
The Second Side of the Coin—Resilience, Meaningfulness and Joyful Moments in Home Health Care Workers during the COVID-19 Pandemic


Abstract
:1. Introduction
1.1. Resources within the Job Demands–Resources Model
1.2. Resilience and Meaning of Work
1.3. Joyful Moments
1.4. Resources in Times of COVID-19
1.5. Home Health Care
1.6. Study Aims
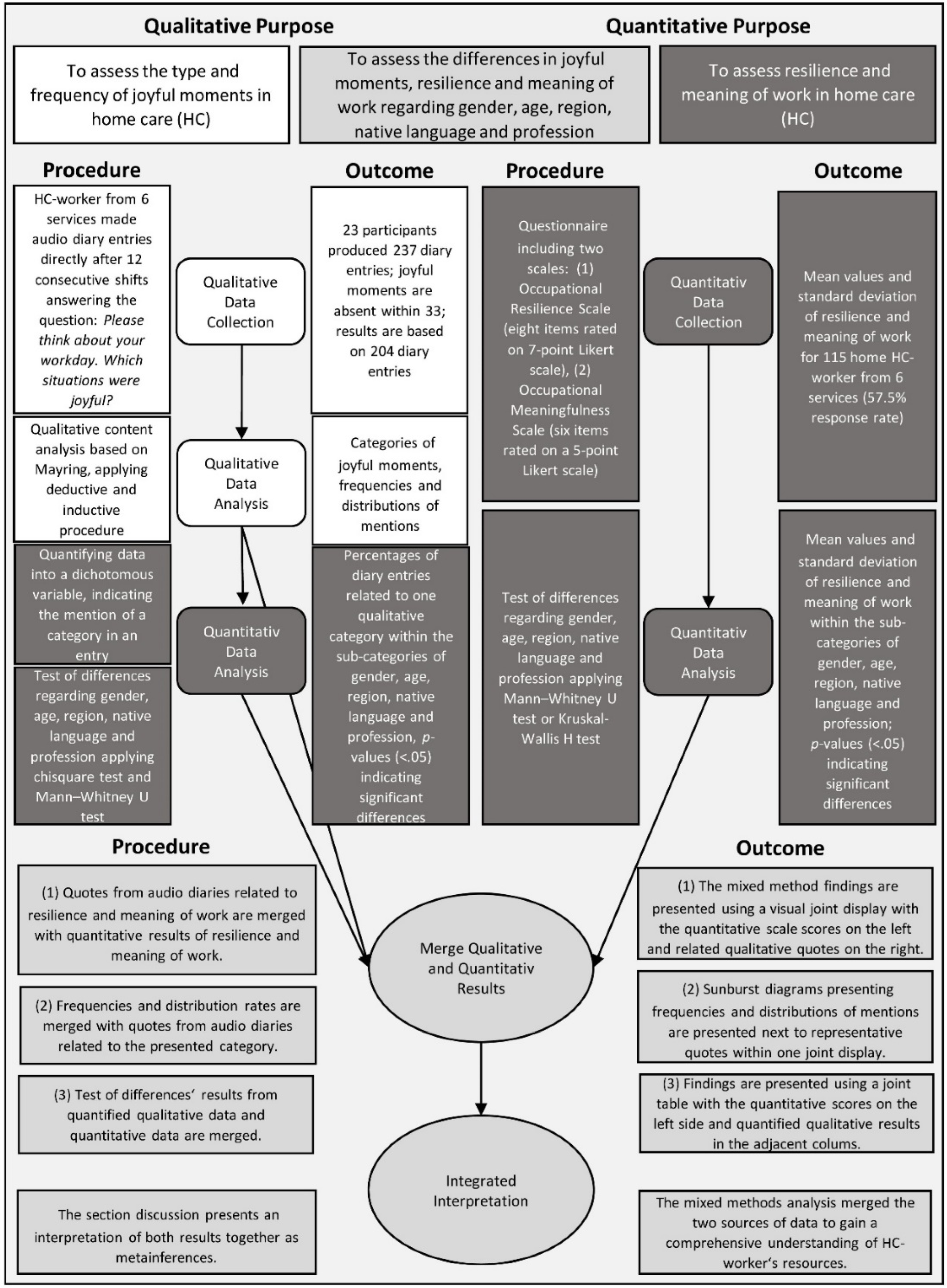
2. Materials and Methods
2.1. Quantitative Methods
2.1.1. Data Collection
2.1.2. Quantitative Measures
2.1.3. Quantitative Statistical Analysis of Quantitative and Qualitative Data
2.2. Qualitative Methods
2.2.1. Data Collection
2.2.2. Data Analysis
3. Results
3.1. Sample
3.2. State of Resilience and Meaning of Work
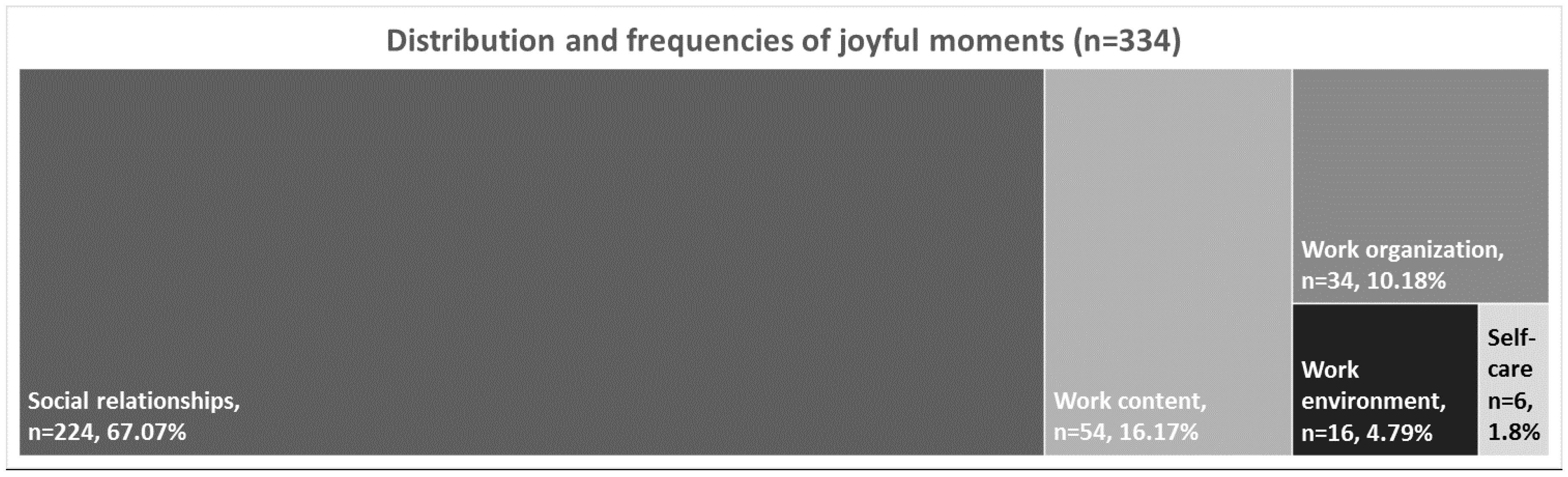
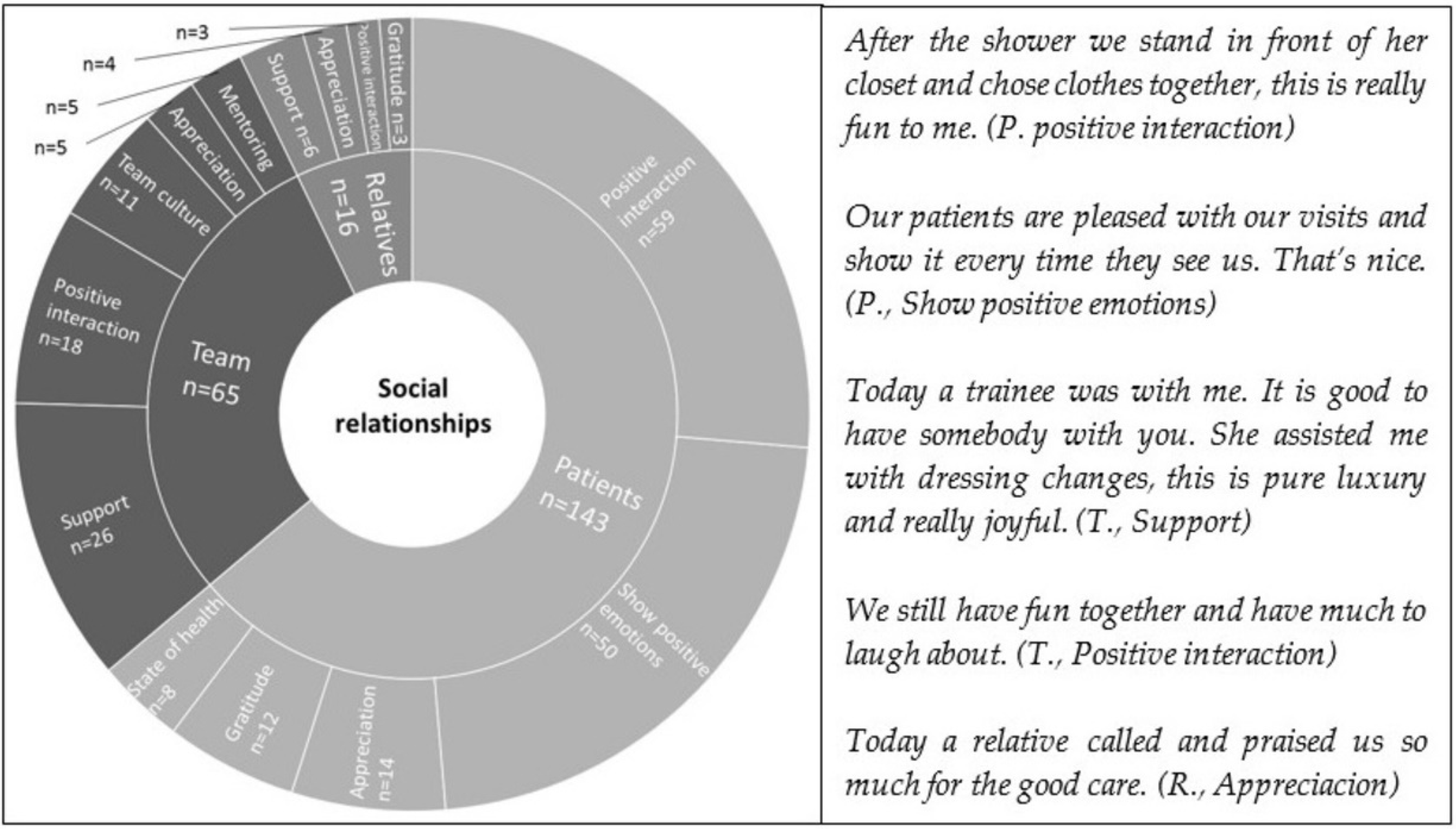
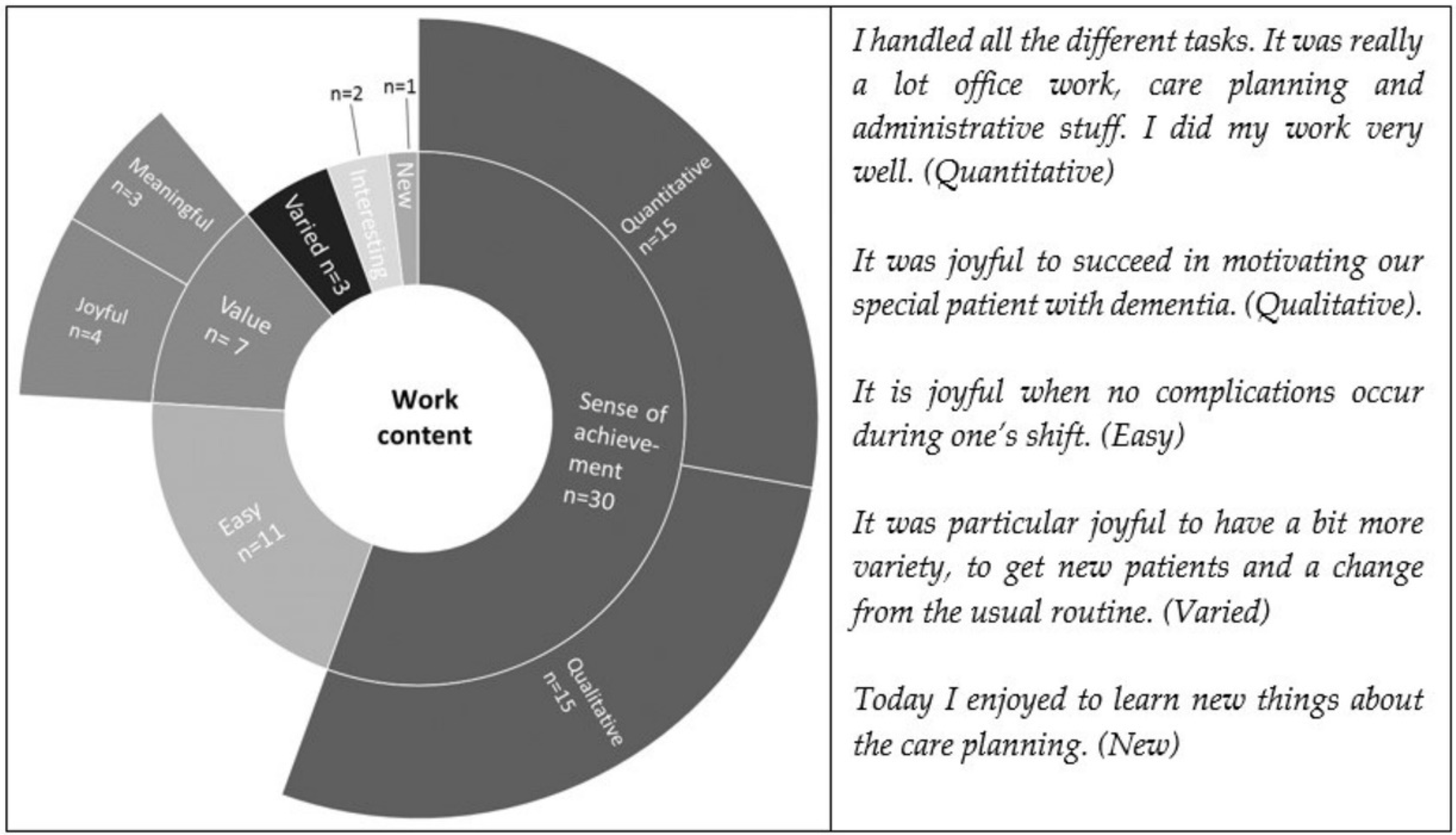
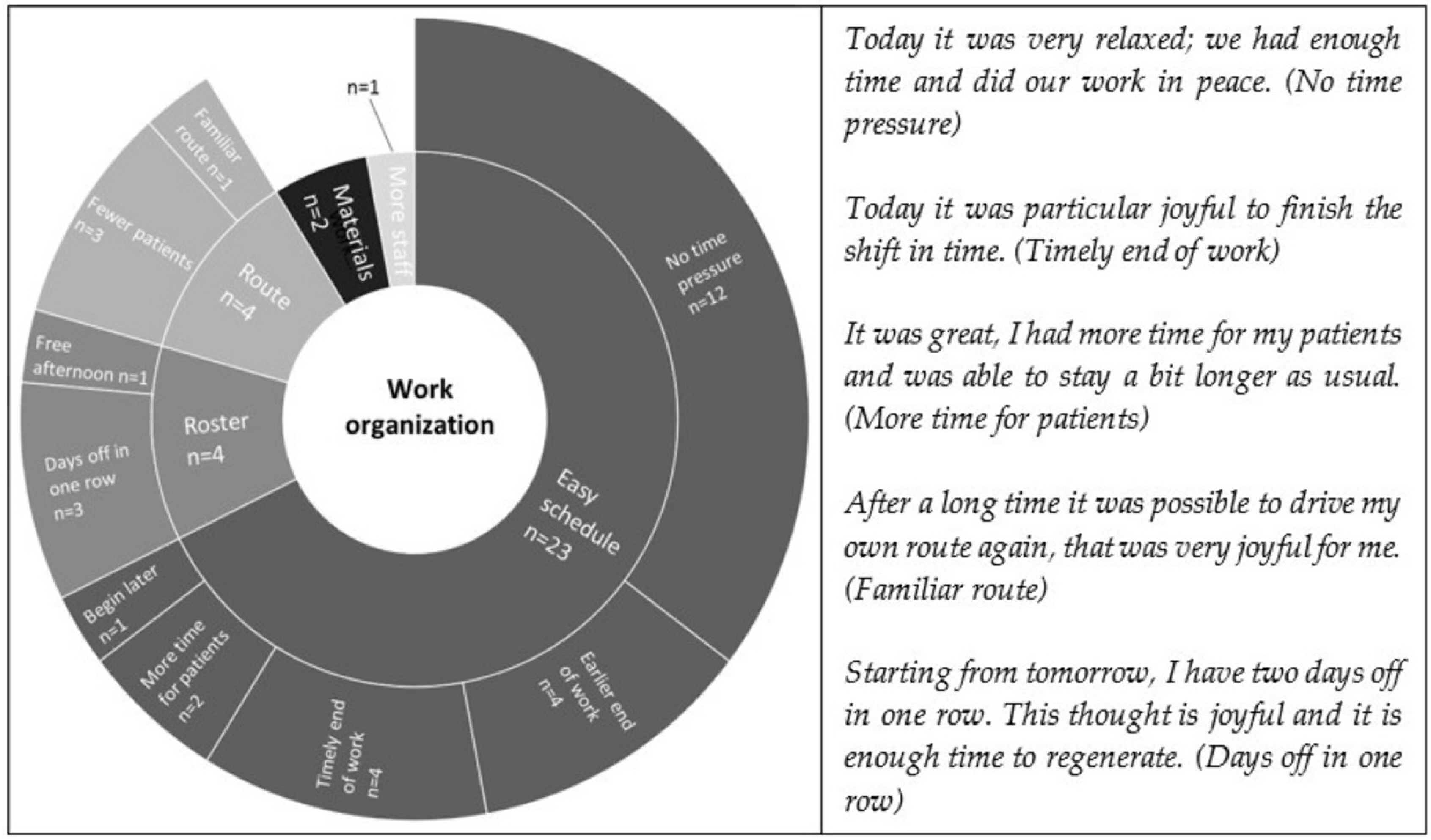
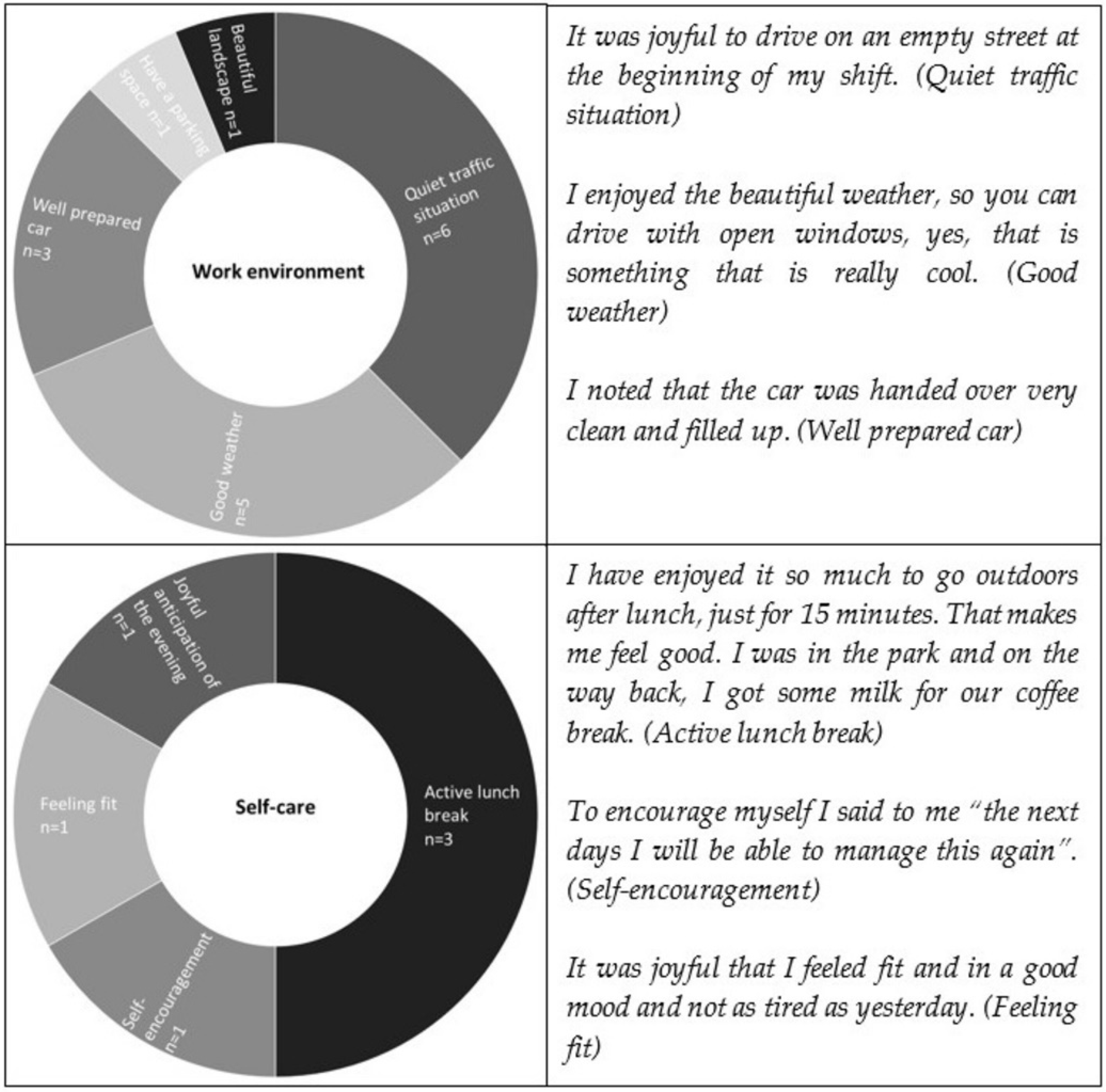
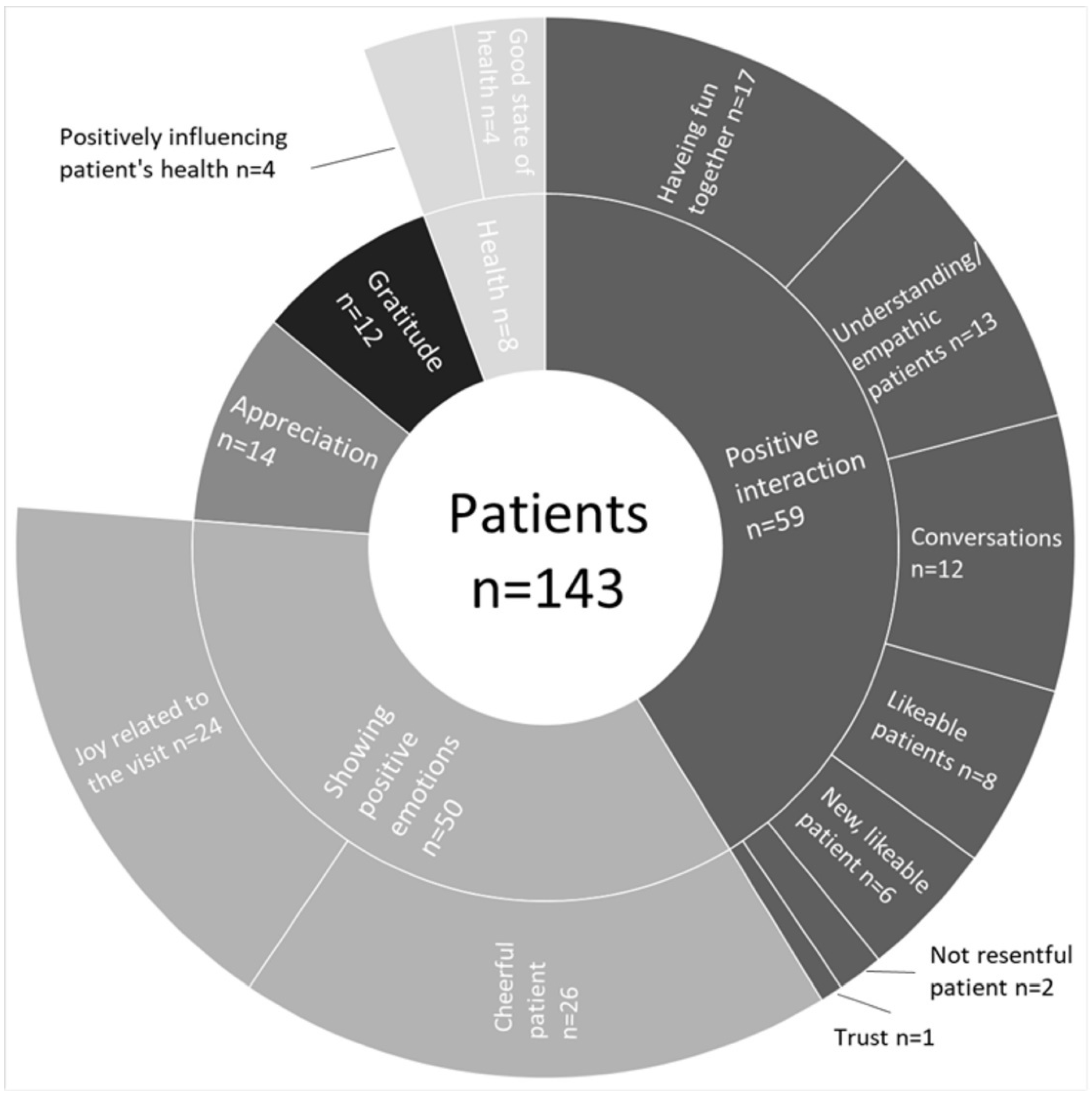
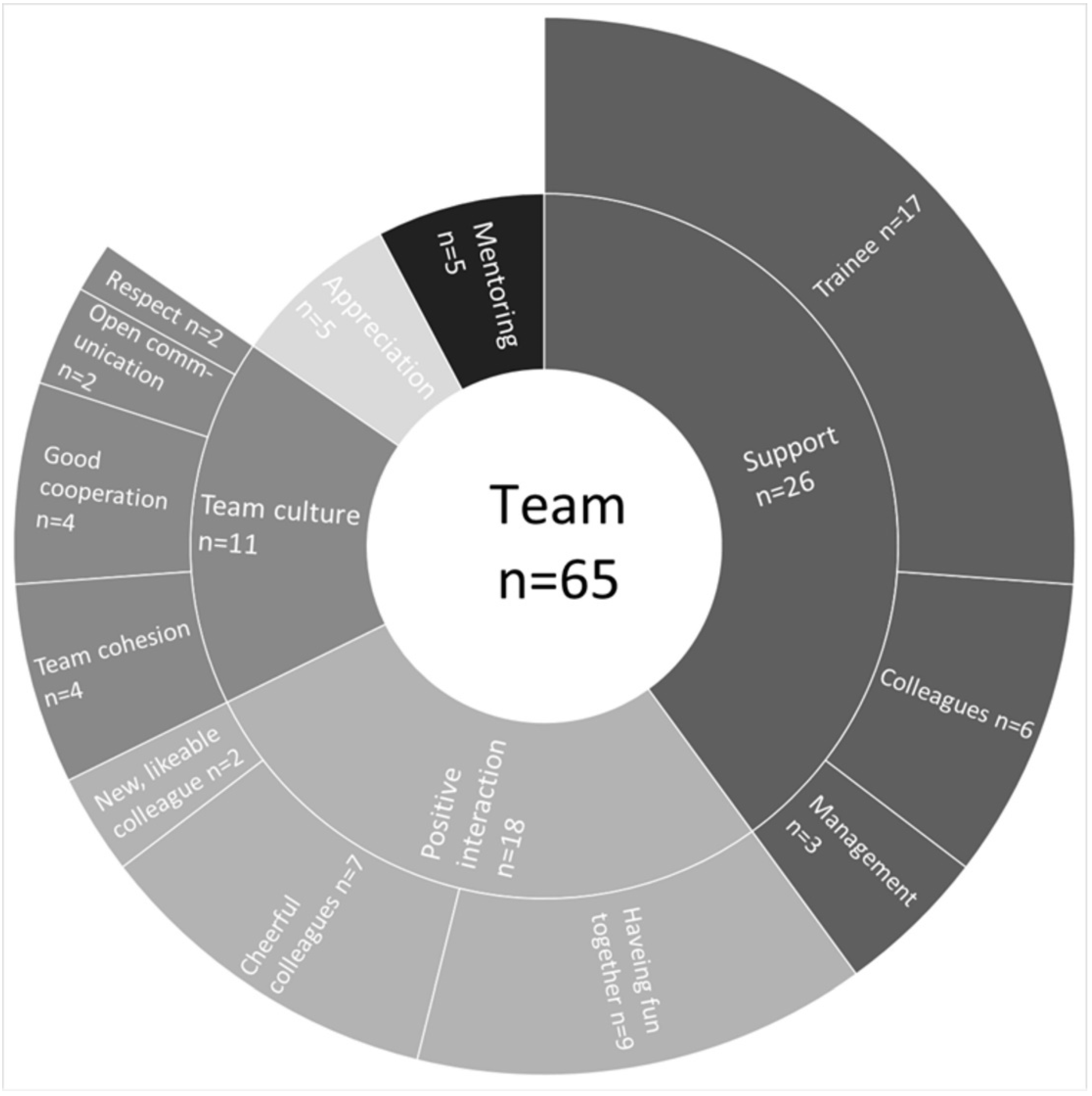
3.3. Types and Frequencies of Joyful Moments
3.4. Differences in Resilience, Meaning of Work and Joyful Moments
4. Discussion
4.1. Resilience and Meaning of Work
4.2. Joyful Moments
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix B

Appendix C

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Quantitative | Qualitative | |||||
|---|---|---|---|---|---|---|---|
| Meaning of Work | Resilience | Social Relationships | Work Content | Work Organization | Work Environment | Self-Care | |
| Gender | U = 413 Z = −3.61 | U = 549 Z = −2.51 | Χ2(1) = 0.46 | Χ2(1) = 4.83 | Χ2(1) = 0.30 | χ2(1) = 2.16 | χ2(1) = 0.64 |
| Age | Χ2(2) = 5.06 | Χ2(2) = 1.14 | U = 3805 Z = −0.21 | U = 2367 Z = −3.66 | U = 2411 Z = −0.66 | U = 1077 Z = −1.63 | U = 498 Z = −0.70 |
| Native language | U = 1139 Z = −0.15 | U = 923 Z = −1.46 | Χ2(1) = 0.89 | Χ2(1) = 1.28 | Χ2(1) = 2.29 | χ2(1) = 0.07 | χ2(1) = 1.81 |
| Region | U = 1120 Z = −2.42 | U = 1153 Z = −1.70 | Χ2(1) = 7.35 | Χ2(1) = 10.1 | Χ2(1) = 0.13 | χ2(1) = 0.62 | χ2(1) = 2.71 |
| Profession | U = 496 Z = −1.64 | U = 612 Z =−0.36 | Χ2(1) = 10.1 | Χ2(1) = 0.23 | χ2(1) = 0.76 | χ2(1) = 2.07 | χ2(1) = 18.85 |
References
- Mittelmark, M.B. Introduction to the Handbook of Salutogenesis. In The Handbook of Salutogenesis; Mittelmark, M.B., Sagy, S., Eriksson, M., Bauer, G.F., Pelikan, J.M., Lindström, B., Espnes, G.A., Eds.; Springer: Berlin/Heidelberg, Germany, 2017; pp. 3–5. [Google Scholar]
- Gomez-Salgado, J.; Navarro-Abal, Y.; Lopez-Lopez, M.J.; Romero-Martin, M.; Climent-Rodriguez, J.A. Engagement, Passion and Meaning of Work as Modulating Variables in Nursing: A Theoretical Analysis. Int. J. Environ. Res. Public Health 2019, 16, 108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cottrell, L. Joy and happiness: A simultaneous and evolutionary concept analysis. J. Adv. Nurs. 2016, 72, 1506–1517. [Google Scholar] [CrossRef] [PubMed]
- Jenny, G.J.; Bauer, G.F.; Forbech Vinje, H.; Vogt, K.; Torp, S. The Application of Salutogenesis to Work. In The Handbook of Salutogenesis; Mittelmark, M.B., Sagy, S., Eriksson, M., Bauer, G.F., Pelikan, J.M.L., Espnes, G.A., Eds.; Springer: Cham, Germany, 2017. [Google Scholar]
- Demerouti, E.; Nachreiner, F. Zum Arbeitsanforderungen-Arbeitsressourcen-Modell von Burnout und Arbeitsengagement—Stand der Forschung. Z. Für Arb. 2018, 73, 119–130. [Google Scholar] [CrossRef] [Green Version]
- Bakker, A.B.; Demerouti, E. Job demands-resources theory: Taking stock and looking forward. J. Occup. Health Psychol. 2017, 22, 273–285. [Google Scholar] [CrossRef]
- Demerouti, E.; Bakker, A.B.; Nachreiner, F.; Schaufeli, W.B. The job demands-resources model of burnout. J. Appl. Psychol. 2001, 86, 499–512. [Google Scholar] [CrossRef]
- Schaufeli, W.B. Applying the Job Demands-Resources model. Organ. Dyn. 2017, 46, 120–132. [Google Scholar] [CrossRef]
- Xanthopoulou, D.; Bakker, A.B.; Dollard, M.F.; Demerouti, E.; Schaufeli, W.B.; Taris, T.W.; Schreurs, P.J.G. When do job demands particularly predict burnout? J. Manag. Psychol. 2007, 22, 766–786. [Google Scholar] [CrossRef] [Green Version]
- Diehl, E.; Rieger, S.; Letzel, S.; Schablon, A.; Nienhaus, A.; Escobar Pinzon, L.C.; Dietz, P. Health and intention to leave the profession of nursing—Which individual, social and organisational resources buffer the impact of quantitative demands? A cross-sectional study. BMC Palliat. Care 2020, 19, 83. [Google Scholar] [CrossRef]
- Van der Heijden, B.; Brown Mahoney, C.; Xu, Y. Impact of Job Demands and Resources on Nurses’ Burnout and Occupational Turnover Intention Towards an Age-Moderated Mediation Model for the Nursing Profession. Int. J. Environ. Res. Public Health 2019, 16, 2011. [Google Scholar] [CrossRef] [Green Version]
- Broetje, S.; Jenny, G.J.; Bauer, G.F. The Key Job Demands and Resources of Nursing Staff: An Integrative Review of Reviews. Front. Psychol. 2020, 11, 84. [Google Scholar] [CrossRef]
- Keyko, K.; Cummings, G.G.; Yonge, O.; Wong, C.A. Work engagement in professional nursing practice: A systematic review. Int. J. Nurs. Stud. 2016, 61, 142–164. [Google Scholar] [CrossRef] [PubMed]
- McVicar, A. Scoping the common antecedents of job stress and job satisfaction for nurses (2000–2013) using the job demands-resources model of stress. J. Nurs. Manag. 2016, 24, E112–E136. [Google Scholar] [CrossRef] [PubMed]
- Seligman, M.E.P.; Csikszentmihalyi, M. Positive Psychology: An Introduction. In Flow and the Foundations of Positive Psychology; Springer: Dordrecht, The Netherlands, 2014. [Google Scholar]
- Tomo, A.; De Simone, S. Using the job demands-resources approach to assess employee well-being in healthcare. Health Serv. Manage. Res. 2019, 32, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Milan, B.; Cano-Vindel, A.; Lopez-Doriga, P.; Medrano, L.A.; Breitbart, W. Meaning of work and personal protective factors among palliative care professionals. Palliat. Support. Care 2019, 17, 381–387. [Google Scholar] [CrossRef] [Green Version]
- Yu, F.; Raphael, D.; Mackay, L.; Smith, M.; King, A. Personal and work-related factors associated with nurse resilience: A systematic review. Int. J. Nurs. Stud. 2019, 93, 129–140. [Google Scholar] [CrossRef]
- Fredrickson, B.L. The role of positive emotions in positive psychology. The broaden-and-build theory of positive emotions. Am. Psychol. 2001, 56, 218–226. [Google Scholar] [CrossRef]
- Windle, G. What is resilience? A review and concept analysis. Rev. Clin. Gerontol. 2010, 21, 152–169. [Google Scholar] [CrossRef]
- Cooper, A.L.; Brown, J.A.; Rees, C.S.; Leslie, G.D. Nurse resilience: A concept analysis. Int. J. Ment. Health Nurs. 2020, 29, 553–575. [Google Scholar] [CrossRef]
- Delgado, C.; Upton, D.; Ranse, K.; Furness, T.; Foster, K. Nurses’ resilience and the emotional labour of nursing work: An integrative review of empirical literature. Int. J. Nurs. Stud. 2017, 70, 71–88. [Google Scholar] [CrossRef]
- Lee, S. A concept analysis of ’Meaning in work’ and its implications for nursing. J. Adv. Nurs. 2015, 71, 2258–2267. [Google Scholar] [CrossRef] [Green Version]
- Malloy, D.C.; Fahey-McCarthy, E.; Murakami, M.; Lee, Y.; Choi, E.; Hirose, E.; Hadjistavropoulos, T. Finding Meaning in the Work of Nursing: An International Study. Online J. Issues Nurs. 2015, 20, 7. [Google Scholar] [CrossRef] [PubMed]
- Schadenhofer, P.; Kundi, M.; Abrahamian, H.; Blasche, G.; Stummer, H.; Kautzky-Willer, A. Job-related meaningfulness moderates the association between over-commitment and emotional exhaustion in nurses. J. Nurs. Manag. 2018, 26, 820–832. [Google Scholar] [CrossRef] [PubMed]
- Gloria, C.T.; Steinhardt, M.A. Relationships Among Positive Emotions, Coping, Resilience and Mental Health. Stress Health 2016, 32, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Gergen Barnett, K.A. In Pursuit of the Fourth Aim in Health Care: The Joy of Practice. Med. Clin. N. Am. 2017, 101, 1031–1040. [Google Scholar] [CrossRef]
- Wilkes, L.; Doull, M.; Ng Chok, H.; Mashingaidze, G. Enjoyment in nursing—Experiences from the clinical milieu. J. Clin. Nurs. 2016, 25, 656–663. [Google Scholar] [CrossRef]
- Galuska, L.; Hahn, J.; Polifroni, E.C.; Crow, G. A Narrative Analysis of Nurses’ Experiences With Meaning and Joy in Nursing Practice. Nurs. Adm. Q 2018, 42, 154–163. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Vizheh, M.; Qorbani, M.; Arzaghi, S.M.; Muhidin, S.; Javanmard, Z.; Esmaeili, M. The mental health of healthcare workers in the COVID-19 pandemic: A systematic review. J. Diabetes Metab. Disord. 2020, 19, 1967–1978. [Google Scholar] [CrossRef]
- Sahebi, A.; Nejati-Zarnaqi, B.; Moayedi, S.; Yousefi, K.; Torres, M.; Golitaleb, M. The prevalence of anxiety and depression among healthcare workers during the COVID-19 pandemic: An umbrella review of meta-analyses. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 107, 110247. [Google Scholar] [CrossRef]
- Mojtahedzadeh, N.; Wirth, T.; Nienhaus, A.; Harth, V.; Mache, S. Job Demands, Resources and Strains of Outpatient Caregivers during the COVID-19 Pandemic in Germany: A Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 3684. [Google Scholar] [CrossRef]
- Lorente, L.; Vera, M.; Peiro, T. Nurses stressors and psychological distress during the COVID-19 pandemic: The mediating role of coping and resilience. J. Adv. Nurs. 2021, 77, 1335–1344. [Google Scholar] [CrossRef] [PubMed]
- Baskin, R.G.; Bartlett, R. Healthcare worker resilience during the COVID-19 pandemic: An integrative review. J. Nurs. Manag. 2021, 29, 2329–2342. [Google Scholar] [CrossRef] [PubMed]
- Huerta-González, S.; Selva-Medrano, D.; López-Espuela, F.; Caro-Alonso, P.; Novo, A.; Rodríguez-Martín, B. The Psychological Impact of COVID-19 on Front Line Nurses: A Synthesis of Qualitative Evidence. Int. J. Environ. Res. Public Health 2021, 18, 2975. [Google Scholar] [CrossRef] [PubMed]
- De Kock, J.H.; Latham, H.A.; Leslie, S.J.; Grindle, M.; Munoz, S.A.; Ellis, L.; Polson, R.; O’Malley, C.M. A rapid review of the impact of COVID-19 on the mental health of healthcare workers: Implications for supporting psychological well-being. BMC Public Health 2021, 21, 104. [Google Scholar] [CrossRef]
- Blanco-Donoso, L.M.; Moreno-Jimenez, J.; Gallego-Alberto, L.; Amutio, A.; Moreno-Jimenez, B.; Garrosa, E. Satisfied as professionals, but also exhausted and worried!!: The role of job demands, resources and emotional experiences of Spanish nursing home workers during the COVID-19 pandemic. Health Soc. Care Community 2022, 30, e148–e160. [Google Scholar] [CrossRef]
- Statistisches-Bundesamt. Pflegebedürftige Nach Versorgungsart. Available online: https://www.destatis.de/DE/Presse/Pressemitteilungen/2020/12/PD20_507_224.html;jsessionid=776D5420EFBD6C101985FE79F4996C51.live742 (accessed on 12 January 2022).
- Statistisches-Bundesamt. 3,4 Millionen Pflege Bedürftige zum Jahresende 2017. Available online: https://www.destatis.de/DE/Presse/Pressemitteilungen/2018/12/PD18_501_224.html (accessed on 17 January 2022).
- Bureau of Labor Statistics, U.S. Department of Labor. Home Health and Personal Care Aides. Available online: https://www.bls.gov/ooh/healthcare/home-health-aides-and-personal-care-aides.htm (accessed on 18 January 2022).
- Kusmaul, N.; Butler, S.; Hageman, S. The Role of Empowerment in Home Care Work. J. Gerontol. Soc. Work 2020, 63, 316–334. [Google Scholar] [CrossRef]
- Jones, C.D.; Bowles, K.H. Emerging Challenges and Opportunities for Home Health Care in the Time of COVID-19. J. Am. Med. Dir. Assoc. 2020, 21, 1517–1518. [Google Scholar] [CrossRef]
- Isfort, M.; Rottländer, R.; Weidner, F.; Tucman, D.; Gehlen, D.; Hylla, J. Pflege-Thermometer 2016. Eine Bundesweite Befragung von Leitungskräften zur Situation der Pflege und Patientenversorgung in der Ambulanten Pflege. Available online: https://www.dip.de/fileadmin/data/pdf/projekte_DIP-Institut/Endbericht_Pflege-Thermometer_2016-MI-2.pdf (accessed on 22 March 2022).
- Treviranus, F.; Mojtahedzadeh, N.; Harth, V.; Mache, S. Psychische Belastungsfaktoren und Ressourcen in der ambulanten Pflege. Zent. Für Arb. Arb. Und Ergon. 2020, 71, 32–37. [Google Scholar] [CrossRef]
- Otto, A.K.; Bischoff, L.L.; Wollesen, B. Work-Related Burdens and Requirements for Health Promotion Programs for Nursing Staff in Different Care Settings: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2019, 16, 3586. [Google Scholar] [CrossRef] [Green Version]
- De Groot, K.; Maurits, E.E.M.; Francke, A.L. Attractiveness of working in home care: An online focus group study among nurses. Health Soc. Care Community 2018, 26, e94–e101. [Google Scholar] [CrossRef] [Green Version]
- Fetters, M.D.; Curry, L.A.; Creswell, J.W. Achieving integration in mixed methods designs-principles and practices. Health Serv. Res. 2013, 48, 2134–2156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curry, N.-S. Mixed Methods in Health Science Research; Sage: Thousand Oaks, CA, USA, 2015. [Google Scholar]
- Fetters, M.D. The Mixed Methods Research Workbook. In Activities for Designing, Implementing, and Publishing Projects; SAGE: Thousand Oaks, CA, USA, 2020. [Google Scholar]
- Soucek, R.; Pauls, N.; Ziegler, M.; Schlett, C. Entwicklung eines Fragebogens zur Erfassung resilienten Verhaltens bei der Arbeit. Wirtschaftspsychologie 2015, 17, 13–22. [Google Scholar]
- May, D.R.; Gilson, R.L.; Harter, L.M. The psychological conditions of meaningfulness, safety and availability and the engagement of the human spirit at work. J. Occup. Organ. Psychol. 2004, 77, 11–37. [Google Scholar] [CrossRef]
- Weckmüller, H.; Wendel, Y.; Schwarz, J. Sinnvolle Arbeit in der Altenpflege. Prävention Und Gesundh. 2019, 15, 43–49. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: New York, NY, USA, 1988. [Google Scholar]
- Cottingham, M.D.; Johnson, A.H.; Erickson, R.J. “I Can Never Be Too Comfortable”: Race, Gender, and Emotion at the Hospital Bedside. Qual. Health Res. 2018, 28, 145–158. [Google Scholar] [CrossRef] [Green Version]
- Gordon, H.J.; Demerouti, E.; Le Blanc, P.M.; Bakker, A.B.; Bipp, T.; Verhagen, M.A.M.T. Individual job redesign: Job crafting interventions in healthcare. J. Vocat. Behav. 2018, 104, 98–114. [Google Scholar] [CrossRef]
- Crozier, S.E.; Cassell, C.M. Methodological considerations in the use of audio diaries in work psychology: Adding to the qualitative toolkit. J. Occup. Organ. Psychol. 2016, 89, 396–419. [Google Scholar] [CrossRef] [Green Version]
- Mayring, P. Qualitative Inhaltsanalyse. Grundlagen und Techniken Qualitative Content Analysis. Basics and Techniques; Beltz: Weinheim, Germany, 2015. [Google Scholar]
- VERBI-Software. MAXQDA—Software für Qualitative Datenanalyse; Consult. Sozialforschung GmbH: Berlin, Germany, 1989–2021. [Google Scholar]
- Pauls, N.; Schlett, C.; Soucek, R.; Ziegler, M.; Frank, N. Resilienz durch Training personaler Ressourcen stärken: Evaluation einer web-basierten Achtsamkeitsintervention. Gruppe. Interaktion. Organisation. Z. Für Angew. Organ. (GIO) 2016, 47, 105–117. [Google Scholar] [CrossRef]
- Kunzelmann, A.; Rigotti, T. How time pressure is associated with both work engagement and emotional exhaustion: The moderating effects of resilient capabilities at work. Ger. J. Hum. Resour. Manag. Z. Für Pers. 2020, 35, 309–336. [Google Scholar] [CrossRef]
- Ang, S.Y.; Uthaman, T.; Ayre, T.C.; Mordiffi, S.Z.; Ang, E.; Lopez, V. Association between demographics and resilience—a cross-sectional study among nurses in Singapore. Int. Nurs. Rev. 2018, 65, 459–466. [Google Scholar] [CrossRef]
- Zheng, Z.; Gangaram, P.; Xie, H.; Chua, S.; Ong, S.B.C.; Koh, S.E. Job satisfaction and resilience in psychiatric nurses: A study at the Institute of Mental Health, Singapore. Int. J. Ment. Health Nurs. 2017, 26, 612–619. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.; Zhou, Y.; Wang, S.; Luo, T.; Huang, M.; Zeng, Y. Exploratory study on resilience and its influencing factors among hospital nurses in Guangzhou, China. Int. J. Nurs. Sci. 2018, 5, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Strandås, M.; Wackerhausen, S.; Bondas, T. Gaming the system to care for patients: A focused ethnography in Norwegian public home care. BMC Health Serv. Res. 2019, 19, 121. [Google Scholar] [CrossRef] [PubMed]
- Galuska, L.A.; Bursch, B. Meaning, Joy, and Critical Care Nurse Well-Being: A Call to Action. Crit. Care Nurs. Clin. N. Am. 2020, 32, 349–367. [Google Scholar] [CrossRef]
- Wilkes, L.; Doull, M.; Ng Chok, H.; Mashingaidze, G. Developing a tool to measure the factors influencing nurses’ enjoyment of nursing. J. Clin. Nurs. 2017, 26, 1854–1860. [Google Scholar] [CrossRef]
- Timonen, V.; Lolich, L. “The Poor Carer”: Ambivalent Social Construction of the Home Care Worker in Elder Care Services. J. Gerontol. Soc. Work 2019, 62, 728–748. [Google Scholar] [CrossRef]
- Siegrist, J. Effort-reward imbalance at work and cardiovascular diseases. Int. J. Occup. Med. Environ. Health 2010, 23, 279–285. [Google Scholar] [CrossRef] [Green Version]
- Schulz, M.; Damkröger, A.; Heins, C.; Wehlitz, L.; Löhr, M.; Driessen, M.; Behrens, J.; Wingenfeld, K. Effort-reward imbalance and burnout among German nurses in medical compared with psychiatric hospital settings. J. Psychiatr. Ment. Health Nurs. 2009, 16, 225–233. [Google Scholar] [CrossRef]
- Gräske, J.; Forbrig, T.A.; Koppe, L.; Urban, S.; Neumann, F.; Boguth, K. Effort-Reward Imbalance, Ability to Work and the Desire for Career Exits: A Cross-sectional Study of Nurses. Gesundheitswesen. Available online: https://www.thieme-connect.com/products/ejournals/abstract/10.1055/a-1706-0629 (accessed on 22 March 2022). [CrossRef]
- Bühler, S.; Buntenbach, A. Arbeitsbedingungen in der Alten- und Krankenpflege, 2018. DGB-Index Gute Arbeit Web Site. Available online: https://index-gute-arbeit.dgb.de/++co++df07ee92-b1ba-11e8-b392-52540088cada (accessed on 22 March 2022).
- Deeg, M.D.; May, D.R. The Benefits to the Human Spirit of Acting Ethically at Work: The Effects of Professional Moral Courage on Work Meaningfulness and Life Well-Being. J. Bus. Ethics 2021, 1–15. [Google Scholar] [CrossRef]
- Hognestad Haaland, G.; Olsen, E.; Mikkelsen, A. The association between supervisor support and ethical dilemmas on Nurses’ intention to leave: The mediating role of the meaning of work. J. Nurs. Manag. 2021, 29, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Haahr, A.; Norlyk, A.; Martinsen, B.; Dreyer, P. Nurses experiences of ethical dilemmas: A review. Nurs. Ethics 2020, 27, 258–272. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, N.D.; Markkanen, P.K.; Kriebel, D.; Galligan, C.J.; Quinn, M.M. “That’s not my job”: A mixed methods study of challenging client behaviors, boundaries, and home care aide occupational safety and health. Am. J. Ind. Med. 2020, 63, 368–378. [Google Scholar] [CrossRef] [PubMed]
- Ris, I.; Schnepp, W.; Mahrer Imhof, R. An integrative review on family caregivers’ involvement in care of home-dwelling elderly. Health Soc. Care Community 2019, 27, e95–e111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heyn, L.; Ellington, L.; Eide, H. An exploration of how positive emotions are expressed by older people and nurse assistants in homecare visits. Patient Educ. Couns. 2017, 100, 2125–2127. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Carrillo, G.; Torres-Marin, J.; Corbacho-Lobato, J.M.; Carretero-Dios, H. The effect of humour on nursing professionals’ psychological well-being goes beyond the influence of empathy: A cross-sectional study. Scand J. Caring. Sci. 2020, 34, 474–483. [Google Scholar] [CrossRef]
- Persson, S.S.; Lindstrom, P.N.; Pettersson, P.; Andersson, I. Workplace relationships impact self-rated health: A survey of Swedish municipal health care employees. Work 2018, 60, 85–94. [Google Scholar] [CrossRef]
- Fjortoft, A.K.; Oksholm, T.; Delmar, C.; Forland, O.; Alvsvag, H. Home-care nurses’ distinctive work: A discourse analysis of what takes precedence in changing healthcare services. Nurs. Inq. 2021, 28, e12375. [Google Scholar] [CrossRef]
- Rohwer, E.; Mojtahedzadeh, N.; Neumann, F.A.; Nienhaus, A.; Augustin, M.; Harth, V.; Zyriax, B.C.; Mache, S. The Role of Health Literacy among Outpatient Caregivers during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 11743. [Google Scholar] [CrossRef]
- Markkanen, P.; Brouillette, N.; Quinn, M.; Galligan, C.; Sama, S.; Lindberg, J.; Karlsson, N. “It changed everything”: The safe Home care qualitative study of the COVID-19 pandemic’s impact on home care aides, clients, and managers. BMC Health Serv. Res. 2021, 21, 1055. [Google Scholar] [CrossRef]
- Sun, N.; Wei, L.; Shi, S.; Jiao, D.; Song, R.; Ma, L.; Wang, H.; Wang, C.; Wang, Z.; You, Y.; et al. A qualitative study on the psychological experience of caregivers of COVID-19 patients. Am. J. Infect. Control 2020, 48, 592–598. [Google Scholar] [CrossRef] [PubMed]
- Rippstein-Leuenberger, K.; Mauthner, O.; Bryan Sexton, J.; Schwendimann, R. A qualitative analysis of the Three Good Things intervention in healthcare workers. BMJ Open 2017, 7, e015826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sexton, J.B.; Adair, K.C. Forty-five good things: A prospective pilot study of the Three Good Things well-being intervention in the USA for healthcare worker emotional exhaustion, depression, work-life balance and happiness. BMJ Open 2019, 9, e022695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Younas, A.; Pedersen, M.; Tayaben, J.L. Review of Mixed-Methods Research in Nursing. Nurs. Res. 2019, 68, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Irvine, F.E.; Clark, M.T.; Efstathiou, N.; Herber, O.R.; Howroyd, F.; Gratrix, L.; Sammut, D.; Trumm, A.; Hanssen, T.A.; Taylor, J.; et al. The state of mixed methods research in nursing: A focused mapping review and synthesis. J. Adv. Nurs. 2020, 76, 2798–2809. [Google Scholar] [CrossRef] [PubMed]



| Variable | Questionnaire (n = 115) | Audio Diary, Participants (n = 23) | Audio Diary, Entries (n = 237) |
|---|---|---|---|
| Age, years, mean ± SD | 47.83 ± 11.72 | 46.70 ± 10.40 | 46.22 ± 10.46 |
| Gender, female (%) | 81.74 | 91.30 | 91.50 |
| Native language, German (%) | 73.04 | 78.26 | 76.70 |
| Region, urban (%) | 46.96 | 47.83 | 49.20 |
| Profession, care worker (%) | 87.83 | 86.96 | 89.40 |
| Variable | Mean ± SD (n) | Quotes |
|---|---|---|
| Resilience (OR) OR—Emotional Coping OR—Comprehensive Planning OR—Positive Reframing OR—Focused Action | 5.52 ± 1.04 (n = 107) 5.46 ± 1.34 (n = 111) 5.96 ± 1.18 (n = 112) 5.17 ± 1.58 (n = 110) 5.55 ± 1.29 (n = 109) | I was able to make my tour just in time, although it was challenging. That was joyful today. We have one special patient. He does not want to take a shower more often than every two or three weeks. Even then, it is difficult and he allows not all of us to help him. Today I managed that he takes a shower. Every time when I showered him successfully, I am proud. That motivates me. I just managed to complete my tasks, although many things happened unexpectedly. |
| Meaning of work (OM) | 4.10 ± 0.92 (n = 111) | Today, all clients were very kind and they expressed their appreciation for the help we deliver. It is a really great feeling when you recognize that you make wonderful and right things. The situation is this, you make, and you are allowed to make, a very meaningful job, which is very fulfilling. A lot of money does not characterize it but meaningfulness. At the end of the day, you go home with a good conscience. You go home with the certainty, with the benevolent certainty, that today you did something good. You give lonely people who stay socially isolated at home a motivating reason to participate in society and help them to live their life in dignity. |
| Variable Heading | Quantitative | Qualitative | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Meaning of Work | Resilience | Social Relationships | Work Content | Work Organization | Work Environment | Self-Care | ||||||||
| Mean (SD) | p-Value | Mean (SD) | p-Value | % | p-Value | % | p-Value | % | p-Value | % | p-Value | % | p-Value | |
| Gender | ||||||||||||||
| Female | 4.26 (0.79) | <0.001 r = 0.34 | 5.67 (0.92) | 0.012 r = 0.24 | 75.5 | 0.496 | 20.1 | 0.028 w = 0.15 | 15.2 | 0.583 | 6.5 | 0.142 | 3.3 | 0.424 |
| Male | 3.3 (1.13) | 4.94 (1.13) | 68.4 | 42.1 | 10.5 | 15.8 | 0.0 | |||||||
| Age | ||||||||||||||
| 20–36 | 3.77 (0.86) | 0.080 | 5.28 (1.24) | 0.565 | 78.3 | 0.834 | 41.3 | <0.001 r = 0.26 | 17.4 | 0.507 | 2.2 | 0.104 | 0.0 | 0.482 |
| 37–53 | 4.15 (0.98) | 5.58 (1.03) | 72.5 | 21.3 | 15.0 | 7.5 | 7.5 | |||||||
| 54–70 | 4.19 (0.89) | 5.55 (0.98) | 75.3 | 11.7 | 13.0 | 10.4 | 0.0 | |||||||
| Native language | ||||||||||||||
| German | 4.11 (0.93) | 0.877 | 5.63 (0.91) | 0.144 | 76.4 | 0.345 | 20.4 | 0.258 | 12.7 | 0.130 | 7.6 | 0.798 | 3.8 | 0.178 |
| Not German | 4.08 (0.90) | 5.21 (1.30) | 69.6 | 28.3 | 21.7 | 6.5 | 0.0 | |||||||
| Region | ||||||||||||||
| Rural | 4.32 (0.74) | 0.015 r = 0.23 | 5.70 (0.89) | 0.089 | 83.2 | 0.007 w = 0.19 | 12.9 | 0.002 w = 0.22 | 13.9 | 0.714 | 5.9 | 0.432 | 1.0 | 0.100 |
| Urban | 3.83 (1.05) | 5.31 (1.18) | 66.7 | 31.4 | 15.7 | 8.8 | 4.9 | |||||||
| Profession | ||||||||||||||
| Care worker | 4.17 (0.85) | 0.101 | 5.53 (1.06) | 0.722 | 78.3 | 0.001 w = 0.22 | 21.7 | 0.631 | 15.6 | 0.383 | 8.3 | 0.150 | 1.1 | <0.001 w = 0.30 |
| Administrative staff | 3.60 (1.23) | 5.43 (1.02) | 47.8 | 26.1 | 8.7 | 0.0 | 17.4 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gebhard, D.; Neumann, J.; Wimmer, M.; Mess, F. The Second Side of the Coin—Resilience, Meaningfulness and Joyful Moments in Home Health Care Workers during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 3836. https://doi.org/10.3390/ijerph19073836
Gebhard D, Neumann J, Wimmer M, Mess F. The Second Side of the Coin—Resilience, Meaningfulness and Joyful Moments in Home Health Care Workers during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(7):3836. https://doi.org/10.3390/ijerph19073836
Chicago/Turabian StyleGebhard, Doris, Julia Neumann, Magdalena Wimmer, and Filip Mess. 2022. "The Second Side of the Coin—Resilience, Meaningfulness and Joyful Moments in Home Health Care Workers during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 7: 3836. https://doi.org/10.3390/ijerph19073836
APA StyleGebhard, D., Neumann, J., Wimmer, M., & Mess, F. (2022). The Second Side of the Coin—Resilience, Meaningfulness and Joyful Moments in Home Health Care Workers during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 19(7), 3836. https://doi.org/10.3390/ijerph19073836