
How Well Are Hand Hygiene Practices and Promotion Implemented in Sierra Leone? A Cross-Sectional Study in 13 Public Hospitals

 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
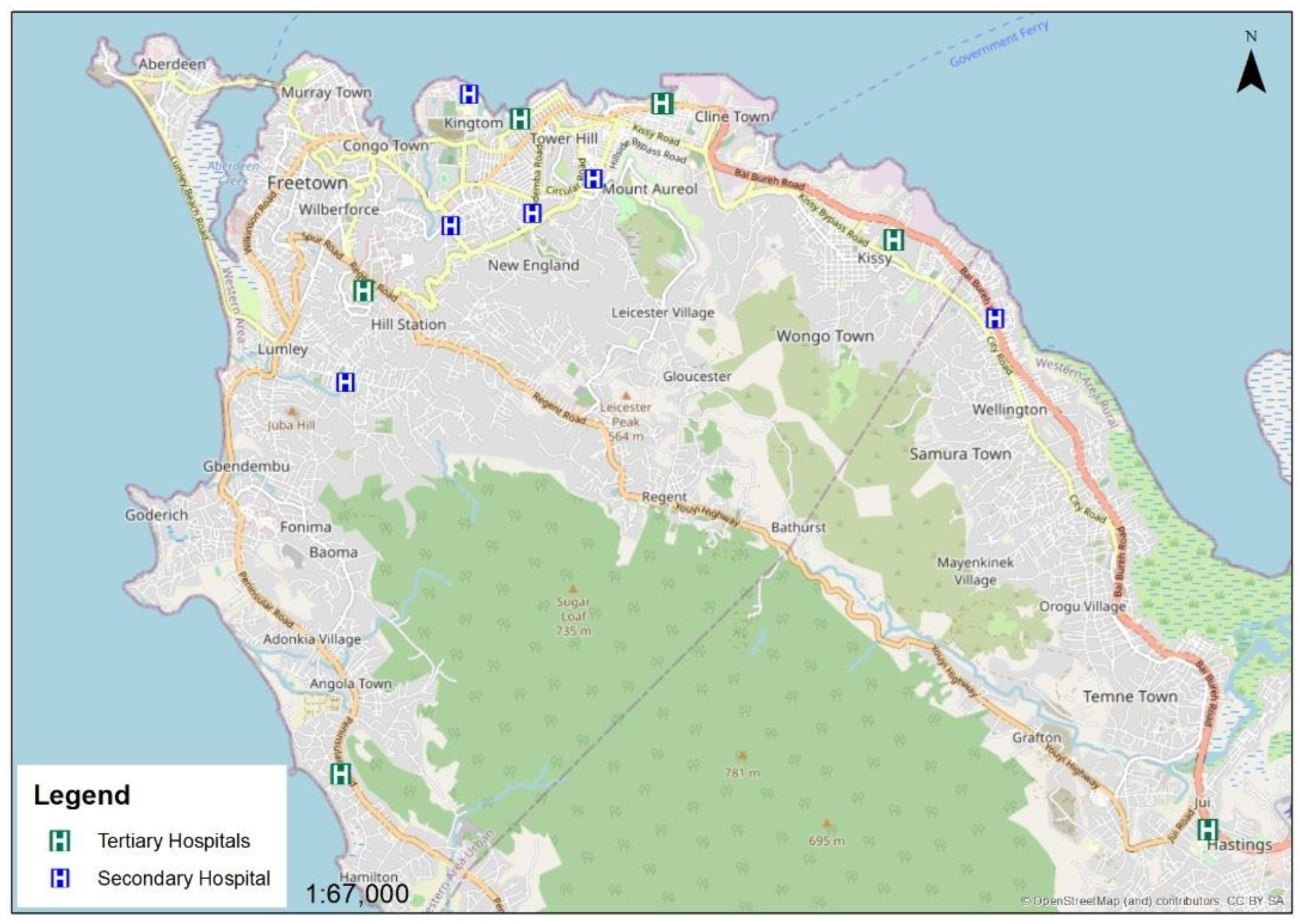
2.2. Study Setting
2.3. Study Population
2.4. Data Variables
2.5. Data Collection, Analysis, and Statistics
3. Results
3.1. Characteristics of the Hospitals
3.2. HHSAF Assessment Scores of the Hospitals
3.2.1. The Total Facility Score Generated from the HHSAF Tool
3.2.2. The Domains Scores of the 2021 HHSAF
3.2.3. The Performance of Hospitals across the Domains
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
Appendix A

{kind=link}
| System Change | |||
|---|---|---|---|
| Question | Answer | Score | N (%) |
| 1.1. How easily available is alcohol-based handrub in your healthcare facility? | Not available | 0 | 0 (0.0) |
| Available facility-wide with continuous supply (with efficacy and tolerability proven) | 10 | 3 (23.1) | |
| Available facility-wide with continuous supply, and at the point of care in the majority of wards (with efficacy and tolerability proven) | 30 | 4 (30.8) | |
| Available facility-wide with continuous supply at each point of care (with efficacy and tolerability proven) | 50 | 6 (46.2) | |
| 1.2. What is the sink: bed ratio? | Less than 1:10 | 0 | 1 (7.7) |
| At least 1:10 in most wards | 5 | 8 (61.5) | |
| At least 1:10 facility-wide and 1:1 in isolation rooms and in intensive care units | 10 | 4 (30.8) | |
| 1.3. Is there a continuous supply of clean, running water? | No | 0 | 5 (38.5) |
| Yes | 10 | 8 (61.5) | |
| 1.4. Is soap available at each sink? | No | 0 | 3 (23.1) |
| Yes | 10 | 10 (76.9) | |
| 1.5. Are single-use towels available at each sink? | No | 0 | 13 (100) |
| Yes | 10 | 0 (0.0) | |
| 1.6. Is there dedicated/available budget for the continuous procurement of hand hygiene products (e.g., alcohol-based handrubs)? | No | 0 | 13 (100) |
| Yes | 10 | 0 (0.0) | |
| 1.7. Is there a realistic plan in place to improve the infrastructure in your healthcare facility? | No | 0 | 13 (100) |
| Yes | 5 | 0 (0.0) | |
| |||
| Question | Answer | Score | N (%) |
| 2.1. a How frequently do your healthcare workers receive training regarding hand hygiene in your facility? | At least once | 5 | 3 (23.1) |
| Regular training for medical and nursing staff, or all professional categories(at least annually) | 10 | 4 (30.8) | |
| Mandatory training for all professional categories at commencement of employment, then ongoing regular training(at least annually) | 20 | 6 (46.2) | |
| 2.1. b Is a process in place to confirm that all healthcare workers complete this training? | No | 0 | 3 (23.1) |
| Yes | 20 | 10 (76.9) | |
| 2.3. Is a professional with adequate skills to serve as trainer for hand hygiene educational programs active within the healthcare facility? | No | 0 | 1 (7.7) |
| Yes | 15 | 12 (92.3) | |
| 2.4. Is a system in place for training and validation of hand hygiene compliance observers? | No | 0 | 1 (7.7) |
| Yes | 15 | 12 (92.3) | |
| 2.5. Is there a dedicated budget that allows for hand hygiene training? | No | 0 | 12 (92.3) |
| Yes | 10 | 1 (7.7) | |
| |||
| Question | Answer | Score | N (%) |
| 3.1. Are regular (at lease annual) ward-based audits undertaken to assess the availability of handrub, soap, single-use towels and other hand hygiene resources? | No | 0 | 11 (84.6) |
| Yes | 10 | 2 (15.4) | |
| 3.2. Is healthcare worker knowledge of the following topics assessed at least annually (e.g., after education session)? | |||
| 3.2. a The indications for hand hygiene | No | 0 | 2 (15.4) |
| Yes | 5 | 11 (84.6) | |
| 3.2. b The correct technique for hand hygiene | No | 0 | 3 (23.1) |
| Yes | 5 | 10 (76.9) | |
| 3.3. Indirect Monitoring of Hand Hygiene Compliance | |||
| 3.3. a Is consumption of alcohol-based handrub monitored regularly (at least every 3 months)? | No | 0 | 4 (30.8) |
| Yes | 5 | 9 (69.2) | |
| 3.3. b Is consumption of soap monitored regularly (at least every 3 months)? | No | 0 | 4 (30.8) |
| Yes | 5 | 9 (69.2) | |
| 3.3. c Is alcohol-based handrub consumption at least 20 L per 1000 patient-days? | No | 0 | 10 (76.9) |
| Yes | 5 | 3 (23.1) | |
| 3.4. Direct Monitoring of Hand Hygiene Compliance | |||
| 3.4. a How frequently is direct observation of hand hygiene compliance performed using the WHO hand hygiene observation tools (or similar technique)? | Never | 0 | 1 (7.7) |
| Annually | 10 | 1 (7.7) | |
| Every 3 months or more often | 15 | 11 (84.6) | |
| 3.4. b What is the overall hand hygiene compliance rate according to the WHO hand hygiene observation tool (or similar technique) in your facility? | <30% | 0 | 4 (30.8) |
| 31–40% | 5 | 2 (15.4) | |
| 41–50% | 10 | 4 (30.8) | |
| 51–60% | 15 | 3 (23.4) | |
| 61–70% | 20 | 0 (0.0) | |
| 71–80% | 25 | 0 (0.0) | |
| |||
| Question | Answer | Score | N (%) |
| 4.1. Are the following posters (or locally produced equivalent with similar contents) displayed? | |||
| 4.1. a Poster explaining the indications for hand hygiene | Not displayed | 0 | 2 (15.4) |
| Displayed in some wards/treatment areas | 15 | 0 (0.0) | |
| Displayed in most wards/treatment areas | 20 | 2 (15.4) | |
| Displayed in all wards/treatment areas | 25 | 9 (69.2) | |
| 4.1. b Poster explaining the correct use of handrub | Not displayed | 0 | 1 (7.7) |
| Displayed in some wards/treatment areas | 5 | 1 (7.7) | |
| Displayed in most wards/treatment areas | 10 | 3 (23.1) | |
| Displayed in all wards/treatment areas | 15 | 8 (61.5) | |
| 4.1. c Poster explaining correct handwashing technique | Not displayed | 0 | 0 (0.0) |
| Displayed in some wards/treatment areas | 5 | 0 (0.0) | |
| Displayed in most wards/treatment areas | 7.5 | 5 (38.5) | |
| Displayed at every sink in all wards/treatment areas | 10 | 8 (61.5) | |
| 4.2. How frequently does a systematic audit of all posters for evidence of damage occur, with replacement as required? | Never | 0 | 13 (100) |
| At least annually | 10 | 0 (0.0) | |
| Every 2–3 months | 15 | 0 (0.0) | |
| 4.3. Is hand hygiene promotion undertaken by displaying and regularly updating posters other than those mentioned above? | No | 0 | 10 (76.9) |
| Yes | 10 | 3 (23.1) | |
| 4.4. Are hand hygiene information leaflets available on wards? | No | 0 | 13 (100) |
| Yes | 10 | 0 (0.0) | |
| 4.5. Are other workplace reminders located throughout the facility? (e.g., hand hygiene campaign screensavers badges, stickers, etc) | No | 0 | 11 (84.6) |
| Yes | 15 | 2 (15.2) | |
| |||
| Question | Answer | Score | N (%) |
| 5.1. With regard to a hand hygiene team that is dedicated to the promotion and implementation of optimal hand hygiene practice in your facility: | |||
| 5.1. a Is such a team established? | No | 0 | 1 (7.7) |
| Yes | 5 | 12 (92.3) | |
| 5.1. b Does this team meet on a regular basis (at least annually)? | No | 0 | 3 (23.1) |
| Yes | 5 | 10 (76.9) | |
| 5.1. c Does this team have dedicated time to conduct hand hygiene promotion? | No | 0 | 6 (46.2) |
| Yes | 5 | 7 (53.9) | |
| 5.4. Are systems for identification of hand hygiene leaders from all disciplines in place? | |||
| 5.4. a A system for designation of hand hygiene champions | No | 0 | 6 (46.2) |
| Yes | 5 | 7 (53.9) | |
| 5.4. b A system for recognition and utilization of hand hygiene role models | No | 0 | 8 (61.5) |
| Yes | 5 | 5 (38.5) | |
| 5.5. Regarding patient involvement in hand hygiene promotion: | |||
| 5.5. a Are patients informed about the importance of hand hygiene? | No | 0 | 6 (46.2) |
| Yes | 5 | 7 (53.9) | |
| 5.5. b Has a formalized program of patient engagement been undertaken? | No | 0 | 10 (76.9) |
| Yes | 10 | 3 (23.1) | |
References
- World Health Organization. Report on the Burden of Endemic Health Care-Associated Infection Worldwide Clean Care Is Safer Care. 2011. Available online: https://apps.who.int/iris/bitstream/handle/10665/80135/9789241501507_eng.pdf (accessed on 10 July 2021).
- Jia, H.; Li, L.; Li, W.; Hou, T.; Ma, H.; Yang, Y.; Wu, A.; Liu, Y.; Wen, J.; Yang, H.; et al. Impact of Healthcare-Associated Infections on Length of Stay: A Study in 68 Hospitals in China. BioMed Res. Int. 2019, 2019, 2590563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serra-Burriel, M.; Keys, M.; Campillo-Artero, C.; Agodi, A.; Barchitta, M.; Gikas, A.; Palos, C.; López-Casasnovas, G. Impact of multi-drug resistant bacteria on economic and clinical outcomes of healthcare-associated infections in adults: Systematic review and meta-analysis. PLoS ONE 2020, 15, e0227139. [Google Scholar] [CrossRef] [PubMed]
- Alp, E.; Damani, N. Healthcare-associated infections in Intensive Care Units: Epidemiology and infection control in low-to-middle income countries. J. Infect. Dev. Ctries. 2015, 9, 1040–1045. [Google Scholar] [CrossRef] [Green Version]
- Irek, E.O.; Aliyu, A.A.; Dahiru, T.; Obadare, T.O.; Aboderin, A.O. Healthcare-associated infections and compliance of hand hygiene among healthcare workers in a tertiary health facility, southwest Nigeria. J. Infect. Prev. 2019, 20, 289–296. [Google Scholar] [CrossRef]
- Ali, S.; Birhane, M.; Bekele, S.; Kibru, G.; Teshager, L.; Yilma, Y.; Ahmed, Y.; Fentahun, N.; Assefa, H.; Gashaw, M.; et al. Healthcare associated infection and its risk factors among patients admitted to a tertiary hospital in Ethiopia: Longitudinal study. Antimicrob. Resist. Infect. Control 2018, 7, 2. [Google Scholar] [CrossRef] [Green Version]
- Lakoh, S.; Li, L.; Sevalie, S.; Guo, X.; Adekanmbi, O.; Yang, G.; Adebayo, O.; Yi, L.; Coker, J.M.; Wang, S.; et al. Antibiotic resistance in patients with clinical features of healthcare-associated infections in an urban tertiary hospital in Sierra Leone: A cross-sectional study. Antimicrob. Resist. Infect. Control 2020, 9, 10–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakoh, S.; Yi, L.; Sevalie, S.; Guo, X.; Adekanmbi, O.; Smalle, I.O.; Williams, N.; Barrie, U.; Koroma, C.; Zhao, Y.; et al. Incidence and risk factors of surgical site infections and related antibiotic resistance in Freetown, Sierra Leone: A prospective cohort study. Antimicrob. Resist. Infect. Control 2022, 11, 39. [Google Scholar] [CrossRef]
- Kingston, L.; O’Connell, N.; Dunne, C. Hand hygiene-related clinical trials reported since 2010: A systematic review. J. Hosp. Infect. 2016, 92, 309–320. [Google Scholar] [CrossRef]
- WHO 2010: Hand Hygiene Self-Assessment Framework 2010. Available online: https://www.who.int/gpsc/country_work/hhsa_framework_October_2010.pdf (accessed on 10 January 2022).
- Stewardson, A.; Allegranzi, B.; Perneger, T.; Attar, H.; Pittet, D. Testing the WHO Hand Hygiene Self-Assessment Framework for usability and reliability. J. Hosp. Infect. 2012, 83, 30–35. [Google Scholar] [CrossRef]
- Ministry of Health and Sanitation; Government of Sierra Leone. Ebola Viral Disease Situation Report. Available online: https://reliefweb.int/sites/reliefweb.int/files/resources/Ebola-Situation-Report_Vol-260.pdf (accessed on 28 January 2022).
- GoSL. 2016: National Infection Prevention and Control Policy. Available online: www.afro.who.int/publications/national-infection-prevention-and-control-guidelines-2016 (accessed on 10 January 2022).
- SSL. 2015: Sierra Leone Population Census. Available online: https://www.statistics.sl/images/StatisticsSL/Documents/Census/2015/sl_2015_phc_thematic_report_on_pop_structure_and_pop_distribution.pdf (accessed on 14 January 2022).
- World Bank Group. Sierra Leone 2021 Economic Update. Available online: https://openknowledge.worldbank.org/bitstream/handle/10986/35784/Sierra-Leone-2021-Economic-Update-Welfare-and-Poverty-Effects-of-the-COVID-19-Pandemic.pdf?sequence=5 (accessed on 28 January 2022).
- GoSL SLMTDP. Development-Documents-National-Development-Plan-2019-23-47099. 2018. Available online: https://www.imf.org/en/Publications/CR/Issues/2019/07/09/Sierra-Leone-Economic-Development-Documents-National-Development-Plan-2019-23-47099 (accessed on 14 January 2022).
- MICS. 2017: SIERRA LEONE MULTIPLE INDICATOR CLUSTER SURVEY. 2017. Available online: https://www.statistics.sl/images/StatisticsSL/Documents/sierra_leone_mics6_2017_report.pdf (accessed on 14 January 2022).
- WHO. 2016: Summary Report: Hand Hygiene Self-Assessment Framework Survey 2015/2016. A Report from the WHO Infection Prevention and Control Global Unit. Available online: https://apps.who.int/iris/bitstream/handle/10665/330067/WHO-HIS-SDS-2016.7-eng.pdf?sequence=1&isAllowed=y (accessed on 17 January 2022).
- Kilpatrick, C.; Tartari, E.; Gayet-Ageron, A.; Storr, J.; Tomczyk, S.; Allegranzi, B.; Pittet, D. Global hand hygiene improvement progress: Two surveys using the WHO Hand Hygiene Self-Assessment Framework. J. Hosp. Infect. 2018, 100, 202–206. [Google Scholar] [CrossRef]
- Allegranzi, B.; Conway, L.; Larson, E.; Pittet, D. Status of the implementation of the World Health Organization multimodal hand hygiene strategy in United States of America health care facilities. Am. J. Infect. Control 2014, 42, 224–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakoh, S.; Firima, E.; Williams, C.E.E.; Conteh, S.K.; Jalloh, M.B.; Sheku, M.G.; Adekanmbi, O.; Sevalie, S.; Kamara, S.A.; Kamara, M.A.S.; et al. An Intra-COVID-19 Assessment of Hand Hygiene Facility, Policy and Staff Compliance in Two Hospitals in Sierra Leone: Is There a Difference between Regional and Capital City Hospitals? Trop. Med. Infect. Dis. 2021, 6, 204. [Google Scholar] [CrossRef] [PubMed]
- Ataiyero, Y.; Dyson, J.; Graham, M. Barriers to hand hygiene practices among health care workers in sub-Saharan African countries: A narrative review. Am. J. Infect. Control 2019, 47, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Nwaokenye, J.; Lakoh, S.; Morgan, J. Perceptions of Nigerian healthcare workers towards hand hygiene: A qualitative study. Pan Afr. Med. J. 2020, 36, 204. [Google Scholar] [CrossRef]
- Loftus, M.J.; Guitart, C.; Tartari, E.; Stewardson, A.J.; Amer, F.; Bellissimo-Rodrigues, F.; Lee, Y.F.; Mehtar, S.; Sithole, B.L.; Pittet, D. Hand hygiene in low- and middle-income countries. Int. J. Infect. Dis. 2019, 86, 25–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- An, B.; Yang, S.J. The evaluation of a multimodal hand hygiene improvement strategy in Cambodian hospitals. J. Infect. Dev. Ctries. 2020, 14, 1047–1053. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.; Sharma, M.; Koushal, V. Compliance to Hand Hygiene World Health Organization Guidelines in Hospital Care. Int. J. Prev. Med. 2014, 5, 127–128. [Google Scholar]
- Wiedenmayer, K.; Msamba, V.-S.; Chilunda, F.; Kiologwe, J.C.; Seni, J. Impact of hand hygiene intervention: A comparative study in health care facilities in Dodoma region, Tanzania using WHO methodology. Antimicrob. Resist. Infect. Control 2020, 9, 80. [Google Scholar] [CrossRef]
- Omilabu, S.; Salu, O.; Oke, B.; James, A. The West African ebola virus disease epidemic 2014–2015: A commissioned review. Niger. Postgrad. Med. J. 2016, 23, 49–56. [Google Scholar] [CrossRef] [Green Version]
- Lakoh, S.; Jiba, D.F.; Baldeh, M.; Adekanmbi, O.; Barrie, U.; Seisay, A.L.; Deen, G.F.; Salata, R.A.; Yendewa, G.A. Impact of COVID-19 on Tuberculosis Case Detection and Treatment Outcomes in Sierra Leone. Trop. Med. Infect. Dis. 2021, 6, 154. [Google Scholar] [CrossRef]
- WHO. Sierra Leone Confirms First Case of COVID-19: 2020. Available online: https://www.afro.who.int/news/sierra-leone-confirms-first-case-covid-19 (accessed on 17 January 2022).
- Choe, P.G.; Lim, J.; Kim, E.J.; Kim, J.H.; Shin, M.J.; Kim, S.R.; Choi, J.Y.; Choi, Y.H.; Lee, K.W.; Koo, H.; et al. Impact of national policy on hand hygiene promotion activities in hospitals in Korea. Antimicrob. Resist. Infect. Control 2020, 9, 157. [Google Scholar] [CrossRef] [PubMed]
- Uneke, C.J.; Ndukwe, C.D.; Oyibo, P.G.; Nwakpu, K.O.; Nnabu, R.C.; Prasopa-Plaizier, N. Promotion of hand hygiene strengthening initiative in a Nigerian teaching hospital: Implication for improved patient safety in low-income health facilities. Braz. J. Infect. Dis. 2014, 18, 21–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmen, I.C.; Seneza, C.; Nyiranzayisaba, B.; Nyiringabo, V.; Bienfait, M.; Safdar, N. Improving Hand Hygiene Practices in a Rural Hospital in Sub-Saharan Africa. Infect. Control Hosp. Epidemiol. 2016, 37, 834–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]

| Total Score | Hand Hygiene Level | Definition |
|---|---|---|
| 0–125 | Inadequate | indicates insufficient hand hygiene practices and promotion, and requires significant improvement |
| 126–250 | Basic | indicates that some measures are in place but not satisfactory and therefore requires further improvement |
| 251–375 | Intermediate or Consolidation | indicates appropriate hand hygiene promotion strategies and improvements in hand hygiene practices, but requires long-term planning to ensure continual improvement and progress |
| 376–500 | Advanced or Embeddinge | iindicates sustained hand hygiene promotion and practice as well as a quality and safety culture surrounding hand hygiene promotion within the organization |
| Hospital Characteristics | Secondary Hospitals (N = 6) | Tertiary Hospitals (N = 7) |
|---|---|---|
| N (%) | N (%) | |
| Type of hospital | 6 (100) | 7 (100) |
| Location of hospital | ||
| Urban | 6 (100) | 5 (71) |
| Rural | 0 (0) | 2 (29) |
| Bed capacity | ||
| <50 | 3 (50) | 0(0) |
| 51–100 | 3 (50) | 1 (14) |
| 101–150 | 0 (0) | 1 (14) |
| 151–200 | 0 (0) | 2 (29) |
| >200 | 0 (0) | 3 (43) |
| Staff capacity | ||
| ≤200 | 2 (33) | 3 (43) |
| 201–400 | 4 (67) | 0 (0) |
| 400–600 | 0 (0) | 3 (43) |
| ≥601 | 0 (0) | 1 (14) |
| Units/wards | ||
| <10 | 1 (17) | 0 (0) |
| 10–20 | 4 (66) | 4 (57) |
| >20 | 1 (17) | 3 (43) |
| Hospital Type | Hospital | Nurses | Doctors & CHOs † | Pharmacy & Laboratory Personnel | Others * |
|---|---|---|---|---|---|
| Secondary | S1 | 149 | 10 | 11 | 33 |
| S2 | 124 | 12 | 3 | 6 | |
| S3 | 252 | 15 | 29 | 16 | |
| S4 | 173 | 20 | 30 | 51 | |
| S5 | 184 | 6 | 19 | 14 | |
| S6 | 35 | 1 | 5 | 2 | |
| Tertiary | T1 | 420 | 36 | 24 | 87 |
| T2 | 295 | 31 | 23 | 34 | |
| T3 | 51 | 5 | 14 | 35 | |
| T4 | 62 | 9 | 8 | 13 | |
| T5 | 87 | 9 | 4 | 3 | |
| T6 | 294 | 49 | 25 | 79 | |
| T7 | 442 | 42 | 25 | 137 |
| Hospital Type | Hospital/Mean ± SD | SC | TE | EF | RW | ISC | Total Score | Hand Hygiene Level |
|---|---|---|---|---|---|---|---|---|
| Secondary | S1 | 35 | 80 | 48 | 55 | 50 | 268 | Intermediate |
| S2 | 40 | 35 | 58 | 50 | 30 | 248 | Basic | |
| S3 | 55 | 80 | 65 | 50 | 65 | 315 | Intermediate | |
| S4 | 80 | 50 | 45 | 70 | 30 | 275 | Intermediate | |
| S5 | 50 | 70 | 60 | 45 | 65 | 290 | Intermediate | |
| S6 | 75 | 50 | 68 | 63 | 50 | 305 | Intermediate | |
| Mean ± SD | 48 ± 11 | 72 ± 21 | 55 ± 14 | 36 ± 15 | 43 ± 13 | 260 ± 30 | Intermediate | |
| Tertiary | T1 | 40 | 100 | 75 | 33 | 35 | 283 | Intermediate |
| T2 | 65 | 75 | 65 | 25 | 65 | 295 | Intermediate | |
| T3 | 55 | 65 | 35 | 15 | 40 | 210 | Basic | |
| T4 | 50 | 75 | 53 | 38 | 40 | 255 | Intermediate | |
| T5 | 30 | 55 | 35 | 68 | 25 | 213 | Basic | |
| T6 | 30 | 55 | 35 | 68 | 25 | 213 | Basic | |
| T7 | 75 | 80 | 60 | 70 | 90 | 375 | Intermediate | |
| Mean ± SD | 56 ± 21 | 63 ± 13 | 53 ± 14 | 62 ± 10 | 50 ± 25 | 284 ± 58 | Intermediate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lakoh, S.; Maruta, A.; Kallon, C.; Deen, G.F.; Russell, J.B.W.; Fofanah, B.D.; Kamara, I.F.; Kanu, J.S.; Kamara, D.; Molleh, B.; et al. How Well Are Hand Hygiene Practices and Promotion Implemented in Sierra Leone? A Cross-Sectional Study in 13 Public Hospitals. Int. J. Environ. Res. Public Health 2022, 19, 3787. https://doi.org/10.3390/ijerph19073787
Lakoh S, Maruta A, Kallon C, Deen GF, Russell JBW, Fofanah BD, Kamara IF, Kanu JS, Kamara D, Molleh B, et al. How Well Are Hand Hygiene Practices and Promotion Implemented in Sierra Leone? A Cross-Sectional Study in 13 Public Hospitals. International Journal of Environmental Research and Public Health. 2022; 19(7):3787. https://doi.org/10.3390/ijerph19073787
Chicago/Turabian StyleLakoh, Sulaiman, Anna Maruta, Christiana Kallon, Gibrilla F. Deen, James B. W. Russell, Bobson Derrick Fofanah, Ibrahim Franklyn Kamara, Joseph Sam Kanu, Dauda Kamara, Bailah Molleh, and et al. 2022. "How Well Are Hand Hygiene Practices and Promotion Implemented in Sierra Leone? A Cross-Sectional Study in 13 Public Hospitals" International Journal of Environmental Research and Public Health 19, no. 7: 3787. https://doi.org/10.3390/ijerph19073787
APA StyleLakoh, S., Maruta, A., Kallon, C., Deen, G. F., Russell, J. B. W., Fofanah, B. D., Kamara, I. F., Kanu, J. S., Kamara, D., Molleh, B., Adekanmbi, O., Tavernor, S., Guth, J., Sagili, K. D., & Wilkinson, E. (2022). How Well Are Hand Hygiene Practices and Promotion Implemented in Sierra Leone? A Cross-Sectional Study in 13 Public Hospitals. International Journal of Environmental Research and Public Health, 19(7), 3787. https://doi.org/10.3390/ijerph19073787