
Expert Consensus on a Proposed Study Framework to Explore Factors Influencing Plasmodium knowlesi Malaria Preventive Behavior: A Modified Delphi Method Protocol

 , , , and
, , , and 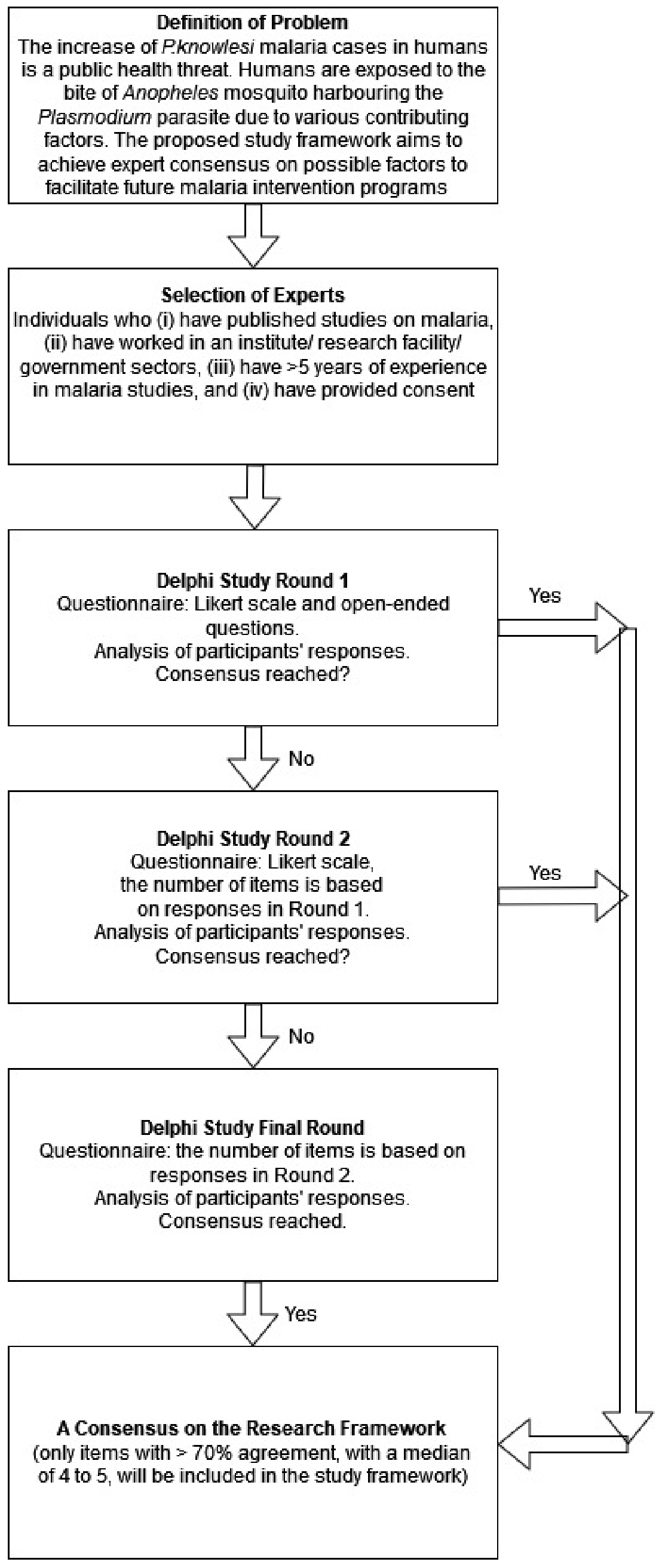{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods and Analysis
2.1. Study Aim
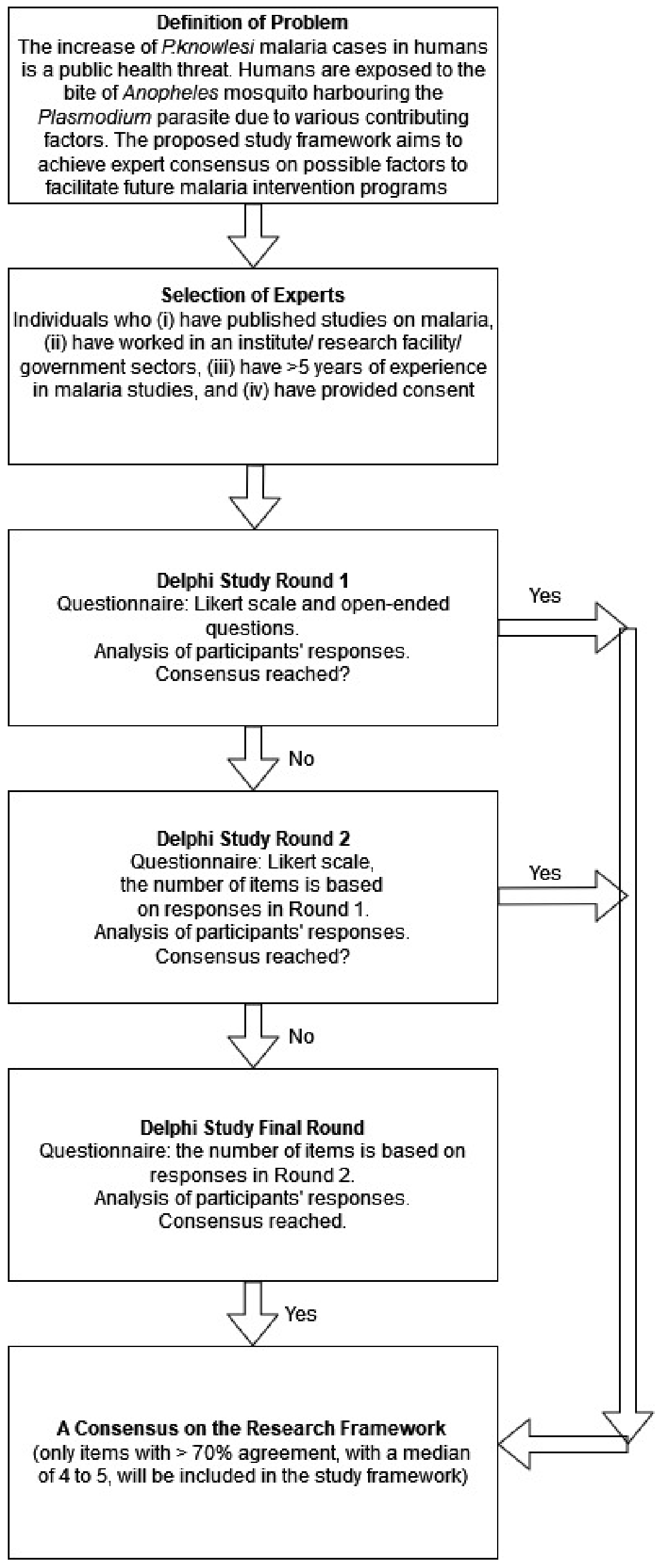
2.2. Procedure
2.3. First Step: The Problem Statement
2.4. Second Step: The Selection of Experts
2.5. Third Step: Round 1 of the Study
2.5.1. Questionnaire Validation
2.5.2. Pilot Study
2.5.3. Round 1
2.6. Fourth Step: Round 2 of the Study
2.7. Final Step: Round 3
2.8. Current Status
2.9. Patient and Public Involvement
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dalkey, N. An experimental study of group opinion. Futures 1969, 1, 408–426. [Google Scholar] [CrossRef]
- Powell, C. The Delphi technique: Myths and realities. J. Adv. Nurs. 2003, 41, 376–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Habibi, A.; Sarafrazi, A.; Izadyar, S. Delphi technique theoretical framework in qualitative research. Int. J. Eng. Sci. 2014, 3, 8–13. [Google Scholar]
- Hsu, C.-C.; Sandford, B.A. The Delphi technique: Making sense of consensus. Pract. Assess. Res. Eval. 2007, 12, 1–8. [Google Scholar] [CrossRef]
- Keeney, S.; Hasson, F.; McKenna, H. Consulting the oracle: Ten lessons from using the Delphi technique in nursing research. J. Adv. Nurs. 2006, 53, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Okoli, C.; Pawlowski, S.D. The Delphi method as a research tool: An example, design considerations and applications. Inf. Manag. 2004, 42, 15–29. [Google Scholar] [CrossRef] [Green Version]
- Rajhans, V.; Rege, S.; Memon, U.; Shinde, A. Adopting a modified Delphi technique for revisiting the curriculum: A useful approach during the COVID-19 pandemic. Qual. Res. J. 2020, 20, 373–382. [Google Scholar] [CrossRef]
- Mahajan, V.; Linstone, H.A.; Turoff, M. The Delphi Method: Techniques and Applications. J. Mark. Res. 2002, 13, 317. [Google Scholar] [CrossRef]
- Humphrey-Murto, S.; Varpio, L.; Gonsalves, C.; Wood, T.J. Using consensus group methods such as Delphi and Nominal Group in medical education research. Med. Teach. 2017, 39, 14–19. [Google Scholar] [CrossRef]
- Hasson, F.; Keeney, S. Enhancing rigour in the Delphi technique research. Technol. Forecast. Soc. Chang. 2011, 78, 1695–1704. [Google Scholar] [CrossRef]
- Boulkedid, R.; Abdoul, H.; Loustau, M.; Sibony, O.; Alberti, C. Using and Reporting the Delphi Method for Selecting Healthcare Quality Indicators: A Systematic Review. PLoS ONE 2011, 6, e20476. [Google Scholar] [CrossRef]
- Sekayi, D.; Kennedy, A. Qualitative Delphi Method: A Four Round Process with a Worked Example. Qual. Rep. 2017, 22, 2755–2763. [Google Scholar] [CrossRef]
- Slade, S.C.; Dionne, C.E.; Underwood, M.; Buchbinder, R. Standardised method for reporting exercise programmes: Protocol for a modified Delphi study. BMJ Open 2014, 4, e006682. [Google Scholar] [CrossRef] [Green Version]
- Vogel, C.; Zwolinsky, S.; Griffiths, C.; Hobbs, M.; Henderson, E.; Wilkins, E. A Delphi study to build consensus on the definition and use of big data in obesity research. Int. J. Obes. 2019, 43, 2573–2586. [Google Scholar] [CrossRef] [Green Version]
- Fink-Hafner, D.; Dagen, T.; Doušak, M.; Novak, M. Delphi method: Strengths and weaknesses. Adv. Methodol. Stat. 2019, 16, 1–19. Available online: https://www.researchgate.net/publication/337570516 (accessed on 30 July 2021). [CrossRef]
- Gallotta, B.; Garza-Reyes, J.A.; Anosike, A. Using the Delphi method to verify a framework to implement sustainability ini-tiatives. In Proceedings of the International Conference on Industrial Engineering and Operations Management, Bandung, Indonesia, 6–8 March 2018; Volume 2018, pp. 231–4115. [Google Scholar]
- Niederberger, M.; Spranger, J. Delphi Technique in Health Sciences: A Map. Front. Public Health 2020, 8, 457. [Google Scholar] [CrossRef]
- Yam, C.H.K.; Wong, E.L.Y.; Cheung, A.W.L.; Chan, F.W.K.; Wong, F.Y.Y.; Yeoh, E.-K. Framework and components for effective discharge planning system: A delphi methodology. BMC Health Serv. Res. 2012, 12, 396. [Google Scholar] [CrossRef] [Green Version]
- Culley, J.M. Use of a Computer-Mediated Delphi Process to Validate a Mass Casualty Conceptual Model. Comput. Inform. Nurs. 2011, 29, 272–279. [Google Scholar] [CrossRef] [Green Version]
- SPSS. Statistics. IBM. Available online: https://www.ibm.com/products/spss-statistics (accessed on 27 August 2021).
- Al Juffali, L.A.; Knapp, P.; Al-Aqeel, S.; Watson, M.C. Medication safety problems priorities in community pharmacy in Saudi Arabia: A multi-stakeholder Delphi study using the human factors framework. BMJ Open 2019, 9, e032419. [Google Scholar] [CrossRef]
- Cole, Z.D.; Donohoe, H.M.; Stellefson, M.L. Internet-Based Delphi Research: Case Based Discussion. Environ. Manag. 2013, 51, 511–523. [Google Scholar] [CrossRef]
- Lange, T.; Kopkow, C.; Lützner, J.; Günther, K.-P.; Gravius, S.; Scharf, H.-P.; Stöve, J.; Wagner, R.; Schmitt, J. Comparison of different rating scales for the use in Delphi studies: Different scales lead to different consensus and show different test-retest reliability. BMC Med Res. Methodol. 2020, 20, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Health Communication Capacity Collaborative. Ideation—An HC3 Research Primer: Ideational Model of Communication; IBM: Armonk, NY, USA, 2006; Published Online First; Available online: http://www.healthcommcapacity.org/wp-content/uploads/2015/02/Ideation.pdf (accessed on 27 August 2021).
- Kleinman, A. Concepts and a model for the comparison of medical systems as cultural systems. Soc. Sci. Med. Part B Med Anthr. 1978, 12, 85–93. [Google Scholar] [CrossRef]
- Murdock, G.P.; Wilson, S.F.; Frederick, V. World Distribution of Theories of Illness. Ethnology 1978, 17, 449. [Google Scholar] [CrossRef]
- Verhagen, A.P.; de Vet, H.C.; de Bie, R.A.; Kessels, A.G.; Boers, M.; Bouter, L.M.; Knipschild, P.G. The Delphi List: A Criteria List for Quality Assessment of Randomized Clinical Trials for Conducting Systematic Reviews Developed by Delphi Consensus. J. Clin. Epidemiol. 1998, 51, 1235–1241. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. World Malaria Report: 20 Years of Global Progress and Challenges; World Health Organization: Geneva, Switzerland, 2020; Licence: CC BY-NC-SA 3.0 IGO. [Google Scholar]
- Abeyasinghe, R. Outcomes from the Evidence Review Group on Plasmodium Knowlesi. 2017. Available online: https://www.who.int/malaria/mpac/mpac-mar2017-plasmodium-knowlesi-presentation.pdf (accessed on 30 August 2020).
- World Health Organization (WHO), WHO Malaria Policy Advisory Group. (MPAG) Meeting. 2021. Available online: https://www.who.int/groups/malaria-policy-advisory-group (accessed on 27 August 2021).
- Cooper, D.J.; Rajahram, G.S.; William, T.; Jelip, J.; Mohammad, R.; Benedict, J.; A Alaza, D.; Malacova, E.; Yeo, T.W.; Grigg, M.J.; et al. Plasmodium knowlesi Malaria in Sabah, Malaysia, 2015–2017: Ongoing Increase in Incidence Despite Near-elimination of the Human-only Plasmodium Species. Clin. Infect. Dis. 2020, 70, 361–367. [Google Scholar] [CrossRef] [Green Version]
- Grigg, M.J.; Cox, J.; William, T.; Jelip, J.; Fornace, K.M.; Brock, P.M.; von Seidlein, L.; Barber, B.E.; Anstey, N.M.; Yeo, T.W.; et al. Individual-level factors associated with the risk of acquiring human Plasmodium knowlesi malaria in Malaysia: A case-control study. Lancet Planet. Health 2017, 1, e97–e104. [Google Scholar] [CrossRef]
- Shearer, F.M.; Huang, Z.; Weiss, D.J.; Wiebe, A.; Gibson, H.; Battle, K.; Pigott, D.M.; Brady, O.J.; Putaporntip, C.; Jongwutiwes, S.; et al. Estimating Geographical Variation in the Risk of Zoonotic Plasmodium knowlesi Infection in Countries Eliminating Malaria. PLOS Negl. Trop. Dis. 2016, 10, e0004915. [Google Scholar] [CrossRef]
- Eede, P.V.D.; Van, H.N.; Van Overmeir, C.; Vythilingam, I.; Duc, T.N.; Hung, L.X.; Manh, H.N.; Annette, E.; D’Alessandro, U.; Erhart, A. Human Plasmodium knowlesi infections in young children in central Vietnam. Malar. J. 2009, 8, 249. [Google Scholar] [CrossRef] [Green Version]
- Fornace, K.M.; Nuin, N.A.; Betson, M.; Grigg, M.J.; William, T.; Anstey, N.M.; Yeo, T.W.; Cox, J.; Ying, L.T.; Drakeley, C.J. Asymptomatic and Submicroscopic Carriage ofPlasmodium knowlesiMalaria in Household and Community Members of Clinical Cases in Sabah, Malaysia. J. Infect. Dis. 2016, 213, 784–787. [Google Scholar] [CrossRef] [Green Version]
- Loy, D.E.; Plenderleith, L.J.; Sundararaman, S.A.; Liu, W.; Gruszczyk, J.; Chen, Y.-J.; Trimboli, S.; Learn, G.H.; MacLean, O.A.; Morgan, A.L.K.; et al. Evolutionary history of human Plasmodium vivax revealed by genome-wide analyses of related ape parasites. Proc. Natl. Acad. Sci. USA 2018, 115, E8450–E8459. [Google Scholar] [CrossRef] [Green Version]
- Barber, B.E.; Rajahram, G.S.; Grigg, M.J.; William, T.; Anstey, N.M. World Malaria Report: Time to acknowledge Plasmodium knowlesi malaria. Malar. J. 2017, 16, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figueroa, M.E. A Theory-Based Socioecological Model of Communication and Behavior for the Containment of the Ebola Epidemic in Liberia. J. Health Commun. 2017, 22, 5–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krenn, S.; Cobb, L.; Babalola, S.; Odeku, M.; Kusemiju, B. Using behavior change communication to lead a comprehensive family planning program: The Nigerian Urban Reproductive Health Initiative. Glob. Health Sci. Pract. 2014, 2, 427–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haynes, S.N.; Richard, D.C.S.; Kubany, E.S. Content validity in psychological assessment: A functional approach to concepts and methods. Psychol. Assess. 1995, 7, 238–247. [Google Scholar] [CrossRef]
- Clibbens, N.; Walters, S.; Baird, W. Delphi research: Issues raised by a pilot study. Nurse Res. 2012, 19, 37–44. [Google Scholar] [CrossRef]
- World Health Organization. Multisectoral Approach to the Prevention and Control of Vector-Borne Diseases. 2020. Available online: https://apps.who.int/iris/handle/10665/331861 (accessed on 20 August 2021).
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naserrudin, N.A.; Hod, R.; Jeffree, M.S.; Ahmed, K.; Hassan, M.R. Expert Consensus on a Proposed Study Framework to Explore Factors Influencing Plasmodium knowlesi Malaria Preventive Behavior: A Modified Delphi Method Protocol. Int. J. Environ. Res. Public Health 2022, 19, 4141. https://doi.org/10.3390/ijerph19074141
Naserrudin NA, Hod R, Jeffree MS, Ahmed K, Hassan MR. Expert Consensus on a Proposed Study Framework to Explore Factors Influencing Plasmodium knowlesi Malaria Preventive Behavior: A Modified Delphi Method Protocol. International Journal of Environmental Research and Public Health. 2022; 19(7):4141. https://doi.org/10.3390/ijerph19074141
Chicago/Turabian StyleNaserrudin, Nurul Athirah, Rozita Hod, Mohammad Saffree Jeffree, Kamruddin Ahmed, and Mohd Rohaizat Hassan. 2022. "Expert Consensus on a Proposed Study Framework to Explore Factors Influencing Plasmodium knowlesi Malaria Preventive Behavior: A Modified Delphi Method Protocol" International Journal of Environmental Research and Public Health 19, no. 7: 4141. https://doi.org/10.3390/ijerph19074141
APA StyleNaserrudin, N. A., Hod, R., Jeffree, M. S., Ahmed, K., & Hassan, M. R. (2022). Expert Consensus on a Proposed Study Framework to Explore Factors Influencing Plasmodium knowlesi Malaria Preventive Behavior: A Modified Delphi Method Protocol. International Journal of Environmental Research and Public Health, 19(7), 4141. https://doi.org/10.3390/ijerph19074141