
Enhancement of Skill Competencies in Operative Dentistry Using Procedure-Specific Educational Videos (E-Learning Tools) Post-COVID-19 Era—A Randomized Controlled Trial

 , ,
, ,  ,
,  ,
,
Abstract
:1. Introduction
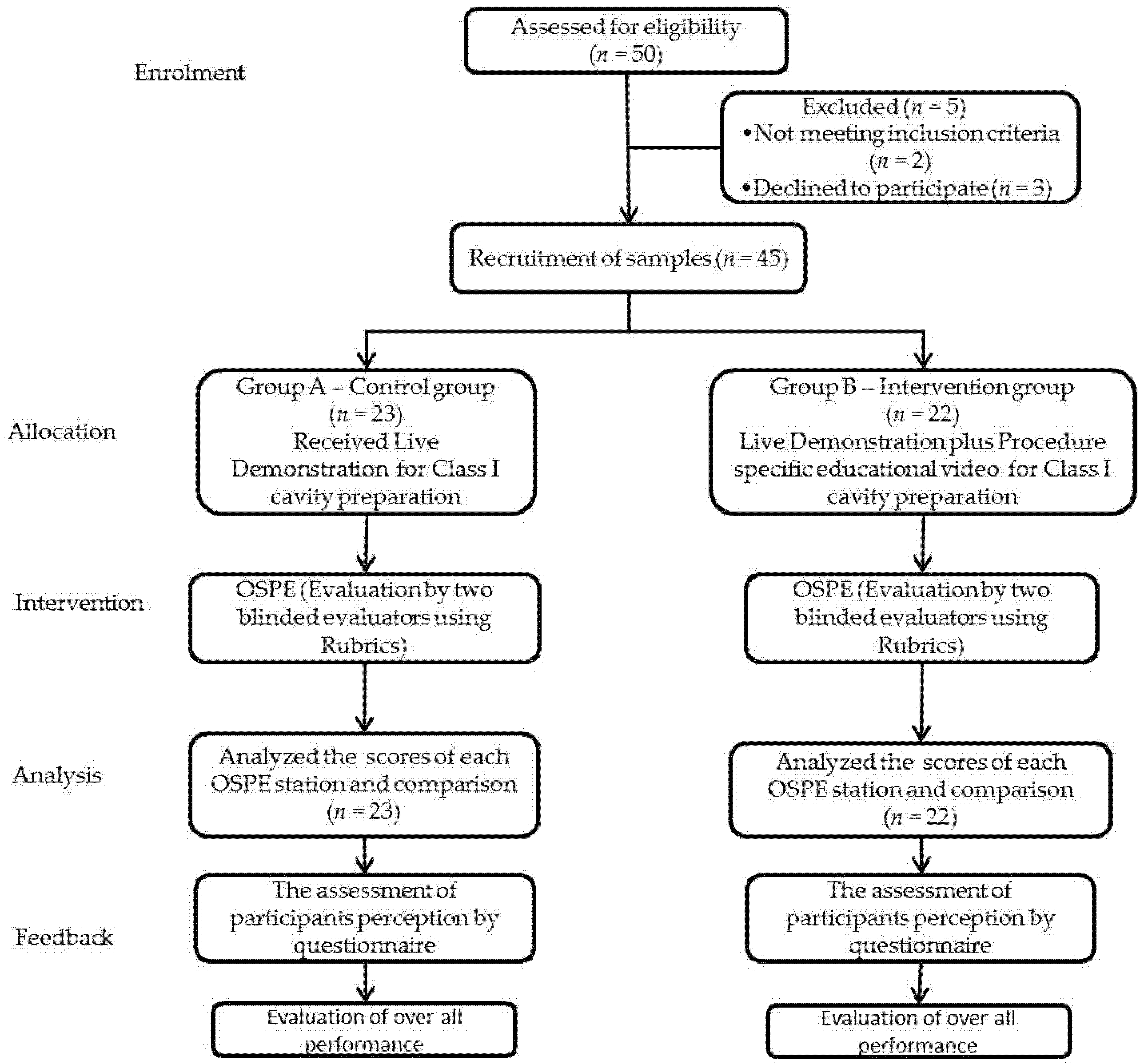
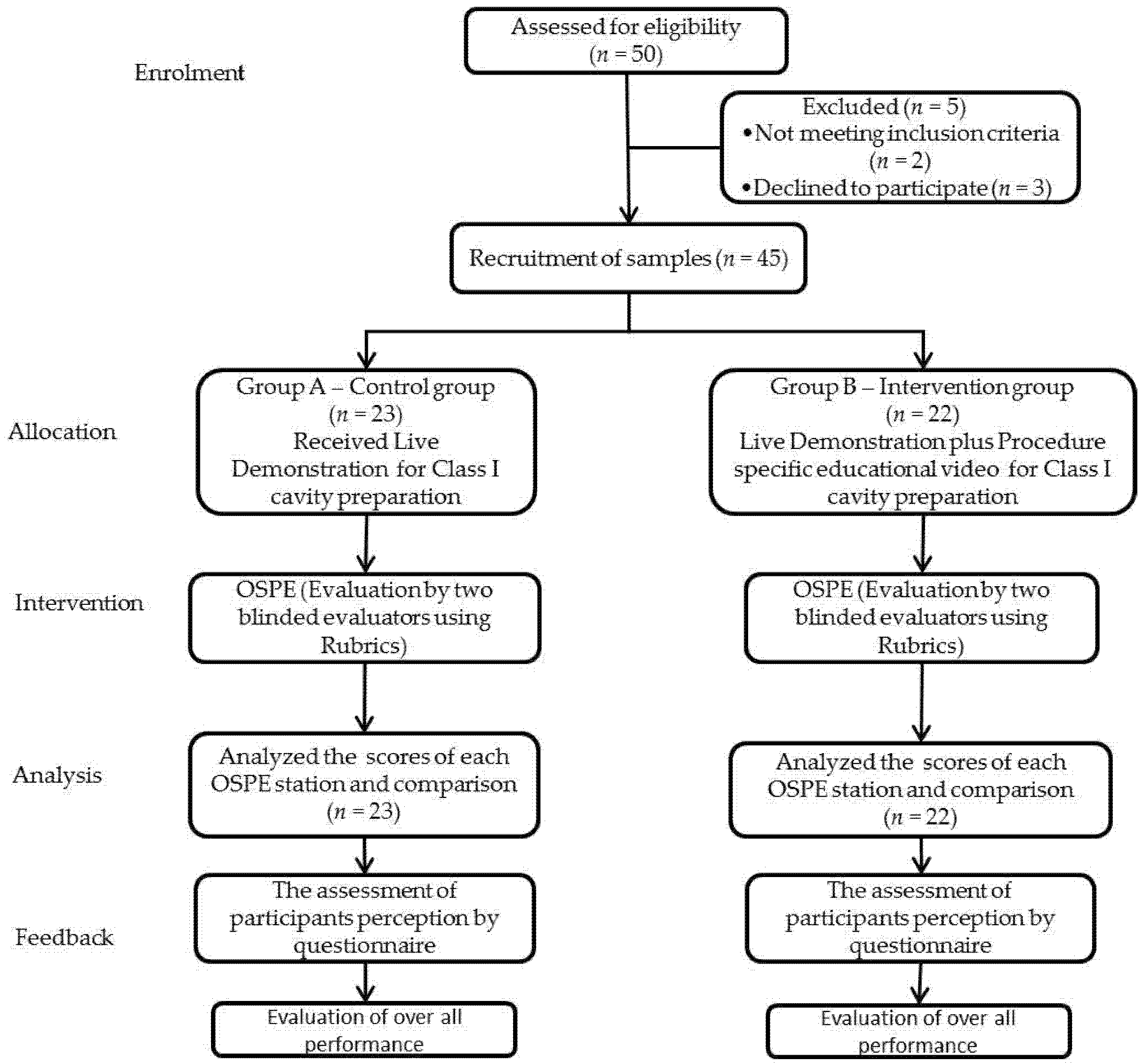
2. Methods
Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sahu, P.K.; Chattu, V.K.; Rewatkar, A.; Sakhamuri, S. Best practices to impart clinical skills during preclinical years of medical curriculum. J. Educ. Health Promot. 2019, 8, 57–64. [Google Scholar] [PubMed]
- Kalaskar, R.R.; Kalaskar, A.R. Effectiveness of 3D video system on the performance of students during preclinical Cavity preparation exercise. J. Educ. Technol. Health Sci. 2015, 2, 57–61. [Google Scholar]
- Alqahtani, N.D.; Al-Jewair, T.; Khalid, A.-M.; Albarakati, S.F.; ALkofide, E.A. Live demonstration versus procedural video: A comparison of two methods for teaching an orthodontic laboratory procedure. BMC Med. Educ. 2015, 15, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Karimi Moonaghi, H.; Derakhshan, A.; Valai, N.; Mortazavi, F. The effectiveness of video-based education on gaining practical learning skills in comparison with demonstrating methods effectiveness among university students. J. Med. Educ. 2003, 4, 27–30. [Google Scholar]
- Buchanan, J.A. Use of simulation technology in dental education. J. Dent. Educ. 2001, 65, 1225–1231. [Google Scholar] [CrossRef]
- Bhola, S.; Hellyer, P. The risks and benefits of social media in dental foundation training. Br. Dent. J. 2016, 221, 609–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naser-Ud-Din, S. Introducing scenario based learning interactive to postgraduates in UQ Orthodontic Program. Eur. J. Dent. Educ. 2015, 19, 169–176. [Google Scholar] [CrossRef]
- Hillenburg, K.; Cederberg, R.; Gray, S.; Hurst, C.; Johnson, G.; Potter, B. E-learning and the future of dental education: Opinions of administrators and information technology specialists. Eur. J. Dent. Educ. 2006, 10, 169–177. [Google Scholar] [CrossRef]
- Cook, D.A.; Erwin, P.J.; Triola, M.M. Computerized virtual patients in health professions education: A systematic review and meta-analysis. Acad. Med. 2010, 85, 1589–1602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hempel, G.; Neef, M.; Rotzoll, D.; Heinke, W. Study of medicine 2.0 due to Web 2.0?!-risks and opportunities for the curriculum in Leipzig. GMS Z. Med. Ausbild. 2013, 30, 10–17. [Google Scholar]
- Jarczewski, A.; Balzer, F.; Stötzner, P.; Ahlers, O. GMS Journal for Medical Education. GMS Z. Med. Ausbild. 2013, 30, 1. [Google Scholar]
- Mahmoodi, B.; Sagheb, K.; Sagheb, K.; Schulz, P.; Willershausen, B.; Al-Nawas, B.; Walter, C. Catalogue of interactive learning objectives to improve an integrated medical and dental curriculum. J. Contemp. Dent. Pract. 2016, 17, 965–968. [Google Scholar] [CrossRef] [PubMed]
- Modha, B. Experiential learning without prior vicarious learning: An insight from the primary dental care setting. Educ. Prim. Care 2021, 32, 49–55. [Google Scholar] [CrossRef] [PubMed]
- AlKarani, A.S.; Thobaity, A.A. Medical Staff Members’ Experiences with Blackboard at Taif University, Saudi Arabia. J. Multidiscip. Healthc. 2020, 13, 1629. [Google Scholar] [CrossRef]
- Ramlogan, S.; Raman, V.; Sweet, J. A comparison of two forms of teaching instruction: Video vs. live lecture for education in clinical periodontology. Eur. J. Dent. Educ. 2014, 18, 31–38. [Google Scholar] [CrossRef]
- Zitzmann, N.U.; Matthisson, L.; Ohla, H.; Joda, T. Digital undergraduate education in dentistry: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 3269. [Google Scholar] [CrossRef] [PubMed]
- Khalaf, K.; El-Kishawi, M.; Mustafa, S.; Al Kawas, S. Effectiveness of technology-enhanced teaching and assessment methods of undergraduate preclinical dental skills: A systematic review of randomized controlled clinical trials. BMC Med. Educ. 2020, 20, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Thilakumara, I.P.; Jayasinghe, R.M.; Rasnayaka, S.K.; Jayasinghe, V.P.; Abeysundara, S. Effectiveness of procedural video versus live demonstrations in teaching laboratory techniques to dental students. J. Dent. Educ. 2018, 82, 898–904. [Google Scholar] [CrossRef] [Green Version]
- Wong, G.; Apthorpe, H.C.; Ruiz, K.; Nanayakkara, S. An innovative educational approach in using instructional videos to teach dental local anaesthetic skills. Eur. J. Dent. Educ. 2019, 23, 28–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soltanimehr, E.; Bahrampour, E.; Imani, M.M.; Rahimi, F.; Almasi, B.; Moattari, M. Effect of virtual versus traditional education on theoretical knowledge and reporting skills of dental students in radiographic interpretation of bony lesions of the jaw. BMC Med. Educ. 2019, 19, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botelho, M.; Gao, X.; Jagannathan, N. A qualitative analysis of students’ perceptions of videos to support learning in a psychomotor skills course. Eur. J. Dent. Educ. 2019, 23, 20–27. [Google Scholar] [PubMed] [Green Version]
- Asghar, S. Impact of Procedure Specific Videos in the Performance of Restorative Procedures by Pre-Clinical dentistry Students. JPDA 2019, 28, 176–180. [Google Scholar]
- Fayaz, A.; Mazahery, A.; Hosseinzadeh, M.; Yazdanpanah, S. Video-based learning versus traditional method for preclinical course of complete denture fabrication. J. Dent. 2015, 16, 21. [Google Scholar]
- Jeyapalan, K.; Mani, U.M.; Christian, J.; Seenivasan, M.K.; Natarajan, P.; Vaidhyanathan, A.K. Influence of Teaching Strategies and its Order of Exposure on Pre-Clinical Teeth Arrangement—A Pilot Study. J. Clin. Diagn. Res. JCDR 2016, 10, ZC93. [Google Scholar] [CrossRef] [PubMed]
- Naseri, M.; Shantiaee, Y.; Rasekhi, J.; Zadsirjan, S.; Bidabadi, M.M.; Khayat, A. Efficacy of video-assisted instruction on knowledge and performance of dental students in access cavity preparation. Iran. Endod. J. 2016, 11, 329. [Google Scholar] [PubMed]
- Almohareb, T. A comparison between video and live demonstrations for teaching dental operative procedures. Pak. Oral Dent. J. 2016, 36, 619–622. [Google Scholar]
- Baidas, L. Comparison of the Con idence Level of Final Year Dental Students in General Practice between two Saudi Dental Colleges in Riyadh”. EC Dent. Sci. 2017, 8, 38–47. [Google Scholar]
- Sandars, J.; Walsh, K. Self-directed learning. Educ. Prim. Care 2016, 27, 151–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gopinath, V.; Nallaswamy, D. A systematic review on the most effective method teaching dentistry to dental students compared to video based learning. Am. J. Educ. Res. 2017, 5, 63–68. [Google Scholar]
- Garbin, C.A.S.; Pacheco Filho, A.C.; Garbin, A.J.I.; Pacheco, K.T.D.S. Instructional video as a teaching/learning tool in times of remote education: A viable alternative. J. Dent. Educ. 2021, 85, 2034–2035. [Google Scholar] [CrossRef] [PubMed]
- Aragon, C.E.; Zibrowski, E.M. Does exposure to a procedural video enhance preclinical dental student performance in fixed prosthodontics? J. Dent. Educ. 2008, 72, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.R.; Cavanaugh, C.; Moore, W.A. Instructional multimedia: An investigation of student and instructor attitudes and student study behavior. BMC Med. Educ. 2011, 11, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Abidi, S.S.R. Healthcare knowledge sharing: Purpose, practices, and prospects. In Healthcare Knowledge Management; Springer: Berlin/Heidelberg, Germany, 2007; pp. 67–86. [Google Scholar]
- Khattak, O.; Ganji, K.K.; Iqbal, A.; Alonazi, M.; Algarni, H.; Alsharari, T. Educational Videos as an Adjunct Learning Tool in Pre-Clinical Operative Dentistry—A Randomized Control Trial. Healthcare 2022, 10, 178. [Google Scholar] [CrossRef]

{kind=link}
| 2 × 2 Contingency Table for Control Group (Before & After) | |||||
|---|---|---|---|---|---|
| Control Group After | Total | p-Value | |||
| Non-Competent | Competent | ||||
| Control group before | Non-competent | 122 | 0 | 122 | 0.352 |
| Competent | 12 | 41 | 53 | ||
| Total | 134 | 41 | 175 | ||
| 2 × 2 Contingency Table for Experimental Group (Before & After) | |||||
|---|---|---|---|---|---|
| Experimental Group After | Total | p-Value | |||
| Non-Competent | Competent | ||||
| Experimental group before | Non-competent | 34 | 0 | 34 | 0.000 |
| Competent | 22 | 119 | 141 | ||
| Total | 56 | 119 | 175 | ||
| Parameter | Variables | B | S.E. | Wald | df | Sig. | Exp (B) | 95% C.I. for EXP (B) | |
|---|---|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||||
| Infection control & Operator position | Gender | 3.69 | 1.10 | 11.17 | 1 | 0.001 | 4.38 | 4.62 | 5.097 |
| CGPA | 5.7 | 1.47 | 15.448 | 1 | 0.000 | 5.25 | 18.17 | 5.25 | |
| Group A | 0.66 | 0.82 | 0.644 | 1 | 0.422 | 1.93 | 0.38 | 9.68 | |
| Group B | 1.2 | 0.72 | 2.78 | 1 | 0.095 | 3.32 | 0.81 | 13.65 | |
| Constant | −26.99 | 6.94 | 15.11 | 1 | 0.000 | 0.000 | |||
| Parameter | Variables | B | S.E. | Wald | df | Sig. | Exp (B) | 95% C.I. for EXP (B) | |
|---|---|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||||
| Tray Organization | Gender | 0.80 | 1.05 | 0.58 | 1 | 0.445 | 2.23 | 0.28 | 3.68 |
| CGPA | 3.25 | 1.10 | 8.72 | 1 | 0.003 | 25.91 | 2.98 | 3.45 | |
| Group A | −1.33 | 0.84 | 2.47 | 1 | 0.115 | 0.26 | 0.05 | 1.38 | |
| Group B | 1.08 | 0.88 | 1.48 | 1 | 0.223 | 2.94 | 0.51 | 2.76 | |
| Constant | −13.14 | 5.24 | 6.28 | 1 | 0.012 | 0.00 | |||
| Parameter | Variables | B | S.E. | Wald | df | Sig. | Exp (B) | 95% C.I. for EXP (B) | |
|---|---|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||||
| Simulator position | Gender | 1.87 | 0.92 | 4.13 | 1 | 0.042 | 6.49 | 1.06 | 6.46 |
| CGPA | 2.41 | 0.89 | 7.20 | 1 | 0.007 | 11.17 | 1.91 | 65.11 | |
| Group A | −1.68 | 0.75 | 5.04 | 1 | 0.025 | 0.18 | 0.04 | 0.80 | |
| Group B | 0.00 | 0.69 | 0.00 | 1 | 1.000 | 1.00 | 0.25 | 3.92 | |
| Constant | −10.15 | 4.24 | 5.71 | 1 | 0.017 | 0.00 | |||
| Parameter | Variables | B | S.E. | Wald | df | Sig. | Exp (B) | 95% C.I. for EXP (B) | |
|---|---|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||||
| Cavity outline and extension | Gender | −1.65 | 1.18 | 1.93 | 1 | 0.164 | 0.19 | 0.01 | 1.96 |
| CGPA | 1.72 | 0.99 | 3.04 | 1 | 0.081 | 5.62 | 0.80 | 3.14 | |
| Group A | −2.15 | 1.02 | 4.40 | 1 | 0.036 | 0.11 | 0.01 | 0.86 | |
| Group B | 0.33 | 0.82 | 0.16 | 1 | 0.684 | 1.39 | 0.28 | 6.97 | |
| Constant | −4.60 | 4.89 | 0.88 | 1 | 0.347 | 0.01 | |||
| Parameter | Variables | B | S.E. | Wald | df | Sig. | Exp (B) | 95% C.I. for EXP (B) | |
|---|---|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||||
| Resistance form & Retention form | Gender | 0.04 | 1.09 | 0.00 | 1 | 0.965 | 1.04 | 0.12 | 8.89 |
| CGPA | 3.93 | 1.31 | 8.98 | 1 | 0.003 | 11.01 | 3.89 | 5.36 | |
| Group A | −0.23 | 0.93 | 0.06 | 1 | 0.804 | 0.79 | 0.126 | 4.99 | |
| Group B | 2.09 | 0.95 | 4.83 | 1 | 0.028 | 8.09 | 1.25 | 3.57 | |
| Constant | −16.28 | 6.20 | 6.88 | 1 | 0.009 | 0.00 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iqbal, A.; Ganji, K.K.; Khattak, O.; Shrivastava, D.; Srivastava, K.C.; Arjumand, B.; AlSharari, T.; Alqahtani, A.M.A.; Hamza, M.O.; AbdelrahmanDafaalla, A.A.E.G. Enhancement of Skill Competencies in Operative Dentistry Using Procedure-Specific Educational Videos (E-Learning Tools) Post-COVID-19 Era—A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 4135. https://doi.org/10.3390/ijerph19074135
Iqbal A, Ganji KK, Khattak O, Shrivastava D, Srivastava KC, Arjumand B, AlSharari T, Alqahtani AMA, Hamza MO, AbdelrahmanDafaalla AAEG. Enhancement of Skill Competencies in Operative Dentistry Using Procedure-Specific Educational Videos (E-Learning Tools) Post-COVID-19 Era—A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(7):4135. https://doi.org/10.3390/ijerph19074135
Chicago/Turabian StyleIqbal, Azhar, Kiran Kumar Ganji, Osama Khattak, Deepti Shrivastava, Kumar Chandan Srivastava, Bilal Arjumand, Thani AlSharari, Ali Mosfer A Alqahtani, May Othman Hamza, and Ahmed Abu El Gasim AbdelrahmanDafaalla. 2022. "Enhancement of Skill Competencies in Operative Dentistry Using Procedure-Specific Educational Videos (E-Learning Tools) Post-COVID-19 Era—A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 7: 4135. https://doi.org/10.3390/ijerph19074135
APA StyleIqbal, A., Ganji, K. K., Khattak, O., Shrivastava, D., Srivastava, K. C., Arjumand, B., AlSharari, T., Alqahtani, A. M. A., Hamza, M. O., & AbdelrahmanDafaalla, A. A. E. G. (2022). Enhancement of Skill Competencies in Operative Dentistry Using Procedure-Specific Educational Videos (E-Learning Tools) Post-COVID-19 Era—A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 19(7), 4135. https://doi.org/10.3390/ijerph19074135