
Experiences and Perspectives of Marketing Authorisation Holders towards Medication Safety Monitoring during Pregnancy: A Pan-European Qualitative Analysis





Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Study Population and Sampling
2.3. Data Collection
2.4. Data Analysis
3. Results
3.1. Characteristics of the Study Participants
3.2. Collection of Data on Medication Use during Pregnancy
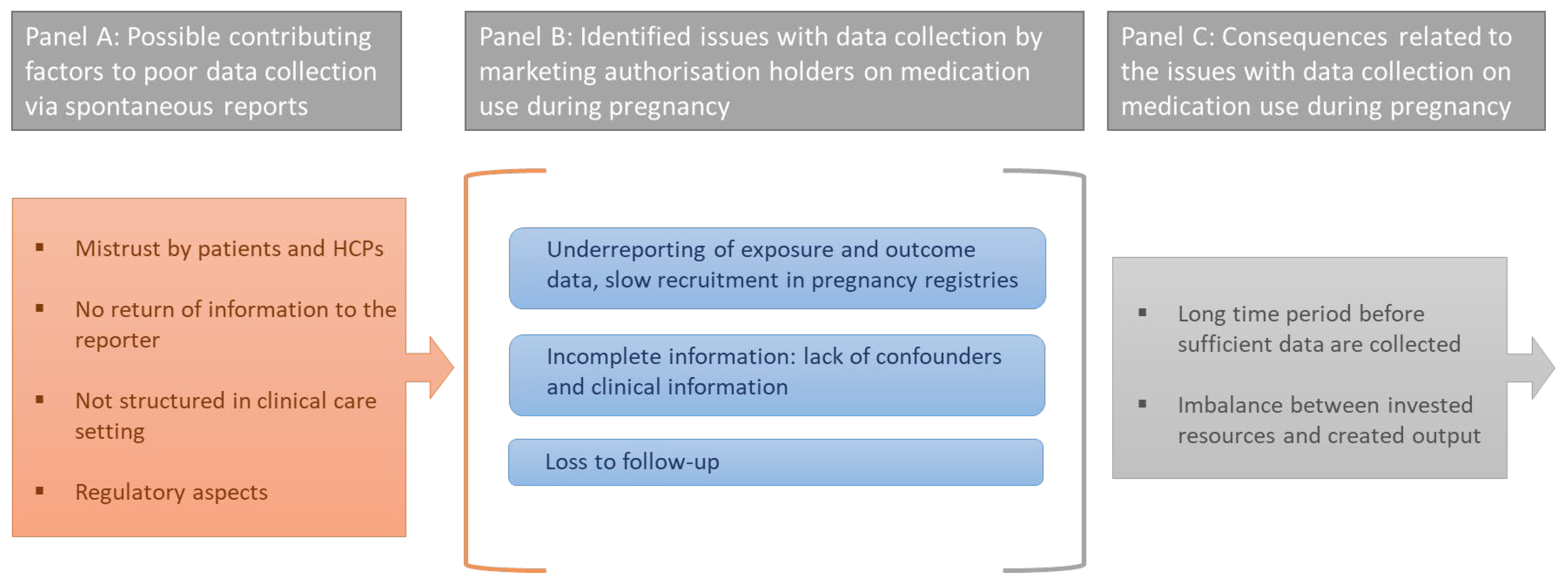
3.2.1. Difficulties with Data Collection on Medication Use during Pregnancy
3.2.2. Data Collection on Long-Term Outcomes Related to Pre-Natal Medication Exposure
3.2.3. Suggestions to Improve Data Collection on Medication Safety during Pregnancy
3.3. Processing of Observational Data on Medication Use during Pregnancy
3.4. Communication of Safety Information in the Label
4. Discussion
4.1. Main Findings
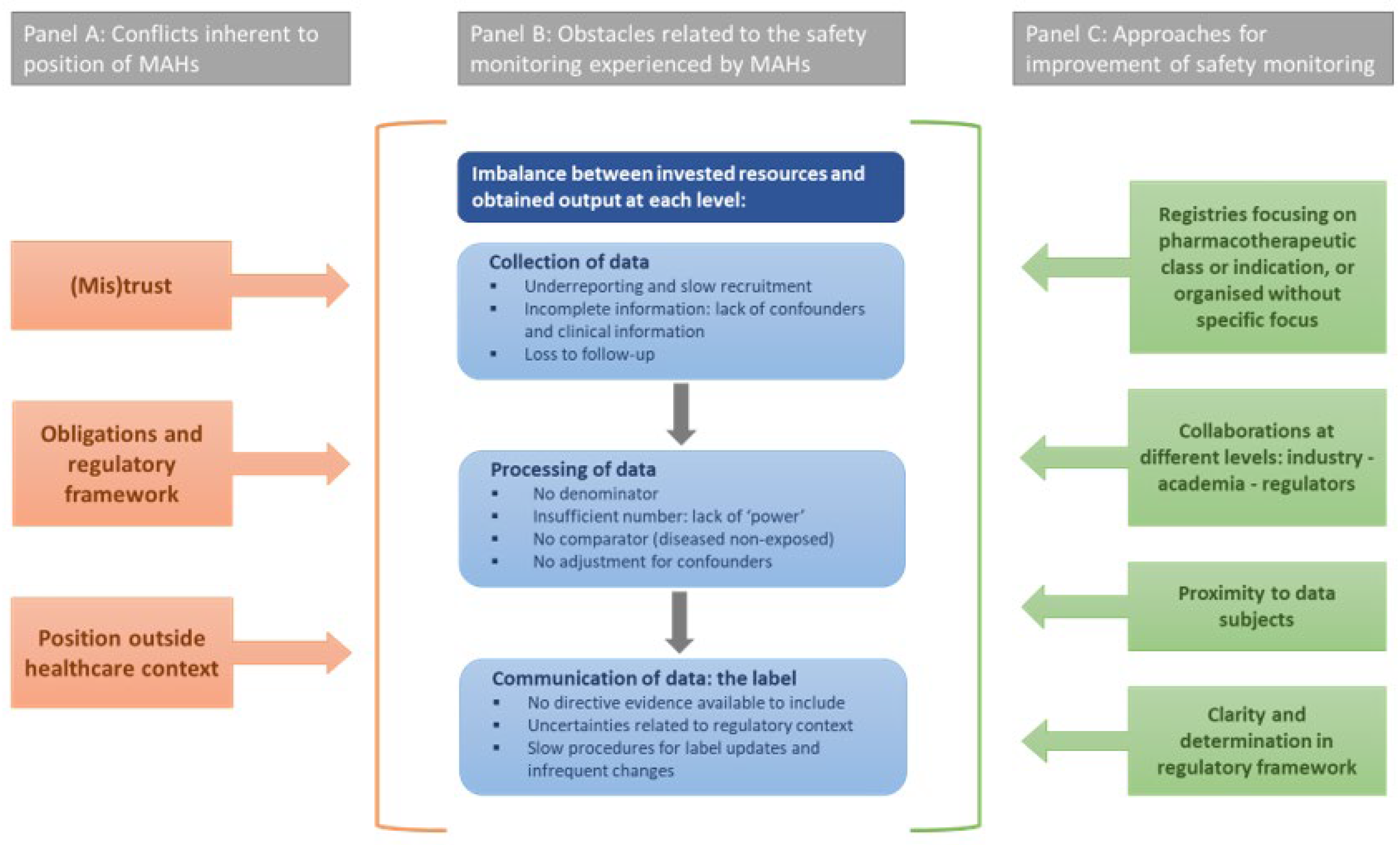
4.2. Approaches for Future Improvement of Safety Monitoring
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Mitchell, A.A.; Gilboa, S.M.; Werler, M.M.; Kelley, K.E.; Louik, C.; Hernández-Díaz, S.; National Birth Defects Prevention Study. Medication use during pregnancy, with particular focus on prescription drugs: 1976–2008. Am. J. Obstet. Gynecol. 2011, 205, 51.e1–51.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lupattelli, A.; Spigset, O.; Twigg, M.J.; Zagorodnikova, K.; Mårdby, A.C.; Moretti, M.E.; Drozd, M.; Panchaud, A.; Hämeen-Anttila, K.; Rieutord, A.; et al. Medication use in pregnancy: A cross-sectional, multinational web-based study. BMJ Open 2014, 4, e004365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adam, M.P.; Polifka, J.E.; Friedman, J. Evolving knowledge of the teratogenicity of medications in human pregnancy. Am. J. Med Genet. Part C Semin. Med. Genet. 2011, 157, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Thorpe, P.G.; Gilboa, S.M.; Hernandez-Diaz, S.; Lind, J.; Cragan, J.D.; Briggs, G.; Kweder, S.; Friedman, J.M.; Mitchell, A.; Honein, M.A.; et al. Medications in the first trimester of pregnancy: Most common exposures and critical gaps in understanding fetal risk. Pharmacoepidemiol. Drug Saf. 2013, 22, 1013–1018. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, A. Systematic Identification of Drugs That Cause Birth Defects—A New Opportunity. N. Engl. J. Med. 2003, 349, 2556–2559. [Google Scholar] [CrossRef]
- Shields, K.; Lyerly, A. Exclusion of Pregnant Women from Industry-Sponsored Clinical Trials. Obstet. Gynecol. 2013, 122, 1077–1081. [Google Scholar] [CrossRef]
- Scaffidi, J.; Mol, B.W.; Keelan, J.A. The pregnant women as a drug orphan: A global survey of registered clinical trials of pharmacological interventions in pregnancy. BJOG Int. J. Obstet. Gynaecol. 2016, 124, 132–140. [Google Scholar] [CrossRef] [Green Version]
- Rubin, R. Pregnant People’s Paradox—Excluded from Vaccine Trials Despite Having a Higher Risk of COVID-19 Complications. JAMA 2021, 325, 1027–1028. [Google Scholar] [CrossRef]
- Van Spall, H.G.C. Exclusion of pregnant and lactating women from COVID-19 vaccine trials: A missed opportunity. Eur. Hear. J. 2021, 42, 2724–2726. [Google Scholar] [CrossRef]
- Mazer-Amirshahi, M.; Samiee-Zafarghandy, S.; Gray, G.; Anker, J.N.V.D. Trends in pregnancy labeling and data quality for US-approved pharmaceuticals. Am. J. Obstet. Gynecol. 2014, 211, 690.e1–690.e11. [Google Scholar] [CrossRef]
- Hoar, R.M. Developmental Toxicity: Extrapolation Across Species. J. Am. Coll. Toxicol. 1995, 14, 11–20. [Google Scholar] [CrossRef]
- Briggs, G.G.; Polifka, J.E.; Wisner, K.; Gervais, E.; Miller, R.K.; Berard, A.; Koren, G.; Forinash, A.; Towers, C.V. Should pregnant women be included in phase IV clinical drug trials? Am. J. Obstet. Gynecol. 2015, 213, 810–815. [Google Scholar] [CrossRef] [PubMed]
- Saint-Raymond, A.; de Vries, C. Medicine safety in pregnancy and ambitions for the EU medicine regulatory framework. Clin. Pharmacol. Ther. 2016, 100, 21–23. [Google Scholar] [CrossRef] [PubMed]
- Cavadino, A.; Sandberg, L.; Öhman, I.; Bergvall, T.; Star, K.; Dolk, H.; Loane, M.; Addor, M.-C.; Barisic, I.; Cavero-Carbonell, C.; et al. Signal Detection in EUROmediCAT: Identification and Evaluation of Medication–Congenital Anomaly Associations and Use of VigiBase as a Complementary Source of Reference. Drug Saf. 2021, 44, 765–785. [Google Scholar] [CrossRef]
- European Medicines Agency—Guideline on Registry-Based Studies (EMA/426390/2021). Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-registry-based-studies_en-0.pdf. (accessed on 23 December 2021).
- European Medicines Agency—GVP Product- or Population-Specific Considerations III: Pregnant and Breastfeeding Women (EMA/653036/2019)—Draft for Public Consultation. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/draft-guideline-good-pharmacovigilance-practices-product-population-specific-considerations-iii_en.pdf (accessed on 23 December 2021).
- US Food and Drug Administration—Postapproval Pregnancy Safety Studies: Guidance for Industry—Draft for Public Consul-tation. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/postapproval-pregnancy-safety-studies-guidance-industry (accessed on 23 December 2021).
- European Federation of Pharmaceutical Industries and Associations—Submission of Comments by EFPIA on GVP Product- or Population-Specific Considerations III: Pregnant and Breastfeeding Women (EMA/653036/2019). Available online: https://www.efpia.eu/media/413688/efpia-comments-on-gvp-population-specific-considerations-iii_-pregnant-and-breastfeeding-women.docx. (accessed on 23 December 2021).
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gale, N.K.; Heath, G.; Cameron, E.; Rashid, S.; Redwood, S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med. Res. Methodol. 2013, 13, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- QSR International Pty Ltd.—NVivo (Released in March 2020). Available online: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home (accessed on 23 December 2021).
- Conception. Available online: https://www.imi-conception.eu (accessed on 23 December 2021).
- Chambers, C.D.; Johnson, D.L. Emerging data on the use of anti-tumor necrosis factor-alpha medications in pregnancy. Birth Defects Res. Part A Clin. Mol. Teratol. 2012, 94, 607–611. [Google Scholar] [CrossRef]
- Hernandez-Diaz, S.; Smith, C.R.; Shen, A.; Mittendorf, R.; Hauser, W.A.; Yerby, M.; Holmes, L.B. Scientific Advisory Committee Comparative safety of antiepileptic drugs during pregnancy. Neurology 2012, 78, 1692–1699. [Google Scholar] [CrossRef] [PubMed]
- King, R.W.; Baca, M.; Armenti, V.T.; Kaplan, B. Pregnancy Outcomes Related to Mycophenolate Exposure in Female Kidney Transplant Recipients. Am. J. Transplant. 2016, 17, 151–160. [Google Scholar] [CrossRef]
- Vorstenbosch, S.; Winkel, B.T.; van Gelder, M.; Kant, A.; Roeleveld, N.; van Puijenbroek, E. Aim and Design of pREGnant, the Dutch Pregnancy Drug Register. Drug Saf. 2018, 42, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Bharti, B.; Lee, S.J.; Lindsay, S.P.; Wingard, D.L.; Jones, K.L.; Lemus, H.; Chambers, C.D. Disease Severity and Pregnancy Outcomes in Women with Rheumatoid Arthritis: Results from the Organization of Teratology Information Specialists Autoimmune Diseases in Pregnancy Project. J. Rheumatol. 2015, 42, 1376–1382. [Google Scholar] [CrossRef] [PubMed]
- Bérard, A. Pharmacoepidemiology Research-Real-World Evidence for Decision Making. Front. Pharmacol. 2021, 12, 723427. [Google Scholar] [CrossRef] [PubMed]
- Lupattelli, A.; Spigset, O.; Nordeng, H. Learning the effects of psychotropic drugs during pregnancy using real-world safety data: A paradigm shift toward modern pharmacovigilance. Int. J. Clin. Pharm. 2018, 40, 783–786. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, D.L.; Uhl, K.; Kweder, S.L. Pregnancy exposure registries. Drug Saf. 2004, 27, 215–228. [Google Scholar] [CrossRef]
- Dublin, S.; Wartko, P.; Mangione-Smith, R. Studying Medication Safety in Pregnancy: A Call for New Approaches, Resources, and Collaborations. Pediatrics 2020, 146, e20201540. [Google Scholar] [CrossRef]
- Broussard, C.S.; Frey, M.T.; Hernandez-Diaz, S.; Greene, M.F.; Chambers, C.D.; Sahin, L.; Sharp, B.A.C.; Honein, M.A. Developing a systematic approach to safer medication use during pregnancy: Summary of a Centers for Disease Control and Prevention–convened meeting. Am. J. Obstet. Gynecol. 2014, 211, 208–214.e1. [Google Scholar] [CrossRef] [Green Version]
- Sahin, L.; Yao, L. Collaboration in Regulatory Science to Facilitate Therapeutic Development for Pregnant Women. Curr. Pharm. Des. 2019, 25, 609–614. [Google Scholar] [CrossRef]
- Charlton, R.A.; Cunnington, M.C.; De Vries, C.S.; Weil, J.G. Data Resources for Investigating Drug Exposure during Pregnancy and Associated Outcomes. Drug Saf. 2008, 31, 39–51. [Google Scholar] [CrossRef]
- Holmes, L.B. Setting Standards for Pregnancy Registries. Drug Saf. 2017, 41, 7–9. [Google Scholar] [CrossRef]
- US Food and Drug Administration (2018) Study Approaches and Methods to Evaluate the Safety of Drugs and Biological Products during Pregnancy in the Post-Approval Setting. Public Meeting, Request for Comments. Available online: https://www.fda.gov/Drugs/NewsEvents/ucm386560.htm (accessed on 23 December 2021).



{kind=link}
{kind=link}
| Demographics of Participants (N = 37) 1 | |
|---|---|
| Gender | |
| Female | 26 (70.3%) |
| Male | 11 (29.7%) |
| Highest educational level | |
| Bachelor | 2 (5.4%) |
| Master | 19 (51.4%) |
| PhD | 16 (43.2%) |
| Department of the current function | |
| Pharmacovigilance | 19 (51.4%) |
| Medical affairs | 6 (16.2%) |
| Epidemiology | 4 (10.8%) |
| Regulatory affairs | 2 (5.4%) |
| Other | 6 (16.2%) |
| Location current function | |
| Belgium | 15 (40.5%) |
| USA | 11 (29.7%) |
| Other European countries | 11 (29.7%) |
| Information on the organisations (N = 9) | |
| Departments in different countries | 7 (77.8%) |
| Location headquarters | |
| USA | 3 (33.3%) |
| Belgium | 2 (22.2%) |
| Switzerland | 2 (22.2%) |
| UK | 1 (11.1%) |
| Japan | 1 (11.1%) |
| Participation in IMI ConcePTION 2 | 5 (55.6%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sillis, L.; Foulon, V.; Verbakel, J.Y.; Ceulemans, M. Experiences and Perspectives of Marketing Authorisation Holders towards Medication Safety Monitoring during Pregnancy: A Pan-European Qualitative Analysis. Int. J. Environ. Res. Public Health 2022, 19, 4248. https://doi.org/10.3390/ijerph19074248
Sillis L, Foulon V, Verbakel JY, Ceulemans M. Experiences and Perspectives of Marketing Authorisation Holders towards Medication Safety Monitoring during Pregnancy: A Pan-European Qualitative Analysis. International Journal of Environmental Research and Public Health. 2022; 19(7):4248. https://doi.org/10.3390/ijerph19074248
Chicago/Turabian StyleSillis, Laure, Veerle Foulon, Jan Y. Verbakel, and Michael Ceulemans. 2022. "Experiences and Perspectives of Marketing Authorisation Holders towards Medication Safety Monitoring during Pregnancy: A Pan-European Qualitative Analysis" International Journal of Environmental Research and Public Health 19, no. 7: 4248. https://doi.org/10.3390/ijerph19074248
APA StyleSillis, L., Foulon, V., Verbakel, J. Y., & Ceulemans, M. (2022). Experiences and Perspectives of Marketing Authorisation Holders towards Medication Safety Monitoring during Pregnancy: A Pan-European Qualitative Analysis. International Journal of Environmental Research and Public Health, 19(7), 4248. https://doi.org/10.3390/ijerph19074248