
COVID-19 Disease Burden Related to Social Vulnerability and Comorbidities: Challenges to Tuberculosis Control



Abstract
:1. Introduction
2. Material and Methods
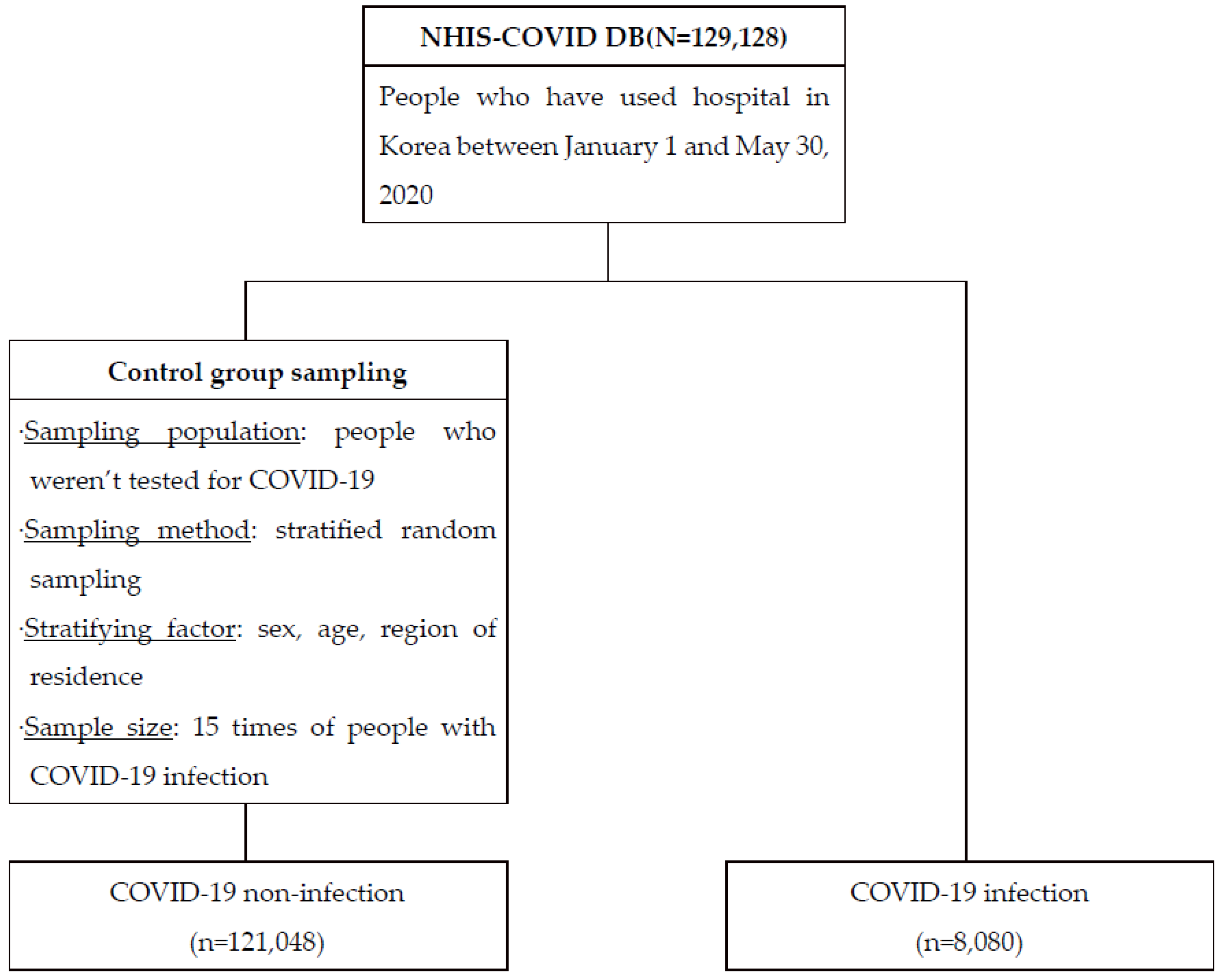
2.1. Data Collection and Study Participants
2.2. Statistical Analysis
2.3. Ethics Statement
3. Results
3.1. COVID-19 Patient Characteristics
3.2. TB and COVID-19 Infection, ICU Admission, and Mortality
3.3. Logistic Regression Analysis for SARS-CoV-2 Infection
3.4. Logistic Regression Analysis for ICU Admission in COVID-19 Patients
3.5. Logistic Regression Analysis for COVID-19 Death in COVID-19 Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Weekly Operational Update on COVID-19; World Health Organization (WHO): Geneva, Switzerland, 2021; Volume 53, pp. 1–10. [Google Scholar]
- World Health Organization. Rapid Communication on Forthcoming Changes to the Programmatic Management of Tuberculosis Preventive Treatment. Available online: http://apps.who.int/bookorders. (accessed on 21 March 2020).
- Lim, W.S.; Liang, C.K.; Assantachai, P.; Auyeung, T.W.; Kang, L.; Lee, W.J.; Lim, J.; Sugimoto, K.; Akishita, M.; Chia, S.; et al. COVID-19 and older people in Asia: Asian Working Group for Sarcopenia calls to actions. Geriatr. Gerontol. Int. 2020, 20, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Courtenay, K.; Perera, B. Courtenay and Perera, COVID-19 and people with intellectual disability: Impacts of a pandemic. Ir. J. Psychol. Med. 2020, 37, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; Guo, Q.; Ji, R.; Wang, H.; Wang, Y.; Zhou, Y. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Ejaz, H.; Alsrhani, A.; Zafar, A.; Javed, H.; Junaid, K.; Abdalla, A.E.; Abosalif, K.O.A.; Ahmed, Z.; Younas, S. COVID-19 and comorbidities: Deleterious impact on infected patients. J. Infect. Public Health 2020, 13, 1833–1839. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Wang, Y.; Fleming, J.; Yu, Y.; Gu, Y.; Liu, C.; Fan, L.; Wang, X.; Cheng, M.; Bi, L.; et al. Active or latent tuberculosis increases susceptibility to COVID-19 and disease severity. MedRxiv 2020, 165, 1–13. [Google Scholar]
- Korea Centers for Disease Control and Prevention. 2020 Annual Report on the Notified Tuberculosis in Korea. Available online: https://www.kdca.go.kr/board/board.es?mid=a20602010000&bid=0034&act=view&list_no=712904 (accessed on 1 September 2021).
- Udwadia, Z.F.; Vora, A.; Tripathi, A.R.; Malu, K.N.; Lange, C.; Raju, R.S. COVID-19 -Tuberculosis interactions: When dark forces collide. Indian J. Tuberc. 2020, 67, S155–S162. [Google Scholar] [CrossRef] [PubMed]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.M.; Sundararajan, V. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grief, S.N.; Miller, J.P. Infectious Disease Issues in Underserved Populations. Prim. Care Clin. Off. Pr. 2017, 44, 67–85. [Google Scholar] [CrossRef] [PubMed]
- Quinn, S.C.; Kumar, S. Health Inequalities and Infectious Disease Epidemics: A Challenge for Global Health Security. Biosecurity Bioterrorism Biodefense Strategy Pract. Sci. 2014, 12, 263–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cannistraci, C.V.; Valsecchi, M.G.; Capua, I. Age-sex population adjusted analysis of disease severity in epidemics as a tool to devise public health policies for COVID-19. Sci. Rep. 2021, 11, 11787. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-Q.; Gou, R.; Diao, Y.-S.; Yin, Q.-H.; Fan, W.-X.; Liang, Y.-P.; Chen, Y.; Wu, M.; Zang, L.; Li, L.; et al. Charlson comorbidity index helps predict the risk of mortality for patients with type 2 diabetic nephropathy. J. Zhejiang Univ. Sci. B 2014, 15, 58–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuswardhani, R.T.; Henrina, J.; Pranata, R.; Lim, M.A.; Lawrensia, S.; Suastika, K. Charlson comorbidity index and a composite of poor outcomes in COVID-19 patients: A systematic review and meta-analysis. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 2103–2109. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Park, S.Y.; Seon, J.Y.; Jeon, W.H.; Nam, S.I.; Park, J.H.; Park, J.S.; Kim, H.Y.; Thakkar, N.; Selvaraj, P.; et al. Intensive Care Unit Capacity and Its Associated Risk Factors During the COVID-19 Surge in the Republic of Korea: Analysis Using Nationwide Health Claims Data. Risk Manag. Healthc. Policy. 2020, 2020, 2571–2581. [Google Scholar] [CrossRef] [PubMed]
- Chakrabarti, B.; Calverley, P.M.; Davies, P.D. Tuberculosis and its incidence, special nature, and relationship with chronic obstructive pulmonary disease. Int. J. Chron. Obstruct. Pulmon. Dis. 2007, 2, 263–272. [Google Scholar] [PubMed]
- Sy, K.T.L.; Haw, N.J.L.; Uy, J. Previous and active tuberculosis increases risk of death and prolongs recovery in patients with COVID-19. Infect. Dis. 2020, 52, 902–907. [Google Scholar] [CrossRef] [PubMed]
- Korea Disease Control and Prevention Agency. 2019 Annual Report on the Notified Tuberculosis in Korea. 2019. Available online: https://nih.go.kr/board/board.es?mid=a40303030000&bid=0034&act=view&list_no=366715 (accessed on 1 September 2021).
- Central Disease Control Headquarters. 2020 Coronavirus Infectious Disease-19 Response Guidelines (7th Edition). 2020. Available online: https://www.kdca.go.kr/board/board.es?mid=a20507020000&bid=0019 (accessed on 1 September 2021).

{kind=link}
| SARS-CoV-2 Infection | ICU Admission | COVID-19 Death | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No | Yes | p-Value | No | Yes | p-Value | No | Yes | p-Value | ||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | |||||
| Sex | Male | 48,539 | 93.7 | 3244 | 6.3 | 1 | 2729 | 84.1 | 515 | 15.9 | <0.0001 * | 3108 | 95.8 | 136 | 4.2 | <0.0001 * |
| Female | 72,509 | 93.7 | 4836 | 6.3 | 4331 | 89.6 | 505 | 10.4 | 4724 | 97.7 | 112 | 2.3 | ||||
| Age, yr | 0–59 | 87,733 | 93.7 | 5856 | 6.3 | 1 | 5314 | 90.7 | 542 | 9.3 | <0.0001 * | 5836 | 99.7 | 20 | 0.3 | <0.0001 * |
| 60–69 | 17,985 | 93.7 | 1200 | 6.3 | 995 | 82.9 | 205 | 17.1 | 1162 | 96.8 | 38 | 3.2 | ||||
| 70–79 | 9255 | 93.7 | 618 | 6.3 | 467 | 75.6 | 151 | 24.4 | 552 | 89.3 | 66 | 10.7 | ||||
| 80+ | 6075 | 93.7 | 406 | 6.3 | 284 | 70.0 | 122 | 30.0 | 282 | 69.5 | 124 | 30.5 | ||||
| Region of residence | Seoul | 8160 | 93.7 | 549 | 6.3 | 1 | 446 | 81.2 | 103 | 18.8 | <0.0001 * | 545 | 99.3 | 4 | 0.7 | <0.0001 * |
| Daegu | 78,960 | 93.8 | 5264 | 6.3 | 4835 | 91.9 | 429 | 8.1 | 5112 | 97.1 | 152 | 2.9 | ||||
| Gyeonggi-do | 6764 | 93.7 | 455 | 6.3 | 336 | 73.8 | 119 | 26.2 | 438 | 96.3 | 17 | 3.7 | ||||
| Gyeongsangbuk-do | 14,340 | 93.8 | 956 | 6.3 | 837 | 87.6 | 119 | 12.4 | 901 | 94.2 | 55 | 5.8 | ||||
| Others | 12,824 | 93.7 | 856 | 6.3 | 606 | 70.8 | 250 | 29.2 | 836 | 97.7 | 20 | 2.3 | ||||
| Health insurance premium | Medical aid | 6560 | 89.1 | 803 | 10.9 | <0.0001 * | 661 | 82.3 | 142 | 17.7 | <0.0001 * | 754 | 93.9 | 49 | 6.1 | <0.0001 * |
| 1st quintile (lowest) | 22,807 | 93.4 | 1602 | 6.6 | 1433 | 89.5 | 169 | 10.5 | 1565 | 97.7 | 37 | 2.3 | ||||
| 2nd quintile | 18,039 | 94.2 | 1102 | 5.8 | 994 | 90.2 | 108 | 9.8 | 1082 | 98.2 | 20 | 1.8 | ||||
| 3rd quintile | 20,518 | 94.0 | 1312 | 6.0 | 1157 | 88.2 | 155 | 11.8 | 1280 | 97.6 | 32 | 2.4 | ||||
| 4th quintile | 22,941 | 94.5 | 1348 | 5.5 | 1188 | 88.1 | 160 | 11.9 | 1310 | 97.2 | 38 | 2.8 | ||||
| 5th quintile (highest) | 30,183 | 94.0 | 1913 | 6.0 | 1627 | 85.0 | 286 | 15.0 | 1841 | 96.2 | 72 | 3.8 | ||||
| CCI Score | 0 | 99,311 | 93.9 | 6469 | 6.1 | <0.0001 * | 5742 | 88.8 | 727 | 11.2 | <0.0001 * | 6381 | 98.6 | 88 | 1.4 | <0.0001 * |
| 1 | 10,603 | 93.7 | 710 | 6.3 | 606 | 85.4 | 104 | 14.6 | 666 | 93.8 | 44 | 6.2 | ||||
| 2 | 8573 | 92.7 | 680 | 7.3 | 545 | 80.1 | 135 | 19.9 | 604 | 88.8 | 76 | 11.2 | ||||
| 3+ | 2561 | 92.1 | 221 | 7.9 | 167 | 75.6 | 54 | 24.4 | 181 | 81.9 | 40 | 18.1 | ||||
| Tuberculosis | No | 120,845 | 93.7 | 8067 | 6.3 | 0.8847 | 7053 | 87.4 | 1014 | 12.6 | 0.0003 * | 7821 | 97.0 | 246 | 3.0 | 0.01 * |
| Yes | 203 | 94.0 | 13 | 6.0 | 7 | 53.8 | 6 | 46.2 | 11 | 84.6 | 2 | 15.4 | ||||
| Multivariate Model 1 | Multivariate Model 2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Adjusted OR | 95% CI | p-Value | Adjusted OR | 95% CI | p-Value | ||||
| LB | UB | LB | UB | ||||||
| Health insurance premium | Medical aid | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) |
| 1st quintile (lowest) | 0.584 | 0.534 | 0.639 | <0.0001 * | 0.604 | 0.552 | 0.661 | <0.0001 * | |
| 2nd quintile | 0.509 | 0.463 | 0.56 | <0.0001 * | 0.528 | 0.479 | 0.582 | <0.0001 * | |
| 3rd quintile | 0.532 | 0.485 | 0.584 | <0.0001 * | 0.551 | 0.502 | 0.605 | <0.0001 * | |
| 4rd quintile | 0.488 | 0.445 | 0.535 | <0.0001 * | 0.505 | 0.46 | 0.555 | <0.0001 * | |
| 5th quintile (highest) | 0.524 | 0.481 | 0.572 | <0.0001 * | 0.542 | 0.496 | 0.592 | <0.0001 * | |
| CCI Score | 0 | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) |
| 1 | 1.005 | 0.927 | 1.089 | 0.9108 | 0.992 | 0.915 | 1.075 | 0.8394 | |
| 2 | 1.173 | 1.081 | 1.274 | 0.0001 * | 1.152 | 1.06 | 1.251 | 0.0008 * | |
| 3+ | 1.23 | 1.069 | 1.416 | 0.0039 * | 1.19 | 1.033 | 1.371 | 0.0159 * | |
| Tuberculosis | No | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) |
| Yes | 0.895 | 0.51 | 1.571 | 0.6993 | 0.884 | 0.504 | 1.553 | 0.6689 | |
| Multivariate Model 1 | Multivariate Model 2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Adjusted OR | 95% CI | p-Value | Adjusted OR | 95% CI | p-Value | ||||
| LB | UB | LB | UB | ||||||
| Sex | Male | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) |
| Female | 0.656 | 0.57 | 0.754 | <0.0001 * | 0.672 | 0.584 | 0.774 | <0.0001 * | |
| Age, yr | 0–59 | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) |
| 60–69 | 2.447 | 2.025 | 2.956 | <0.0001 * | 2.338 | 1.933 | 2.829 | <0.0001 * | |
| 70–79 | 3.957 | 3.158 | 4.958 | <0.0001 * | 3.685 | 2.933 | 4.629 | <0.0001 * | |
| 80+ | 4.897 | 3.731 | 6.427 | <0.0001 * | 4.437 | 3.363 | 5.855 | <0.0001 * | |
| Region of residence | Seoul | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) |
| Daegu | 0.276 | 0.215 | 0.355 | <0.0001 * | 0.271 | 0.211 | 0.348 | <0.0001 * | |
| Gyeonggi-do | 1.346 | 0.986 | 1.837 | 0.0613 | 1.32 | 0.967 | 1.802 | 0.0807 | |
| Gyeongsangbuk-do | 0.353 | 0.259 | 0.48 | <0.0001 * | 0.332 | 0.243 | 0.452 | <0.0001 * | |
| Others | 1.67 | 1.277 | 2.184 | 0.0002 * | 1.651 | 1.263 | 2.159 | 0.0002 * | |
| Health insurance premium | Medical aid | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) |
| 1st quintile (lowest) | 0.594 | 0.459 | 0.769 | <0.0001 * | 0.67 | 0.514 | 0.873 | 0.003 * | |
| 2nd quintile | 0.555 | 0.417 | 0.739 | <0.0001 * | 0.639 | 0.476 | 0.859 | 0.003 * | |
| 3nd quintile | 0.639 | 0.49 | 0.832 | 0.0009 * | 0.735 | 0.559 | 0.965 | 0.0269 * | |
| 4nd quintile | 0.521 | 0.4 | 0.679 | <0.0001 * | 0.598 | 0.455 | 0.785 | 0.0002 * | |
| 5th quintile (highest) | 0.589 | 0.463 | 0.75 | <0.0001 * | 0.676 | 0.527 | 0.869 | 0.0022 * | |
| CCI Score | 0 | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) |
| 1 | 1.129 | 0.888 | 1.436 | 0.3211 | 1.099 | 0.864 | 1.398 | 0.4429 | |
| 2 | 1.383 | 1.098 | 1.742 | 0.0058 * | 1.362 | 1.081 | 1.718 | 0.0089 * | |
| 3+ | 1.342 | 0.938 | 1.919 | 0.1072 | 1.302 | 0.907 | 1.868 | 0.1525 | |
| Tuberculosis | No | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) |
| Yes | 4.087 | 1.223 | 13.663 | 0.0222 * | 4.278 | 1.272 | 14.386 | 0.0188 * | |
| Multivariate Model 1 | Multivariate Model 2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Adjusted OR | 95% CI | p-Value | Adjusted OR | 95% CI | p-Value | ||||
| LB | UB | LB | UB | ||||||
| Sex | Male | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) |
| Female | 0.403 | 0.3 | 0.54 | <0.0001 * | 0.412 | 0.307 | 0.553 | <0.0001 * | |
| Age, yr | 0–59 | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) |
| 60–69 | 7.154 | 4.104 | 12.472 | <0.0001 * | 6.83 | 3.91 | 11.933 | <0.0001 * | |
| 70–79 | 25.366 | 15.027 | 42.819 | <0.0001 * | 24.083 | 14.237 | 40.738 | <0.0001 * | |
| 80+ | 89.827 | 53.219 | 151.615 | <0.0001 * | 83.672 | 49.39 | 141.75 | <0.0001 * | |
| Region of residence | Seoul | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) |
| Daegu | 2.36 | 0.792 | 7.033 | 0.1232 | 2.255 | 0.759 | 6.698 | 0.1434 | |
| Gyeonggi-do | 3.807 | 1.133 | 12.798 | 0.0307 * | 3.54 | 1.054 | 11.887 | 0.0408 * | |
| Gyeongsangbuk-do | 2.791 | 0.907 | 8.589 | 0.0734 | 2.627 | 0.856 | 8.062 | 0.0914 | |
| Others | 2.662 | 0.815 | 8.699 | 0.105 | 2.498 | 0.765 | 8.156 | 0.1296 | |
| Health insurance premium | Medical aid | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) |
| 1st quintile (lowest) | 0.476 | 0.29 | 0.782 | 0.0034* | 0.51 | 0.31 | 0.842 | 0.0084 * | |
| 2nd quintile | 0.54 | 0.3 | 0.974 | 0.0405 * | 0.601 | 0.331 | 1.092 | 0.095 | |
| 3nd quintile | 0.691 | 0.414 | 1.154 | 0.158 | 0.773 | 0.459 | 1.301 | 0.332 | |
| 4nd quintile | 0.496 | 0.304 | 0.808 | 0.0049 * | 0.547 | 0.333 | 0.898 | 0.017 * | |
| 5th quintile (highest) | 0.507 | 0.329 | 0.782 | 0.0021 * | 0.556 | 0.358 | 0.863 | 0.0089 * | |
| CCI Score | 0 | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) |
| 1 | 2.82 | 1.871 | 4.251 | <0.0001 * | 2.744 | 1.82 | 4.139 | <0.0001 * | |
| 2 | 2.67 | 1.856 | 3.84 | <0.0001 * | 2.618 | 1.818 | 3.771 | <0.0001 * | |
| 3+ | 2.395 | 1.504 | 3.813 | 0.0002 * | 2.314 | 1.449 | 3.694 | 0.0004 * | |
| Tuberculosis | No | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) |
| Yes | 2.505 | 0.414 | 15.165 | 0.3175 | 2.588 | 0.415 | 16.137 | 0.3086 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.W.; Seon, J.Y.; Lee, S.H.; Oh, I.H. COVID-19 Disease Burden Related to Social Vulnerability and Comorbidities: Challenges to Tuberculosis Control. Int. J. Environ. Res. Public Health 2022, 19, 3597. https://doi.org/10.3390/ijerph19063597
Lee YW, Seon JY, Lee SH, Oh IH. COVID-19 Disease Burden Related to Social Vulnerability and Comorbidities: Challenges to Tuberculosis Control. International Journal of Environmental Research and Public Health. 2022; 19(6):3597. https://doi.org/10.3390/ijerph19063597
Chicago/Turabian StyleLee, Yeo Wool, Jeong Yeon Seon, Seung Heon Lee, and In Hwan Oh. 2022. "COVID-19 Disease Burden Related to Social Vulnerability and Comorbidities: Challenges to Tuberculosis Control" International Journal of Environmental Research and Public Health 19, no. 6: 3597. https://doi.org/10.3390/ijerph19063597
APA StyleLee, Y. W., Seon, J. Y., Lee, S. H., & Oh, I. H. (2022). COVID-19 Disease Burden Related to Social Vulnerability and Comorbidities: Challenges to Tuberculosis Control. International Journal of Environmental Research and Public Health, 19(6), 3597. https://doi.org/10.3390/ijerph19063597