowledge, Attitudes, Beliefs, and Practices Regarding Dengue in La Réunion Island, France. International Journal of Environmental Research and Public Health, 19(7), 4390. https://doi.org/10.3390/ijerph19074390