
The Epidemiology of Injuries in Spanish Rugby Union División de Honor

 , ,
, ,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Statistical Analysis
3. Results
3.1. Anthropometrics and Habits
3.2. Incidence
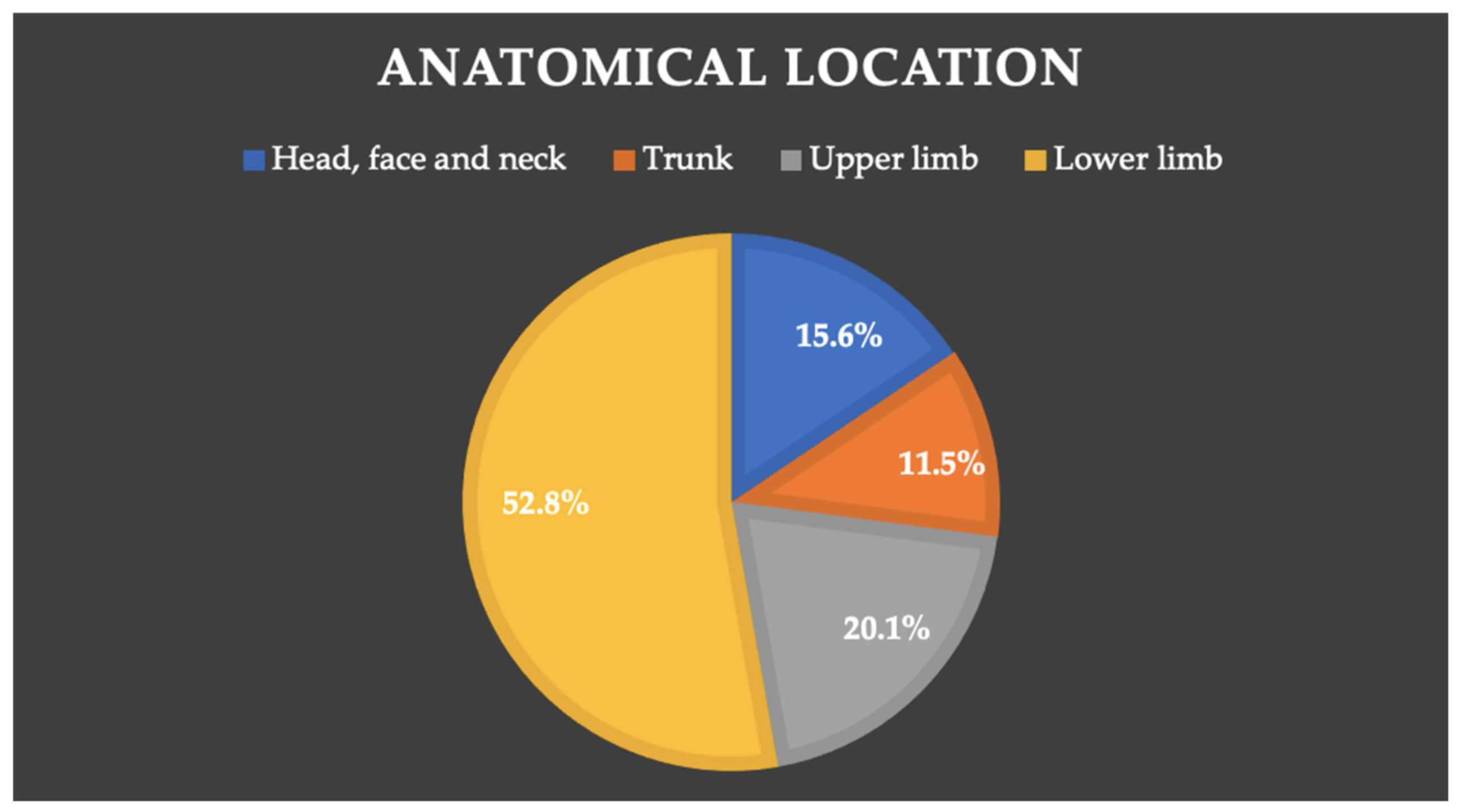
3.3. Anatomical Location
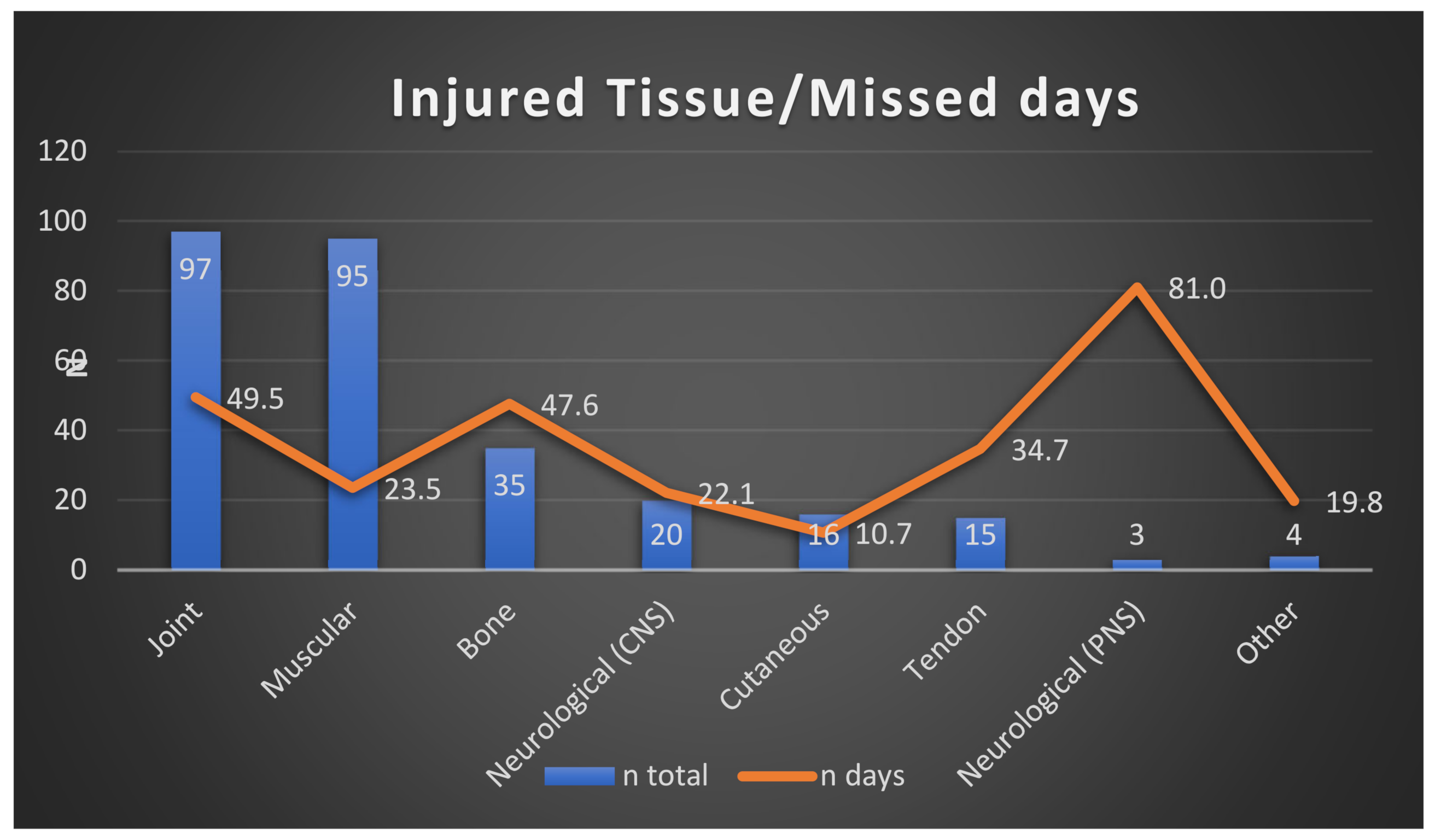
3.4. Injured Tissue
3.5. Injury Type
3.6. Severity
3.7. Injury Mechanism
3.8. Injury Cause
3.9. Place of the Injury
3.10. Time during a Match
3.11. Injury Recurrence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Rugby. World Rugby Year in Review 2019; World Rugby: Dublin, Ireland, 2019; Volume 1, pp. 1–116. [Google Scholar]
- World Rugby. Inside the Meeting that Took Rugby Professional. 2020. Available online: https://www.world.rugby/news/86763/rugby-professional-1995 (accessed on 22 January 2022).
- World Rugby. World Rankings. Men’s Rankings. 2020. Available online: https://www.world.rugby/tournaments/rankings/mru (accessed on 22 January 2022).
- Tier 2 Rugby. Who is Officially Classified as a «Tier 2» Nation? 2014. Available online: http://tier2rugby.blogspot.com/2014/05/who-is-officially-tier-2-nation.html (accessed on 22 January 2022).
- Fuller, C.W.; Laborde, F.; Leather, R.J.; Molloy, M.G. International Rugby Board Rugby World Cup 2007 injury surveillance study. Br. J. Sports Med. 2008, 42, 452–459. [Google Scholar] [CrossRef] [PubMed]
- Willigenburg, N.W.; Borchers, J.R.; Quincy, R.; Kaeding, C.C.; Hewett, T.E. Comparison of Injuries in American Collegiate Football and Club Rugby: A Prospective Cohort Study. Am. J. Sports Med. 2016, 44, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Fuller, C.W.; Sheerin, K.; Targett, S. Rugby World Cup 2011: International Rugby Board injury surveillance study. Br. J. Sports Med. 2013, 47, 1184–1191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuller, C.W.; Taylor, A.; Kemp, S.P.T.; Raftery, M. Rugby World Cup 2015: World Rugby injury surveillance study. Br. J. Sports Med. 2017, 51, 51–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, S.; Trewartha, G.; Kemp, S.P.T.; Brooks, J.H.M.; Fuller, C.W.; Taylor, A.E.; Cross, M.J.; Shaddick, G.; Stokes, K.A. How Much Rugby is Too Much? A Seven-Season Prospective Cohort Study of Match Exposure and Injury Risk in Professional Rugby Union Players. Sports Med. 2017, 47, 2395–2402. [Google Scholar] [CrossRef]
- Cruz-Ferreira, A.M.; Cruz-Ferreira, E.M.; Ribeiro, P.B.; Santiago, L.M.; Taborda-Barata, L. Epidemiology of Time-Loss Injuries in Senior and Under-18 Portuguese Male Rugby Players. J. Hum. Kinet. 2018, 62, 73–80. [Google Scholar] [CrossRef] [Green Version]
- López-Valenciano, A.; Ruiz-Pérez, I.; Garcia-Gómez, A.; Vera-Garcia, F.J.; De Ste Croix, M.; Myer, G.D.; Ayala, F. Epidemiology of injuries in professional football: A systematic review and meta-analysis. Br. J. Sports Med. 2020, 54, 711–718. [Google Scholar] [CrossRef]
- Viviers, P.L.; Viljoen, J.T.; Derman, W. A Review of a Decade of Rugby Union Injury Epidemiology: 2007–2017. Sports Health 2018, 10, 223–227. [Google Scholar] [CrossRef]
- Fuller, C.W. Catastrophic injury in rugby union: Is the level of risk acceptable? Sports Med. 2008, 38, 975–986. [Google Scholar] [CrossRef]
- Chavarro-Nieto, C.; Beaven, M.; Gill, N.; Hébert-Losier, K. Hamstrings injury incidence, risk factors, and prevention in Rugby Union players: A systematic review. Physician Sports Med. 2021, 1–19. [Google Scholar] [CrossRef]
- Yeomans, C.; Kenny, I.C.; Cahalan, R.; Warrington, G.D.; Harrison, A.J.; Purtill, H.; Lyons, M.; Campbell, M.J.; Glynn, L.G.; Comyns, T.M. Injury Trends in Irish Amateur Rugby: An Epidemiological Comparison of Men and Women. Sports Health 2021, 13, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Barden, C.; Bekker, S.; Brown, J.C.; Stokes, K.A.; McKay, C.D. Evaluating the Implementation of Injury Prevention Strategies in Rugby Union and League: A Systematic Review using the RE-AIM Framework. Int. J. Sports Med. 2021, 42, 112–121. [Google Scholar] [CrossRef] [PubMed]
- Ato, M.; López-García, J.J.; Benavente, A. Un sistema de clasificación de los diseños de investigación en psicología. An. Psychol. 2013, 29, 1038–1059. [Google Scholar] [CrossRef] [Green Version]
- Fuller, C.W.; Molloy, M.G.; Bagate, C.; Bahr, R.; Brooks, J.H.M.; Donson, H.; Kemp, S.P.T.; McCrory, P.; McIntosh, A.S.; Meeuwisse, W.H.; et al. Consensus statement on injury definitions and data collection procedures for studies of injuries in rugby union. Br. J. Sports Med. 2007, 41, 328–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Medical Association. Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191. [Google Scholar] [CrossRef] [Green Version]
- Whitehouse, T.; Orr, R.; Fitzgerald, E.; Harries, S.; McLellan, C.P. The Epidemiology of Injuries in Australian Professional Rugby Union 2014 Super Rugby Competition. Orthop. J. Sports Med. 2016, 4, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Schwellnus, M.P.; Thomson, A.; Derman, W.; Jordaan, E.; Readhead, C.; Collins, R.; Morris, I.; Srauss, O.; Van der Linde, E.; Williams, A. More than 50% of players sustained a time-loss injury (>1 day of lost training or playing time) during the 2012 Super Rugby Union Tournament: A prospective cohort study of 17,340 player-hours. Br. J. Sports Med. 2014, 48, 1306–1315. [Google Scholar] [CrossRef] [Green Version]
- Brooks, J.H.M.; Fuller, C.W.; Kemp, S.P.T.; Reddin, D.B. Epidemiology of injuries in English professional rugby union: Part 1 match injuries. Br. J. Sports Med. 2005, 39, 757–766. [Google Scholar] [CrossRef] [Green Version]
- Schneiders, A.G.; Takemura, M.; Wassinger, C.A. A prospective epidemiological study of injuries to New Zealand premier club rugby union players. Phys. Ther. Sport 2009, 10, 85–90. [Google Scholar] [CrossRef]
- Solis-Mencia, C.; Ramos-Álvarez, J.J.; Murias-Lozano, R.; Aramberri, M.; Saló, J.C. Epidemiology of injuries sustained by elite under-18 rugby players. J. Athl. Train. 2019, 54, 1187–1191. [Google Scholar] [CrossRef] [Green Version]
- Tucker, R.; Lancaster, S.; Davies, P.; Street, G.; Starling, L.; de Coning, C.; Brown, J. Trends in player body mass at men’s and women’s Rugby World Cups: A plateau in body mass and differences in emerging rugby nations. BMJ Open Sport Exerc. Med. 2021, 7, e885. [Google Scholar] [CrossRef] [PubMed]
- Fuller, C.W.; Taylor, A.E.; Brooks, J.H.M.; Kemp, S.P.T. Changes in the stature, body mass and age of English professional rugby players: A 10-year review. J. Sports Sci. 2013, 31, 795–802. [Google Scholar] [CrossRef] [PubMed]
- Brooks, J.H.M.; Fuller, C.W.; Kemp, S.P.T.; Reddin, D.B. Epidemiology of injuries in English professional rugby union: Part 2 training injuries. Br. J. Sports Med. 2005, 39, 767–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bathgate, A.; Best, J.; Craig, G.; Jamieson, M. A prospective study of injuries to elite Australian rugby union players. Br. J. Sports Med. 2002, 36, 265–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Full Sample | Backs | Forwards | ||||
|---|---|---|---|---|---|---|
| (n = 258) | (n = 114) | (n = 144) | ||||
| Mean | SD | Mean | SD | Mean | SD | |
| Weight (kg) | 94.0 | 14.2 | 83.2 | 8.8 | 102.5 | 11.6 |
| Height (cm) | 181.6 | 7.2 | 178.5 | 5.9 | 184.1 | 7.1 |
| Age (years) | 25.4 | 4.6 | 24.3 | 3.8 | 26.2 | 5.0 |
| Years playing rugby | 12.4 | 5.5 | 12.3 | 5.1 | 12.4 | 5.8 |
| Training days/week | 4.0 | 0.7 | 4.0 | 0.7 | 4.0 | 0.8 |
| Training hours/day | 2.4 | 0.5 | 2.4 | 0.5 | 2.4 | 0.5 |
| Hours spent training in the gym | 3.5 | 1.6 | 3.5 | 1.6 | 3.6 | 1.5 |
| Hours spent training on natural turf | 5.0 | 2.7 | 5.0 | 2.8 | 5.0 | 2.7 |
| Hours spent training on artificial turf | 0.9 | 1.6 | 1.0 | 1.7 | 0.9 | 1.6 |
| N previous injuries | 1.6 | 1.3 | 1.6 | 1.3 | 1.6 | 1.4 |
| Injured Tissue | Injury Type | n Injury Type | % Injury Type | n Total | % Total |
|---|---|---|---|---|---|
| Joint | 98 | 34.0% | |||
| Sprain/Ligament injury | 80 | 27.8% | |||
| Dislocation/Subluxation | 14 | 4.7% | |||
| Meniscus, cartilage or disk injury | 2 | 0.7% | |||
| Bruises, bumps or contusions | 2 | 0.7% | |||
| Muscular | 95 | 33.0% | |||
| Rupture, strain, tear or cramp | 87 | 30.2% | |||
| Bruises, bumps or contusions | 8 | 2.8% | |||
| Bone | 35 | 12.1% | |||
| Fracture | 21 | 7.3% | |||
| Other bone injuries | 8 | 2.8% | |||
| Bruises, bumps or contusions | 6 | 2.1% | |||
| Neurological (CNS) | 20 | 6.9% | |||
| Concussion | 20 | 6.9% | |||
| Cutaneous | 16 | 5.6% | |||
| Laceration, cut or wound | 15 | 5.2% | |||
| Abrasion or severe scrape | 1 | 0.3% | |||
| Tendon | 16 | 5.6% | |||
| Tendinopathy, tendon rupture or bursitis | 16 | 5.6% | |||
| Neurological (PNS) | 4 | 1.4% | |||
| Spinal compression | 3 | 1.0% | |||
| Peripheral nerve injury | 1 | 0.3% | |||
| Other | 4 | 1.4% | |||
| Dental injury | 2 | 0.7% | |||
| Bruises, bumps or contusions | 2 | 0.7% | |||
| 288 | 100.00% |
| n (%) | Injury Incidence | IC 95% | |
|---|---|---|---|
| Anterior talofibular ligament injury (Ankle) | 35 (12.2%) | 0.5/1000 h | (0.3–0.7) |
| Hamstrings tears | 24 (8.3%) | 0.3/1000 h | (0.2–0.5) |
| Concussion | 20 (6.9%) | 0.3/1000 h | (0.2–04) |
| Low back pain | 19 (6.6%) | 0.3/1000 h | (0.1–0.4) |
| Calf tears | 17 (5.9%) | 0.2/1000 h | (0.1–0.4) |
| Medial collateral ligament injury (Knee) | 15 (5.2%) | 0.2/1000 h | (0.1–0.3) |
| Quadriceps tears | 14 (4.9%) | 0.2/1000 h | (0.1–0.3) |
| Acromioclavicular joint injury (Shoulder) | 13 (4.5%) | 0.2/1000 h | (0.1–0.3) |
| Glenohumeral joint luxation (Shoulder) | 8 (2.8%) | 0.1/1000 h | (0.0–0.1) |
| Fracture of the nose | 5 (1.7%) | 0.1/1000 h | (0.0–0.1) |
| Anterior cruciate ligament injury (Knee) | 5 (1.7%) | 0.1/1000 h | (0.0–0.1) |
| n | Mean (Days) | SD | Minimum | Maximum | |
|---|---|---|---|---|---|
| Without contact | 93 | 28.6 | 40.5 | 2 | 231 |
| Being tackled | 49 | 57.5 | 70.7 | 4 | 266 |
| Tackling | 60 | 38.7 | 55.0 | 2 | 308 |
| Maul | 2 | 52.5 | 23.3 | 36 | 69 |
| Ruck | 25 | 27.4 | 37.3 | 2 | 174 |
| Line-out | 6 | 26.5 | 10.4 | 14 | 41 |
| Scrum | 12 | 42.6 | 59.3 | 2 | 209 |
| Collision | 27 | 27.4 | 28.9 | 2 | 90 |
| Other | 11 | 14.3 | 10.0 | 4 | 37 |
| Total | 285 | 35.6 | 49.8 | 2 | 308 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murias-Lozano, R.; Mendía, L.; Sebastián-Obregón, F.J.S.; Solís-Mencia, C.; Hervás-Pérez, J.P.; Garnacho-Castaño, M.V.; Maté-Muñoz, J.L.; García-Fernández, P. The Epidemiology of Injuries in Spanish Rugby Union División de Honor. Int. J. Environ. Res. Public Health 2022, 19, 3882. https://doi.org/10.3390/ijerph19073882
Murias-Lozano R, Mendía L, Sebastián-Obregón FJS, Solís-Mencia C, Hervás-Pérez JP, Garnacho-Castaño MV, Maté-Muñoz JL, García-Fernández P. The Epidemiology of Injuries in Spanish Rugby Union División de Honor. International Journal of Environmental Research and Public Health. 2022; 19(7):3882. https://doi.org/10.3390/ijerph19073882
Chicago/Turabian StyleMurias-Lozano, Roberto, Luis Mendía, Francisco Javier San Sebastián-Obregón, Cristian Solís-Mencia, Juan Pablo Hervás-Pérez, Manuel Vicente Garnacho-Castaño, José Luis Maté-Muñoz, and Pablo García-Fernández. 2022. "The Epidemiology of Injuries in Spanish Rugby Union División de Honor" International Journal of Environmental Research and Public Health 19, no. 7: 3882. https://doi.org/10.3390/ijerph19073882
APA StyleMurias-Lozano, R., Mendía, L., Sebastián-Obregón, F. J. S., Solís-Mencia, C., Hervás-Pérez, J. P., Garnacho-Castaño, M. V., Maté-Muñoz, J. L., & García-Fernández, P. (2022). The Epidemiology of Injuries in Spanish Rugby Union División de Honor. International Journal of Environmental Research and Public Health, 19(7), 3882. https://doi.org/10.3390/ijerph19073882