
A Citizen Science Approach to Identifying Indoor Environmental Barriers to Optimal Health for under 5s Experiencing Homelessness in Temporary Accommodation

 ,
, 
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Theoretical Frameworks
2.3. Study Design
2.4. Study Setting
2.5. Study Overview and Co-Design
2.5.1. Citizen Science Approach
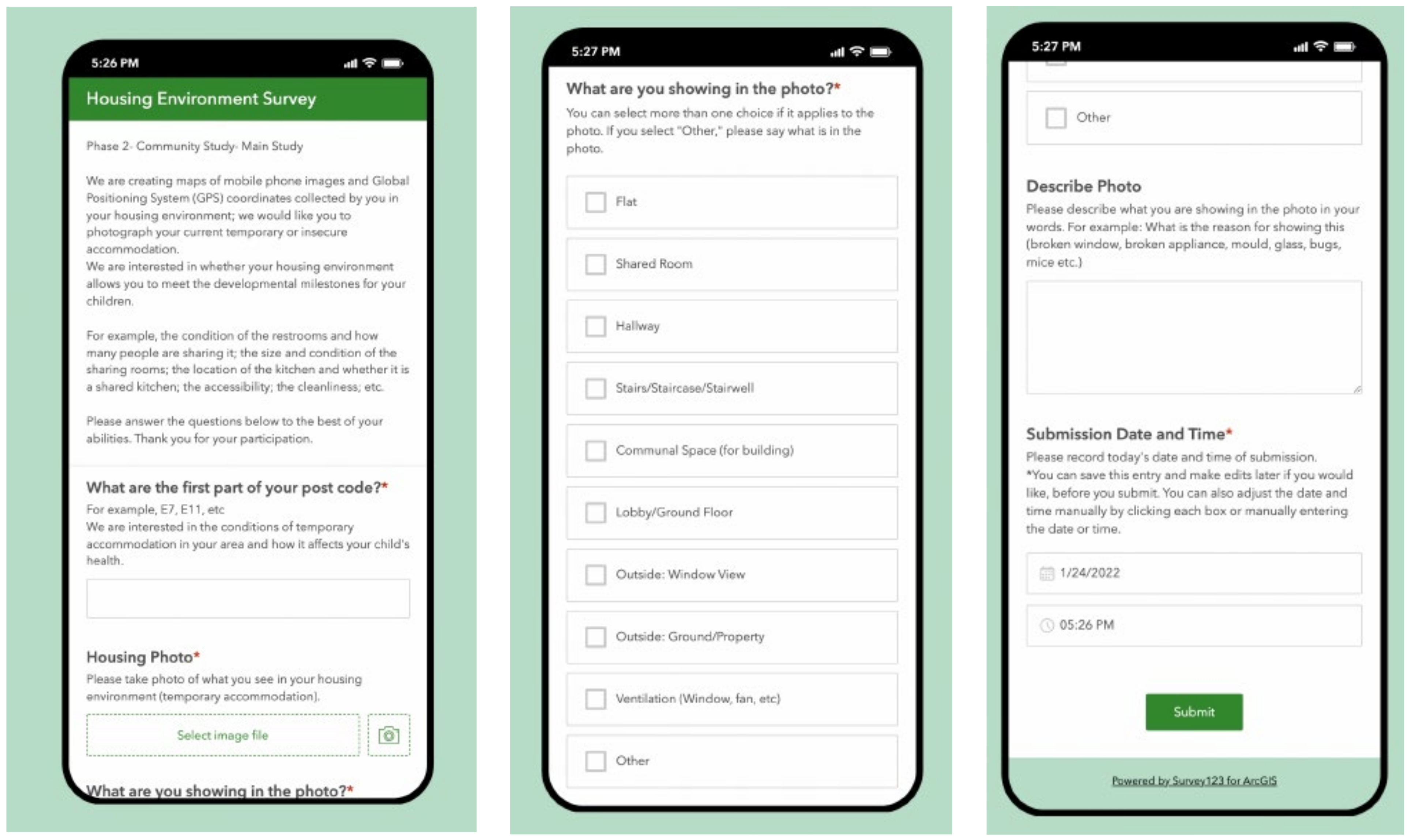
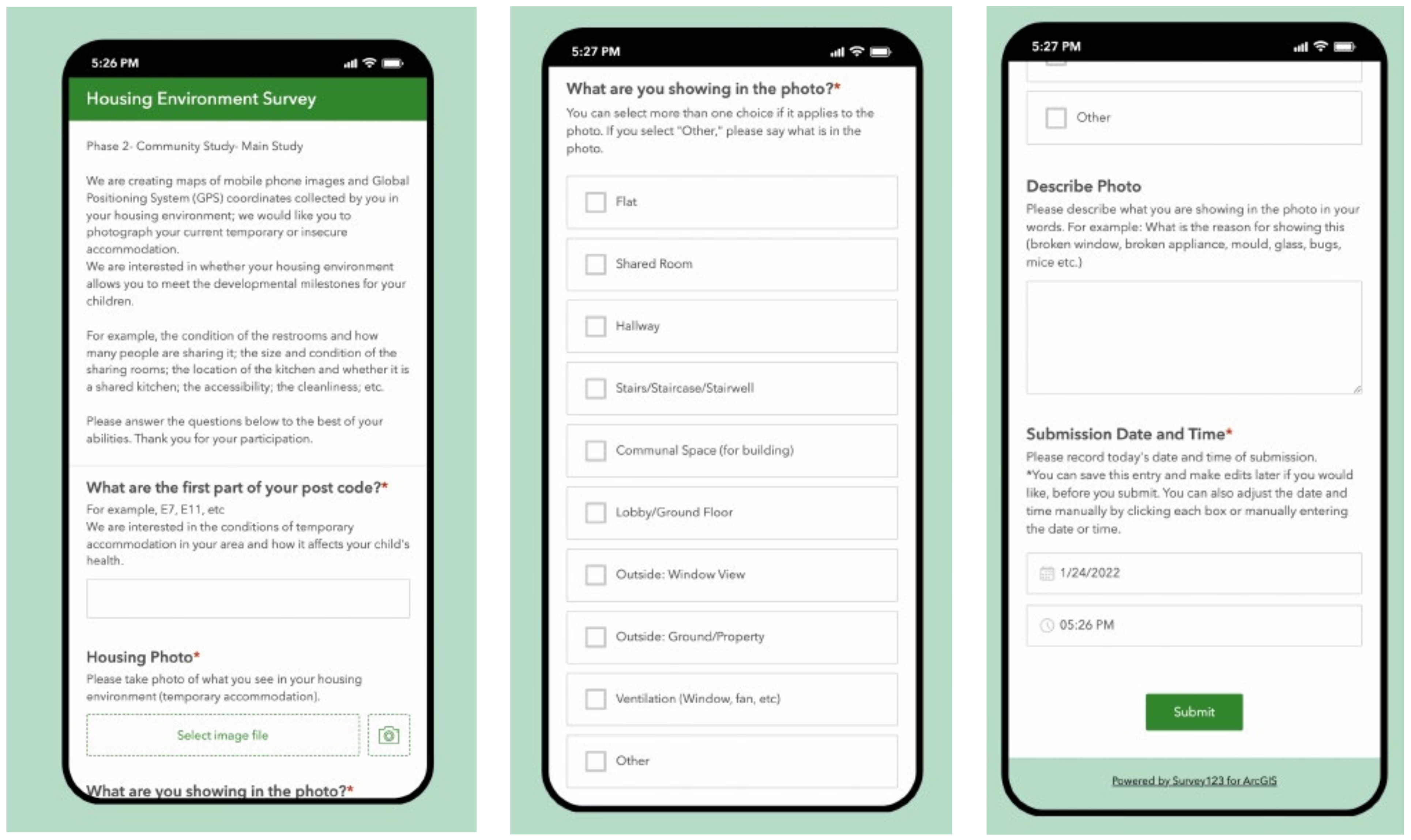
2.5.2. Part I: Mobile App Housing Survey
2.5.3. Part II: House Visits
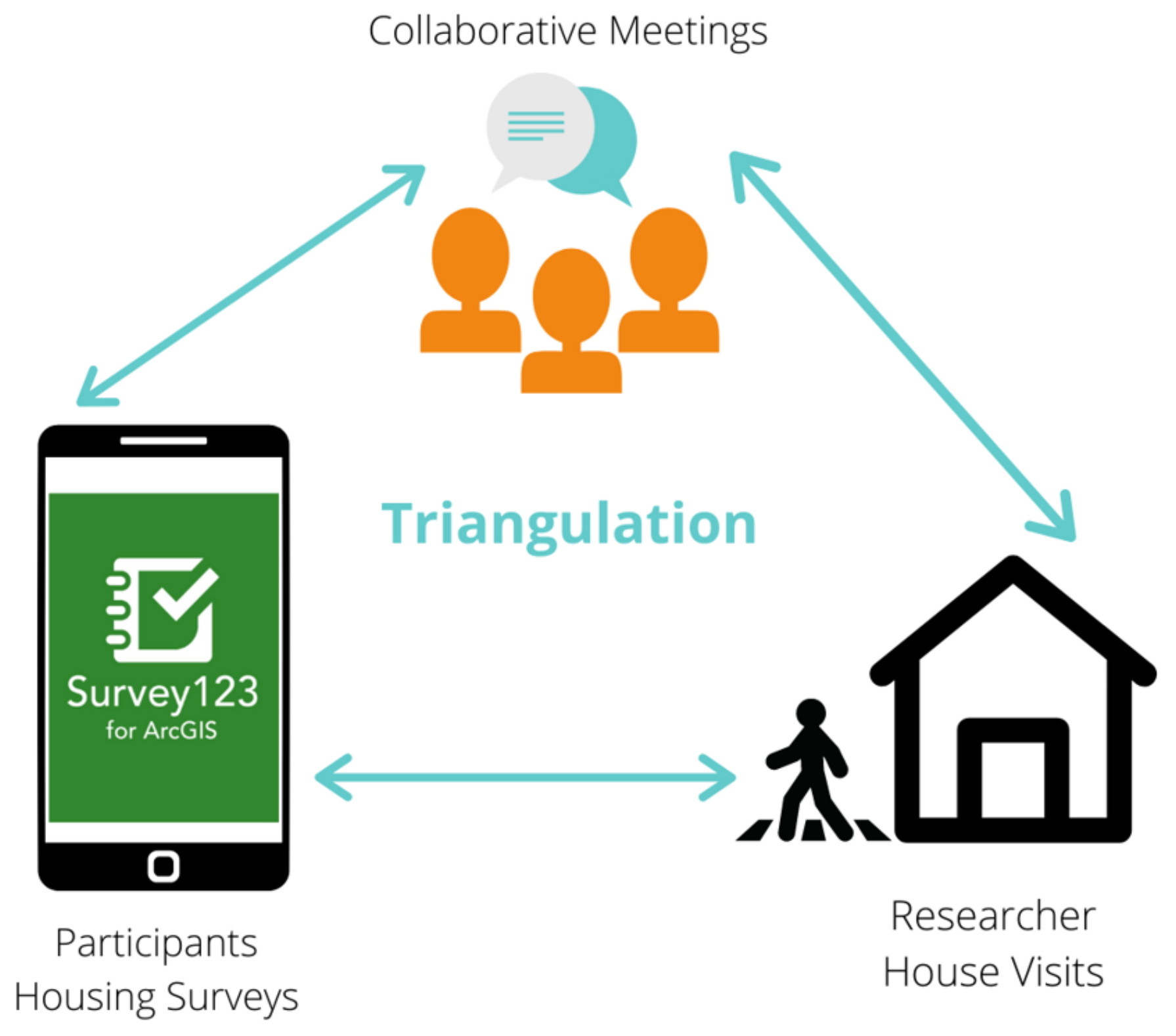
2.5.4. Part III: Collaborative Meetings
2.5.5. Pilot and Refinement of Study Tools
2.6. Recruitment
2.7. Analysis
3. Results
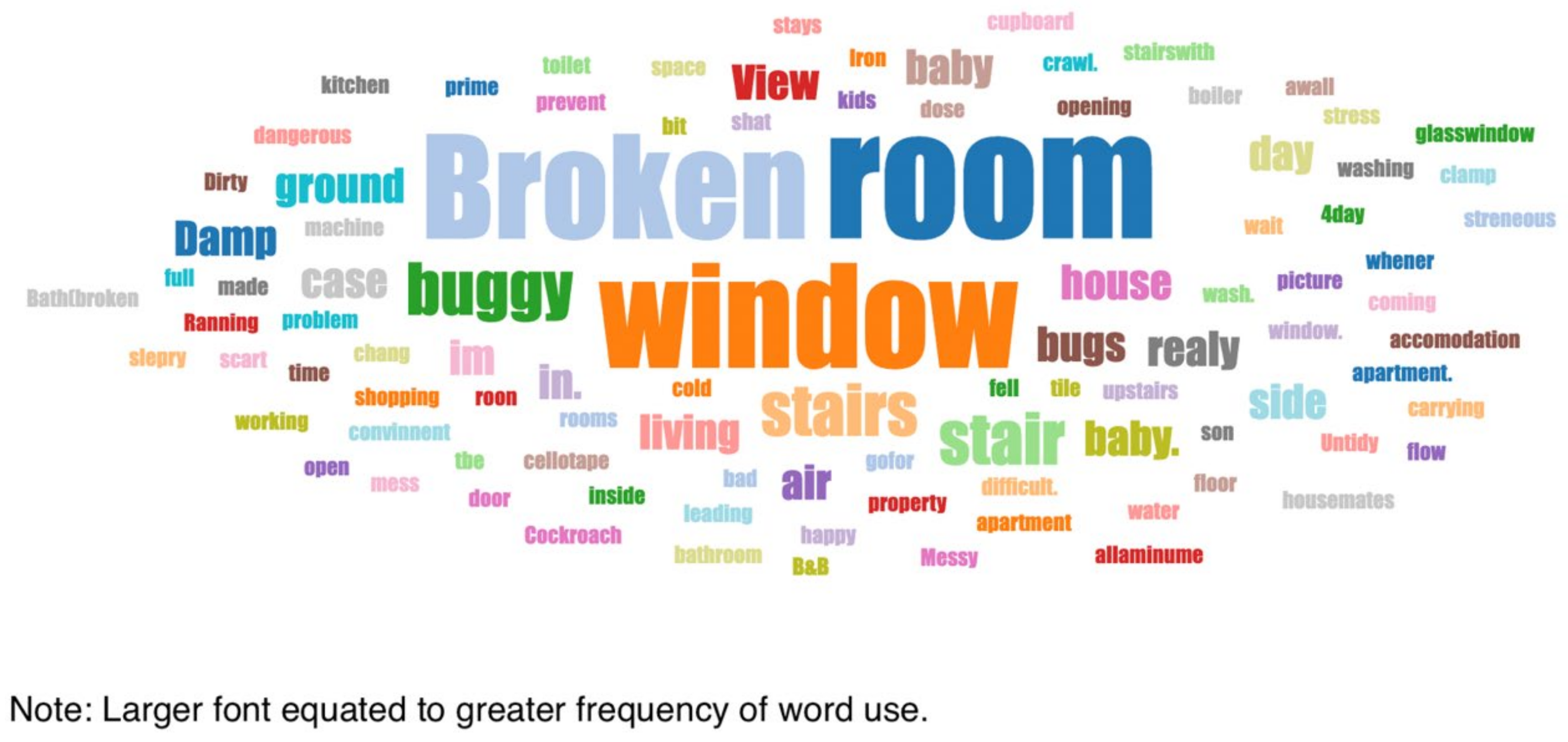
3.1. Mobile App Housing Survey
3.2. House Visits
3.3. Collaborative Meetings
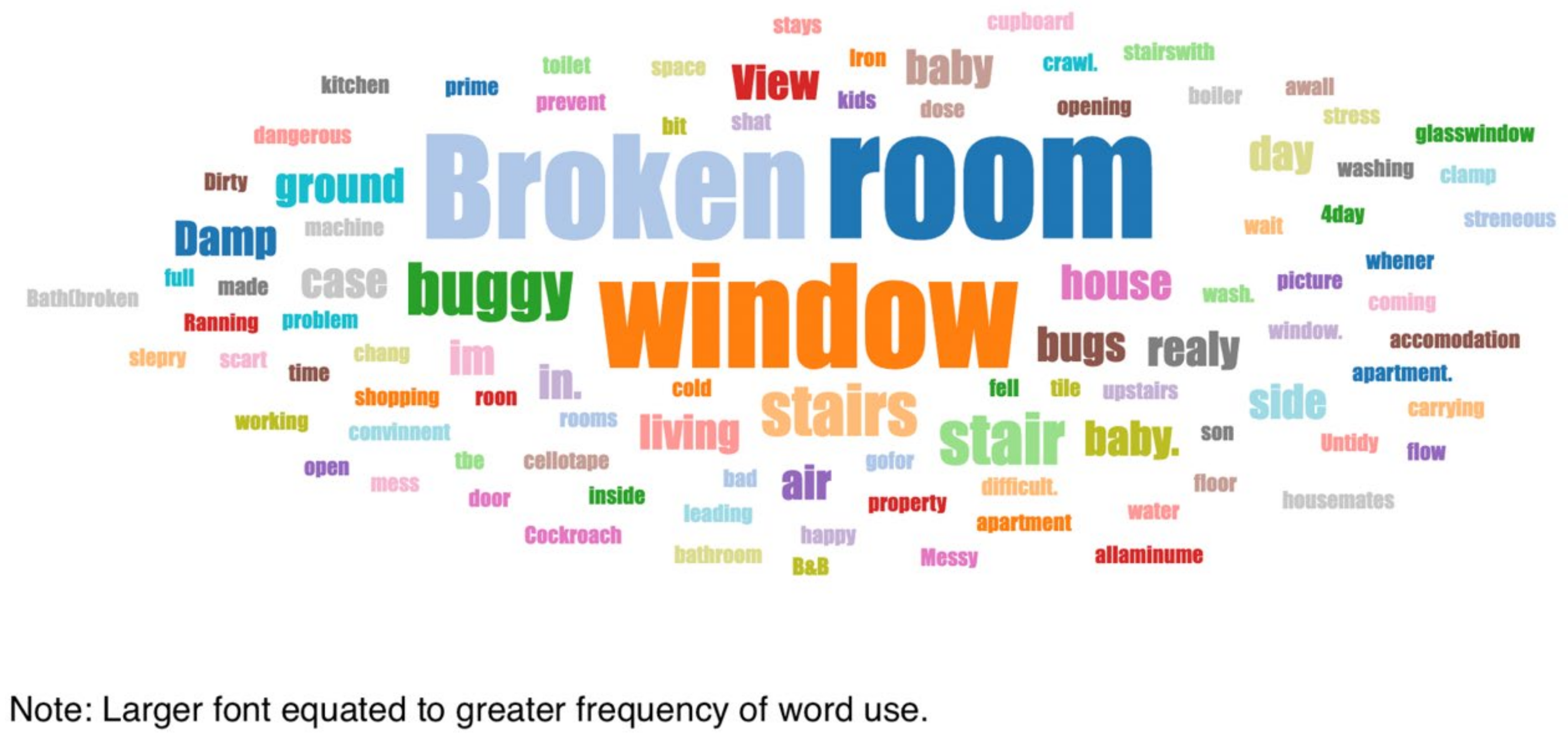
3.4. Thematic Analysis
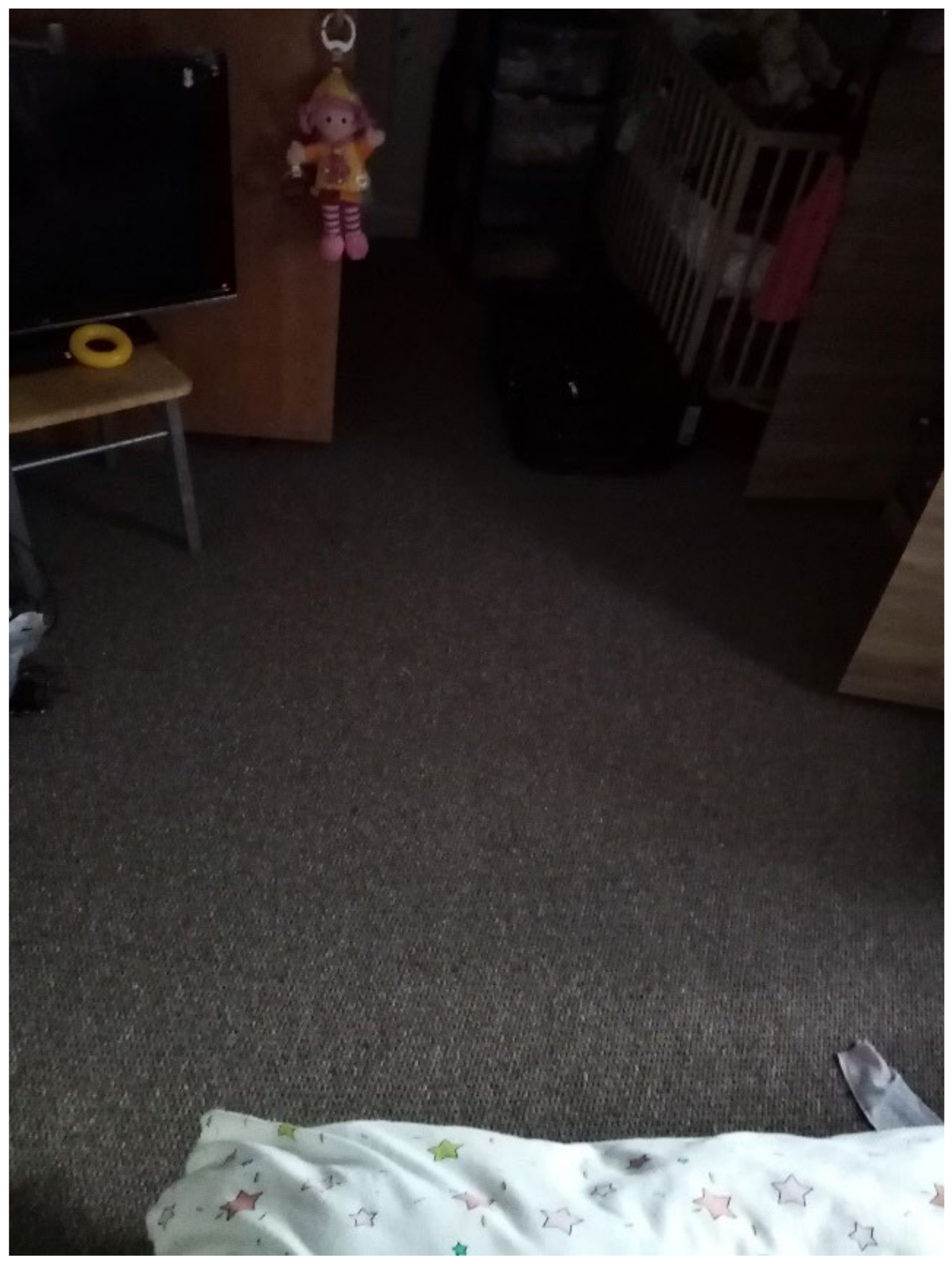
3.4.1. Overcrowding and Shared Facilities
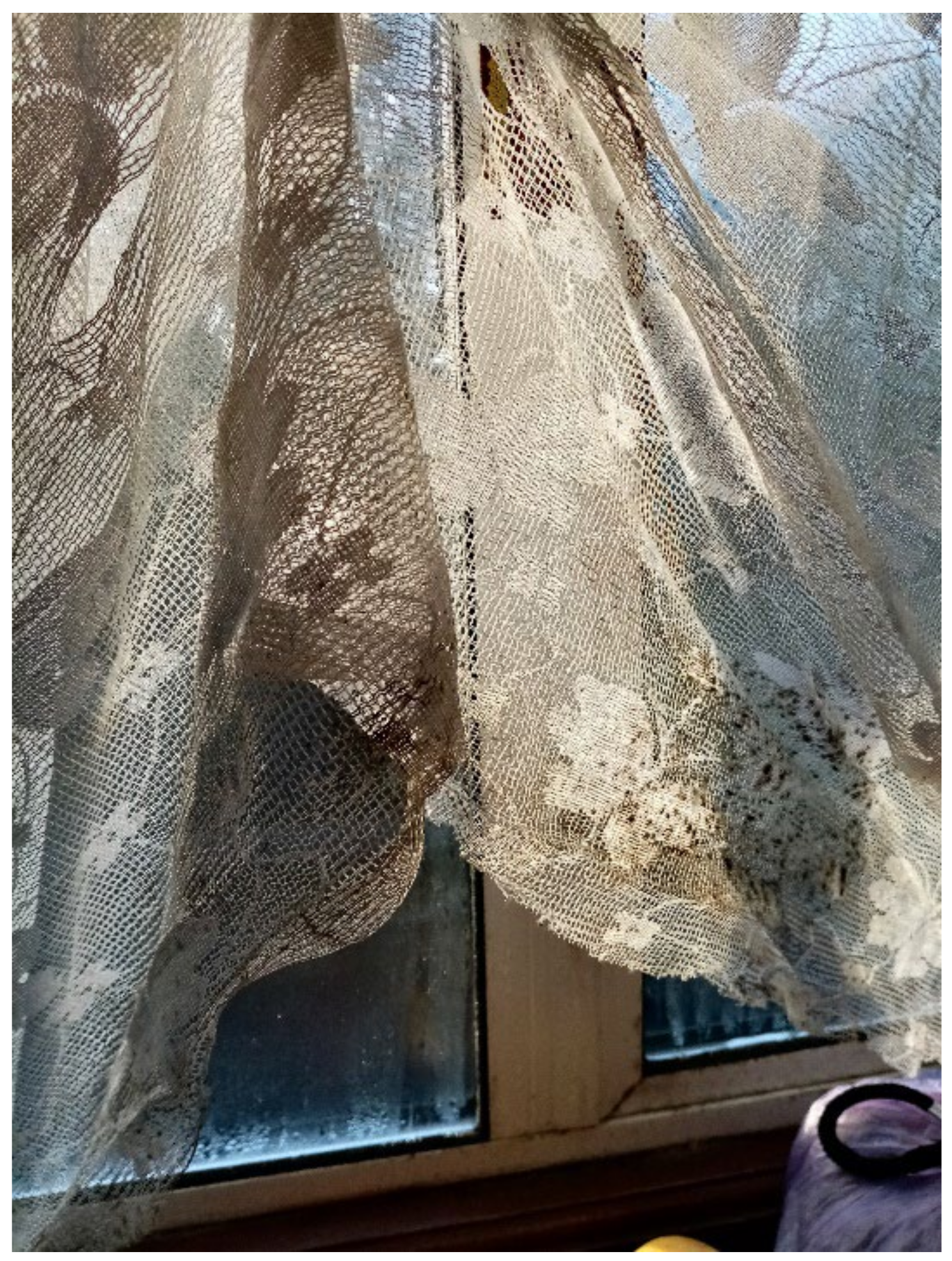
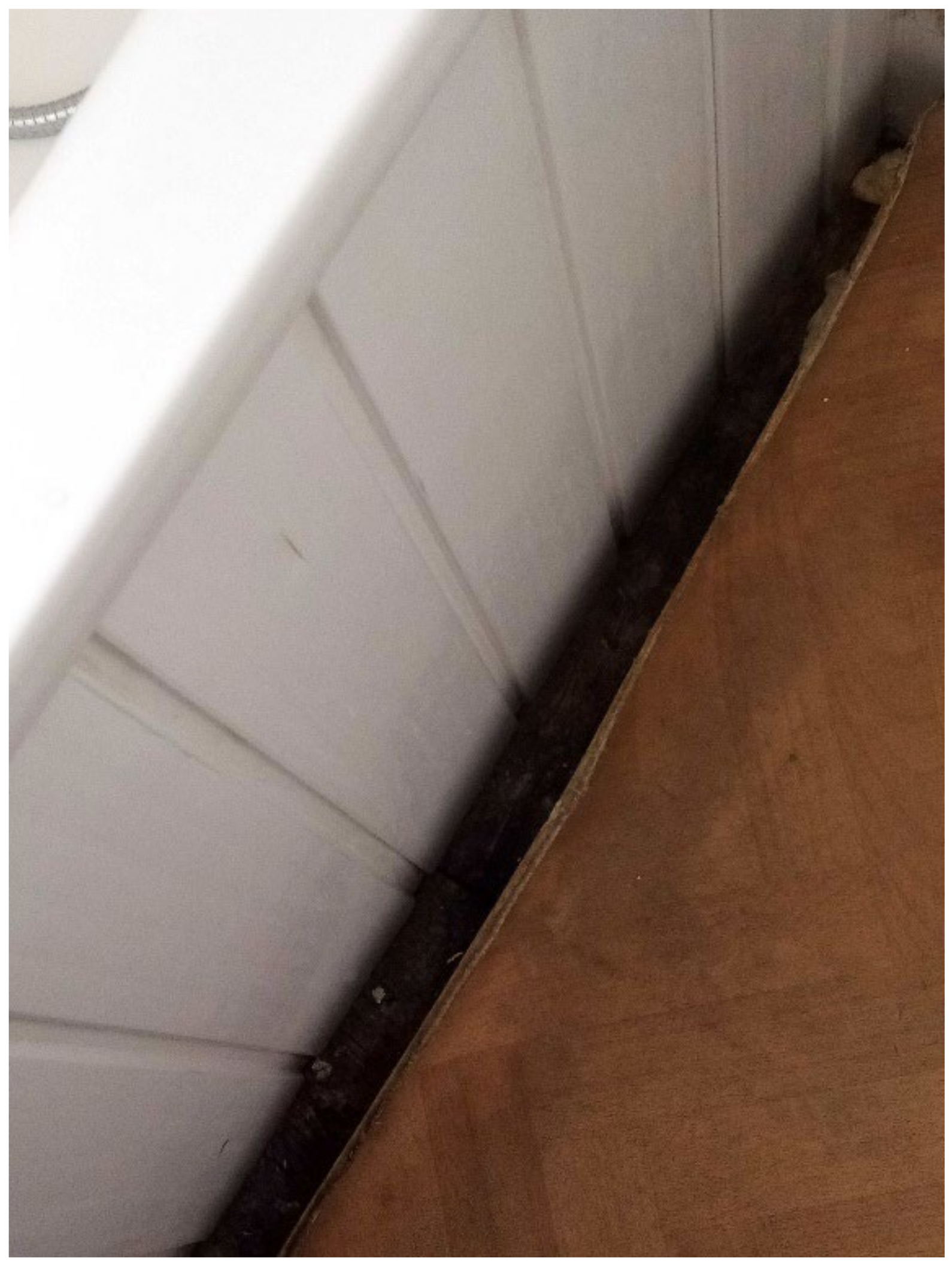
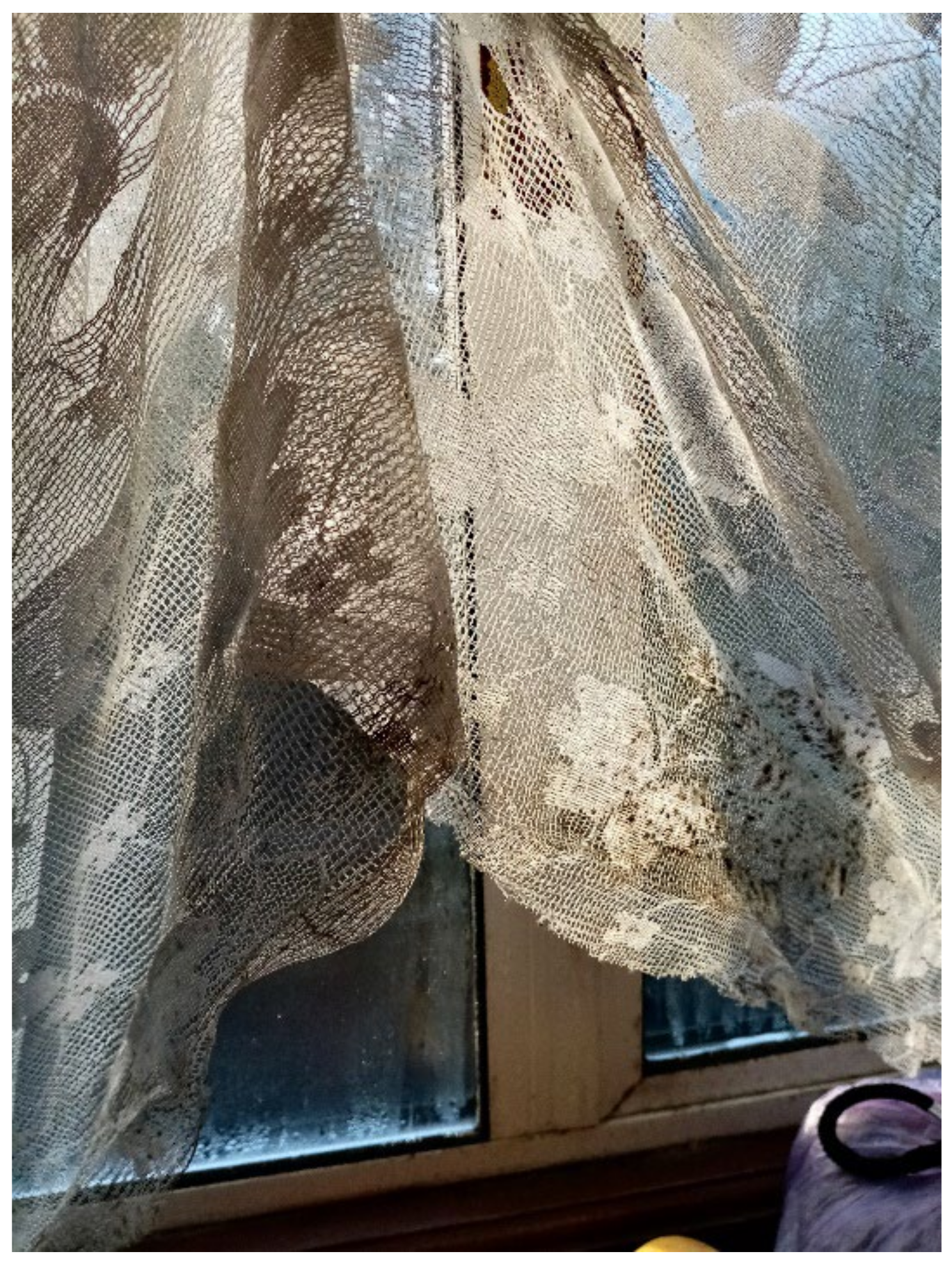
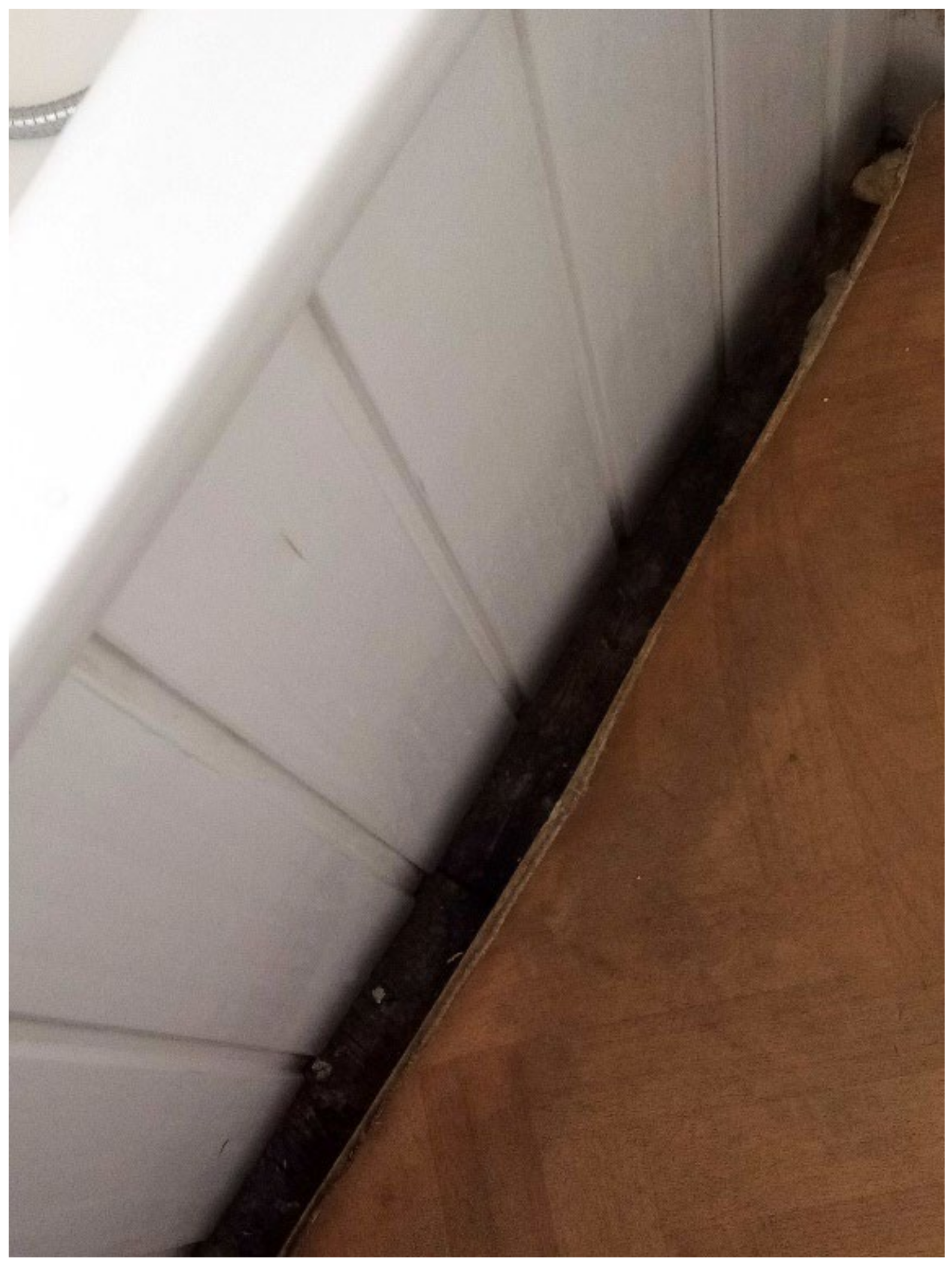
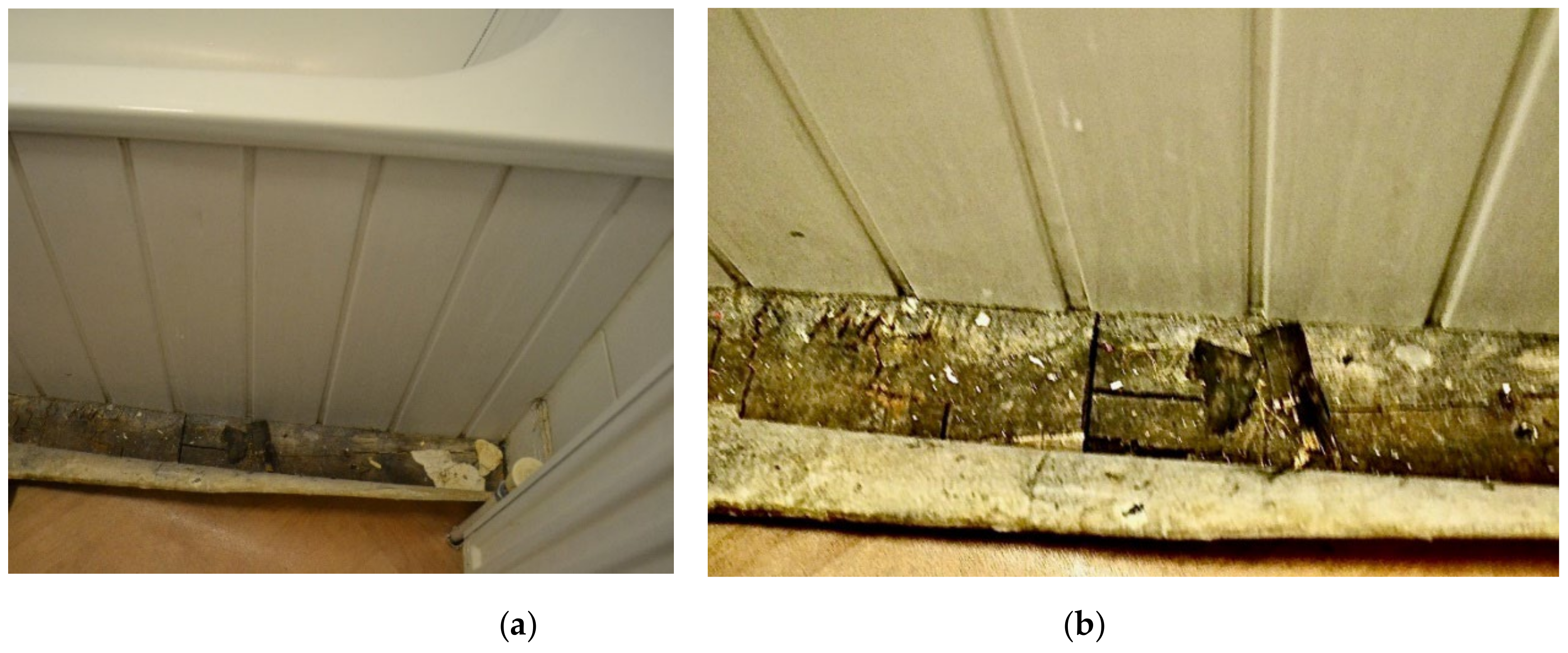
3.4.2. Dampness/Mold Growth
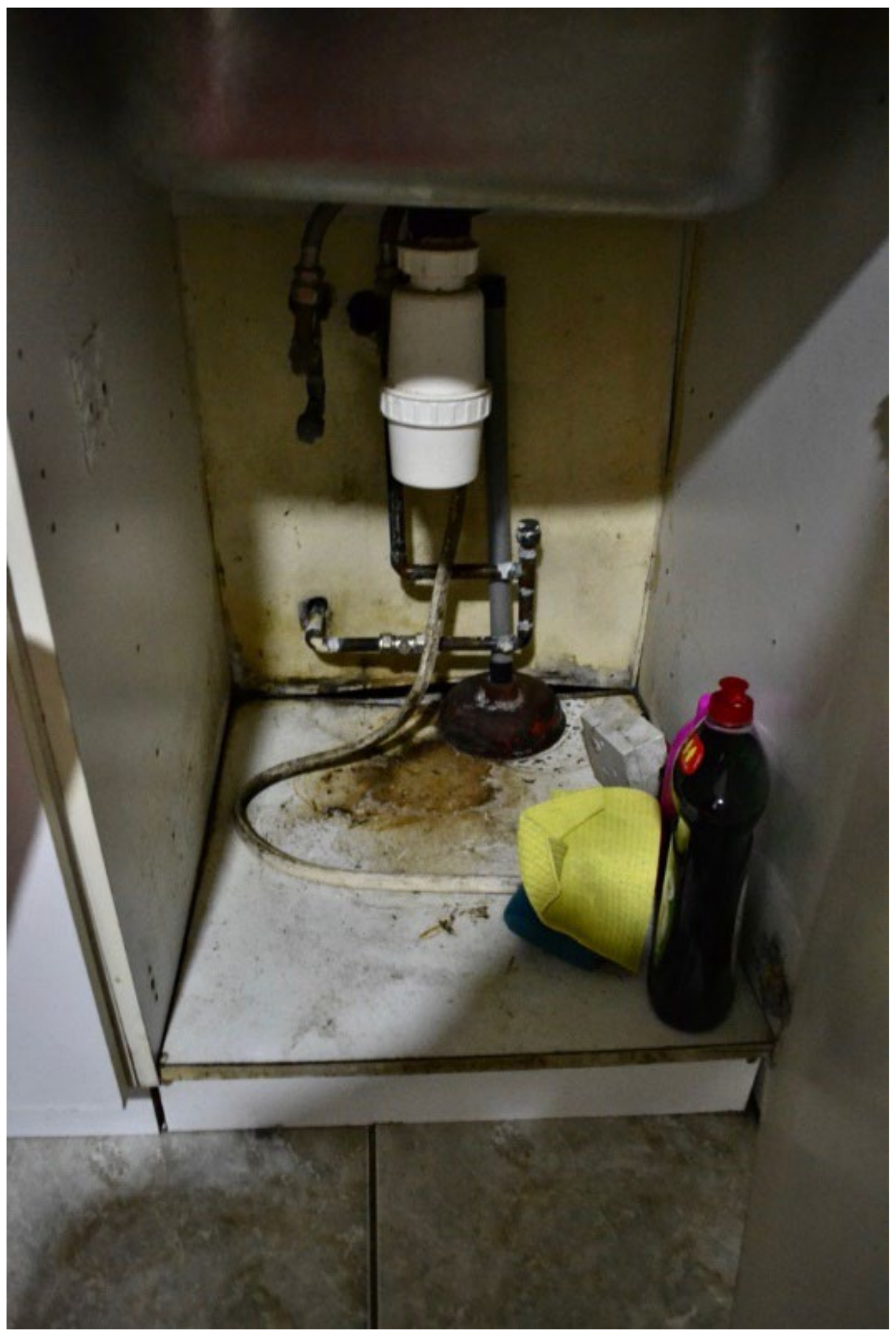
3.4.3. Poor/Inadequate Kitchen/Toilet Facilities
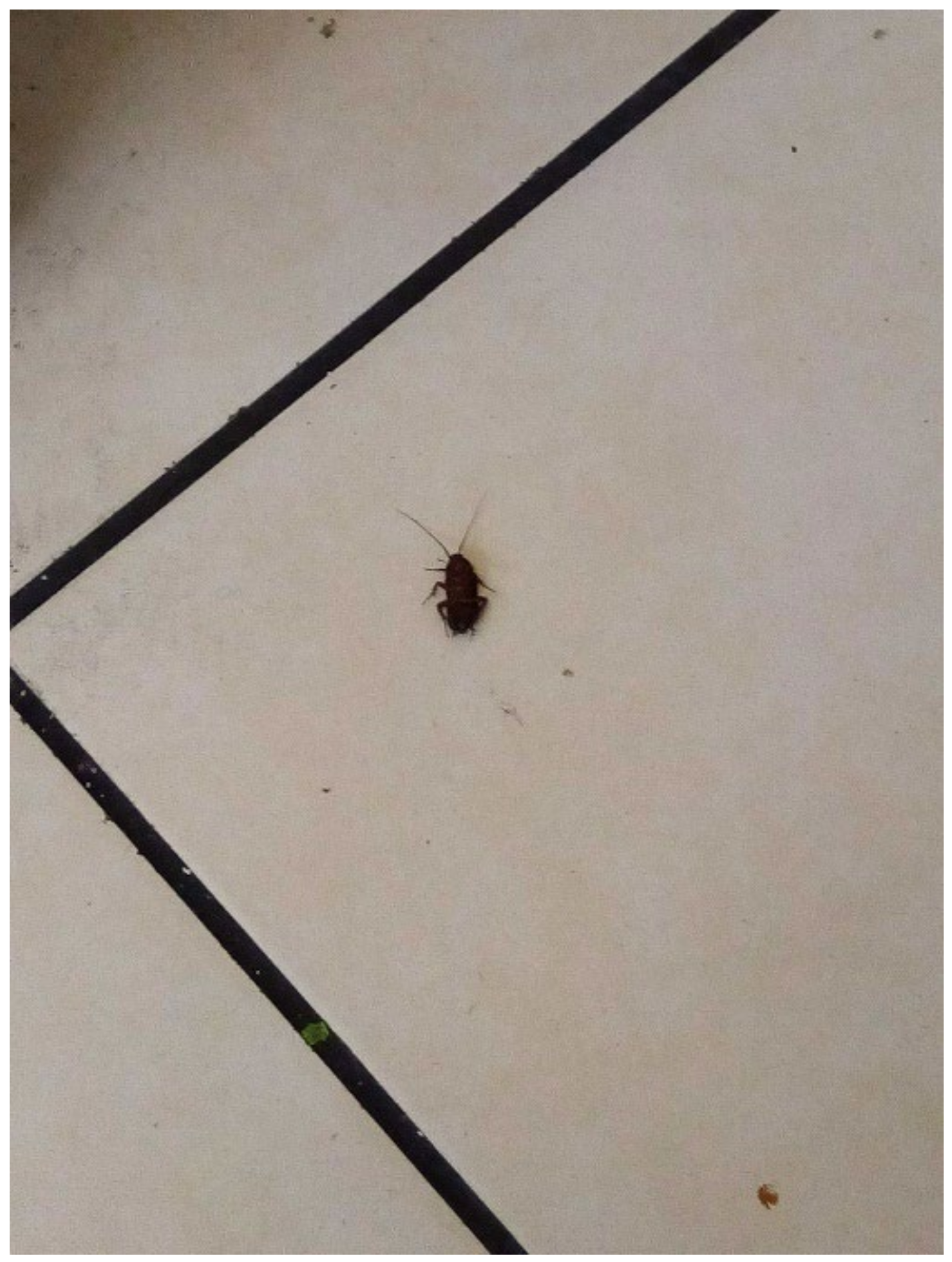
3.4.4. Infestations/Vermin
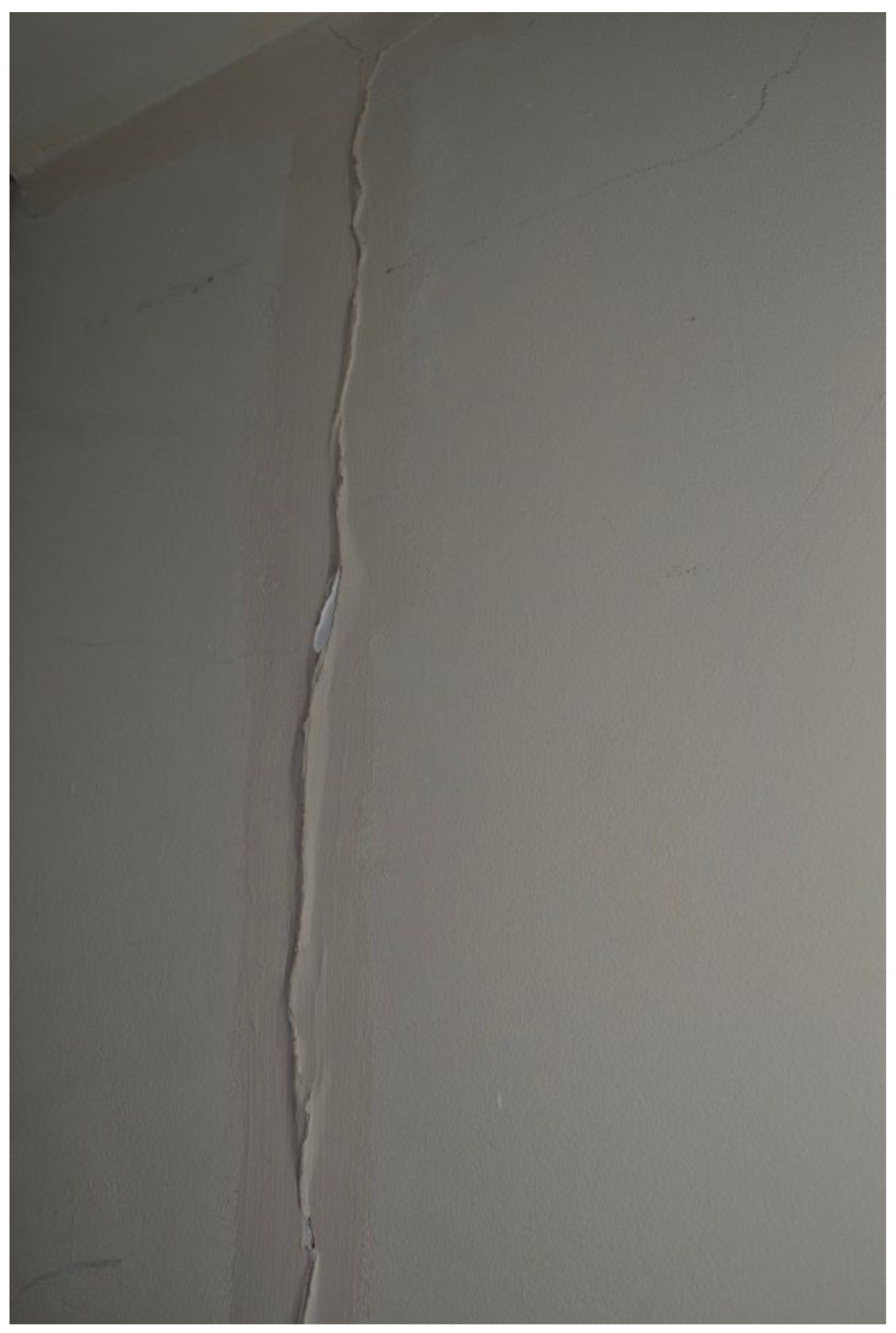
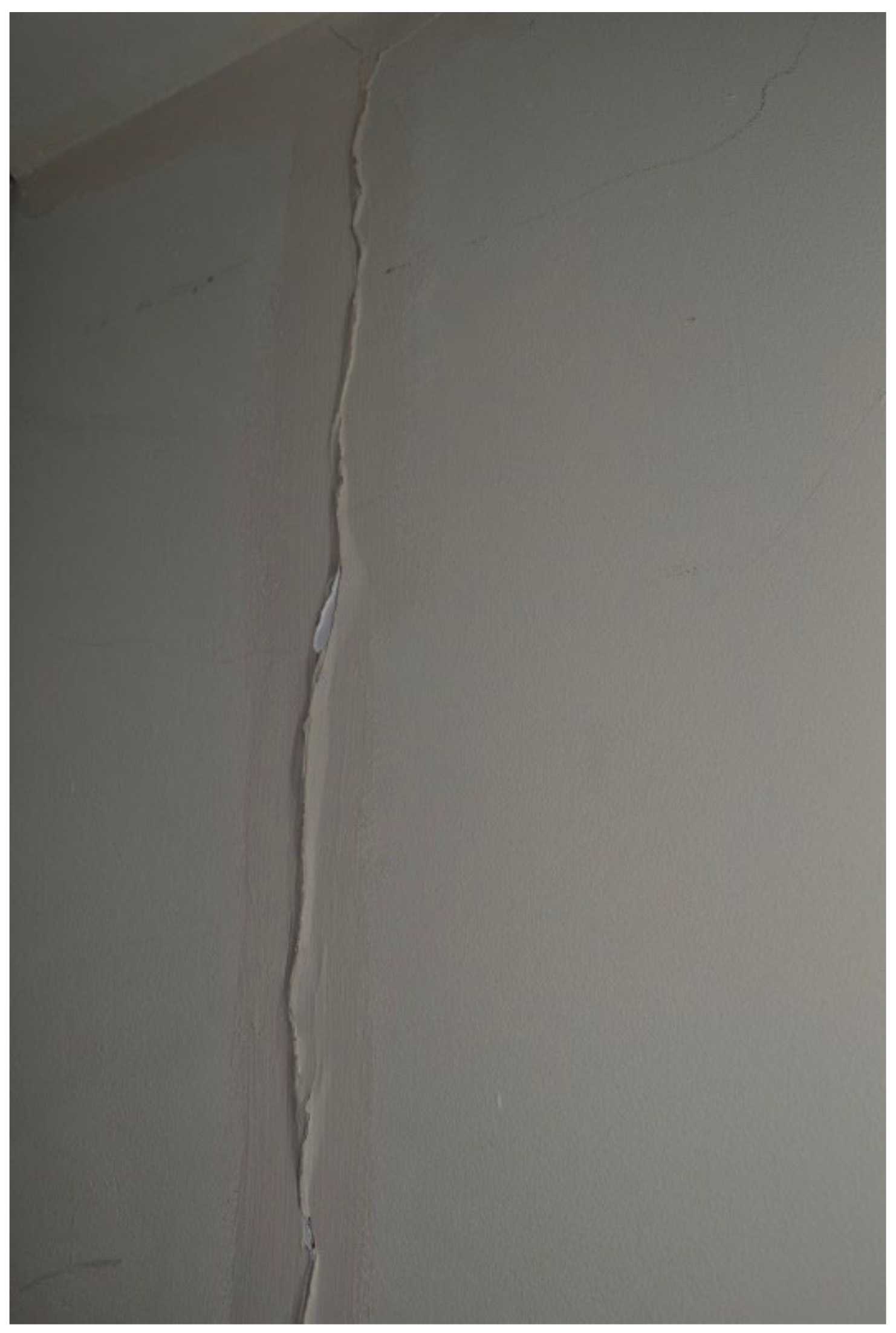
3.4.5. Structural Problems and/or Disrepair
3.4.6. Unsafe Electrical Systems and Appliances
3.4.7. Excessively Cold Due to Inadequate Temperature Regulation
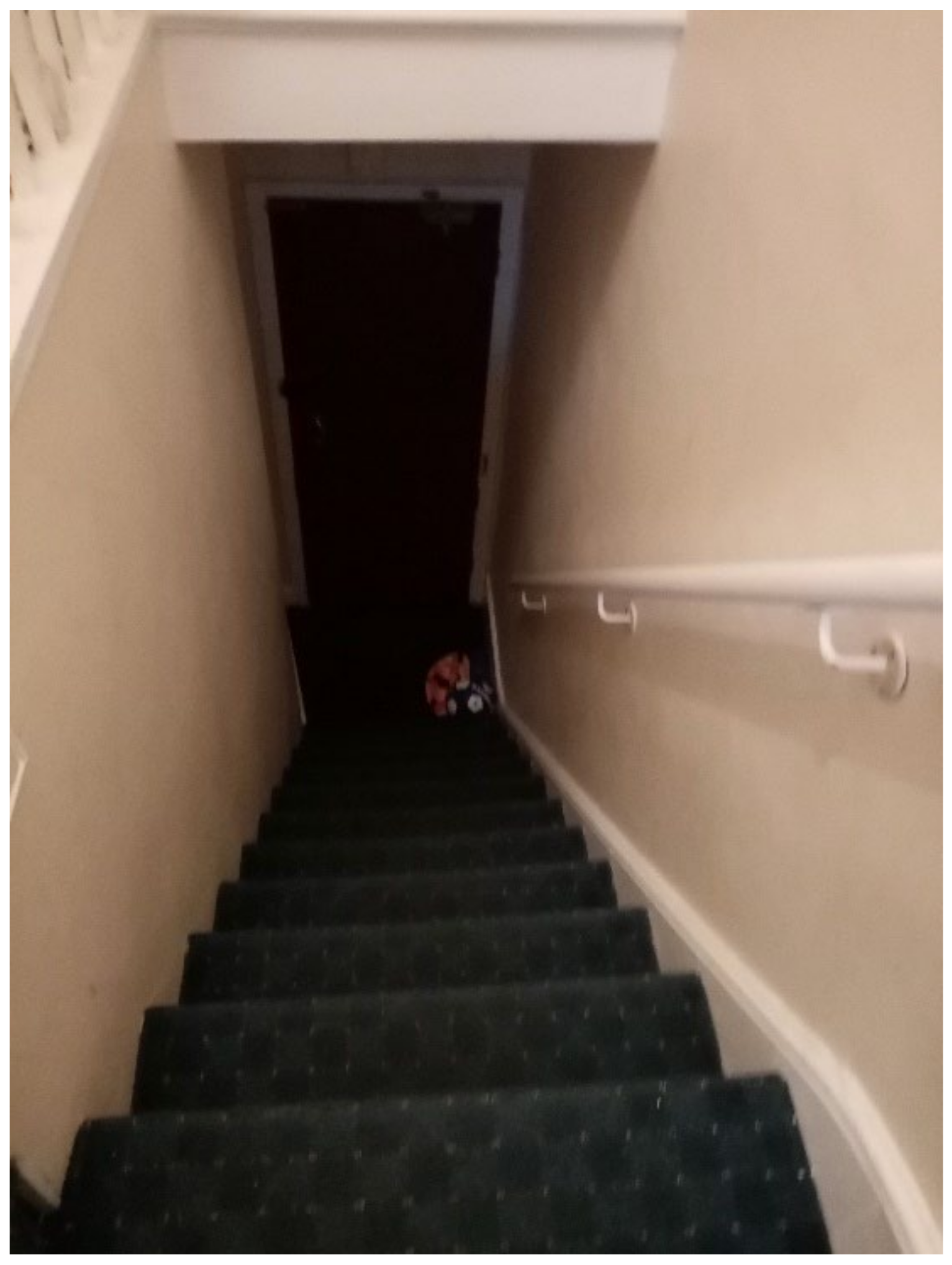
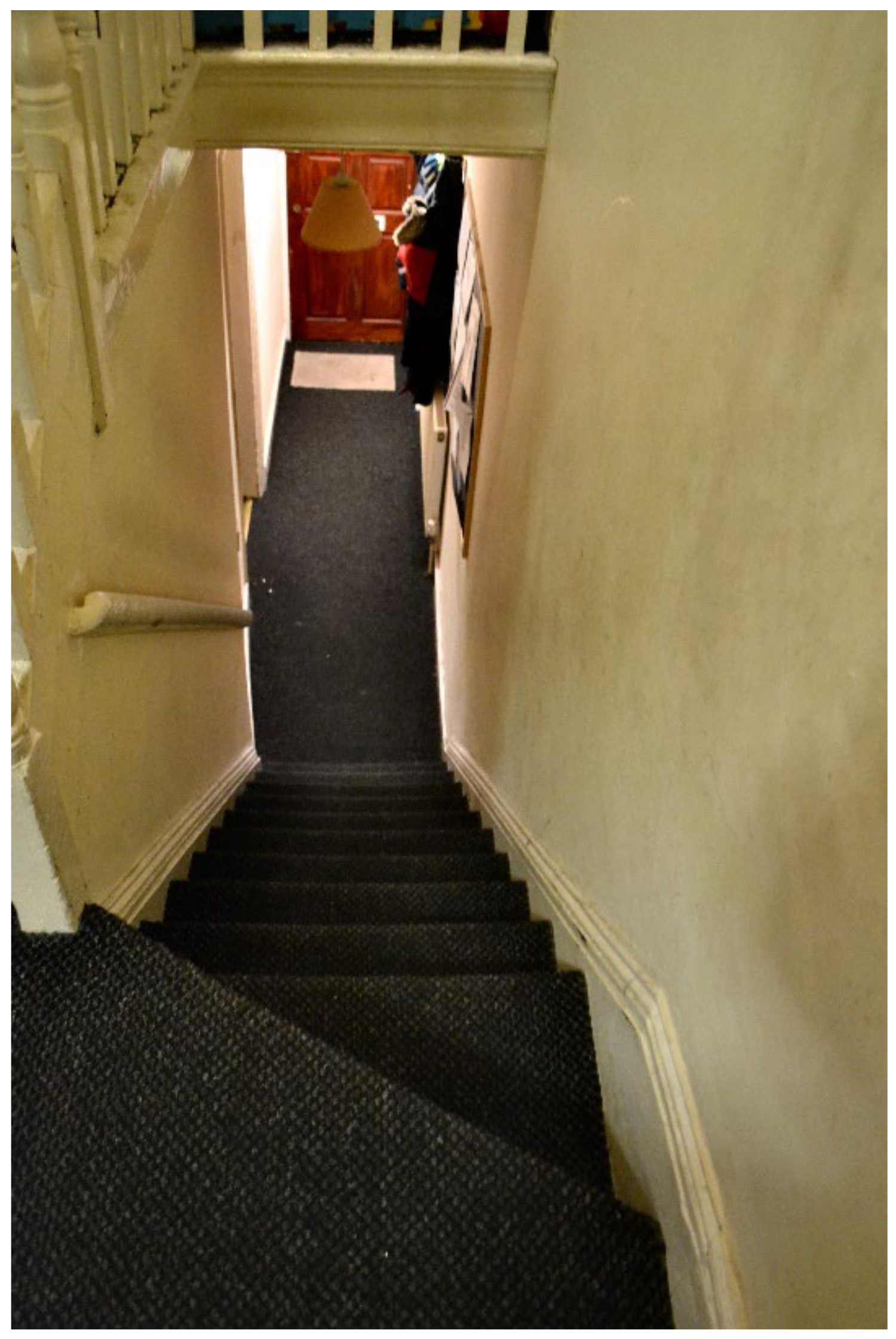
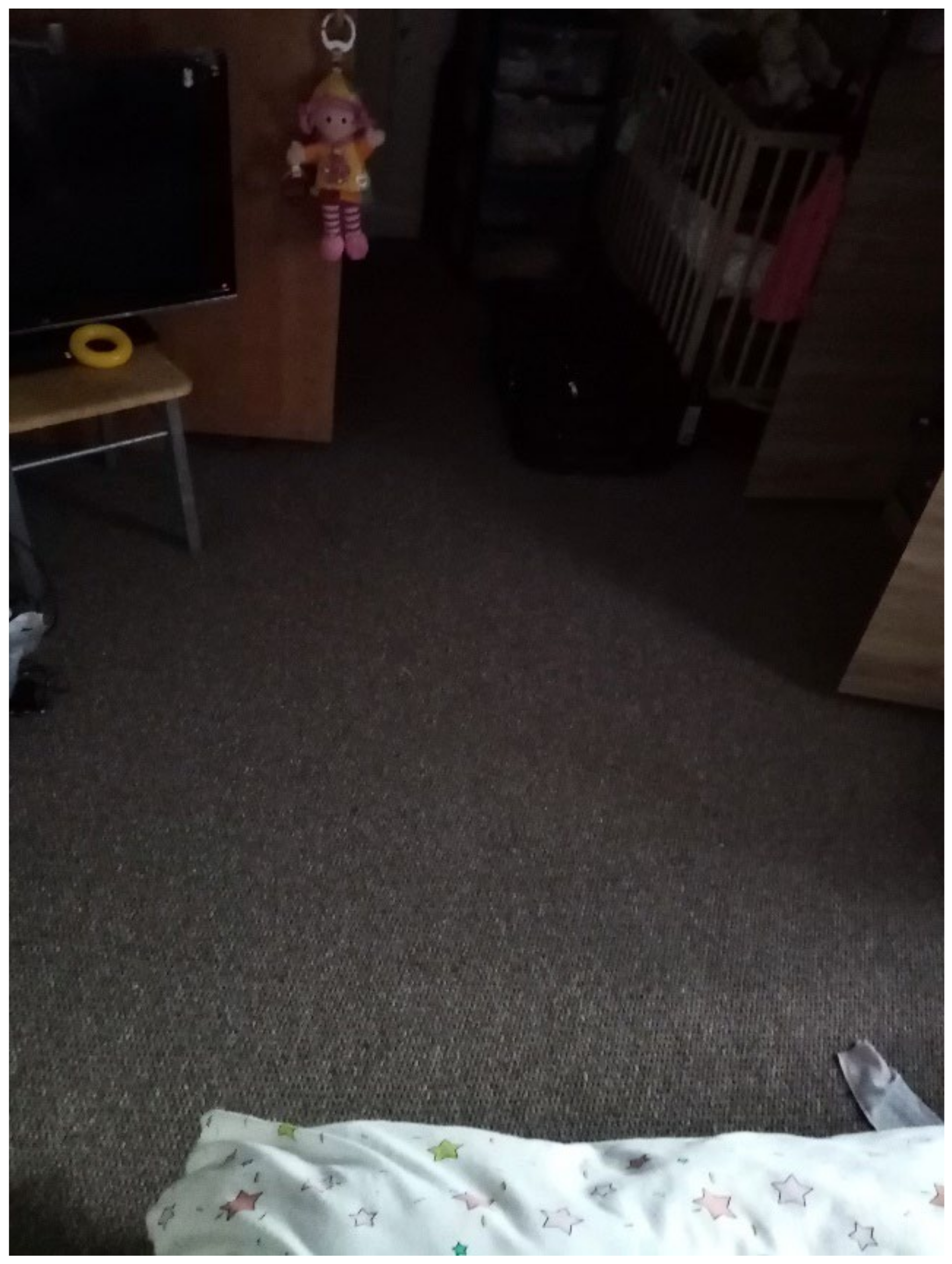
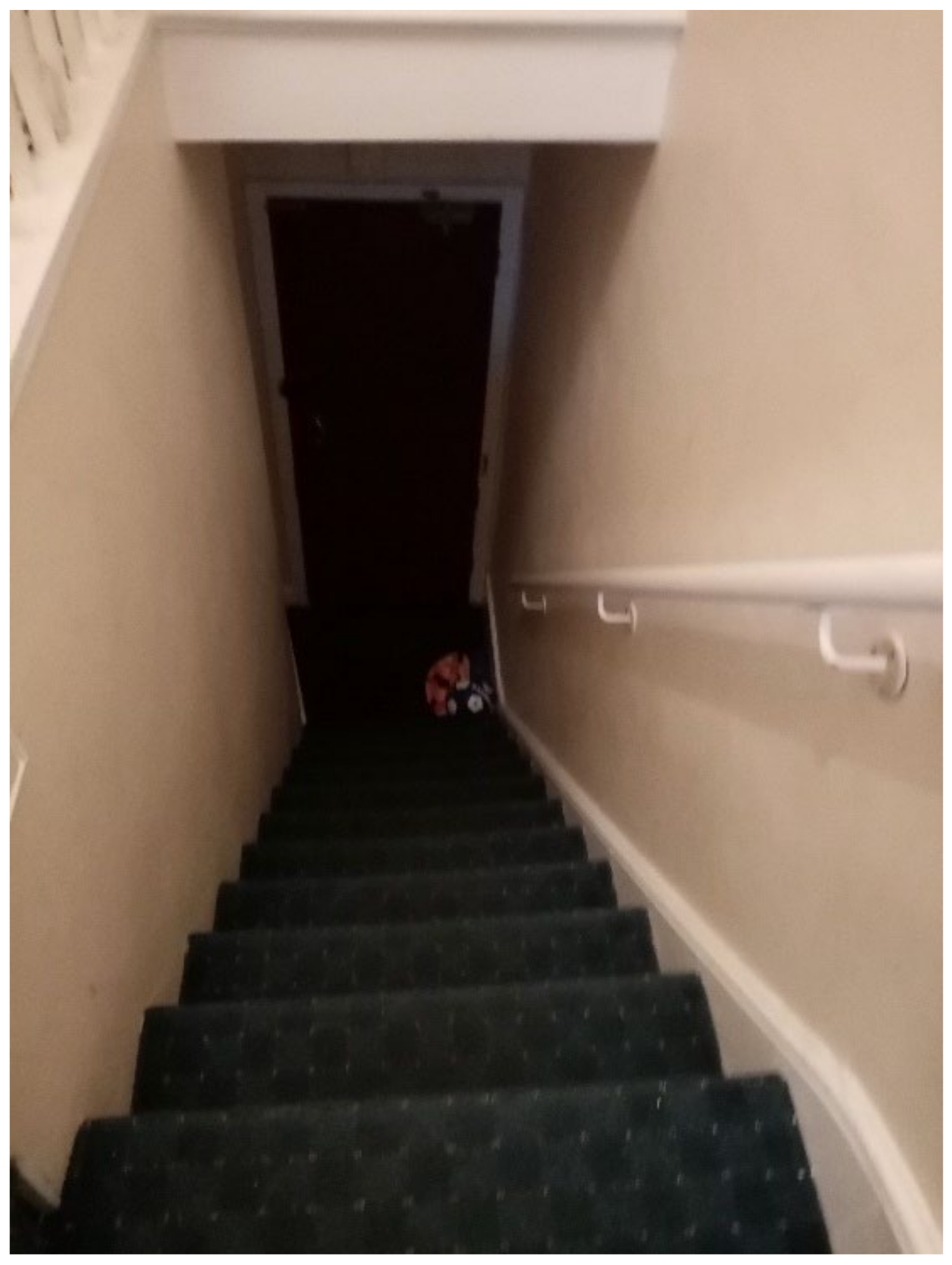
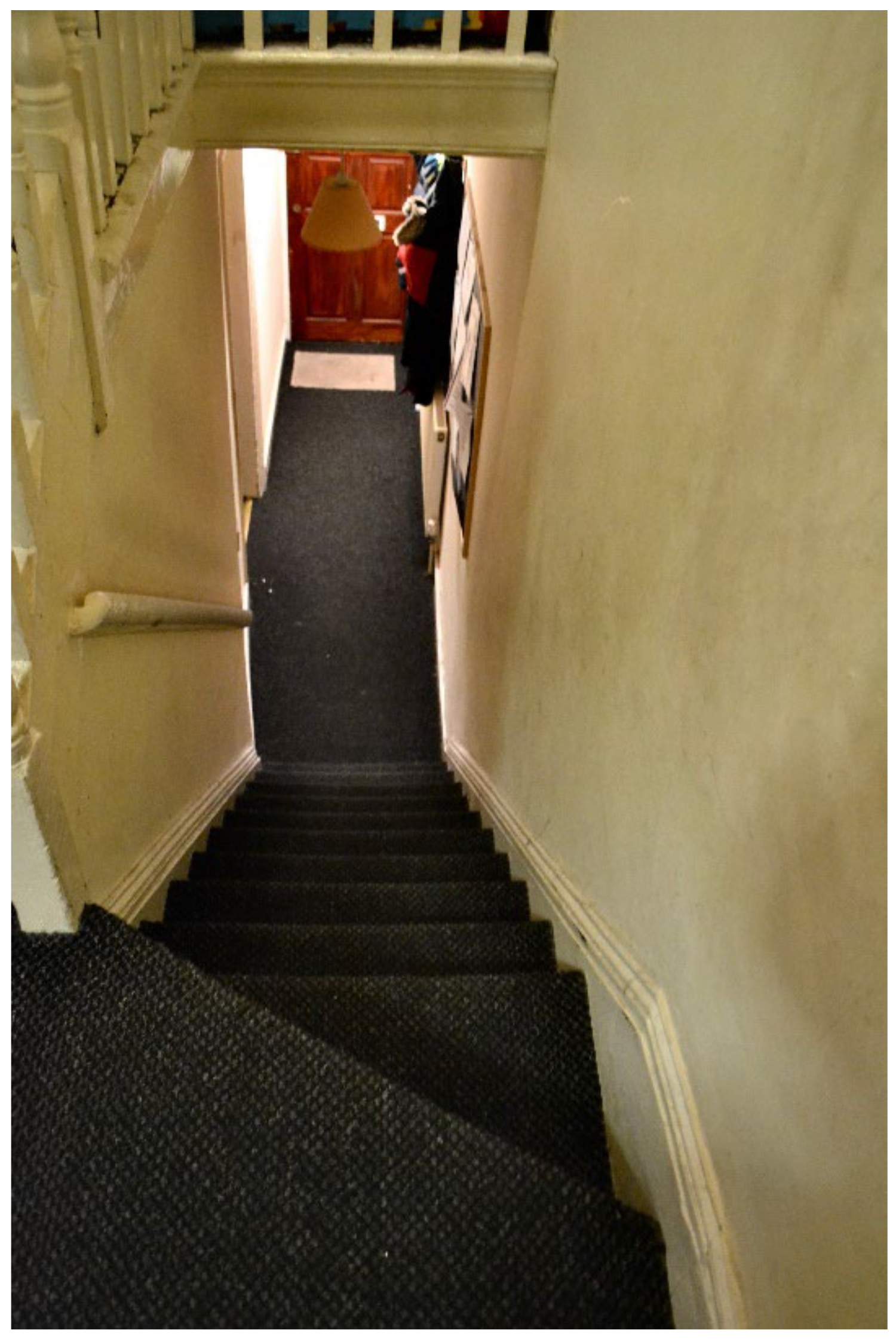
3.4.8. Unsafe Surfaces That Risk Causing Trips or Falls
4. Discussion
4.1. Benefits and Ethical Challenges of Citizen Science
4.2. Health Implications
4.3. Contribution to the Literature
4.4. Policy Implications
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Black, M.M.; Merseth, K.A. First 1000 Days and Beyond: Strategies to Achieve the Sustainable Development Goals. In Developmental Science and Sustainable Development Goals for Children and Youth; Springer: Cham, Switzerland, 2018; pp. 97–112. [Google Scholar] [CrossRef]
- Cusick, S.; Georgieff, M.K. The First 1000 Days of Life: The Brain’s Window of Opportunity. Available online: https://www.unicef-irc.org/article/958-the-first-1000-days-of-life-the-brains-window-of-opportunity.html (accessed on 15 March 2019).
- Walker, S.P.; Wachs, T.D.; Gardner, J.M.; Lozoff, B.; Wasserman, G.A.; Pollitt, E.; Carter, J.A. Child development: Risk factors for adverse outcomes in developing countries. Lancet 2007, 369, 145–157. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. CDC’s Developmental Milestones. Available online: https://www.cdc.gov/ncbddd/actearly/milestones/index.html (accessed on 1 January 2022).
- Moore, T.; Arefadib, N.; Deery, A.; West, S. The First Thousand Days The First Thousand Days: An Evidence Paper; Centre for Community Child Health: Parkville, VIC, Australia, 2017. [Google Scholar]
- Marmot, M.; Allen, J.; Boyce, T.; Goldblatt, P.; Morrison, J. Health Equity In England: The Marmot Review 10 Years On; Institute of Health Equity: London, UK, 2020. [Google Scholar]
- Transforming Early Childhood in England—UCL Press. Available online: https://www.uclpress.co.uk/products/128464 (accessed on 18 September 2020).
- OECD. OECD Affordable Housing Database. In OECD-Social Policy Division-Directorate of Employment, Labour and Social Affairs; OECD: Paris, France, 2022; Available online: http://oe.cd/ahd (accessed on 3 October 2021).
- Rosenthal, D.M.; Lewis, C.; Heys, M.; Schoenthaler, A.M.; Ucci, M.; Hayward, A.; Lakhanpaul, M. Barriers to Optimal Health for Under 5s Experiencing Homelessness and Living In Temporary Accommodation in High-Income Countries: A Scoping Review. Ann. Public Health Res. 2021, 8, 1103. Available online: https://www.jscimedcentral.com/PublicHealth/publichealth-8-1103.pdf (accessed on 3 October 2021).
- Speak, S. The State of Homelessness in Developing Countries. 2019. Available online: https://www.un.org/development/desa/dspd/wp-content/uploads/sites/22/2019/05/SPEAK_Suzanne_Paper.pdf (accessed on 19 January 2022).
- National Institute of Statistics, Ministry of Planning Cambodia. Estimation Of Homeless Children in Seven Cities in Cambodia; National Institute of Statistics: Phnom Penh, Cambodia, 2017; Available online: http://www.cpcnetwork.org/wp-content/uploads/2017/01/Estimation-of-Homeless-Children-Across-Seven-Cities-in-Cambodia.pdf (accessed on 13 January 2022).
- UNDESA Voice. First-Ever United Nations Resolution on Homelessness | DISD. Available online: https://www.un.org/development/desa/dspd/2020/03/resolution-homelessness/ (accessed on 13 January 2022).
- The Economic and Social Council. E/RES/2020/7, Affordavle Housing and Social Protection Systems for All to Address Homelessness; United Nations: New York, NY, USA, 2020; Available online: https://undocs.org/E/RES/2020/7 (accessed on 13 January 2022).
- Zima, B.T.; Wells, K.B.; Freeman, H.E. Emotional and behavioral problems and severe academic delays among sheltered homeless children in Los Angeles County. Am. J. Public Health 1994, 84, 260–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vostanis, P.; Grattan, E.; Cumella, S. Mental health problems of homeless children and families: Longitudinal study. BMJ 1998, 316, 899–902. [Google Scholar] [CrossRef] [Green Version]
- Jetelina, K.K.; Reingle Gonzalez, J.; Clutter, M.O.; Sanders, C.; Baidhya, S.; Schulte, M.C.; Tsai, R. Unmet physical and mental healthcare needs of children with a history of familial homelessness and unstable housing. J. Soc. Distress Homeless 2018, 27, 135–140. [Google Scholar] [CrossRef]
- Cooper, C. Citizen Science: How Ordinary People Are Changing the Face of Discovery; Duckworth Publishers: London, UK, 2017; ISBN 9780715652346. [Google Scholar]
- Haklay, M.; Motion, A.; Balázs, B.; Kieslinger, B.; Greshake Tzovaras, B.; Nold, C.; Dörler, D.; Fraisl, D.; Riemenschneider, D.; Heigl, F.; et al. ECSA’s Characteristics of Citizen Science. Zenodo 2020. [Google Scholar] [CrossRef]
- United States Environmental Protection Agency. Ports Primer: 8.2 Citizen Science Projects. Available online: https://www.epa.gov/community-port-collaboration/ports-primer-82-citizen-science-projects (accessed on 15 July 2021).
- Gearheard, S.; Aporta, C.; Aipellee, G.; O’Keefe, K. The Igliniit project: Inuit hunters document life on the trail to map and monitor arctic change. Can. Geogr. 2011, 55, 42–55. [Google Scholar] [CrossRef]
- Den Broeder, L.; Devilee, J.; Van Oers, H.; Schuit, A.J.; Wagemakers, A. Citizen Science for public health. Health Promot. Int. 2018, 33, 505–514. [Google Scholar] [CrossRef]
- PatientsLikeMe. PatientsLikeMe Live Better, Together! Available online: https://www.patientslikeme.com/ (accessed on 13 November 2021).
- Snik, F.; Rietjens, J.H.H.; Apituley, A.; Volten, H.; Mijling, B.; Di Noia, A.; Heikamp, S.; Heinsbroek, R.C.; Hasekamp, O.P.; Smit, J.M.; et al. Mapping atmospheric aerosols with a citizen science network of smartphone spectropolarimeters. Geophys. Res. Lett. 2014, 41, 7351–7358. [Google Scholar] [CrossRef]
- UCL Research Ethics—UCL—University College London. Applying to the UCL REC. Available online: https://www.ucl.ac.uk/research-ethics/ethical-approval/applying-ucl-rec (accessed on 27 March 2020).
- Unicef Module 1: Understanding the Social Ecological Model (SEM) and Communication for Development (C4D). Social Ecological Model. Available online: https://nanopdf.com/download/understanding-the-social-ecological-model-and_pdf (accessed on 14 January 2022).
- Barton, H.; Grant, M. A health map for the local human habitat. J. R. Soc. Promot. Health 2006, 126, 252–253. [Google Scholar] [CrossRef]
- Senabre Hidalgo, E.; Perelló, J.; Becker, F.; Bonhoure, I.; Legris, M.; Cigarini, A. Participation and Co-creation in Citizen Science. In The Science of Citizen Science; Springer: Cham, Switzerland, 2021; pp. 199–218. ISBN 978-3-030-58278-4. Available online: https://link.springer.com/chapter/10.1007/978-3-030-58278-4_11 (accessed on 22 January 2022).
- Bekhet, A.K.; Zauszniewski, J.A. Methodological Triangulation: An Approach to Understanding Data. Nurse Res. 2012, 20, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Campbell, R.; Goodman-Williams, R.; Feeney, H.; Fehler-Cabral, G. Assessing Triangulation Across Methodologies, Methods, and Stakeholder Groups: The Joys, Woes, and Politics of Interpreting Convergent and Divergent Data. Am. J. Eval. 2018, 41, 125–144. [Google Scholar] [CrossRef]
- Noble, H.; Heale, R. Triangulation in research, with examples. Evid. Based. Nurs. 2019, 22, 67–68. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, L. The Housing Crisis Generation: How Many Children Are Homeless in Britain; Shelter: London, UK, 2018. [Google Scholar]
- Shelter. Homeless in a Pandemic: 253,000 People Are Trapped in Temporary Accommodation; Shelter: London, UK, 2020; Available online: https://england.shelter.org.uk/media/press_release/homeless_in_a_pandemic_253000_people_are_trapped_in_temporary_accommodation_ (accessed on 31 October 2021).
- Trust for London, L.P.P. London Households in Temporary Accommodation. Available online: https://www.trustforlondon.org.uk/data/temporary-accommodation-borough/ (accessed on 25 July 2021).
- ONS. UK Homelessness: 2005 to 2018—Assessment of the Comparability and Coherence of Existing UK Government Data Sources on Homelessness; Office for National Statistics: Newport, UK, 2019. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/housing/articles/ukhomelessness/2005to2018 (accessed on 16 January 2022).
- ECSA (European Citizen Science Association). Ten Principles of Citizen Science; ECSA: Berlin, Germany, 2015. [Google Scholar] [CrossRef]
- WhatsApp LLC WhatsApp. Available online: https://www.whatsapp.com/ (accessed on 14 January 2022).
- HOW TO: Create a Survey in Survey123. 2017, pp. 1–12. Available online: https://schools.esriuk.com/wp-content/uploads/Getting-Started-with-Survey123.pdf (accessed on 14 January 2022).
- Esri ArcGIS ArcGIS Survey123. Available online: https://survey123.arcgis.com/ (accessed on 14 January 2022).
- Stafford Borough Council. Health and Housing Services Housing Health and Safety Rating System: The 29 Hazards. Available online: https://www.staffordbc.gov.uk/housing-health-and-safety-rating-system-the-29-hazards (accessed on 24 August 2021).
- Office of the Deputy Prime Minister. Housing Housing Health and Safety Rating System Enforcement Guidance; Office of the Deputy Prime Minister: London, UK, 2004; ISBN 9781851128464. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/7853/safetyratingsystem.pdf (accessed on 24 August 2021).
- FEANTSA. ETHOS—European Typology of Homelessness and Housing Exclusion; FEANTSA: Brussels, Belgium, 2005; Available online: https://www.feantsa.org/en/toolkit/2005/04/01/ethos-typology-on-homelessness-and-housing-exclusion (accessed on 24 August 2021).
- Kosmala, M.; Wiggins, A.; Swanson, A.; Simmons, B. Assessing data quality in citizen science. Front. Ecol. Environ. 2016, 14, 551–560. [Google Scholar] [CrossRef] [Green Version]
- Maguire, M.; Delahunt, B. Doing a thematic analysis: A practical, step-by-step guide for learning and teaching scholars. All Irel. J. High. Educ. 2017, 9, 3351–3354. [Google Scholar]
- Kingfisher. If Walls Could Talk; Kingfisher: London, UK, 2020; Available online: https://www.kingfisher.com/content/dam/kingfisher/Corporate/Images/Other/Kingfisher%20Unfit%20Housing%20Research%20Report%20UK%20V6_Sireena.pdf (accessed on 14 January 2022).
- Rosenthal, D.; Heys, M.; Schoenthaler, A.; Lewis, C.; Ucci, M.; Hayward, A.; Lakhanpaul, M. 920 Identifying housing-level barriers to optimal health for Under 5s experiencing homelessness: A citizen science approach. Arch. Dis. Child. 2021, 106, 163. [Google Scholar] [CrossRef]
- Adams, J.; Bateman, B.; Becker, F.; Cresswell, T.; Flynn, D.; McNaughton, R.; Oluboyede, Y.; Robalino, S.; Ternent, L.; Sood, B.G.; et al. Triangulation and integration of results. In Effectiveness and Acceptability of Parental Financial Incentives and Quasi-Mandatory Schemes for Increasing Uptake of Vaccinations in Preschool Children: Systematic Review, Qualitative Study and Discrete Choice Experiment; NIHR Journals Library: Southampton, UK, 2015. [Google Scholar]
- Maxwell, J.A. Using Qualitative Methods for Causal Explanation. Field Methods 2016, 16, 243–264. [Google Scholar] [CrossRef]
- OECD. Housing Overcrowding (Indicator). Available online: https://data.oecd.org/inequality/housing-overcrowding.htm (accessed on 29 December 2021).
- Shribman, S.; Billingham, K. Healthy Child Programme: Pregnancy and the First Five Years of Life; COI for Department of Health: London, UK, 2009. [Google Scholar]
- NICE 1 Recommendations | Physical Activity for Children and Young People | Guidance | NICE. Available online: https://www.nice.org.uk/guidance/ph17/chapter/1-Recommendations#definitions (accessed on 29 December 2021).
- Weather in November 2019 in London, England, United Kingdom. Available online: https://www.timeanddate.com/weather/uk/london/historic?month=11&year=2019 (accessed on 24 November 2021).
- Resnik, D.B.; Elliott, K.C.; Miller, A.K. A framework for addressing ethical issues in citizen science. Environ. Sci. Policy 2015, 54, 475–481. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Public Health and the Environment; The Ministry of Health, Welfare and Sport. 10 Benefits of Citizen Science | RIVM Magazines 2018. Available online: https://magazines.rivm.nl/en/2018/10/citizen-science/10-benefits-citizen-science (accessed on 10 November 2021).
- Holdcroft, A. Gender bias in research: How does it affect evidence based medicine? J. R. Soc. Med. 2007, 100, 2–3. [Google Scholar] [CrossRef]
- Burchard, E.G. Medical research: Missing patients. Nature 2014, 513, 301–302. [Google Scholar] [CrossRef] [Green Version]
- Resnik, D.B. Scientific Research and the Public Trust. Sci. Eng. Ethics 2010, 17, 399–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danielsen, F.; Burgess, N.D.; Balmford, A. Monitoring Matters: Examining the Potential of Locally-based Approaches. Biodivers. Conserv. 2005, 14, 2507–2542. [Google Scholar] [CrossRef]
- Riesch, H.; Potter, C. Citizen science as seen by scientists: Methodological, epistemological and ethical dimensions. Public Underst. Sci. 2014, 23, 107–120. [Google Scholar] [CrossRef] [PubMed]
- Garrett, M.H.; Rayment, P.R.; Hooper, M.A.; Abramson, M.J.; Hooper, B.M. Indoor airborne fungal spores, house dampness and associations with environmental factors and respiratory health in children. Clin. Exp. Allergy 1998, 28, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Hägerhed-Engman, L.; Sigsgaard, T.; Samuelson, I.; Sundell, J.; Janson, S.; Bornehag, C.G. Low home ventilation rate in combination with moldy odor from the building structure increase the risk for allergic symptoms in children. Indoor Air 2009, 19, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Tischer, C.G.; Hohmann, C.; Thiering, E.; Herbarth, O.; Müller, A.; Henderson, J.; Granell, R.; Fantini, M.P.; Luciano, L.; Bergström, A.; et al. Meta-analysis of mould and dampness exposure on asthma and allergy in eight European birth cohorts: An ENRIECO initiative. Allergy 2011, 66, 1570–1579. [Google Scholar] [CrossRef]
- Mendell, M.J.; Mirer, A.G.; Cheung, K.; Douwes, J.; Sigsgaard, T.; Bønløkke, J.; Meyer, H.W.; Hirvonen, M.R.; Roponen, M. Health Effects Associated with Dampness and Mould—WHO Guidelines for Indoor Air Quality—NCBI Bookshelf. Available online: https://www.ncbi.nlm.nih.gov/books/NBK143940/ (accessed on 11 December 2021).
- Doggett, S.L.; Dwyer, D.E.; Peñas, P.F.; Russell, R.C. Bed Bugs: Clinical Relevance and Control Options. Clin. Microbiol. Rev. 2012, 25, 164–192. [Google Scholar] [CrossRef] [Green Version]
- Oudgenoeg-Paz, O.; Atun-Einy, O.; van Schaik, S.D.M. Two Cultural Models on Infant Motor Development: Middle Class Parents in Israel and the Netherlands. Front. Psychol. 2020, 11, 119. [Google Scholar] [CrossRef]
- Hillard, P.J.A. Practical Pediatric and Adolescent Gynecology. In Developmental Delay: Chapter 28; Allen, L., Ornstein, M., Eds.; John Wiley and Sons, Ltd.: Hoboken, NJ, USA, 2013. [Google Scholar] [CrossRef]
- Orton, E.; Kendrick, D.; West, J.; Tata, L.J. Persistence of Health Inequalities in Childhood Injury in the UK; A Population-Based Cohort Study of Children under 5. PLoS ONE 2014, 9, e111631. [Google Scholar] [CrossRef]
- Children’s Commissioner. Bleak Houses: Tackling the Crisis of Family Homelessness in England; Children’s Commissioner: London, UK, 2019. [Google Scholar]
- Riley, R.; Johnson, T.; Pearson, L. An audit into homeless families in temporary accommodation. Br. J. Community Nurs. 2001, 6, 18–25. [Google Scholar] [CrossRef]
- Croft, L.A.; Marossy, A.; Wilson, T.; Atabong, A. A building concern? The health needs of families in temporary accommodation. J. Public Health 2021, 43, 581–586. [Google Scholar] [CrossRef] [PubMed]
- The Young People’s Health Partnership; Homeless Link; Public Health England; The Health & Wellbeing Alliance; The Queen’s Nursing Institute. Addressing Health Inequalities in Homeless Children, Young People and Families A Toolkit for Public Health Nurses 2 Addressing Health Inequalities in Homeless Children, Young People and Families A Toolkit for Public Health Nurses KEY FACTS i Contents; VSCE Health & Wellbeing Alliance: London, UK, 2018. [Google Scholar]
- Shelter England. Shelter Legal England—Suitability of Homelessness Accommodation. Available online: https://england.shelter.org.uk/professional_resources/legal/homelessness_applications/offers_and_suitability_of_accommodation_for_homeless_applicants/suitability_of_homelessness_accommodation (accessed on 22 August 2021).
- Legislation.gov.uk Housing Act 1996. Available online: https://www.legislation.gov.uk/ukpga/1996/52/part/VII (accessed on 22 August 2021).
- Department for Levelling Up, Housing and Communities. Chapter 17: Suitability of Accommodation—Homelessness Code of Guidance for Local Authorities—Guidance; Department for Levelling Up, Housing and Communities: London, UK, 2018. [Google Scholar]
- Ministry of Housing, Communities & Local Government. Homelessness Code of Guidance for Local Authorities; Ministry of Housing, Communities & Local Government: London, UK, 2018. [Google Scholar]
- Farmer, T.; Robinson, K.; Elliott, S.J.; Eyles, J. Developing and implementing a triangulation protocol for qualitative health research. Qual. Health Res. 2006, 16, 377–394. [Google Scholar] [CrossRef] [PubMed]
- Fiske, A.; Prainsack, B.; Buyx, A. Meeting the needs of underserved populations: Setting the agenda for more inclusive citizen science of medicine. J. Med. Ethics 2019, 45, 617–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgan, A.M.; Lifshay, J. Community Engagement in Public Health; Contra Costa Health Services Public Health Division: Martinez, CA, USA, 2006; pp. 1–8. Available online: https://cchealth.org/public-health/pdf/community_engagement_in_ph.pdf (accessed on 3 January 2022).
- Cappuccio, F.P.; Barbato, A.; Kerry, S.M. Hypertension, diabetes and cardiovascular risk in ethnic minorities in the UK. Br. J. Diabetes 2016, 3, 286–293. [Google Scholar] [CrossRef]
- Khan, J.M.; Beevers, G.; Jawad, D.; Khan, M. Management of hypertension in ethnic minorities. Heart 2005, 91, 1105–1109. [Google Scholar] [CrossRef] [Green Version]
- Swope, C.B.; Hernández, D. Housing as a determinant of health equity: A conceptual model. Soc. Sci. Med. 2019, 243, 112571. [Google Scholar] [CrossRef]
- World Health Organization. Health Promotion Glossary of Terms 2021; World Health Organization: Geneva, Switzerland, 2021; pp. 1–44. ISBN 9789240038349. [Google Scholar]




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Description | Observation Data Collected |
|---|---|
|
|
| Inclusion Criteria |
|---|
| • Be a service-user of the charity |
| • Be in temporary or insecure accommodation * at the time of the study |
| • Be staying in London in a Newham or non-Newham postcode |
| • Pregnant and/or mother of children aged <5 years |
| • Ability to communicate in English |
| • Be willing to send/receive text messages |
| • Be willing to have a house visit by the researcher |
| • Be willing to collect data on a mobile app |
| • Be >16 years of age |
| Exclusion Criteria |
| • Refuse or are unable to provide informed consent |
| • Father of children aged <5 years |
| • Have significant psychiatric comorbidity, cognitive impairment, which may impair ability to provide informed consent (as documented in The Magpie Project’s client records) |
| • Plan to discontinue support and services at the charity within the study period |
| Thematic Category | HHSRS Hazard Category and Description | Health Effects (Taken from HHSRS) | House Visits | Participant Surveys | Collaborative Meetings |
|---|---|---|---|---|---|
| I. Overcrowding and Shared Facilities | 11. Crowding and space Hazards associated with lack of space for living, sleeping, and normal household or family life | -Psychological distress and mental disorders, increased risk of hygiene issues, accidents, and personal space and privacy compromised. -Increased risk of infection (e.g., COVID-19) | + | + | + |
| 13. Lighting Threats to physical and mental health associated with inadequate natural or artificial light, including the psychological effects associated with the view from the property through glazing | Depression and psychological effects due to lack of natural light. Eye strain from glare and inadequate light | + | + | NA | |
| 14. Noise Threats to physical and mental health due to exposure to noise within the property or within its curtilage | Psychological and physiological changes resulting from lack of sleep, poor concentration, headaches, and anxiety | + | NA | + | |
| 17. Personal hygiene, sanitation, and drainage Threats of infections and threat to mental health associated with personal hygiene, including personal and clothes washing facilities, sanitation, and drainage | Stomach and intestinal disease, skin infections, and depression | + | + | + | |
| II. Dampness/Mold Growth | 1. Damp and mold growth Health threats due to dust mites, mold or fungal including mental and social wellbeing health threats associated with damp, humid, and moldy conditions | Allergies, asthma, effects of toxins from mold and fungal infections | + | + | + |
| III. Poor/Inadequate Kitchen/toilet Facilities | 16. Food safety Threats of infection from poor provision and facilities to store, prepare, and cook food | Stomach and intestinal disease, diarrhea, vomiting, stomach upset, and dehydration | + | + | + |
| 19. Falls associated with baths Falls associated with a bath, shower, or similar facility | Physical injuries: cuts, lacerations, swellings, and bruising | + | + | NA | |
| IV. Infestations/Vermin | 15. Domestic hygiene, pests, and refuse Health hazards due to poor design, layout, and construction, making it hard to keep clean and hygienic, attracting pests, and inadequate and unhygienic provision for storing household waste | Stomach and intestinal disease, infection, asthma, allergies, disease from rats, and physical hazards | + | + | + |
| V. Structural Problems/Disrepair | 26. Collision and entrapment Risks of physical injuries from trapping body parts in architectural features such as trapping fingers in doors and windows and colliding with objects such as windows, doors, and low ceilings | Physical injuries such as cuts and bruising to the body | + | + | + |
| 29. Structural collapse and falling elements ** The threat of the dwelling collapsing, or part of the fabric being displaced or falling due to inadequate fixing or disrepair or as a result of adverse weather conditions | Physical injuries | + | + | + | |
| VI. Unsafe Electrics | 23. Electrical hazards Hazards from electric shock and electricity burns | Electric shock and burns | + | + | + |
| 24. Fire Threats to health from exposure to uncontrolled fire and associated smoke. It includes injuries from clothing catching fire, a common injuring when trying to put a fire out | Burns, being overcome by smoke, or death | + | + | + | |
| 25. Flames, hot surfaces, and materials Burns or injuries caused by contact with a hot flame or fire, hot objects, and non-water-based liquids. Scalds caused by contact with hot liquids and vapors | Burns, scalds, permanent scarring, and death | + | + | NA | |
| VII. Excessively Cold Due to Inadequate Temperature Regulation | 2. Excess cold ** Threats to health from cold indoor temperatures. A healthy indoor temperature is 18 to 21 °C | -Respiratory conditions: flu, pneumonia, and bronchitis -Cardiovascular conditions: heart attacks and strokes | + | + | + |
| VIII. Unsafe Surfaces That Risk Causing Trips or Falls | 20. Falls on the level surfaces Falls on any level surface such as floor, yards, and paths, including falls associated with trip steps, thresholds, or ramps where the change in level is less than 300 mm | Physical injuries: bruising, fractures, head, brain, and spinal injuries | + | + | NA |
| 21. Falls associated with stairs and steps Falls associated with stairs and ramps where the change in level is greater than 300 mm. It includes internal stairs or ramps within a property, external steps or ramps associated with the property, access to the property and to shared facilities or means of escape from fire and falls over stairs, ramp or step guarding | Physical injuries: bruising, fractures, head, brain, and spinal injuries | + | + | + | |
| 22. Falls between levels Falls from one level to another, inside or outside a dwelling where the difference is more than 300 mm. Including falls from balconies, landings, or out of windows | Physical injuries | + | + | + | |
| 28. Ergonomics Threats of physical strain associated with functional space and other features at the dwelling | Strain and sprain injuries | + | + | + |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosenthal, D.M.; Ucci, M.; Heys, M.; Schoenthaler, A.; Lakhanpaul, M.; Hayward, A.; Lewis, C. A Citizen Science Approach to Identifying Indoor Environmental Barriers to Optimal Health for under 5s Experiencing Homelessness in Temporary Accommodation. Int. J. Environ. Res. Public Health 2022, 19, 3976. https://doi.org/10.3390/ijerph19073976
Rosenthal DM, Ucci M, Heys M, Schoenthaler A, Lakhanpaul M, Hayward A, Lewis C. A Citizen Science Approach to Identifying Indoor Environmental Barriers to Optimal Health for under 5s Experiencing Homelessness in Temporary Accommodation. International Journal of Environmental Research and Public Health. 2022; 19(7):3976. https://doi.org/10.3390/ijerph19073976
Chicago/Turabian StyleRosenthal, Diana Margot, Marcella Ucci, Michelle Heys, Antoinette Schoenthaler, Monica Lakhanpaul, Andrew Hayward, and Celine Lewis. 2022. "A Citizen Science Approach to Identifying Indoor Environmental Barriers to Optimal Health for under 5s Experiencing Homelessness in Temporary Accommodation" International Journal of Environmental Research and Public Health 19, no. 7: 3976. https://doi.org/10.3390/ijerph19073976
APA StyleRosenthal, D. M., Ucci, M., Heys, M., Schoenthaler, A., Lakhanpaul, M., Hayward, A., & Lewis, C. (2022). A Citizen Science Approach to Identifying Indoor Environmental Barriers to Optimal Health for under 5s Experiencing Homelessness in Temporary Accommodation. International Journal of Environmental Research and Public Health, 19(7), 3976. https://doi.org/10.3390/ijerph19073976