
Health Literacy in Portugal: Results of the Health Literacy Population Survey Project 2019–2021


 ,
,  ,
,  , ,
, , 
Highlights
- The HLS19 shows good psychometric properties in a Portuguese sample.
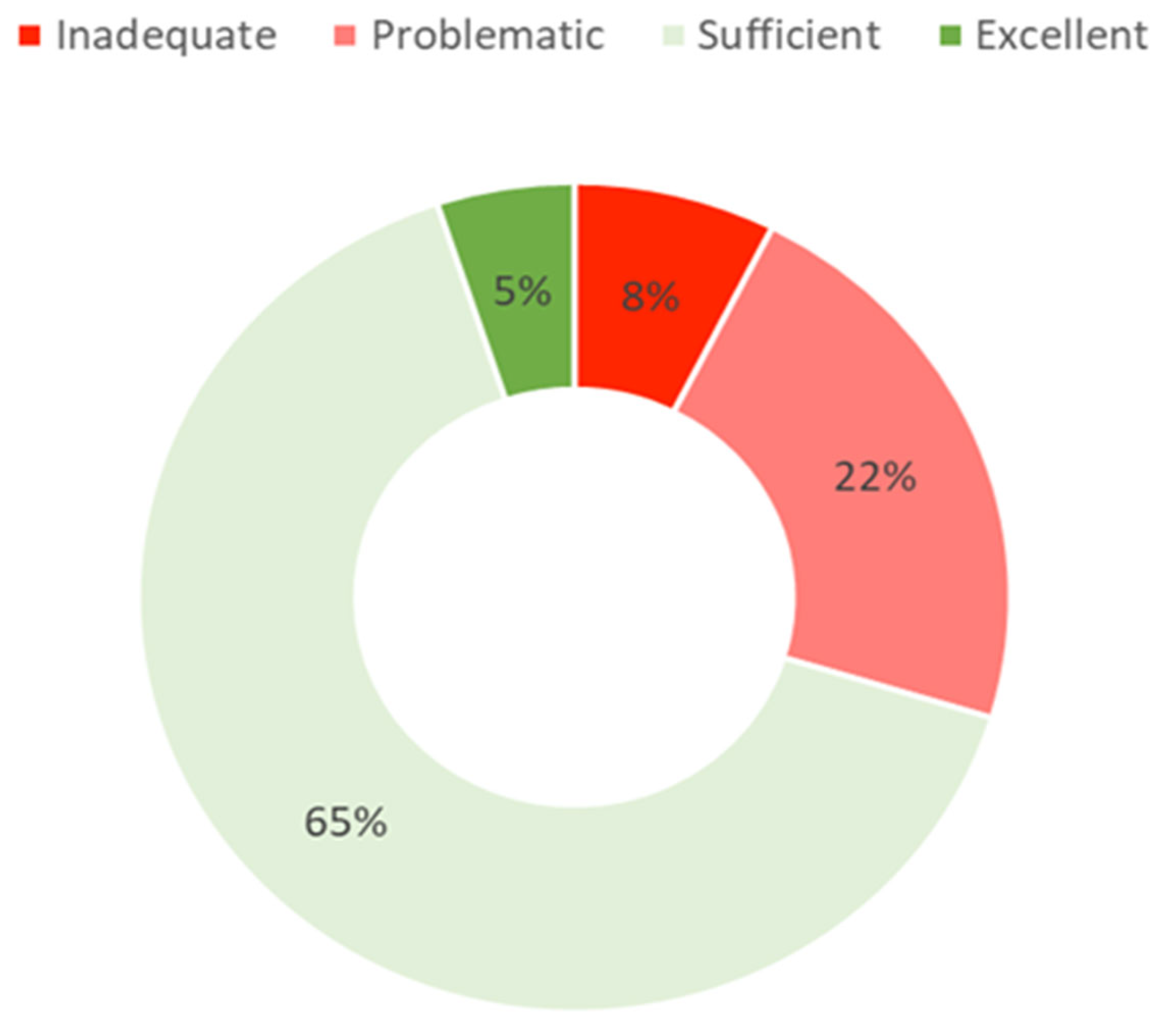
- Although most people (7 out of 10) showed high health literacy levels, these levels are dependent on the individual’s socioeconomic status.
- Vaccination health literacy revealed the highest health literacy level among specific health literacies.
- The HLS19 is a feasible measure to assess health literacy.
- There is a social gradient for health literacy which highlights the need for continuous and regular monitoring of health literacy at the population level.
- Contextual factors related to COVID-19 may have contributed to improving the population’s knowledge on vaccination.
Abstract
:1. Introduction
- translate and adapt HLS19 tools (HLS19-Q12 and three optional packages) for assessing personal health literacy in Portugal;
- explore psychometric characteristics of the Portuguese HLS19 Questionnaire (HLS19-Q12);
- establish health literacy levels in the Portuguese population;
- measure new topics on health literacy, specifically digital health literacy (HL-DIGI), navigational health literacy (HL-NAV), and vaccination health literacy (HL-VAC) in the Portuguese population;
- explore associations between health literacy levels and some health literacy correlates (determinants and consequences) in the Portuguese population.
2. Materials and Methods
3. Results
3.1. Descriptive Statistics
3.1.1. Correlate Items
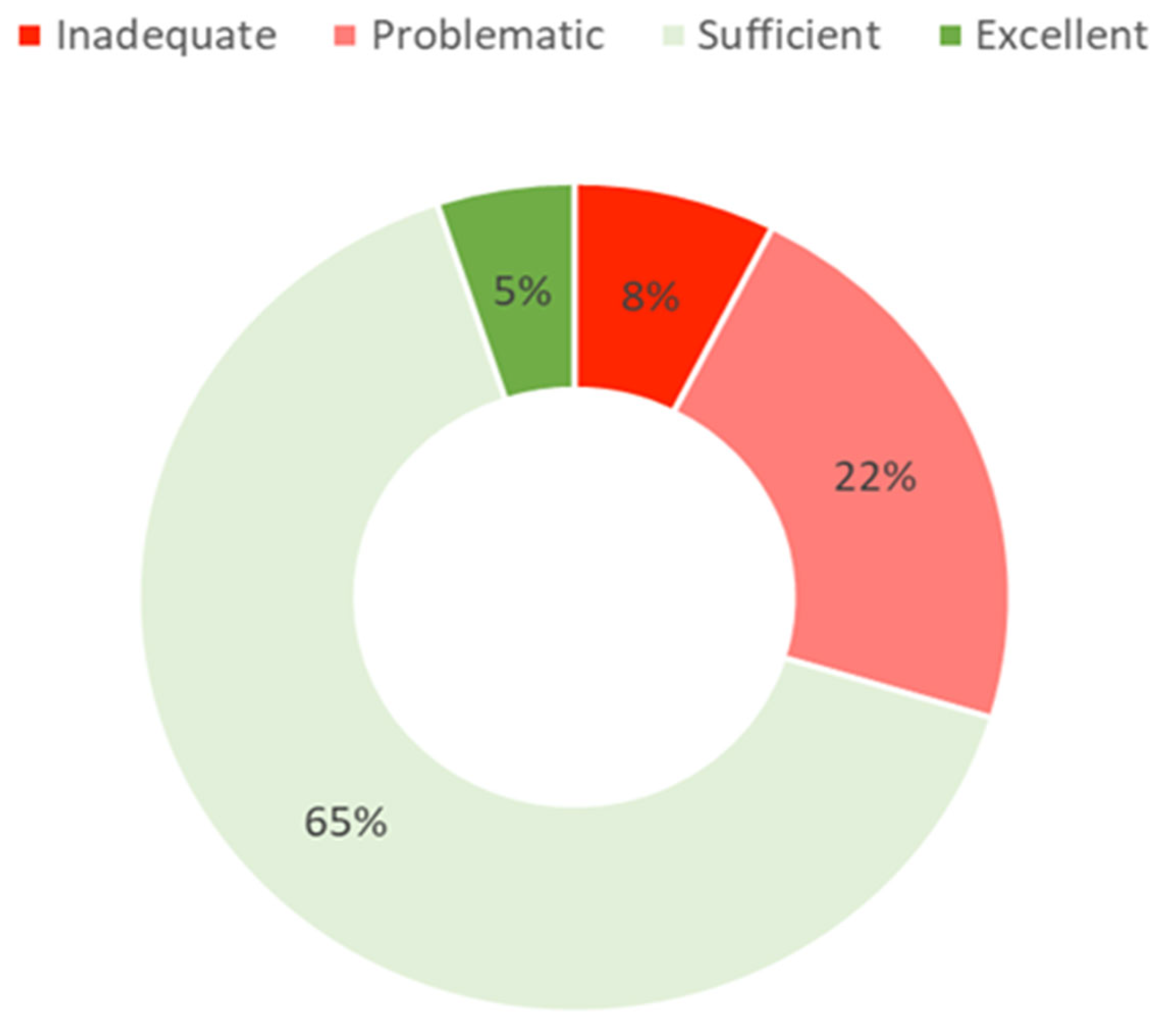
3.1.2. General Health Literacy
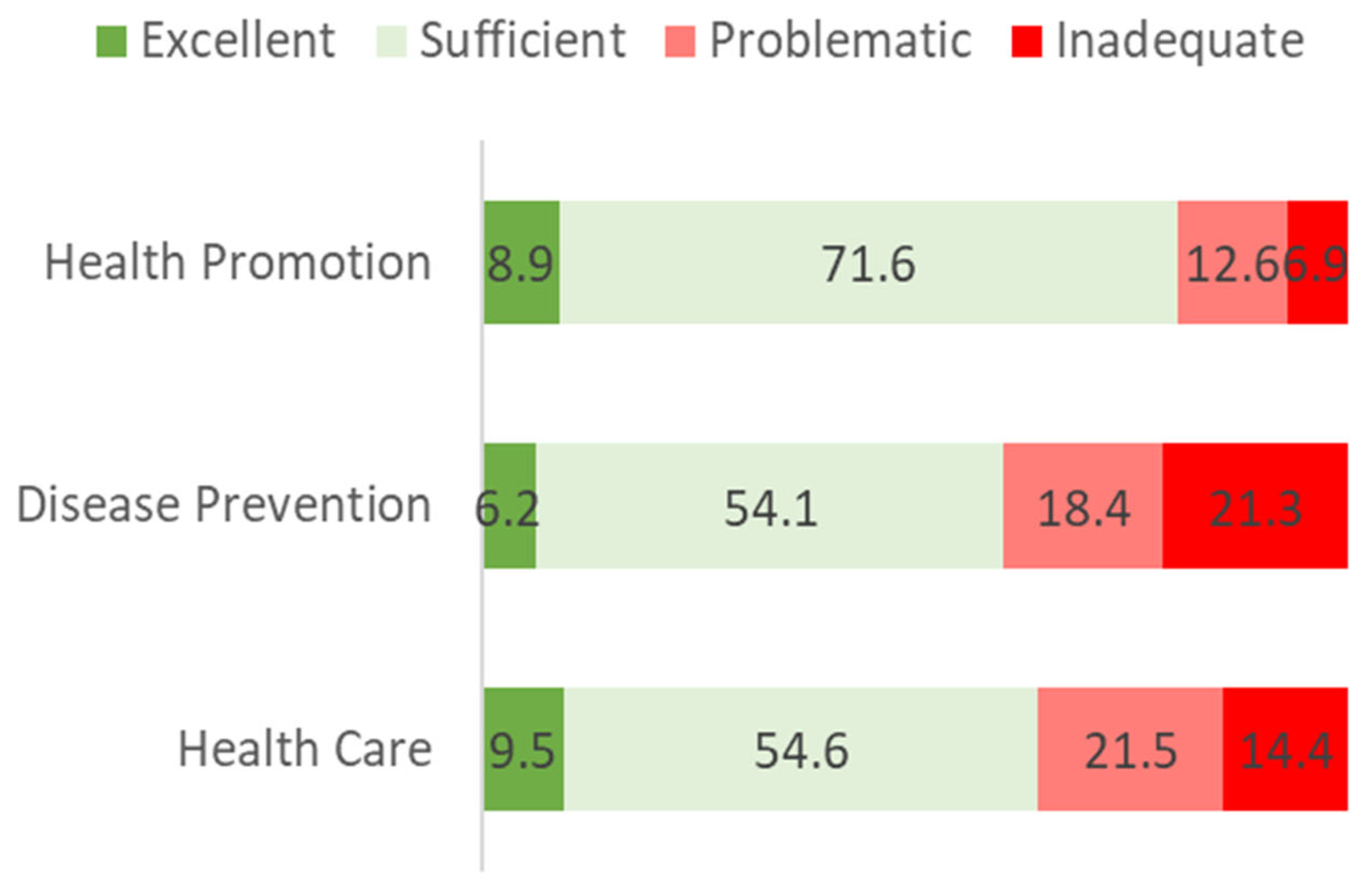
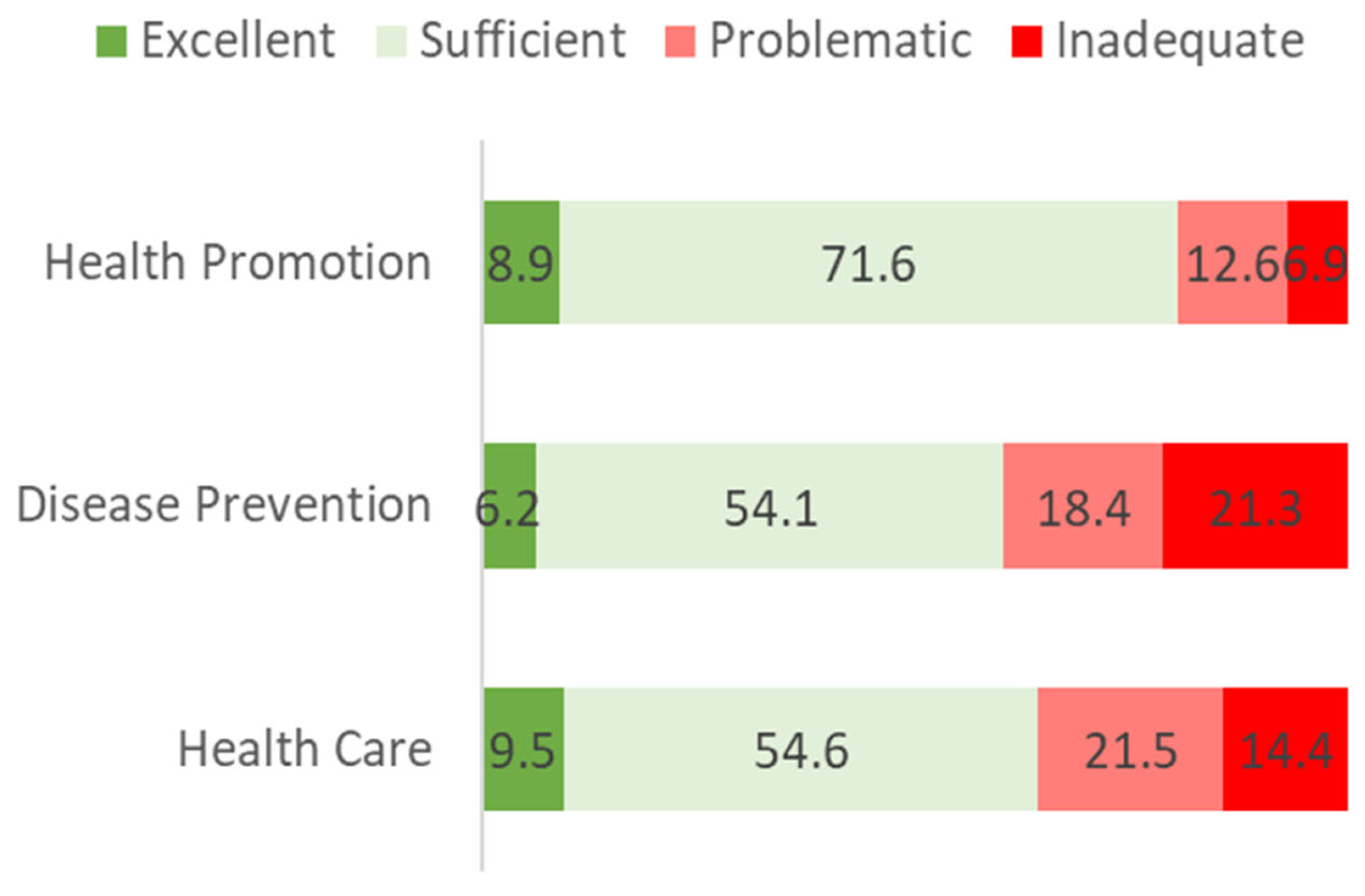
3.1.3. Dimensions of Health Literacy
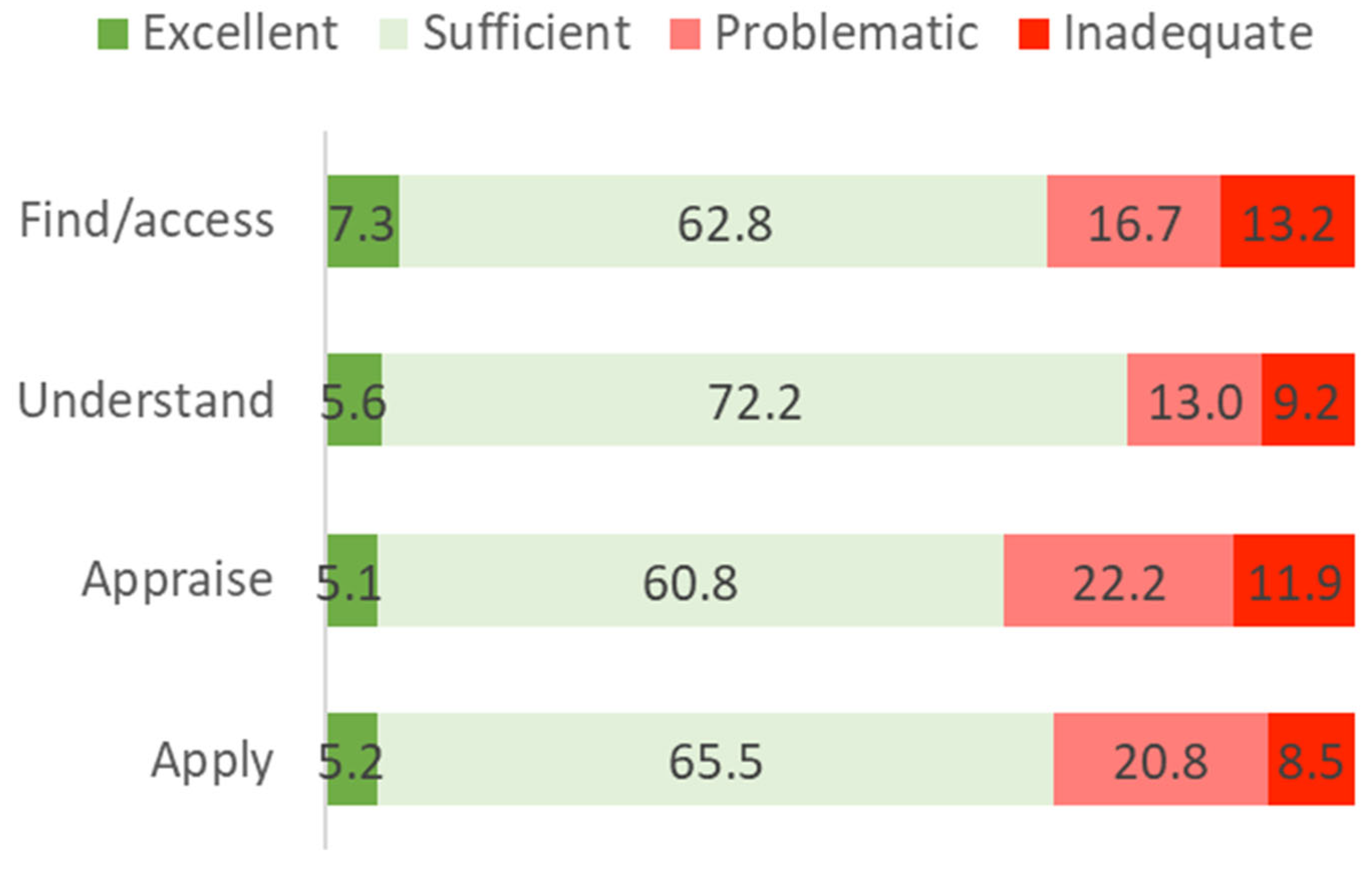
3.1.4. Processing Health-Related Information
3.1.5. Health Literacy Optional Packages
3.2. Inference Statistics
3.2.1. Determinants of Health Literacy
3.2.2. Correlations between HL, HL-DIGI, HL-NAV and HL-VAC
3.2.3. Internal Consistency for HLS19-Q12 and Optional Packages
3.3. Factorial Structure for HLS19-Q12
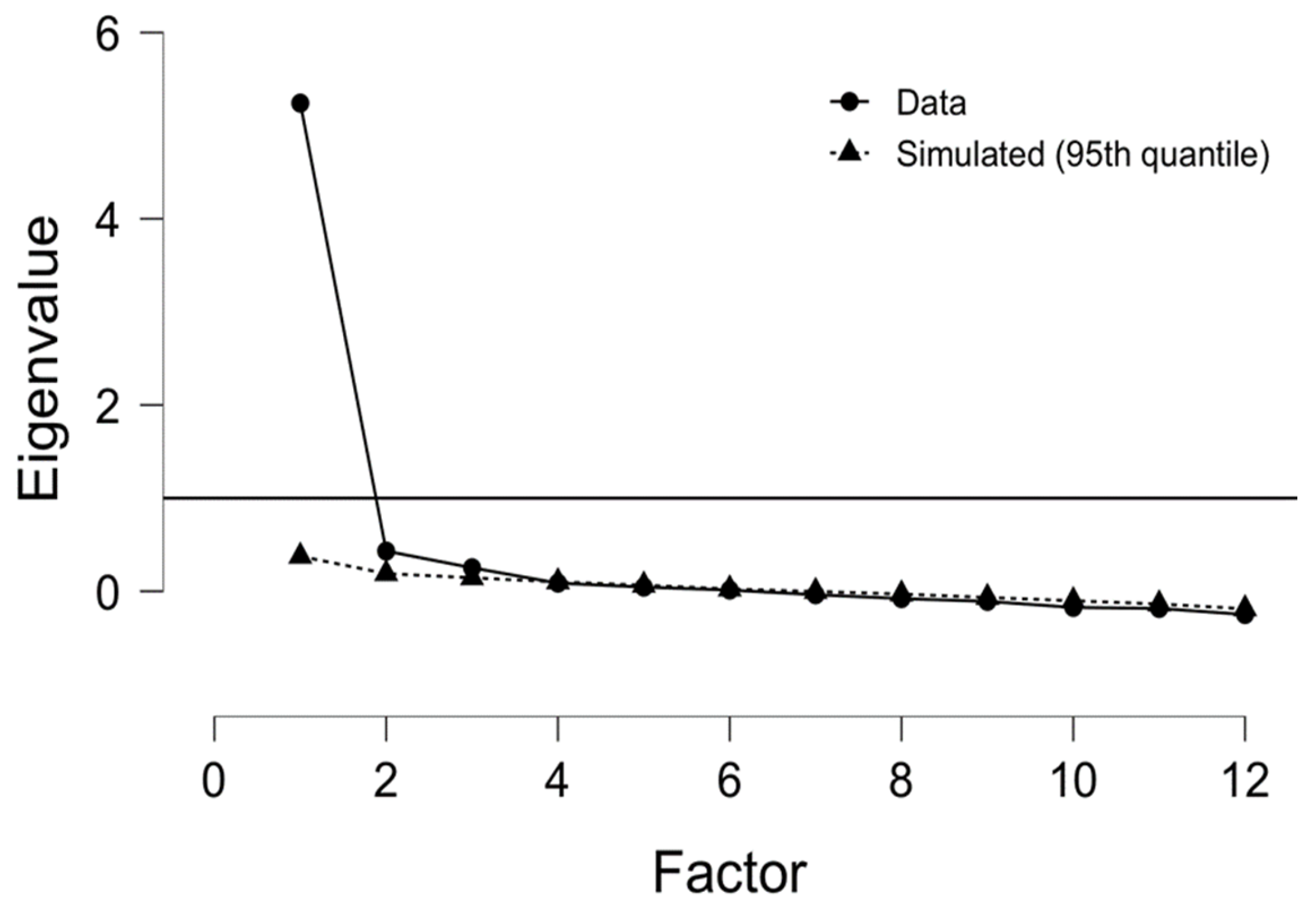
3.3.1. Exploratory Factor Analysis (EFA)
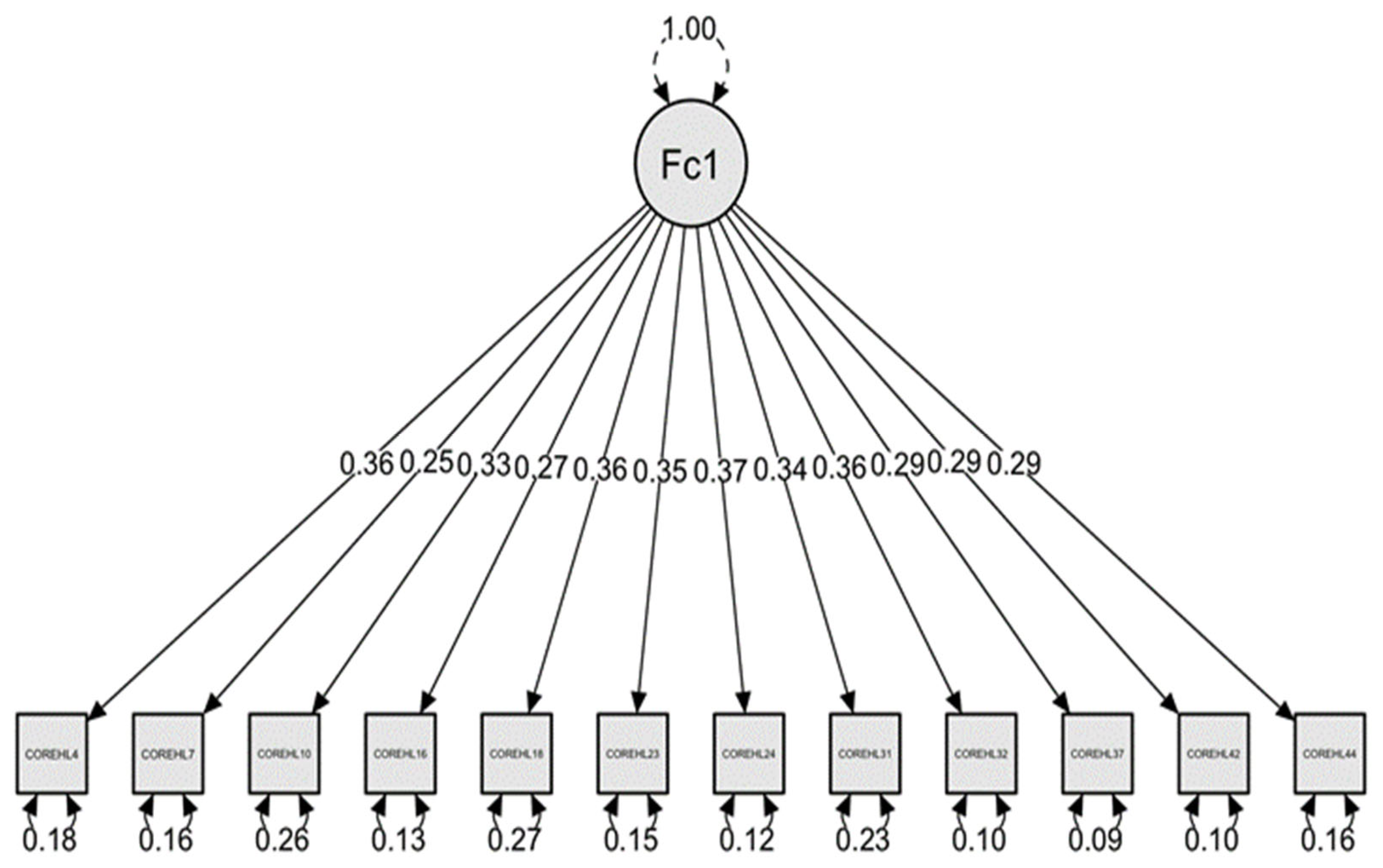
3.3.2. Confirmatory Factor Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| HL | General health literacy |
| HLS19-PT | Portuguese Health Literacy Population Survey Project 2019–2021 |
| HLS19-Q12 | 12-item version of the Health Literacy Survey from the Health Literacy Population Survey Project 2019–2021 |
| HLS19-Q16 | 16-item version of the Health Literacy Survey from the Health Literacy Population Survey Project 2019–2021 |
| HLS19-Q47 | 47-item version of the Health Literacy Survey from the Health Literacy Population Survey Project 2019–2021 |
| HLS-EU | European Health Literacy Survey |
| HLS-EU 2009–2012 | European Health Literacy Project |
| HLS-EU-Q47 | European Health Literacy Project 47-item Questionnaire |
| HLS-EU-Q86 | HLS-EU-Q47 supplemented with an additional section with 39 items referring to determinants and consequences used to conduct the first comparative European health literacy survey in 2011 |
| HL-DIGI | Digital health literacy |
| HL-NAV | Navigational health literacy |
| HL-VAC | Vaccination health literacy |
| HLS19-DIGI | Digital Health Literacy (instrument) |
| HLS19-NAV | Navigational Health Literacy (instrument) |
| HLS19-VAC | Vaccination Health Literacy (instrument) |
| ISCED | International Standard Classification of Education |
| M-POHL | Action Network on Measuring Population and Organizational Health Literacy |
| HLS19 | Health Literacy Population Survey Project 2019–2021 |
| EFA | Exploratory factor analysis |
| VIF | Variance Inflation Factor |
| CFA | Confirmatory Factor Analysis |
References
- Sørensen, K.; van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.M.; Slonska, Z.; Brand, H.; (HLS-EU) Consortium European Health Literacy Project. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sørensen, K.; van den Broucke, S.; Pelikan, J.M.; Fullam, J.; Doyle, G.; Slonska, Z.; Kondilis, B.; Stoffels, V.; Osborne, R.H.; Brand, H.; et al. Measuring health literacy in populations: Illuminating the design and development process of HLS-EU-Q. BMC Public Health 2013, 13, 948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sørensen, K.; Pelikan, J.M.; Röthlin, F.; Ganahl, K.; Slonska, Z.; Doyle, G.; Fullam, J.; Kondilis, B.; Agrafiotis, D.; Uiters, E.; et al. Health literacy in Europe: Comparative results of the European health literacy survey (HLS-EU). Eur. J. Public Health 2015, 25, 1053–1058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espanha, R.; Ávila, P. Health Literacy Survey Portugal: A Contribution for the Knowledge on Health and Communications. Procedia Comput. Sci 2016, 100, 1033–1041. [Google Scholar] [CrossRef] [Green Version]
- M-POHL Action Network. Available online: https://m-pohl.net/mpohl_action_network (accessed on 14 August 2021).
- Arriaga, M.T.; dos Santos, B.; Silva, A.; Mata, F.; Chaves, N.; Freitas, G. Plano de Ação Para a Literacia Em Saúde 2019–2021; Direção-Geral da Saúde: Lisboa, Portugal, 2018; Available online: https://www.dgs.pt/documentos-e-publicacoes/plano-de-acao-para-a-literacia-em-saude-2019-2021-pdf.aspx (accessed on 14 August 2021).
- Portugal. Ministério da Saúde. Direção-Geral da Saúde. Níveis de Literacia em Saúde—PORTUGAL, Lisboa: Direção-Geral da Saúde, 2021. Available online: https://www.dgs.pt/documentos-e-publicacoes/estudo-apresenta-nivel-de-literacia-em-saude-dos-portugueses-pdf.aspx (accessed on 3 March 2022).
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 6th ed.; Person Education: Boston, MA, USA, 2012. [Google Scholar]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 3rd ed.; Macmillan: New York, NY, USA, 1995. [Google Scholar]
- Nunnally, J.C.; Bernstein, I.H. Psychometric Theory; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- Finbråten, H.S.; Wilde-Larsson, B.; Nordström, G.; Pettersen, K.S.; Trollvik, A.; Guttersrud, Ø. Establishing the HLS-Q12 short version of the European Health Literacy Survey Questionnaire: Latent trait analyses applying Rasch modelling and confirmatory factor analysis. BMC Health Serv. Res. 2018, 18, 506. [Google Scholar] [CrossRef] [PubMed]
- Bentler, P.M. Comparative Fit Indexes in Structural Models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Kline, R.B. Principles and Practice of Structural Equation Modelling; Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Bröder, J.; Okan, O.; Bauer, U.; Bollweg, T.M.; Brulan, D.; Pinheiro, P. Child and youth health literacy: A conceptual analysis and proposed target-group-centred definition. Int. J. Environ. Res. Public Health 2019, 16, 3417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griese, L.; Berens, E.M.; Nowak, P.; Pelikan, J.M.; Schaeffer, D. Challenges in navigating the health care system: Development of an instrument measuring navigation health literacy. Int. J. Environ. Res. Public Health 2020, 17, 5731. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Health Literacy: The Solid Facts; WHO Regional Office for Europe: Copenhagen, Denmark, 2013; Available online: https://apps.who.int/iris/handle/10665/326432 (accessed on 14 August 2021).
- Kutner, M.; Greenberg, E.; Jin, Y.; Paulsen, C. The Health Literacy of America’s Adults: Results from the 2003 National Assessment of Adult Literacy (NCES 2006-483); National Center for Education Statistics: Washington, DC, USA, 2006. [Google Scholar]
- Moreira, L. Health Literacy for People-Centred Care: Where Do OECD Countries Stand? OECD Health Working Papers No. 107; OCED: Paris, France, 2018. [Google Scholar] [CrossRef]
- World Health Organization. Draft WHO European Roadmap for Implementation of Health Literacy Initiatives through the Life Course. Regional Committee for Europe (69th Session); WHO Regional Office for Europe: Copenhagen, Denmark, 2019; Available online: https://www.euro.who.int/__data/assets/pdf_file/0003/409125/69wd14e_Rev1_RoadmapOnHealthLiteracy_190323.pdf (accessed on 3 March 2022).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HLS19 Core | HLS19-Q12 | HL Measurement | HL Correlates |
|---|---|---|---|
| Short Version with 12 Items for Measuring General Health Literacy | Mandatory Correlates for General HL Measurement (31 Items) Such as Age, Education, Socioeconomic Status, etc. | ||
| Optional packages | Digital Health Literacy (HLS19-DIGI) | Sub-scale with 16 items for measuring digital health literacy | |
| Navigational Health Literacy (HLS19-NAV) | Sub-scale with 12 items for measuring navigational health literacy | ||
| Vaccination Health Literacy (HLS19-VAC) | Sub-scale with 14 items for measuring vaccination health literacy | ||
| Frequency (n) | % | |
|---|---|---|
| Gender | ||
| Male | 604 | 48.4 |
| Female | 643 | 51.6 |
| Formal education | ||
| No formal education or below ISCED 1 | 98 | 7.9 |
| ISCED 1 Primary education | 208 | 16.7 |
| ISCED 2 Lower secondary education | 199 | 16.0 |
| ISCED 3 Upper secondary education | 380 | 30.5 |
| ISCED 4 Post-secondary but non-tertiary education | 17 | 1.4 |
| ISCED 5 Short-cycle tertiary education | 19 | 1.5 |
| ISCED 6 Bachelor’s or equivalent level | 272 | 21.8 |
| ISCED 7 Master’s or equivalent level | 47 | 3.8 |
| ISCED 8 Doctoral or equivalent level | 7 | .6 |
| Employment status | ||
| Employed | 680 | 54.6 |
| Self-employed | 81 | 6.5 |
| Unemployed | 104 | 8.3 |
| Retired | 211 | 16.9 |
| Unable to work due to long-standing health problems | 10 | .8 |
| Student, trainee | 136 | 10.9 |
| Fulfilling domestic tasks | 21 | 1.7 |
| Compulsory military or civilian service | 3 | .2 |
| Pay all the expenses at the end of the month | ||
| Very easy | 40 | 3.2 |
| Easy | 667 | 53.5 |
| Difficult | 439 | 35.2 |
| Very difficult | 68 | 5.5 |
| Don’t know/Don’t answer | 33 | 2.6 |
| Afford medication if needed | ||
| Very easy | 87 | 7.0 |
| Easy | 809 | 64.9 |
| Difficult | 266 | 21.3 |
| Very difficult | 28 | 2.2 |
| Don’t know/Don’t answer | 57 | 4.6 |
| Afford medical examination if needed | ||
| Very easy | 75 | 6.0 |
| Easy | 770 | 61.7 |
| Difficult | 310 | 24.9 |
| Very difficult | 32 | 2.6 |
| Don’t know/Don’t answer | 60 | 4.8 |
| Factor 1 | |
|---|---|
| COREHL 4 | 0.587 |
| COREHL 7 | 0.599 |
| COREHL 10 | 0.601 |
| COREHL 16 | 0.544 |
| COREHL 18 | 0.672 |
| COREHL 23 | 0.684 |
| COREHL 24 | 0.749 |
| COREHL 31 | 0.635 |
| COREHL 32 | 0.791 |
| COREHL 37 | 0.699 |
| COREHL 42 | 0.720 |
| COREHL 44 | 0.605 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arriaga, M.; Francisco, R.; Nogueira, P.; Oliveira, J.; Silva, C.; Câmara, G.; Sørensen, K.; Dietscher, C.; Costa, A. Health Literacy in Portugal: Results of the Health Literacy Population Survey Project 2019–2021. Int. J. Environ. Res. Public Health 2022, 19, 4225. https://doi.org/10.3390/ijerph19074225
Arriaga M, Francisco R, Nogueira P, Oliveira J, Silva C, Câmara G, Sørensen K, Dietscher C, Costa A. Health Literacy in Portugal: Results of the Health Literacy Population Survey Project 2019–2021. International Journal of Environmental Research and Public Health. 2022; 19(7):4225. https://doi.org/10.3390/ijerph19074225
Chicago/Turabian StyleArriaga, Miguel, Rita Francisco, Paulo Nogueira, Jorge Oliveira, Carlota Silva, Gisele Câmara, Kristine Sørensen, Christina Dietscher, and Andreia Costa. 2022. "Health Literacy in Portugal: Results of the Health Literacy Population Survey Project 2019–2021" International Journal of Environmental Research and Public Health 19, no. 7: 4225. https://doi.org/10.3390/ijerph19074225
APA StyleArriaga, M., Francisco, R., Nogueira, P., Oliveira, J., Silva, C., Câmara, G., Sørensen, K., Dietscher, C., & Costa, A. (2022). Health Literacy in Portugal: Results of the Health Literacy Population Survey Project 2019–2021. International Journal of Environmental Research and Public Health, 19(7), 4225. https://doi.org/10.3390/ijerph19074225