
The Impact of Acute Tinnitus on Listening Effort: A Study Based on Clinical Observations of Sudden Sensorineural Hearing Loss Patients

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Audiological Tests
2.3. Tinnitus Measurements
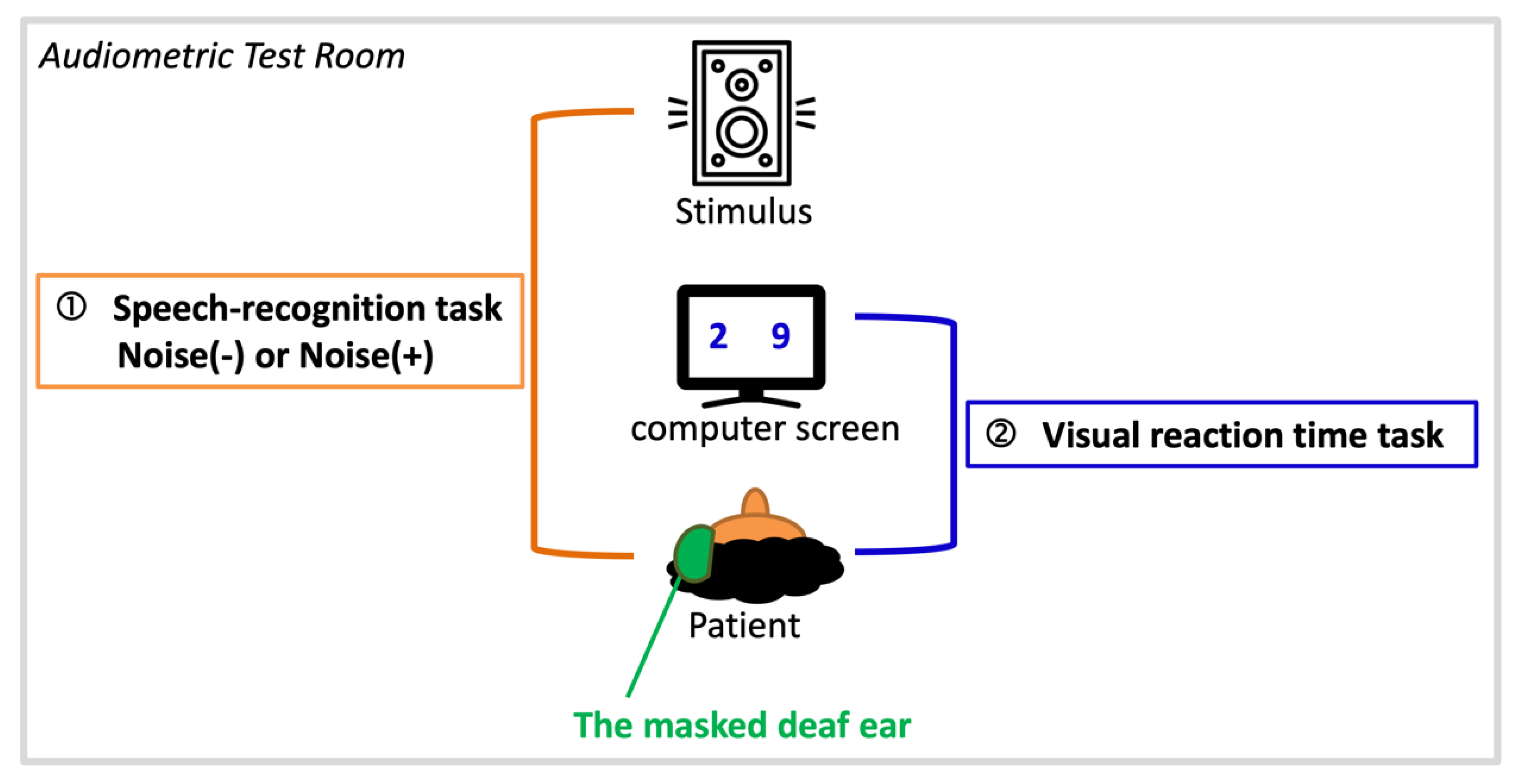
2.4. Dual-Task Paradigm
2.5. Statistical Analysis
3. Results
3.1. Patients’ Characteristics and Audiological Results
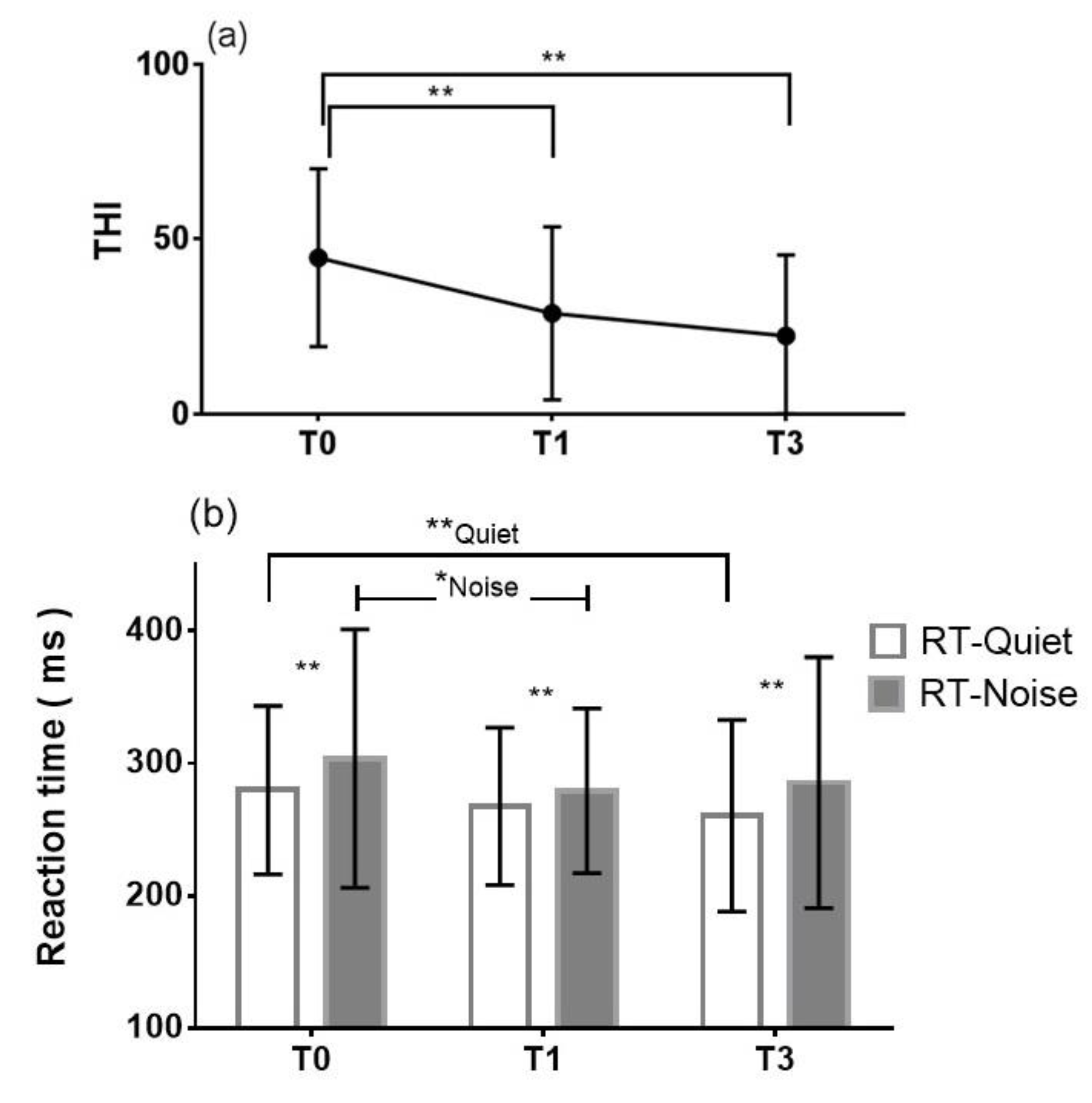
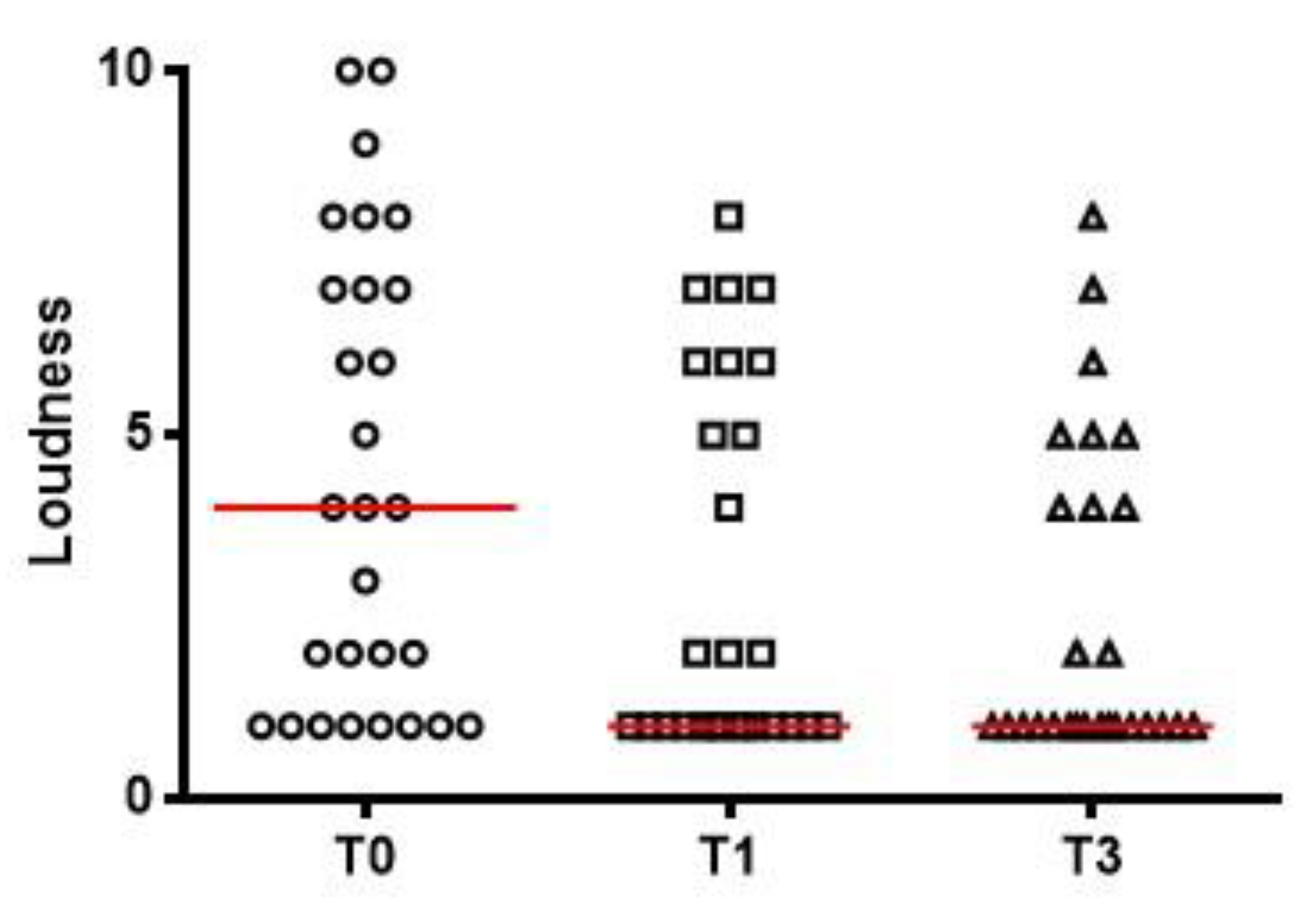
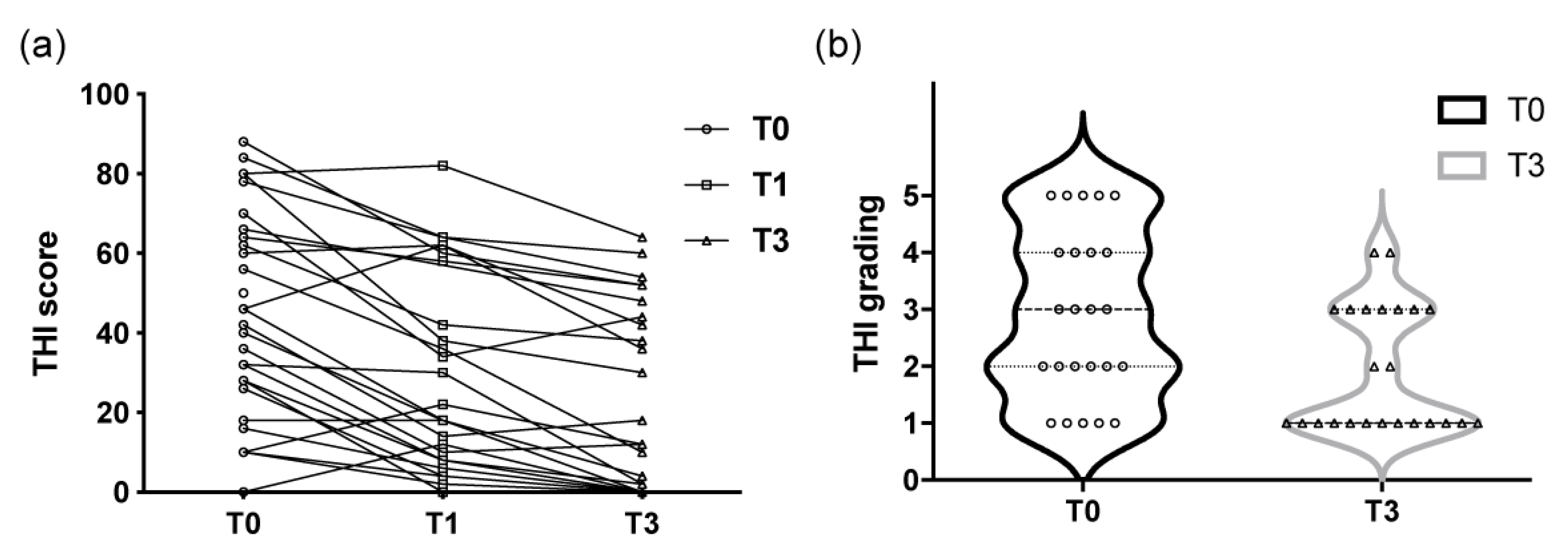
3.2. Severity of Tinnitus—THI Scores and Loudness Matching
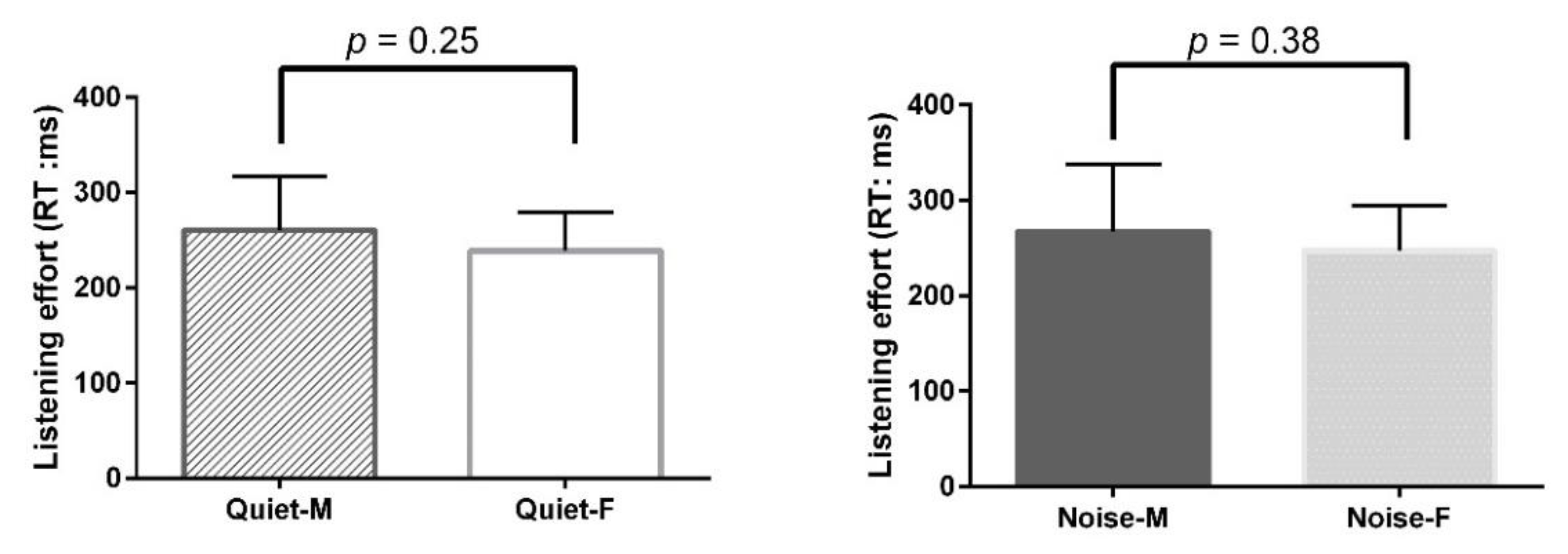
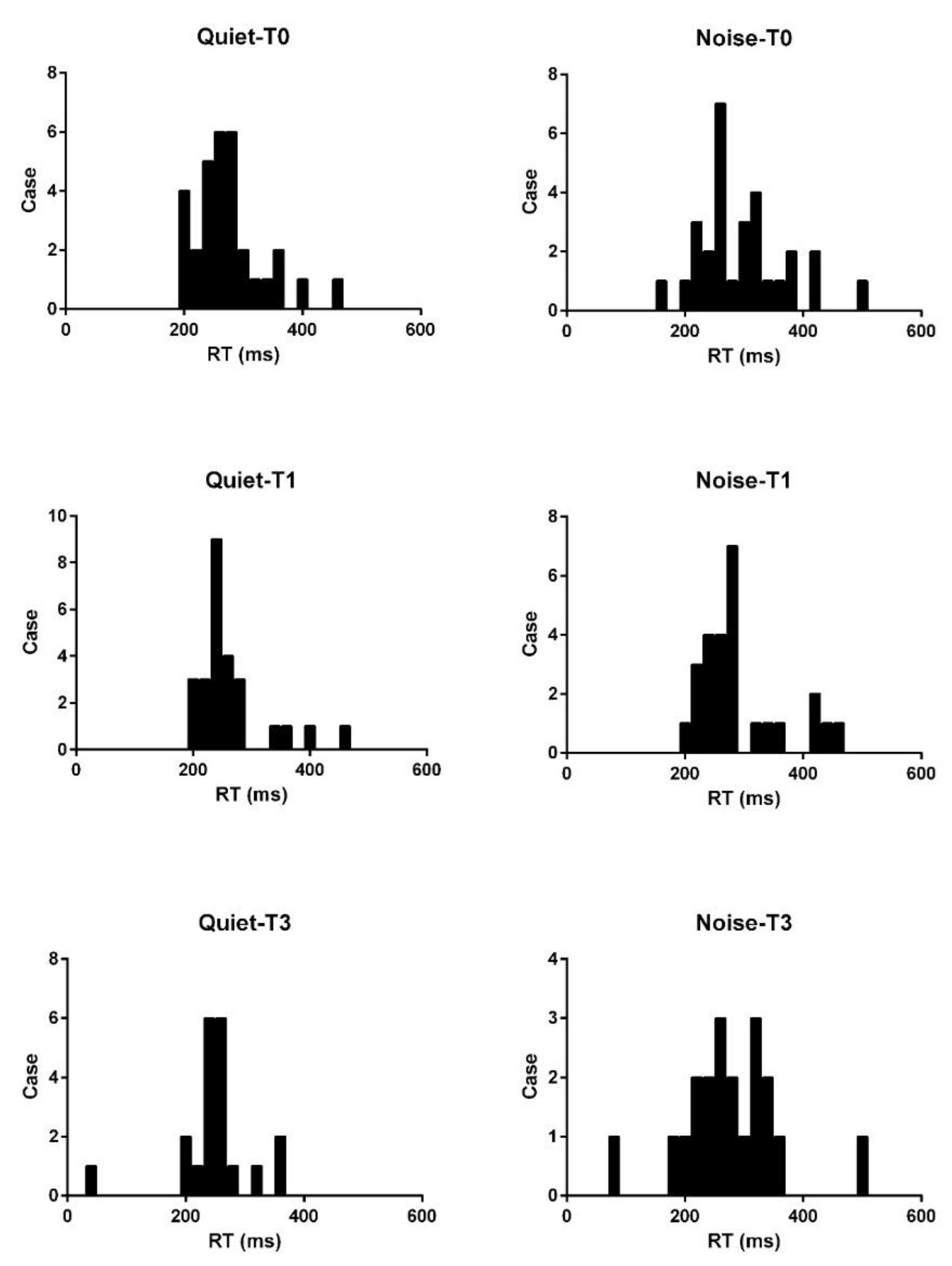
3.3. Listening Effort of the Unaffected Ear—Dual-Task Performance
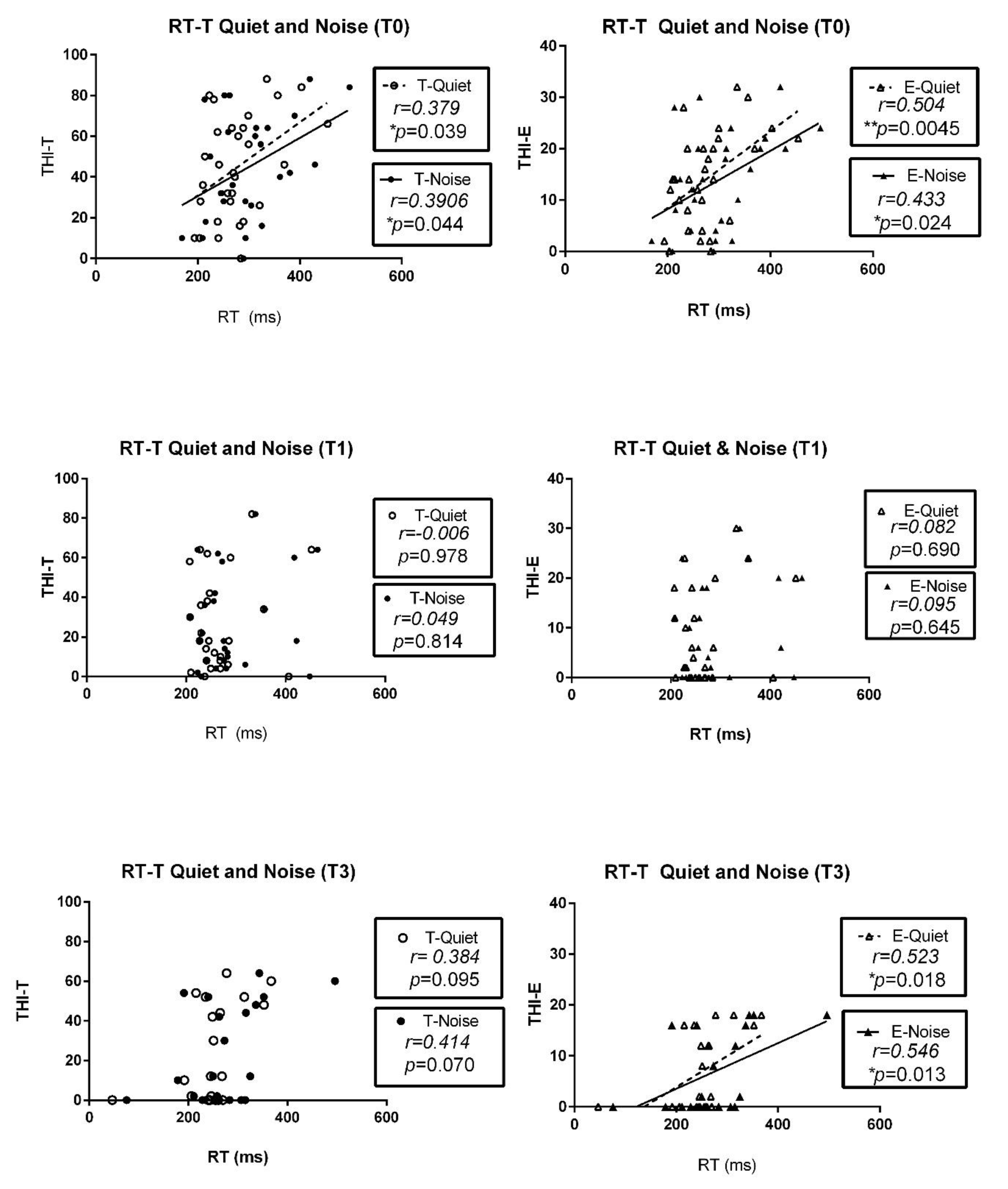
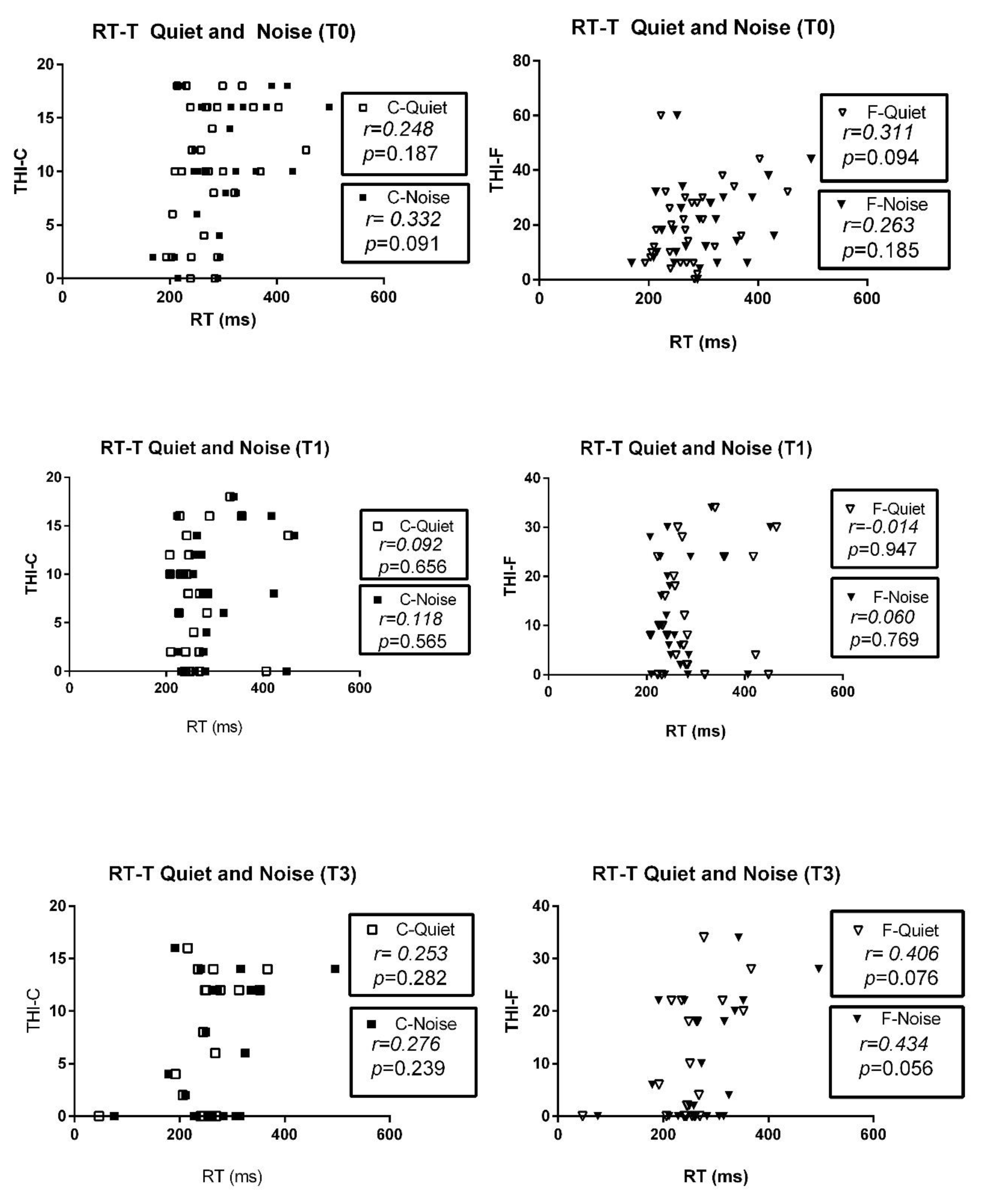
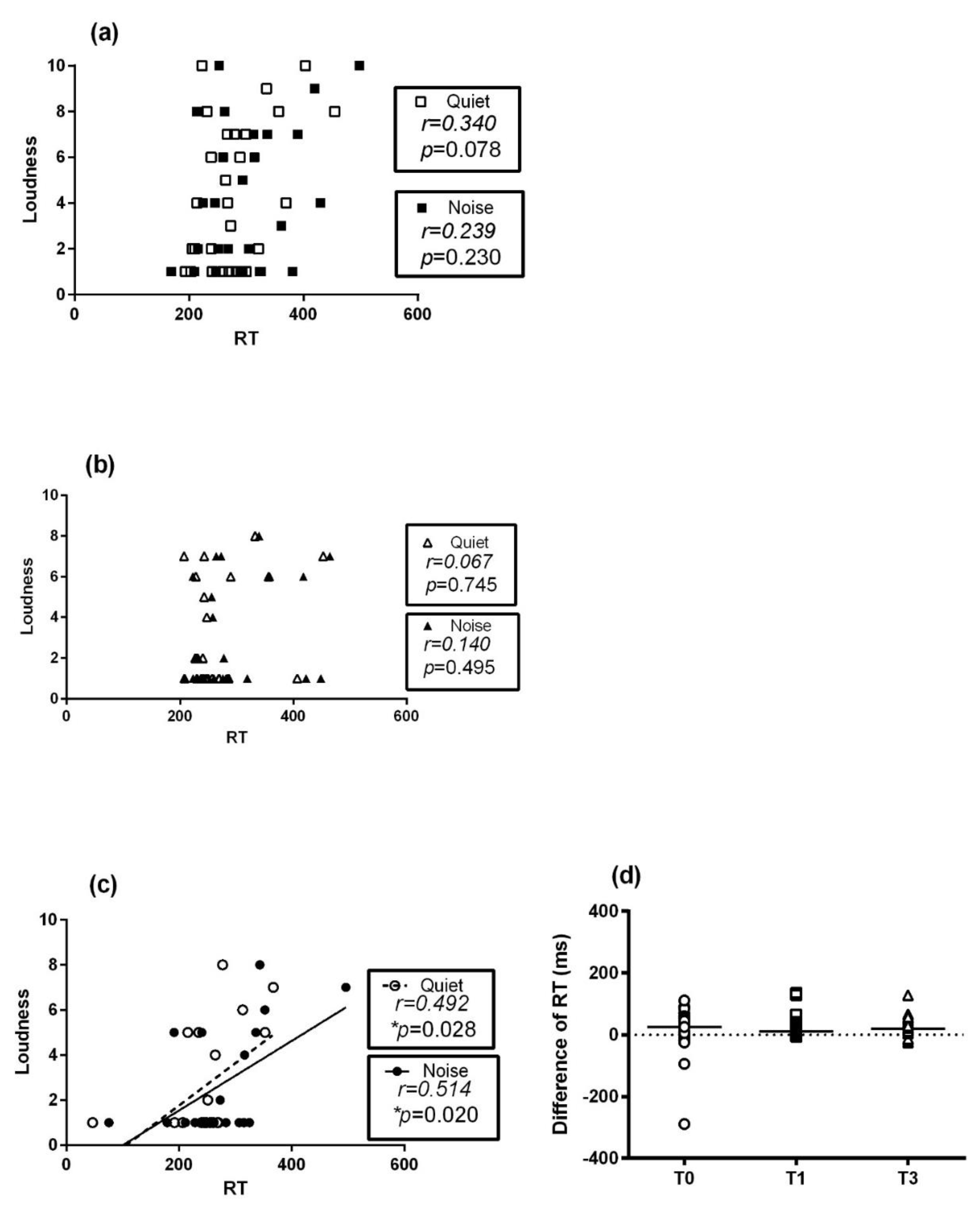
3.4. Correlations between Tinnitus and Dual-Task Performance
4. Discussion
4.1. Measurement of Listening Effort
4.2. Factors Influencing Listening Effort
4.3. Changes in Tinnitus and Listening Effort during the Clinical Course
4.4. Relationship between Acute Tinnitus and Listening Effort
4.5. Limitations of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A
Appendix B
Appendix C
- Preliminary data: healthy, tinnitus-free subjects
- Subjects: 28
- Male: 14; Female 14
- Age (years): 38.50 ± 12.41; (range = 20–55)
- Listening effort (visual reaction time): Quiet: 249.80 ± 48.90 ms; Noise: 257.27 ± 59.28 ms.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (Hz) | SRT | 250 | 500 | 1k | 2k | 4k | 8k | |
|---|---|---|---|---|---|---|---|---|
| Left | Average | 13.39 | 14.11 | 13.04 | 12.68 | 10.89 | 14.82 | 15.18 |
| SD | 5.94 | 6.95 | 5.50 | 6.73 | 8.17 | 9.86 | 15.96 | |
| Right | Average | 13.21 | 15.71 | 14.29 | 13.21 | 11.96 | 15.18 | 16.25 |
| SD | 5.97 | 6.63 | 6.77 | 6.12 | 7.50 | 9.86 | 11.99 | |
| Left Side (Hz) | SRT | 250 | 500 | 1k | 2k | 4k | 8k | ||
|---|---|---|---|---|---|---|---|---|---|
| Listening effort | Quiet | r | 0.1038 | 0.2316 | 0.2590 | 0.2850 | 0.1821 | 0.2204 | 0.2028 |
| p | 0.5991 | 0.2356 | 0.1832 | 0.1415 | 0.3537 | 0.2598 | 0.3007 | ||
| Noise | r | 0.2068 | 0.2584 | 0.2300 | 0.3635 | 0.2507 | 0.2988 | 0.3388 | |
| p | 0.2911 | 0.1842 | 0.2391 | 0.0572 | 0.1981 | 0.1224 | 0.0778 | ||
| Right Side (Hz) | SRT | 250 | 500 | 1k | 2k | 4k | 8k | ||
|---|---|---|---|---|---|---|---|---|---|
| Listening effort | Quiet | r | 0.2029 | 0.09965 | 0.1134 | 0.1895 | 0.1517 | −0.05045 | 0.1852 |
| p | 0.3005 | 0.6139 | 0.5655 | 0.3340 | 0.4409 | 0.7987 | 0.3455 | ||
| Noise | r | 0.2967 | 0.1586 | 0.05614 | 0.3251 | 0.2184 | 0.006638 | 0.2751 | |
| p | 0.1253 | 0.4201 | 0.7766 | 0.0914 | 0.2642 | 0.9733 | 0.1565 | ||
Appendix D
References
- Hicks Candace, B.; Tharpe Anne, M. Listening Effort and Fatigue in School-Age Children With and Without Hearing Loss. JSLHR 2002, 45, 573–584. [Google Scholar]
- Peelle, J.E. Listening effort: How the cognitive consequences of acoustic challenge are reflected in brain and behavior. Ear Hear. 2018, 39, 204. [Google Scholar] [CrossRef] [PubMed]
- Manche, S.K.; Madhavi, J.; Meganadh, K.R.; Jyothy, A. Association of tinnitus and hearing loss in otological disorders: A decade-long epidemiological study in a South Indian population. Braz. J. Otorhinolaryngol. 2016, 82, 643–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tyler, R.S.; Baker, L.J. Difficulties experienced by tinnitus sufferers. J. Speech Hear. Disord. 1983, 48, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, G.P.; Calder, J.A.; Newman, C.W.; Peterson, E.L.; Wharton, J.A.; Ahmad, B. Electrophysiological indices of selective auditory attention in subjects with and without tinnitus. Hear. Res. 1996, 97, 66–74. [Google Scholar] [CrossRef]
- Stevens, C.; Walker, G.; Boyer, M.; Gallagher, M. Severe tinnitus and its effect on selective and divided attention: Acufeno severo y sus efectos sobre la atención selectiva y dividida. Int. J. Audiol. 2007, 46, 208–216. [Google Scholar] [CrossRef] [PubMed]
- Fabijańska, A.; Smurzyński, J.; Hatzopoulos, S.; Kochanek, K.; Bartnik, G.; Raj-Koziak, D.; Mazzoli, M.; Skarżynski, P.H.; Jędrzejczak, W.W.; Szkiełkowska, A. The relationship between distortion product otoacoustic emissions and extended high-frequency audiometry in tinnitus patients. Part 1: Normally hearing patients with unilateral tinnitus. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2012, 18, CR765. [Google Scholar] [CrossRef] [Green Version]
- Savastano, M. Tinnitus with or without hearing loss: Are its characteristics different? Eur. Arch. Oto-Rhino-Laryngol. 2008, 265, 1295–1300. [Google Scholar] [CrossRef]
- Kowalska, S.; Sułkowski, W. Tinnitus in noise-induced hearing impairment. Med. Pracy 2001, 52, 305–313. [Google Scholar]
- Degeest, S.; Keppler, H.; Corthals, P. The effect of tinnitus on listening effort in normal-hearing young adults: A preliminary study. J. Speech Lang. Hear. Res. 2017, 60, 1036–1045. [Google Scholar] [CrossRef]
- Juul Jensen, J.; Callaway, S.L.; Lunner, T.; Wendt, D. Measuring the impact of tinnitus on aided listening effort using pupillary response. Trends Hear. 2018, 22, 2331216518795340. [Google Scholar] [CrossRef] [PubMed]
- Stachler, R.J.; Chandrasekhar, S.S.; Archer, S.M.; Rosenfeld, R.M.; Schwartz, S.R.; Barrs, D.M.; Brown, S.R.; Fife, T.D.; Ford, P.; Ganiats, T.G. Clinical practice guideline: Sudden hearing loss. Otolaryngol.—Head Neck Surg. 2012, 146, S1–S35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandrasekhar, S.S.; Tsai Do, B.S.; Schwartz, S.R.; Bontempo, L.J.; Faucett, E.A.; Finestone, S.A.; Hollingsworth, D.B.; Kelley, D.M.; Kmucha, S.T.; Moonis, G.; et al. Clinical Practice Guideline: Sudden Hearing Loss (Update). Otolaryngol. Head Neck Surg. 2019, 161, S1–S45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, Y.-F.; Chu, Y.-C.; Tu, T.-Y.; Shiao, A.-S.; Wu, S.-L.; Liao, W.-H. Modified Siegel’s criteria for sudden sensorineural hearing loss: Reporting recovery outcomes with matched pretreatment hearing grades. J. Chin. Med. Assoc. JCMA 2018, 81, 1008–1012. [Google Scholar] [CrossRef]
- Byl, F.M., Jr. Sudden hearing loss: Eight years’ experience and suggested prognostic table. Laryngoscope 1984, 94, 647–661. [Google Scholar] [CrossRef]
- Singh, A.; Irugu, D.V.K. Sudden sensorineural hearing loss—A contemporary review of management issues. J. Otol. 2020, 15, 67–73. [Google Scholar] [CrossRef]
- Xie, W.; Dai, Q.; Liu, J.; Liu, Y.; Hellström, S.; Duan, M. Analysis of clinical and laboratory findings of idiopathic sudden sensorineural hearing loss. Sci. Rep. 2020, 10, 6057. [Google Scholar] [CrossRef] [Green Version]
- Nosrati-Zarenoe, R.; Arlinger, S.; Hultcrantz, E. Idiopathic sudden sensorineural hearing loss: Results drawn from the Swedish national database. Acta Oto-Laryngol. 2007, 127, 1168–1175. [Google Scholar] [CrossRef]
- Murai, K.; Tsuiki, T.; Kusano, H.; Shishido, K. Clinical study of audiograms in the initial stage and fixed stage of sudden deafness. Acta Oto-Laryngol. 1994, 114, 17–20. [Google Scholar] [CrossRef]
- Hultcrantz, M.; Sylvén, L.; Borg, E. Ear and hearing problems in 44 middle-aged women with Turner’s syndrome. Hear. Res. 1994, 76, 127–132. [Google Scholar] [CrossRef]
- Ceylan, A.; Celenk, F.; Kemaloğlu, Y.; Bayazıt, Y.; Göksu, N.; Özbi, S. Impact of prognostic factors on recovery from sudden hearing loss. J. Laryngol. Otol. 2007, 121, 1035–1040. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, E.S.; Charlotte, A.; Dorian, O.H.; Linda, M.L. Sudden sensorineural hearing loss. Lancet 2010, 375, 1203–1211. [Google Scholar]
- Nogueira-Neto, F.B.; Gallardo, F.P.; de Barros Suzuki, F.A.; de Oliveira Penido, N. Prognostic and evolutive factors of tinnitus triggered by sudden sensorineural hearing loss. Otol. Neurotol. 2016, 37, 627–633. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.; Liu, T. The relationship of tinnitus recovery and hearing improvement in idiopathic sudden sensorineural hearing loss. J. Hear. Sci. 2017, 7, 110. [Google Scholar]
- Penner, M.J. Masking of tinnitus and central masking. J. Speech Hear. Res. 1987, 30, 147–152. [Google Scholar] [CrossRef]
- Olusanya, B.O.; Davis, A.C.; Hoffman, H.J. Hearing loss grades and the International classification of functioning, disability and health. Bull. World Health Organ. 2019, 97, 725. [Google Scholar] [CrossRef]
- Siegel, L.G. The treatment of idiopathic sudden sensorineural hearing loss. Otolaryngol. Clin. N. Am. 1975, 8, 467–473. [Google Scholar] [CrossRef]
- Huang, C.-Y.; Lee, H.-H.; Chung, K.-C.; Chen, H.-C.; Shen, Y.-J.; Wu, J.-L. Relationships among speech perception, self-rated tinnitus loudness and disability in tinnitus patients with normal pure-tone thresholds of hearing. Orl 2007, 69, 25–29. [Google Scholar] [CrossRef]
- Newman, C.W.; Jacobson, G.P.; Spitzer, J.B. Development of the tinnitus handicap inventory. Arch. Otolaryngol.-Head Neck Surg. 1996, 122, 143–148. [Google Scholar] [CrossRef]
- Picou, E.M.; Ricketts, T.A.; Hornsby, B.W. How hearing aids, background noise, and visual cues influence objective listening effort. Ear Hear. 2013, 34, e52–e64. [Google Scholar] [CrossRef]
- Strobach, T.; Frensch, P.A.; Soutschek, A.; Schubert, T. Investigation on the improvement and transfer of dual-task coordination skills. Psychol. Res. 2012, 76, 794–811. [Google Scholar] [CrossRef] [PubMed]
- Liepelt, R.; Strobach, T.; Frensch, P.; Schubert, T. Improved intertask coordination after extensive dual-task practice. Q. J. Exp. Psychol. 2011, 64, 1251–1272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Su, F. Development of standardized phonetically balanced word lists (Zhong kuo yu yin jun hen zi huei biao zhi bian zhi yian jiou). J. Taiwan Otolaryngol.-Head Neck Surg. 1979, 14, 7–16. [Google Scholar]
- Miles, K.; McMahon, C.; Boisvert, I.; Ibrahim, R.; De Lissa, P.; Graham, P.; Lyxell, B. Objective assessment of listening effort: Coregistration of pupillometry and EEG. Trends Hear. 2017, 21, 2331216517706396. [Google Scholar] [CrossRef]
- Gagne, J.-P.; Besser, J.; Lemke, U. Behavioral assessment of listening effort using a dual-task paradigm: A review. Trends Hear. 2017, 21, 2331216516687287. [Google Scholar] [CrossRef] [Green Version]
- Kahneman, D. Attention and Effort; Prentice Hall: Hoboken, NJ, USA, 1973; Volume 1063. [Google Scholar]
- Ward, K.M.; Shen, J.; Souza, P.E.; Grieco-Calub, T.M. Age-related differences in listening effort during degraded speech recognition. Ear Hear. 2017, 38, 74. [Google Scholar] [CrossRef] [Green Version]
- Ohlenforst, B.; Zekveld, A.A.; Jansma, E.P.; Wang, Y.; Naylor, G.; Lorens, A.; Lunner, T.; Kramer, S.E. Effects of hearing impairment and hearing aid amplification on listening effort: A systematic review. Ear Hear. 2017, 38, 267. [Google Scholar] [CrossRef] [Green Version]
- Picou, E.M.; Gordon, J.; Ricketts, T.A. The effects of noise and reverberation on listening effort for adults with normal hearing. Ear Hear. 2016, 37, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Liang, J.; Ou, J.; Cai, W. Mental health in adults with sudden sensorineural hearing loss: An assessment of depressive symptoms and its correlates. J. Psychosom. Res. 2013, 75, 72–74. [Google Scholar] [CrossRef]
| Characteristics | Data |
|---|---|
| Case (Male:Female) | 30 (18:12) |
| Age (years old) | 16–65 |
| mean ± SD | 46.6 ± 16.3 |
| Lesion ear (Right:Left) | 20:10 |
| Duration (day) | 2–60 |
| mean ± SD | 8.5 ± 12.0 |
| median | 4 |
| Other symptoms | |
| tinnitus | 30 |
| vertigo/dizziness | 4/4 |
| T0 | T1 | T3 | ||
|---|---|---|---|---|
| AC1 | Lesioned | 53.13 ± 26.13 | 39.64 ± 21.27 | 38.76 ± 20.50 |
| Unaffected | 18.53 ± 9.58 | 19.02 ± 11.33 | 21.18 ± 10.24 | |
| AC2 | Lesioned | 62.07 ± 20.97 | 42.71 ± 20.95 | 41.83 ± 21.28 |
| Unaffected | 25.40 ± 21.17 | 21.71 ± 13.28 | 14.13 ± 11.94 | |
| SRT | Lesioned | 59.52 ± 25.57 | 34.02 ± 23.21 | 27.92 ± 20.56 |
| Unaffected | 15.17 ± 9.41 | 16.04 ± 11.01 | 16.39 ± 6.14 |
| Hz | 250 | 500 | 1k | 2k | 4k | 8k | |
|---|---|---|---|---|---|---|---|
| Lesioned side | F | 10.79 | 10.93 | 10.76 | 15.34 | 5.17 | 8.34 |
| p | 0.0014 ** | 0.0011 ** | 0.0012 ** | 0.0002 *** | 0.0195 * | 0.0035 ** | |
| Unaffected side | F | 0.2286 | 0.1482 | 0.5819 | 0.4179 | 0.4136 | 0.4401 |
| p | 0.77 | 0.86 | 0.56 | 0.69 | 0.69 | 0.65 |
| r/p Value | |||||
|---|---|---|---|---|---|
| T0 | T1 | T3 | |||
| Quiet | THI | T | 0.3791/* 0.0388 | −0.0058/0.9775 | 0.3837/0.0949 |
| C | 0.2476/0.1871 | 0.9165/0.6561 | 0.2528/0.2822 | ||
| E | 0.5040/** 0.0045 | 0.0821/0.6900 | 0.5232/* 0.0179 | ||
| F | 0.3112/0.0942 | −0.0137/0.9469 | 0.4058/0.0758 | ||
| Loudness | 0.3395/0.0772 | 0.0671/0.7446 | 0.4915/* 0.0278 | ||
| Noise | THI | T | 0.3906/* 0.0440 | 0.0049/0.8136 | 0.4135/0.0700 |
| C | 0.3316/0.0911 | 0.1182/0.5653 | 0.2761/0.2387 | ||
| E | 0.4333/* 0.0240 | 0.0984/0.6449 | 0.5462/* 0.0127 | ||
| F | 0.2629/0.1853 | 0.0604/0.7694 | 0.4335/0.0562 | ||
| Loudness | 0.2389/0.2301 | 0.1402/0.4945 | 0.5144/* 0.0203 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, C.-Y.; Li, D.-S.; Tsai, M.-H.; Chen, C.-H.; Cheng, Y.-F. The Impact of Acute Tinnitus on Listening Effort: A Study Based on Clinical Observations of Sudden Sensorineural Hearing Loss Patients. Int. J. Environ. Res. Public Health 2022, 19, 3661. https://doi.org/10.3390/ijerph19063661
Huang C-Y, Li D-S, Tsai M-H, Chen C-H, Cheng Y-F. The Impact of Acute Tinnitus on Listening Effort: A Study Based on Clinical Observations of Sudden Sensorineural Hearing Loss Patients. International Journal of Environmental Research and Public Health. 2022; 19(6):3661. https://doi.org/10.3390/ijerph19063661
Chicago/Turabian StyleHuang, Chii-Yuan, Dian-Sian Li, Ming-Hsien Tsai, Chih-Hao Chen, and Yen-Fu Cheng. 2022. "The Impact of Acute Tinnitus on Listening Effort: A Study Based on Clinical Observations of Sudden Sensorineural Hearing Loss Patients" International Journal of Environmental Research and Public Health 19, no. 6: 3661. https://doi.org/10.3390/ijerph19063661
APA StyleHuang, C.-Y., Li, D.-S., Tsai, M.-H., Chen, C.-H., & Cheng, Y.-F. (2022). The Impact of Acute Tinnitus on Listening Effort: A Study Based on Clinical Observations of Sudden Sensorineural Hearing Loss Patients. International Journal of Environmental Research and Public Health, 19(6), 3661. https://doi.org/10.3390/ijerph19063661