
Factors Determining the Functional State of Cardiac Surgery Patients with Complicated Postoperative Period


Abstract
1. Background
2. Materials and Methods
2.1. Patient Population
2.2. Assessment of the Functional Status
2.3. Neuromuscular Electrostimulation
2.4. Statistical Analysis
3. Results
4. Discussion
5. Study Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 6MWT | six-minute walk test |
| ADL | activity of daily living |
| BMI | body mass index |
| CABG | coronary artery bypass grafting |
| CBP | cardiopulmonary bypass |
| CLI | chronic limb ischemia |
| COPD | chronic obstructive pulmonary disease |
| CKD-EPI | Chronic Kidney Disease Epidemiology Collaboration |
| GFR | glomerular filtration rate |
| ICU | intensive care unit |
| PCI | percutaneous coronary intervention |
| NMES | neuromuscular electrostimulation |
| NYHA | New York Heart Association |
| SPAP | systolic pulmonary artery pressure |
| FIM | functional independence measure |
References
- Ball, L.; Costantino, F.; Pelosi, P. Postoperative complications of patients undergoing cardiac surgery. Curr. Opin. Crit. Care 2016, 22, 386–392. [Google Scholar] [CrossRef] [PubMed]
- McIsaac, D.I.; McDonald, B.; Wong, C.A.; van Walraven, C. Long-term survival and resource use in critically ill cardiac surgery patients: A population-based study. Can. J. Anaesth. 2018, 65, 985–995. [Google Scholar] [CrossRef] [PubMed]
- Ferrando, A.A.; Lane, H.W.; Stuart, C.A.; Davis-Street, J.; Wolfe, R.R. Prolonged bed rest decreases skeletal muscle and whole body protein synthesis. Am. J. Physiol. 1996, 270, E627–E633. [Google Scholar] [CrossRef] [PubMed]
- Kortebein, P.; Ferrando, A.; Lombeida, J.; Wolfe, R.; Evans, W.J. Effect of 10 days of bed rest on skeletal muscle in healthy older adults. JAMA 2007, 297, 1772–1774. [Google Scholar] [CrossRef]
- Puthucheary, Z.A.; Rawal, J.; McPhail, M.; Connolly, B.; Ratnayake, G.; Chan, P.; Hopkinson, N.S.; Phadke, R.; Dew, T.; Sidhu, P.S.; et al. Acute skeletal muscle wasting in critical illness. JAMA 2013, 310, 1591–1600. [Google Scholar] [CrossRef] [PubMed]
- Hough, C.L.; Needham, D.M. The role of future longitudinal studies in ICU survivors: Understanding determinants and pathophysiology of weakness and neuromuscular dysfunction. Curr. Opin. Crit. Care 2007, 13, 489–496. [Google Scholar] [CrossRef]
- Herridge, M.S.; Tansey, C.M.; Matté, A.; Tomlinson, G.; Diaz-Granados, N.; Cooper, A.; Guest, C.B.; Mazer, C.D.; Mehta, S.; Stewart, T.E.; et al. Functional disability 5 years after acute respiratory distress syndrome. N. Engl. J. Med. 2011, 364, 1293–1304. [Google Scholar] [CrossRef] [PubMed]
- Coker, R.H.; Hays, N.P.; Williams, R.H.; Wolfe, R.R.; Evans, W.J. Bed rest promotes reductions in walking speed, functional parameters, and aerobic fitness in older, healthy adults. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2015, 70, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Cha, S.; Kang, S.; Han, K.; Paik, N.J.; Kim, W.S. High prevalence of physical inactivity after heart valve surgery and its association with long-term mortality: A nationwide cohort study. Eur. J. Prev. Cardiol. 2020, 28, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Kanejima, Y.; Shimogai, T.; Kitamura, M.; Ishihara, K.; Izawa, K.P. Effect of Early Mobilization on Physical Function in Patients after Cardiac Surgery: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 7091. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Xie, G.; Lin, Y.; Chen, L.; Lin, Z.; You, X.; Xie, X.; Dong, D.; Zheng, X.; Li, D.; et al. A systematic review and meta-analysis of the effects of early mobilization therapy in patients after cardiac surgery. Medicine 2021, 100, e25314. [Google Scholar] [CrossRef]
- Honda, Y.; Takahashi, K.; Sasanuma, N.; Itani, Y.; Nagase, M.; Uchiyama, Y.; Tamaki, A.; Sakaguchi, T.; Domen, K. Predictors of Functional Decline in Activities of Daily Living at Discharge in Patients after Cardiovascular Surgery. Circ. J. 2021, 85, 1020–1026. [Google Scholar] [CrossRef] [PubMed]
- Jacob, P.; Gupta, P.; Shiju, S.; Omar, A.S.; Ansari, S.; Mathew, G.; Varghese, M.; Pulimoottil, J.; Varkey, S.; Mahinay, M.; et al. Multidisciplinary, early mobility approach to enhance functional independence in patients admitted to a cardiothoracic intensive care unit: A quality improvement programme. BMJ Open Qual. 2021, 10, e001256. [Google Scholar] [CrossRef] [PubMed]
- Sumin, A.N.; Oleinik, P.A.; Bezdenezhnykh, A.V.; Ivanova, A.V. Neuromuscular electrical stimulation in early rehabilitation of patients with postoperative complications after cardiovascular surgery: A randomized controlled trial. Medicine 2020, 99, e22769. [Google Scholar] [CrossRef]
- Govers, A.C.; Buurman, B.M.; Jue, P.; de Mol, B.A.; Dongelmans, D.A.; de Rooij, S.E. Functional decline of older patients 1 year after cardiothoracic surgery followed by intensive care admission: A prospective longitudinal cohort study. Age Ageing 2014, 43, 575–580. [Google Scholar] [CrossRef]
- Radi, B.; Ambari, A.M.; Dwiputra, B.; Intan, R.E.; Triangto, K.; Santoso, A.; Setianto, B. Determinants and Prediction Equations of Six-Minute Walk Test Distance Immediately After Cardiac Surgery. Front. Cardiovasc. Med. 2021, 8, 685673. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, G.U.; Oliveira Carvalho, V.; de Assis Cacau, L.P.; de Araújo Filho, A.A.; de Cerqueira Neto, M.L.; da Silva, W.M., Jr.; Cerqueira, T.C.; de Santana Filho, V.J. Determinants of distance walked during the six-minute walk test in patients undergoing cardiac surgery at hospital discharge. J. Cardiothorac. Surg. 2014, 9, 95. [Google Scholar] [CrossRef] [PubMed]
- Argunova, Y.A.; Belik, E.V.; Moskin, E.G.; Gruzdeva, O.V.; Pomeshkina, S.A.; Barbarash, O.L. Markers of perioperative myocardial injury in patients undergoing coronary artery bypass grafting depending on the prehabilitation program. Complex Issues Cardiovasc. Dis. 2019, 8, 82–92. [Google Scholar] [CrossRef][Green Version]
- Fernández-Costa, D.; Gómez-Salgado, J.; Castillejo Del Río, A.; Borrallo-Riego, Á.; Guerra-Martín, M.D. Effects of Prehabilitation on Functional Capacity in Aged Patients Undergoing Cardiothoracic Surgeries: A Systematic Review. Healthcare 2021, 9, 1602. [Google Scholar] [CrossRef] [PubMed]
- Da Costa Torres, D.; Dos Santos, P.M.; Reis, H.J.; Paisani, D.M.; Chiavegato, L.D. Effectiveness of an early mobilization program on functional capacity after coronary artery bypass surgery: A randomized controlled trial protocol. SAGE Open Med. 2016, 4, 2050312116682256. [Google Scholar] [CrossRef]
- Cassina, T.; Putzu, A.; Santambrogio, L.; Villa, M.; Licker, M.J. Hemodynamic challenge to early mobilization after cardiac surgery: A pilot study. Ann. Card. Anaesth. 2016, 19, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Malone, D.; Ridgeway, K.; Nordon-Craft, A.; Moss, P.; Schenkman, M.; Moss, M. Physical Therapist Practice in the Intensive Care Unit: Results of a National Survey. Phys. Ther. 2015, 95, 1335–1344. [Google Scholar] [CrossRef] [PubMed]
- Afxonidis, G.; Moysidis, D.V.; Papazoglou, A.S.; Tsagkaris, C.; Loudovikou, A.; Tagarakis, G.; Karapanagiotidis, G.T.; Alexiou, I.A.; Foroulis, C.; Anastasiadis, K. Efficacy of Early and Enhanced Respiratory Physiotherapy and Mobilization after On-Pump Cardiac Surgery: A Prospective Randomized Controlled Trial. Healthcare 2021, 9, 1735. [Google Scholar] [CrossRef]
- Halfwerk, F.R.; van Haaren, J.; Klaassen, R.; van Delden, R.W.; Veltink, P.H.; Grandjean, J.G. Objective Quantification of In-Hospital Patient Mobilization after Cardiac Surgery Using Accelerometers: Selection, Use, and Analysis. Sensors 2021, 21, 1979. [Google Scholar] [CrossRef]
- Borges, D.L.; Silva, M.G.; Silva, L.N.; Fortes, J.V.; Costa, E.T.; Assunção, R.P.; Lima, C.M.; da Silva Nina, V.J.; Bernardo-Filho, M.; Caputo, D.S. Effects of Aerobic Exercise Applied Early After Coronary Artery Bypass Grafting on Pulmonary Function, Respiratory Muscle Strength, and Functional Capacity: A Randomized Controlled Trial. J. Phys. Act. Health 2016, 13, 946–951. [Google Scholar] [CrossRef] [PubMed]
- Iwatsu, K.; Yamada, S.; Iida, Y.; Sampei, H.; Kobayashi, K.; Kainuma, M.; Usui, A. Feasibility of neuromuscular electrical stimulation immediately after cardiovascular surgery. Arch. Phys. Med. Rehabil. 2015, 96, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Hirschhorn, A.D.; Richards, D.; Mungovan, S.F.; Morris, N.R.; Adams, L. Supervised moderate intensity exercise improves distance walked at hospital discharge following coronary artery bypass graft surgery--a randomised controlled trial. Heart Lung Circ. 2008, 17, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Cacciatore, F.; Abete, P.; Mazzella, F.; Furgi, G.; Nicolino, A.; Longobardi, G.; Testa, G.; Langellotto, A.; Infante, T.; Napoli, C.; et al. Six-minute walking test but not ejection fraction predicts mortality in elderly patients undergoing cardiac rehabilitation following coronary artery bypass grafting. Eur. J. Prev. Cardiol. 2012, 19, 1401–1409. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group 1 (n = 31) | Group 2 (n = 29) | p | |
|---|---|---|---|
| Men (n, %) | 26 (83.9) | 17 (58.6) | 0.045 |
| Age (years) | 62.0 [58.0; 65.0] | 65.0 [58.0; 70.0] | 0.131 |
| Height (cm) | 172.0 [167.0; 176.0] | 167,0 [158.0; 174.0] | 0.020 |
| Weight (kg) | 82.0 [70.0; 95.0] | 75.0 [65.0; 85.0] | 0.160 |
| BMI (kg/m2) | 28.4 [24.2; 31.9] | 27.7 [24.5; 30.7] | 0.971 |
| BSA (m2) | 1.94 [1.79; 2.05] | 1.86 [1.73; 1.92] | 0.039 |
| GFR (mL/min/1.73 m2) | 83.4 [76.3; 91.9] | 82.4 [75.7; 89.7] | 0.390 |
| NYHA class ≥ 3 (n, %) | 6 (19.4) | 10 (34.5) | 0.247 |
| MI history (n, %) | 15 (48.4) | 13 (44.83) | 0.802 |
| PCI history (n, %) | 6 (19.4) | 8 (27.6) | 0.547 |
| Hypertension (n, %) | 25 (80.7) | 27 (93.1) | 0.257 |
| Stroke history (n, %) | 2 (6.5) | 6 (20.7) | 0.140 |
| Permanent AF (n, %) | 8 (25.8) | 10 (35.7) | 0.576 |
| Diabetes mellitus (n, %) | 5 (16.1) | 5 (17.9) | 0.590 |
| COPD (n, %) | 11 (35.5) | 9 (31.0) | 0.788 |
| CLI ≥ 2A history (n, %) | 2 (6.5) | 3 (10.3) | 0.666 |
| ICA stenosis > 50% | 4 (14.8) | 6 (21.4) | 0.500 |
| NMES (n, %) | 14 (45.2) | 18 (62.1) | 0.208 |
| Preoperative Examination Data | |||
| End-diastolic volume (mL) | 194.0 [141.0; 272.0] | 187.0 [130.0; 247.0] | 0.976 |
| End-systolic volume (mL) | 83.0 [47.0; 141.0] | 79.0 [54.0; 141.0] | 0.420 |
| Left ventricular ejection fraction (%) | 60.0 [39.0; 65.0] | 57.0 [38.0; 64.0] | 0.762 |
| SPAP, mm Hg | 32.0 [24.5; 37.0] | 39.0 [29.0; 51.0] | 0.051 |
| Types of Surgical Interventions and Their Characteristics | |||
| Isolated CABG (n, %) | 7 (22.6) | 5 (17.2) | 0.750 |
| Aortic valve replacement (n, %) | 1 (3.2) | 3 (10.3) | 0.346 |
| Mitral valve replacement (n, %) | 5 (16.1) | 1 (3.5) | 0.196 |
| CABG+carotid endarterectomy | 2 (6.5) | 0 | 0.492 |
| Combined CABG and valve replacement (n, %) | 3 (9.7) | 7 (20.7) | 0.175 |
| Multivalve operations (n, %) | 3 (9.7) | 2 (6.9) | 0.532 |
| Elective thoracic aorta surgery (n, %) | 2 (6.5) | 4 (13.8) | 0.417 |
| Aortic dissection (n, %) | 1 (3.2) | 2 (6.9) | 0.606 |
| Heart transplantation (n, %) | 2 (6.5) | 2 (6.9) | 0.668 |
| CABG+ventriculoplasty/thrombectomy/radiofrequency ablation | 5 (16.1) | 3 (10.3) | 0.708 |
| Cardiopulmonary bypass (n, %) | 28 (90.3) | 26 (89.7) | 0.632 |
| Cardiopulmonary bypass duration (min) | 109.5 [72.5; 158.5] | 145.5 [117.0; 194.0] | 0.007 |
| Aortic clamping time (min) | 75.0 [45.0; 104.0] | 104.0 [81.0; 130.0] | 0.007 |
| Total duration of surgery (min) | 210.0 [190.0; 260.0] | 245.0 [160.0; 370.0] | 0.384 |
| Peri- and Postoperative Complications in Groups | |||
| Myocardial infarction (n, %) | 0 (0) | 2 (6.9) | 0.229 |
| Heart failure (n, %) | 4 (12.9) | 12 (41.4) | 0.019 |
| Atrial fibrillation (n, %) | 10 (32.3) | 13 (44.8) | 0.427 |
| Sternal wound complication (n,%) | 4 (12.9) | 5 (17.2) | 0.727 |
| Multiple organ failure (n, %) | 5 (16.1) | 10 (34.5) | 0.139 |
| Respiratory failure (n, %) | 5 (16.1) | 7 (24.1) | 0.527 |
| Pericardiocentesis (n, %) | 3 (9.7) | 1 (3.5) | 0.613 |
| Acute renal failure with a course of renal replacement therapy (n, %) | 2 (6.5) | 7 (24.1) | 0.076 |
| Intensive care unit length of stay (d) | 5.5 [3.0; 6.0] | 7.5 [3.0; 12.0] | <0.001 |
| Hospital length of stay (d) | 28.5 [21.0; 36.0] | 33.5 [26.0; 42.0] | 0.089 |
| Group 1 (n = 31) | Group 2 (n = 29) | p | |
|---|---|---|---|
| Right quadriceps strength (kg) | 20.5 [14.4; 27.2] | 18.9 [14.0; 21.8] | 0.101 |
| Left quadriceps strength (kg) | 21.2 [14.9; 29.3] | 17.1 [13.8; 20.3] | 0.083 |
| Right knee flexor strength (kg) | 16.3 [13.4; 23.8] | 12.3 [9.5; 15.1] | 0.003 |
| Left knee flexor strength (kg) | 16.7 [13.2; 25.1] | 12.6 [9.1; 14.9] | 0.001 |
| Right foot extensor strength (kg) | 28.4 [20.0; 36.8] | 22.5 [18.9; 24.9] | 0.007 |
| Right foot flexor strength (kg) | 18.7 [13.1; 23.4] | 14.6 [12.5; 17.6] | 0.043 |
| Left foot extensor strength (kg) | 26.7 [22.2; 36.1] | 21.7 [15.4; 24.9] | <0.001 |
| Left foot flexor strength (kg) | 19.2 [15.4; 23.3] | 13.6 [10.7; 15.9] | <0.001 |
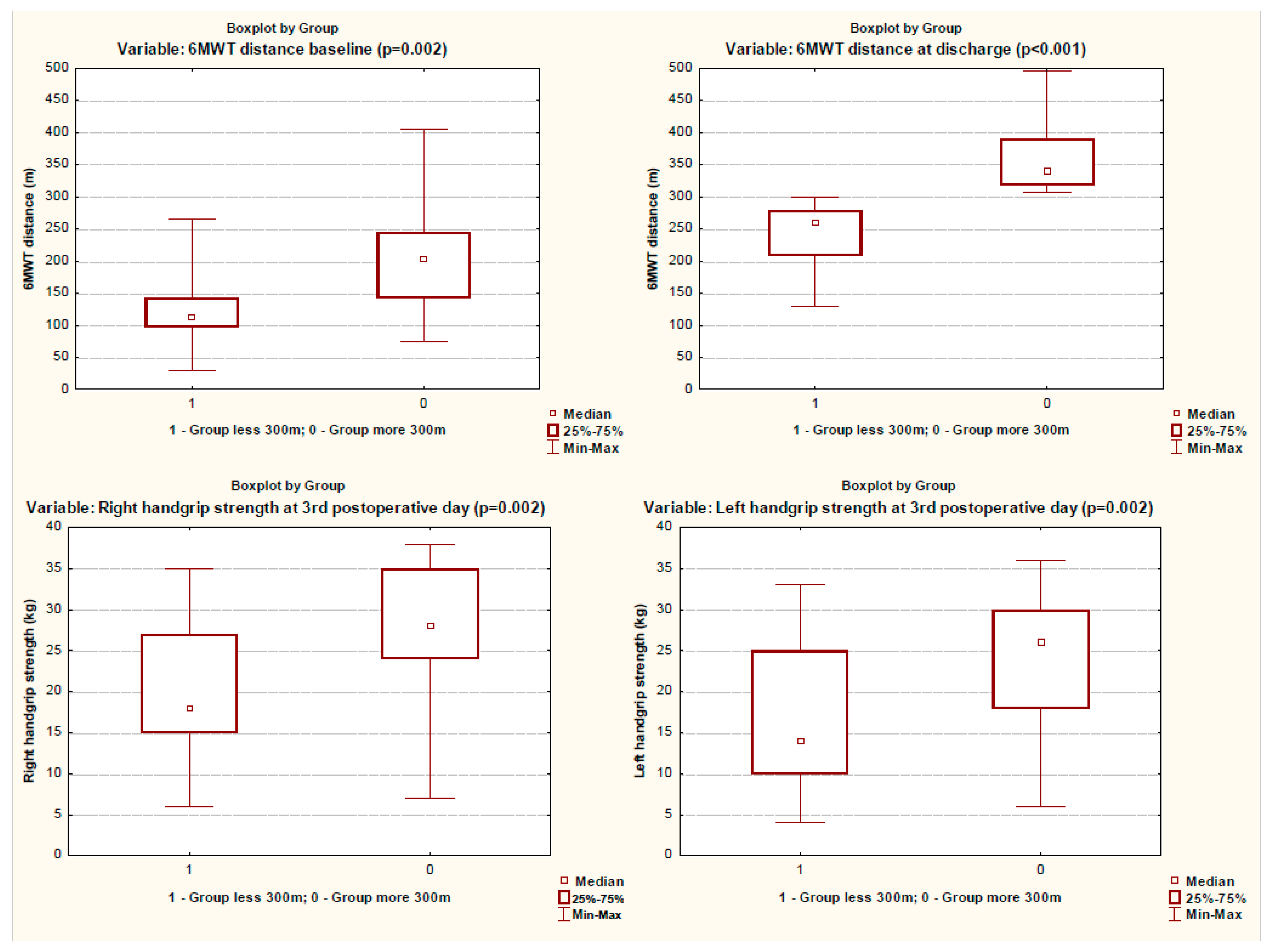
| Distance of 6MWT (m) | 202.5 [142.0; 245.0] | 112.0 [97.0; 143.0] | 0.002 |
| Right handgrip strength (kg) | 28.0 [24.0; 35.0] | 18.0 [15.0; 27.0] | 0.002 |
| Left handgrip strength (kg) | 26.0 [18.0; 30.0] | 14.0 [10.0; 25.0] | 0.002 |
| Group 1 (n = 31) | Group 2 (n = 29) | p | |
|---|---|---|---|
| Right quadriceps strength (kg) | 26.2 [21.4; 29.6] | 23.3 [18.0; 27.7] | 0.083 |
| Left quadriceps strength (kg) | 25.9 [20.7; 30.0] | 22.3 [18.1; 26.1] | 0.056 |
| Right knee flexor strength (kg) | 21.9 [15.8; 25.7] | 14.2 [11.8; 20.1] | 0.003 |
| Left knee flexor strength (kg) | 21.8 [16.9; 27.7] | 15.7 [11.3; 20.2] | 0.001 |
| Right foot extensor strength (kg) | 33.9 [25.2; 38.9] | 25.4 [22.9; 27.8] | <0.001 |
| Right foot flexor strength (kg) | 20.4 [18.0; 25.6] | 16.2 [13.9; 19.2] | <0.002 |
| Left foot extensor strength (kg) | 31.7 [24.7; 37.2] | 23.2 [19.0; 27.7] | <0.001 |
| Left foot flexor strength (kg) | 20.8 [17.8; 24.0] | 14.9 [12.9; 17.4] | <0.001 |
| Distance of 6MWT (m) | 341.0 [318.0; 390.0] | 259.0 [208.0; 278.0] | <0.001 |
| Right handgrip strength (kg) | 32.0 [26.0; 37.0] | 22.0 [18.0; 31.0] | 0.003 |
| Left handgrip strength (kg) | 28.0 [22.0; 32.0] | 18.0 [15.0; 30.0] | 0.002 |
| Dependent Variable: Distance 6MWT | Unstandardized Coefficients | Standardized Coefficients | t | Sig. | |
|---|---|---|---|---|---|
| B | Std. Error | Beta | |||
| Model 1 (total) | |||||
| (Constant) | 452.971 | 72.222 | 6.272 | 0.000 | |
| 6MWT after intensive care unit | 0.273 | 0.151 | 0.234 | 1.803 | 0.085 |
| Cardiopulmonary bypass duration | −0.444 | 0.124 | −0.430 | −3.564 | 0.002 |
| Body mass index | −6.691 | 1.712 | −0.401 | −3.909 | 0.001 |
| Left foot extensor strength | 3.114 | 1.235 | 0.308 | 2.522 | 0.019 |
| Model 2 (patients with NMES) | |||||
| (Constant) | 622.851 | 70.079 | 8.888 | 0.000 | |
| Age | −4.095 | 1.153 | −0.624 | −3.552 | 0.005 |
| Cardiopulmonary bypass duration | −0.380 | 0.156 | −0.427 | −2.430 | 0.035 |
| Model 3 (patients without NMES) | |||||
| (Constant) | 484.451 | 81.021 | 5.979 | 0.000 | |
| Body mass index | −9.315 | 1.960 | −0.588 | −4.753 | 0.001 |
| 6MWT after intensive care unit | 0.332 | 0.140 | 0.327 | 2.376 | 0.039 |
| Left foot extensor strength | 3.162 | 1.388 | 0.321 | 2.278 | 0.046 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sumin, A.N.; Oleinik, P.A.; Bezdenezhnykh, A.V.; Bezdenezhnykh, N.A. Factors Determining the Functional State of Cardiac Surgery Patients with Complicated Postoperative Period. Int. J. Environ. Res. Public Health 2022, 19, 4329. https://doi.org/10.3390/ijerph19074329
Sumin AN, Oleinik PA, Bezdenezhnykh AV, Bezdenezhnykh NA. Factors Determining the Functional State of Cardiac Surgery Patients with Complicated Postoperative Period. International Journal of Environmental Research and Public Health. 2022; 19(7):4329. https://doi.org/10.3390/ijerph19074329
Chicago/Turabian StyleSumin, Alexey N., Pavel A. Oleinik, Andrey V. Bezdenezhnykh, and Natalia A. Bezdenezhnykh. 2022. "Factors Determining the Functional State of Cardiac Surgery Patients with Complicated Postoperative Period" International Journal of Environmental Research and Public Health 19, no. 7: 4329. https://doi.org/10.3390/ijerph19074329
APA StyleSumin, A. N., Oleinik, P. A., Bezdenezhnykh, A. V., & Bezdenezhnykh, N. A. (2022). Factors Determining the Functional State of Cardiac Surgery Patients with Complicated Postoperative Period. International Journal of Environmental Research and Public Health, 19(7), 4329. https://doi.org/10.3390/ijerph19074329