Translation and Cultural Adaptation into Portuguese of the Quality of Dying and Death Scale for Family Members of Patients in Intensive Care Units


Abstract
:1. Background
2. Methods
Study Design and Survey Development
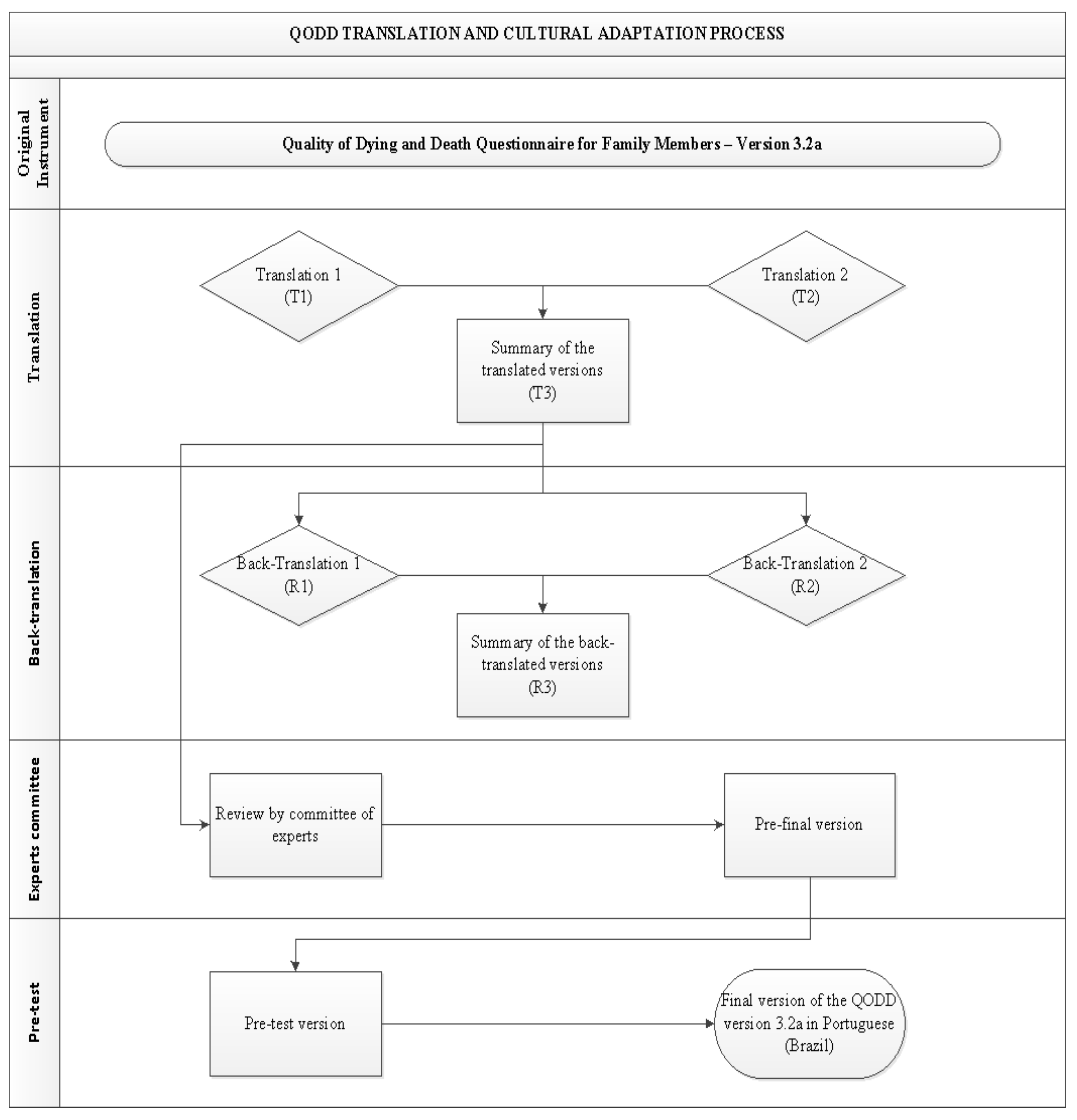
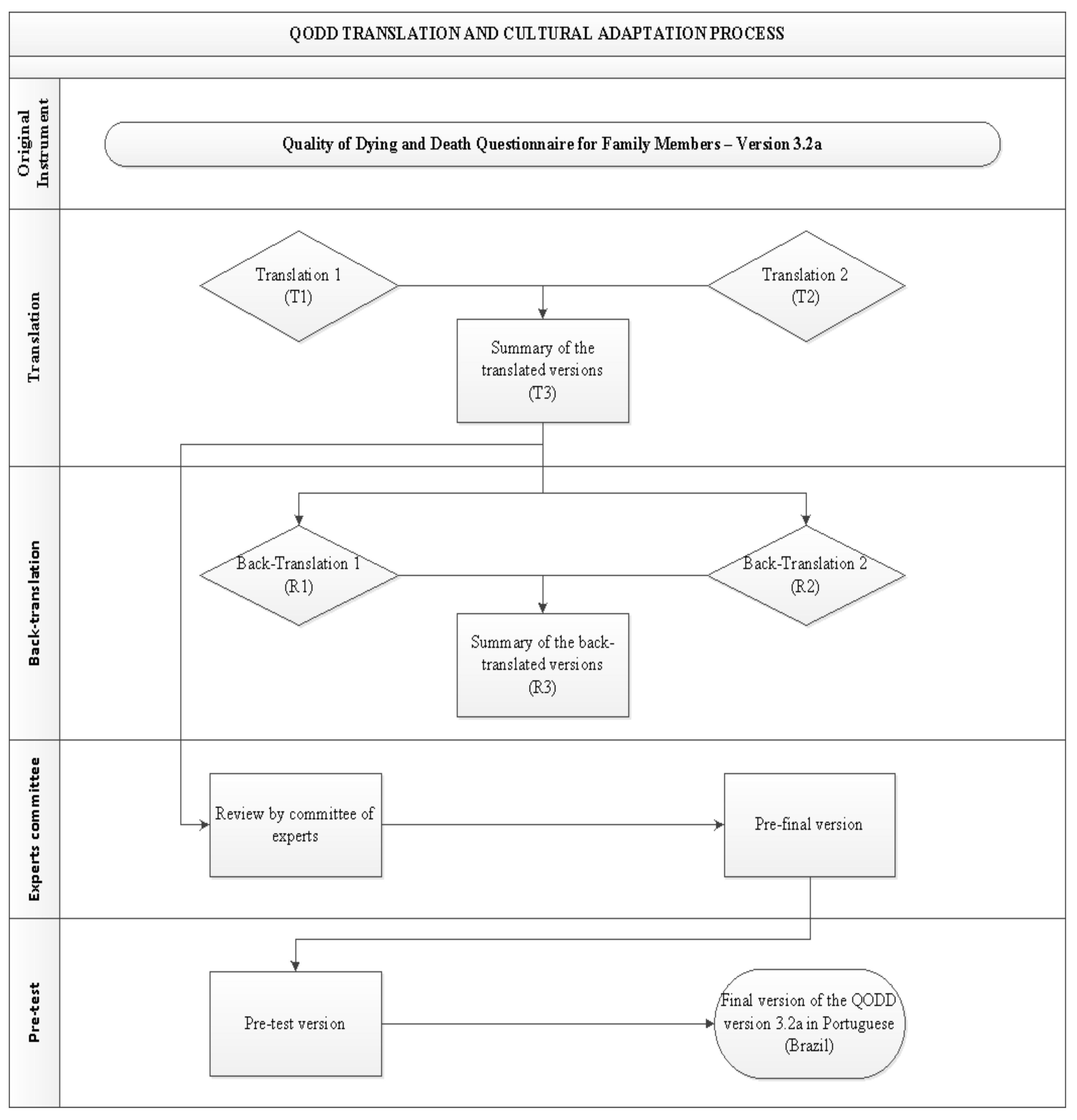
- Translation: It was carried out by two bilingual translators (Portuguese-English) who were native to Brazil and had no prior knowledge of the questionnaire. T1 and T2 were the new versions of the scale, and from these, the summary, T3, was obtained;
- Back-translation: This step was necessary to verify that the translated version reflected the same content as the original version, in addition to any inconsistencies [18]. As a result, version T3 was back-translated into English by two other bilingual natives who had no prior knowledge of the questionnaire, resulting in two back-translated versions named R1 and R2, which were later summarized into a single version named R3;
- Committee of Experts: The final translated version was evaluated by a Committee of Experts to obtain cross-cultural equivalence. For the Expert Committee, seven academics who had clinical experience and publications in the areas of intensive care, palliative care and protocol management were selected. They were selected, based on their scientific knowledge, from a national academic database called Platform Lattes. It is a database that contains all researchers’ curriculum details, their research groups, and areas of expertise from all higher education Brazilian institutions. Next, an invitation email was sent to each of the selected experts including a term of agreement, a copy of the translated instrument i.e., version T3 and a form with instructions as well as the study objectives and how to conduct their analysis/assessment. They used a Likert scale with a score from 1 to 4: 1 (non-representative item), 2 (item needs major revision to be representative), 3 (item needs minor revision to be representative) and 4 (relevant or representative item). The Committee also evaluated the instrument in three categories: semantics, idiomatic and cultural. A Committee of Experts evaluated Version T3 to determine cross-cultural equivalence. The content validity index (CVI) was calculated, considering notes 3 and 4, added and divided by the total number of responses, inferring adequacy of items with CVI ≥ 0.80 [19,20,21].The committee had 15 days to complete their preliminary analyses, and, after their feedback, a synthesis of their individual recommendations was carried out. A face-to-face meeting with the experts was not possible due to COVID-19 restrictions at the time.
- Pre-test phase: This phase was conducted with family members who agreed to participate in the study and responded to the pilot version of the instrument. Invitations to participate were made via telephone, followed the electronic access to QODD at the address. First, the participating institutions provided the list of patients who have died in their intensive care units in the last month. Next, we contacted via telephone potential respondents who were aged 18 or older and were closely involved in the dying process of their loved one in the period between 30 and 90 days after their death and consented to participated in the present study. Those individuals who reported not having emotional capacity or were not located were excluded. The sample was defined based on previous literature [18] that recommends between 30 to 40 participants for this stage which seeks to assess whether all items of the instrument were adequate and understandable to the target population.In addition to the items included in the pre-test version, participants answered a few additional questions: How many stars they would give the questionnaire, with 1 (one star) being the worst possible rating and 5 (five) stars being the best possible rating; and what may have made it difficult to understand while filling out. When the items had a minimum agreement of 75% in the positive responses, they were considered validated. Minor agreement items were thought to be subject to change [22]. Figure 1 depicts all stages of the translation and cultural adaptation process.This study obtained authorization from the authors of the original instrument, as well as, the consent of the Research Ethics Committee, according to the consubstantiated opinion number 2,772,325; and was structured according to guideline recommendations Standards for Quality Improvement Reporting Excellence (SQUIRE 2.0) [23], and by COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) [24].
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gellie, A.; Mills, A.; Levinson, M.; Stephenson, G.; Flynn, E. Death: A foe to be conquered? Questioning the paradigm. Age Ageing 2015, 44, 7–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patrick, D.L.; Engelberg, R.A.; Curtis, J.R. Evaluating the quality of dying and death. J. Pain Symptom Manag. 2001, 22, 717–726. [Google Scholar] [CrossRef]
- Brooks, L.A.; Manias, E.; Nicholson, P. Barriers, enablers and challenges to initiating end-of-life care in an Australian intensive care unit context. Aust. Crit. Care 2017, 30, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Gerritsen, R.T.; Hofhuis, J.G.M.; Koopmans, M.; van der Woude, M.; Bormans, L.; Hovingh, A.; Spronk, P.E. Perception by family members and ICU staff of the quality of dying and death in the ICU: A prospective multicenter study in The Netherlands. Chest 2013, 143, 357–363. [Google Scholar] [CrossRef]
- Mularski, R.; Curtis, J.R.; Osborne, M.; Engelberg, R.A.; Ganzini, L. Agreement among family members in their assessment of the Quality of Dying and Death. J. Pain. Symptom Manag. 2004, 28, 306–315. [Google Scholar] [CrossRef]
- Curtis, J.R.; Patrick, D.L.; Engelberg, R.A.; Norris, K.; Asp, C.; Byock, I. A measure of the quality of dying and death. Initial validation using after-death interviews with family members. J. Pain Symptom Manag. 2002, 24, 17–31. [Google Scholar] [CrossRef]
- Gerritsen, R.T.; Koopmans, M.; Hofhuis, J.G.M.; Curtis, J.R.; Jensen, H.I.; Zijlstra, J.G.; Engelberg, R.A.; Spronk, P.E. Comparing Quality of Dying and Death Perceived by Family Members and Nurses for Patients Dying in US and Dutch ICUs. Chest 2017, 151, 298–307. [Google Scholar] [CrossRef] [Green Version]
- Fortes, C.P.D.D.; Araújo, A.P.Q.C. Check list para tradução e Adaptação Transcultural de questionários em saúde. Cad. Saúde Colet 2019, 27, 202–209. [Google Scholar] [CrossRef]
- Curtis, J.R.; Downey, L.; Engelberg, R.A. The quality of dying and death: Is it ready for use as an outcome measure? Chest 2013, 143, 289–291. [Google Scholar] [CrossRef] [Green Version]
- Downey, L.; Curtis, J.R.; Lafferty, W.E.; Herting, J.R.; Engelberg, R.A. The Quality of Dying and Death Questionnaire (QODD): Empirical domains and theoretical perspectives. J. Pain Symptom Manag. 2010, 39, 9–22. [Google Scholar] [CrossRef]
- Fink-Samnick, E. The Evolution of End-of-Life Care: Ethical Implications for Case Management. Prof. Case Manag. 2016, 21, 180–192. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Cruz, P.E.; Perez, O.P.; Bonati, P.; Parisi, O.T.; Satt, L.T.; Otaiza, M.G.; Yáñez, D.C.; Morgado, A.M. Validation of the Spanish Version of the Quality of Dying and Death Questionnaire (QODD-ESP) in a Home-Based Cancer Palliative Care Program and Development of the QODD-ESP-12. J. Pain Symptom Manag. 2017, 53, 1042–1049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez, D.G.; Cuesta-Vargas, A.I. Cross-cultural adaptation and psychometric testing of the Quality of Dying and Death Questionnaire for the Spanish population. Eur. J. Oncol. Nurs. 2018, 33, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Heckel, M.; Bussmann, S.; Stiel, S.; Weber, M.; Ostgathe, C. Validation of the German version of the Quality of Dying and Death Questionnaire for Informal Caregivers (QODD-D-Ang). J. Pain Symptom Manag. 2015, 50, 402–413. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Mei, X.; Zhang, J.; Zhang, T.; Yin, A.; Qiu, F.; Liu, M. Validation of the Chinese Version of the Quality of Dying and Death Questionnaire for Family Members of ICU Patients. J. Pain Symptom Manag. 2021, 62, 599–608. [Google Scholar] [CrossRef]
- Moslemi, M.; Nikfarid, L.; Nourian, M.; Nasiri, M.; Rezayi, F. Translation, Cultural, and Age-Related Adaptation and Psychometric Properties of Persian Version of “Quality of Dying and Death” in Nurses Working in Neonatal Intensive Care Units. Indian J. Palliat. Care 2020, 26, 34–39. [Google Scholar]
- Glavan, B.J.; Engelberg, R.A.; Downey, L.; Curtis, J.R. Using the medical record to evaluate the quality of end-of-life care in the intensive care unit. Crit. Care Med. 2008, 36, 1138–1146. [Google Scholar] [CrossRef]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [Green Version]
- Newman, I.; Lim, J.; Pineda, F. Content Validity Using a Mixed Methods Approach: Its Application and Development Through the Use of a Table of Specifications Methodology. J. Mix. Methods Res. 2013, 7, 243–260. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T. The content validity index: Are you sure you know what’s being reported? Critique and recommendations. Res. Nurs. Health 2006, 29, 489–497. [Google Scholar] [CrossRef] [Green Version]
- Zamanzadeh, V.; Ghahramanian, A.; Rassouli, M.; Abbaszadeh, A.; Alavi-Majd, H.; Nikanfar, A.R. Design and Implementation Content Validity Study: Development of an instrument for measuring Patient-Centered Communication. J. Caring Sci. 2015, 4, 165–178. [Google Scholar] [CrossRef] [PubMed]
- Teles, L.M.R.; Oliveira, A.S.; Campos, F.C.; Lima, T.M.; Costa, C.C.; Gomes, L.F.S.; Oriá, M.O.B.; Damasceno, D.K.C. Development and validating an educational booklet for childbirth companions. Rev. Esc. Enferm. USP 2014, 48, 977–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogrinc, G.; Davies, L.; Goodman, D.; Batalden, P.; Davidoff, F.; Stevens, D. SQUIRE 2.0 (Standards for QUality Improvement Reporting Excellence): Revised publication guidelines from a detailed consensus process. BMJ Qual. Saf. 2016, 25, 986–992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mokkink, L.B.; Prinsen, C.A.C.; Bouter, L.M.; Vet, H.C.W.; Terwee, C.B. The COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) and how to select an outcome measurement instrument. Braz. J. Phys. Ther. 2016, 20, 105–113. [Google Scholar] [CrossRef] [Green Version]
- Lino, C.R.M.; Brüggemann, O.M.; Souza, M.L.; Barbosa, S.F.F.; Santos, E.K.A. The cross-cultural adaptation of research instruments, conducted by nurses in brazil: An integrative review. Texto Contexto-Enferm. 2017, 26, e1730017. [Google Scholar]
- Buonanno, P.; Jaiola, A.; Palumbo, C.; Spinelli, G.; Terminiello, V.; Servillo, G. Italian validation of the Amsterdam Preoperative Anxiety and Information Scale. Minerva Anestesiol. 2017, 83, 705–711. [Google Scholar] [CrossRef]
- Machado, R.S.; Oriá, M.O.B.; Fernandes, M.A.; Gouveia, M.T.O.; Silva, G.R.F. Translation and cultural adaptation of death attitude profile revised (DAP-r) for use in Brazil. Texto Contexto-Enferm. 2019, 28, e20180238. [Google Scholar] [CrossRef]
- Valer, D.B.; Aires, M.; Fengler, F.L.; Paskulin, L.M.G. Adaptation and validation of the Caregiver Burden Inventory for use with caregivers of elderly individuals. Rev. Latino-Am. Enferm. 2015, 23, 130–138. [Google Scholar] [CrossRef] [Green Version]
- Pirola, W.E.; Paiva, B.S.R.; Barroso, E.M.; Kissane, D.W.; Serrano, C.V.M.P.; Paiva, C.E. Translation and cultural adaptation of the Shame and Stigma Scale (SSS) into Portuguese (Brazil) to evaluate patients with head and neck cancer. Braz. J. Otorhinolaryngol. 2017, 83, 697–704. [Google Scholar] [CrossRef] [Green Version]
- Santana, M.T.E.A.; Gómez-Batiste, X.; Silva, L.M.G.; Gutiérrez, M.G.R. Cross-cultural adaptation and semantic validation of an instrument to identify palliative requirements in Portuguese. Einstein 2020, 18, 16794508. [Google Scholar] [CrossRef]

{kind=link}
| Item | Version | Text | IVC * | ||
|---|---|---|---|---|---|
| Semantics | Idiomatic | Cultural | |||
| Section I—Quality of the Dying and Death Process | |||||
| 5a | Original | How often did your loved one appear to feel at peace with dying? (Circle one number). | |||
| Translation | How often did your loved one seem to feel at peace with death? (Circle a number). | ||||
| Committee Outcome | How often did your loved one seem to feel at peace during the process of dying? (Circle a number). | 1.00 | 1.00 | 1.00 | |
| Guidance | Original | The following questions are answered with either a “Yes” or “No” based on whether your loved one did certain activities. Please rate the quality of that aspect of the dying experience. Again, we are asking you to focus on your loved one’s last several days. | |||
| Translation | The following questions should be answered with “Yes” or “No”, based on whether your loved one has performed certain activities or not. Please rate the quality of that aspect of the dying experience. Again, we ask that you focus on the last days of your loved one. | ||||
| Committee Outcome | The following questions should be answered with “Yes” or “No”, based on whether your loved one has performed or experienced any of the activities, procedures or situations listed in questions 11 through 21. Please rate the quality of that aspect of the dying process experience. Again, we ask that you focus on the last days of your loved one. | 1.00 | 1.00 | 1.00 | |
| 14a | Original | Did your loved one clear up any bad feelings with others? (Circle one number). | |||
| Translation | Has your loved one cleared up bad feelings with other people? (Circle a number). | ||||
| Committee Outcome | Has your loved one resolved any disagreements with someone or exposed their negative feelings to others? (Circle a number). | 1.00 | 1.00 | 0.86 | |
| 15a | Original | Did your loved one have one or more visits from a religious or spiritual advisor? (Circle one number). | |||
| Translation | Has your loved one received one or more visits from a religious or spiritual counselor? (Circle a number). | ||||
| Committee Outcome | Has your loved one received one or more visits from a religious or spiritual leader? (Circle a number). | 1.00 | 1.00 | 1.00 | |
| 16a | Original | Did your loved one have a spiritual service or ceremony before his/her death? (Circle one number). | |||
| Translation | Did your loved one have a spiritual service or ceremony before they died? (Circle a number). | ||||
| Committee Outcome | Did your loved one receive any religious or ritual visits before they died? (Circle a number). | 1.00 | 1.00 | 0.86 | |
| 17a | Original | Did your loved one receive a mechanical ventilator (respirator) to breathe for him/her? (Circle one number). | |||
| Translation | Has your loved one received a mechanical ventilator (respirator) to breathe for him? (Circle a number). | ||||
| Committee Outcome | Was your loved one under artificial respiration, that is, was he placed on mechanical ventilation (respirator) to breathe for him? (Circle a number). | 0.86 | 0.86 | 0.86 | |
| 18a | Original | Did your loved one receive dialysis for his/her kidneys? (Circle one number). | |||
| Translation | Has your loved one received kidney dialysis? (Circle a number). | ||||
| Committee Outcome | Did your loved one undergo kidney dialysis? (Circle a number). | 1.00 | 1.00 | 1.00 | |
| 19a | Original | Did your loved one have his or her funeral arrangements in order prior to death? (Circle one number). | |||
| Translation | Did your loved one have funeral arrangements in place prior to his death? (Circle a number). | ||||
| Committee Outcome | Were your loved one’s funeral arrangements organized before his death? (Circle a number). | 0.86 | 0.86 | 0.86 | |
| 20a | Original | Did your loved one discuss his or her wishes for end-of-life care with his/her doctor—for example, resuscitation or intensive care? (Circle one number). | |||
| Translation | Your loved one discussed your wishes for care at the end of life with his doctor, for example, resuscitation or intensive care? (Circle a number). | ||||
| Committee Outcome | Your loved one discussed his wishes with his doctor about how he would like to be cared for at the end of his life, for example, resuscitation or intensive care? (Circle a number). | 1.00 | 1.00 | 1.00 | |
| 21a | Original | Was anyone present at the moment of your loved one’s death? (Circle one number). | |||
| Translation | Was anyone present at the moment of the death of your loved one? (Circle a number). | ||||
| Committee Outcome | Some family members were present at the moment of the death of your loved one? (Circle a number). | 1.00 | 1.00 | 1.00 | |
| 1–22b | Original | How would you rate this aspect of your loved one’s death? (Circle one number). | |||
| Translation | How would you rate this aspect of your loved one’s death? (Circle a number). | ||||
| Committee Outcome | How would you rate this experience of the death of your loved one? (Circle a number). | 1.00 | 1.00 | 1.00 | |
| 25 | Original | Rate the care your loved one received from his or her doctor during the last several days of his or her life while in the ICU. (Circle the number). | |||
| Translation | Rate the care your loved one received from his doctor in the last days of his life while he was in the ICU. (Circle a number). | ||||
| Committee Outcome | Rate the care that your loved one received from his doctor (assistant or intensive care) in the last days of his life while he was in the ICU. (Circle a number). | 1.00 | 1.00 | 0.86 | |
| Section II—Sociodemographic characterization | |||||
| 1 | Original | When were you born? (Please write the year). | |||
| Translation | When were you born? (Please write the year). | ||||
| Committee Outcome | In what year were you born? (Please write the year). | 1.00 | 1.00 | 0.86 | |
| 2 | Original | When was your loved one born? (Please write the year). | |||
| Translation | When was your loved one born? (Please write the year). | ||||
| Committee Outcome | In what year was your loved one born? (Please write the year). | 1.00 | 1.00 | 1.00 | |
| 7 | Original | What is your ethnicity? (Circle one number). 1. Hispanic or 2. Non-Hispanic. | |||
| Translation | What is your ethnicity? (Circle a number). 1. Brazilian or 2. Non-Brazilian. | ||||
| Committee result | What’s your nationality? (Circle a number). 1. Brazilian or 2 Non-Brazilian. | 1.00 | 1.00 | 1.00 | |
| 8 | Original | What is your race? (Circle all that apply). 1. White 2. Black/African American 3. Asian 4. Pacific Islander 5. Native American or Alaskan 6. Native 7. Other (please specify) | |||
| Translation | What is your race? (Circle all that fit). 1. White 2. Black/African American 3. Yellow/Asian 4. Brown 5. Indigenous 6. Other (please specify) | ||||
| Committee Outcome | What is your ethnicity? (Circle all that fit). 1. White 2. Black/African American 3. Yellow/Asian 4. Brown 5. Indigenous 6. Other (please specify) | 1.00 | 1.00 | 1.00 | |
| 10 | Original | How are you related to your loved one? (Circle one number). | |||
| Translation | What is your relationship with your loved one? (Circle a number). | ||||
| Committee Outcome | What is the degree of kinship with your loved one? (Circle a number). | 1.00 | 1.00 | 1.00 | |
| 11 | Original | Did you live with your loved one? (Circle one number). | |||
| Translation | Did you live or lived with your loved one? (Circle a number). | ||||
| Committee Outcome | Did you live or lived with your loved one? (Circle a number). | 0.86 | 0.86 | 0.86 | |
| 12 | Original | How long have you known your loved one? (Please fill in). | |||
| Translation | How long have you known your loved one? (Please complete). | ||||
| Committee Outcome | There is how long have you known your loved one? (Please complete). | 1.00 | 1.00 | 1.00 | |
| 14 | Original | We would like to get feedback from you on how burdensome it was to complete this questionnaire. This information will help guide us in future research. Overall, how much of a burden on you was this questionnaire? (Circle one number). | |||
| Translation | Please tell us how hard it was to complete this questionnaire. This information will help us to direct our future research. Overall, how laborious was this questionnaire for you? (Circle a number). | ||||
| Committee Outcome | Please tell us How hard was it for you to complete this questionnaire? This information will help us to direct our future research. Considering 0 (zero) as not at all laborious, and 10 (ten) as very laborious. (Circle a number). | 1.00 | 1.00 | 1.00 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meneguin, S.; Benichel, C.R.; Morais, J.F.; Oliveira, C.d. Translation and Cultural Adaptation into Portuguese of the Quality of Dying and Death Scale for Family Members of Patients in Intensive Care Units. Int. J. Environ. Res. Public Health 2022, 19, 3614. https://doi.org/10.3390/ijerph19063614
Meneguin S, Benichel CR, Morais JF, Oliveira Cd. Translation and Cultural Adaptation into Portuguese of the Quality of Dying and Death Scale for Family Members of Patients in Intensive Care Units. International Journal of Environmental Research and Public Health. 2022; 19(6):3614. https://doi.org/10.3390/ijerph19063614
Chicago/Turabian StyleMeneguin, Silmara, Cariston Rodrigo Benichel, José Fausto Morais, and Cesar de Oliveira. 2022. "Translation and Cultural Adaptation into Portuguese of the Quality of Dying and Death Scale for Family Members of Patients in Intensive Care Units" International Journal of Environmental Research and Public Health 19, no. 6: 3614. https://doi.org/10.3390/ijerph19063614
APA StyleMeneguin, S., Benichel, C. R., Morais, J. F., & Oliveira, C. d. (2022). Translation and Cultural Adaptation into Portuguese of the Quality of Dying and Death Scale for Family Members of Patients in Intensive Care Units. International Journal of Environmental Research and Public Health, 19(6), 3614. https://doi.org/10.3390/ijerph19063614