
Reliability of Tooth Width Measurements Delivered by the Clin-Check Pro 6.0 Software on Digital Casts: A Cross-Sectional Study

 , ,
, ,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Intra- and Inter-Operator Reliability
3.2. Clin-Check Pro 6.0 Software within Method Reliability (Repeatablility)
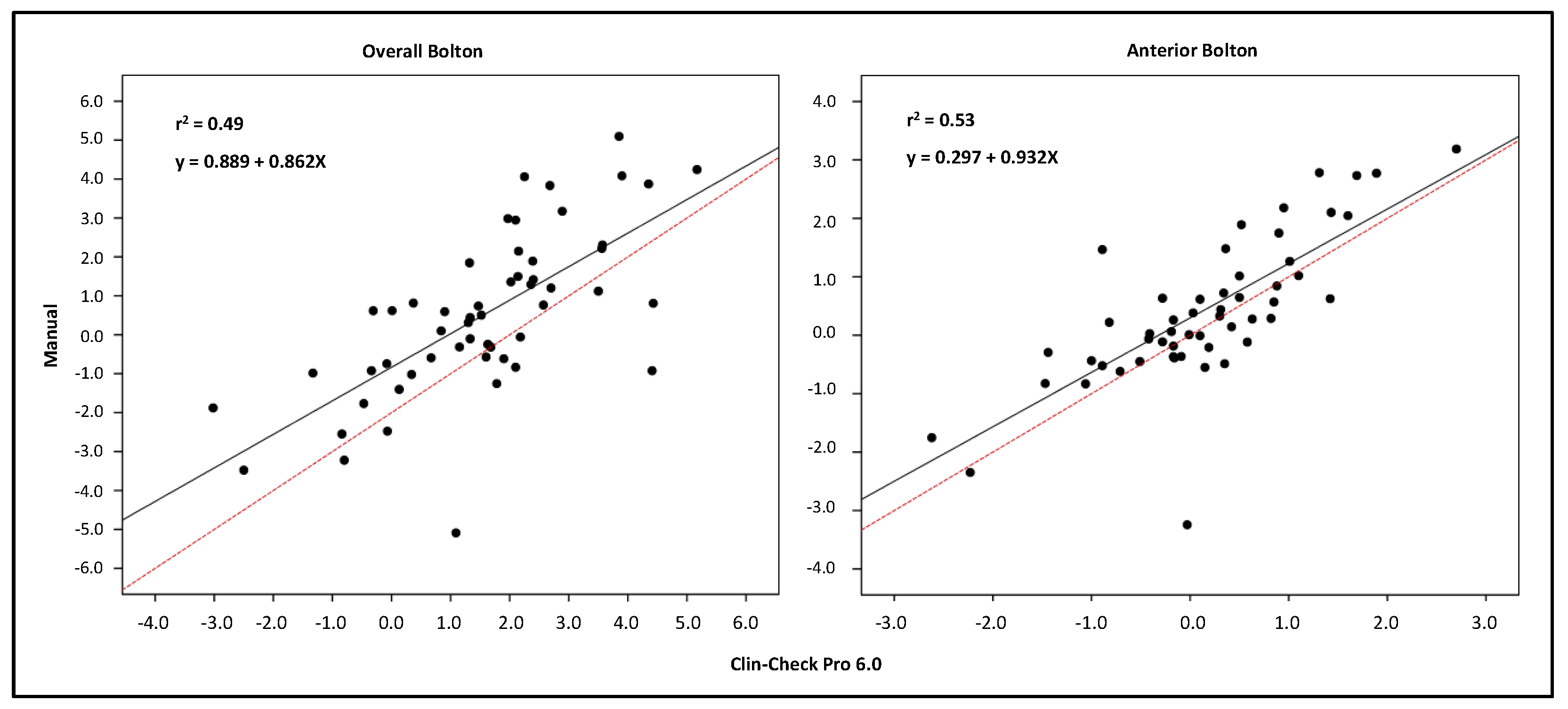
3.3. Agreement between the Manual Method and Clin-Check Pro 6.0 Software
4. Discussion
4.1. Inter- and Inter-Operator Reliability
4.2. Clin-Check Pro 6.0 Software within Method Reliability (Repeatablility)
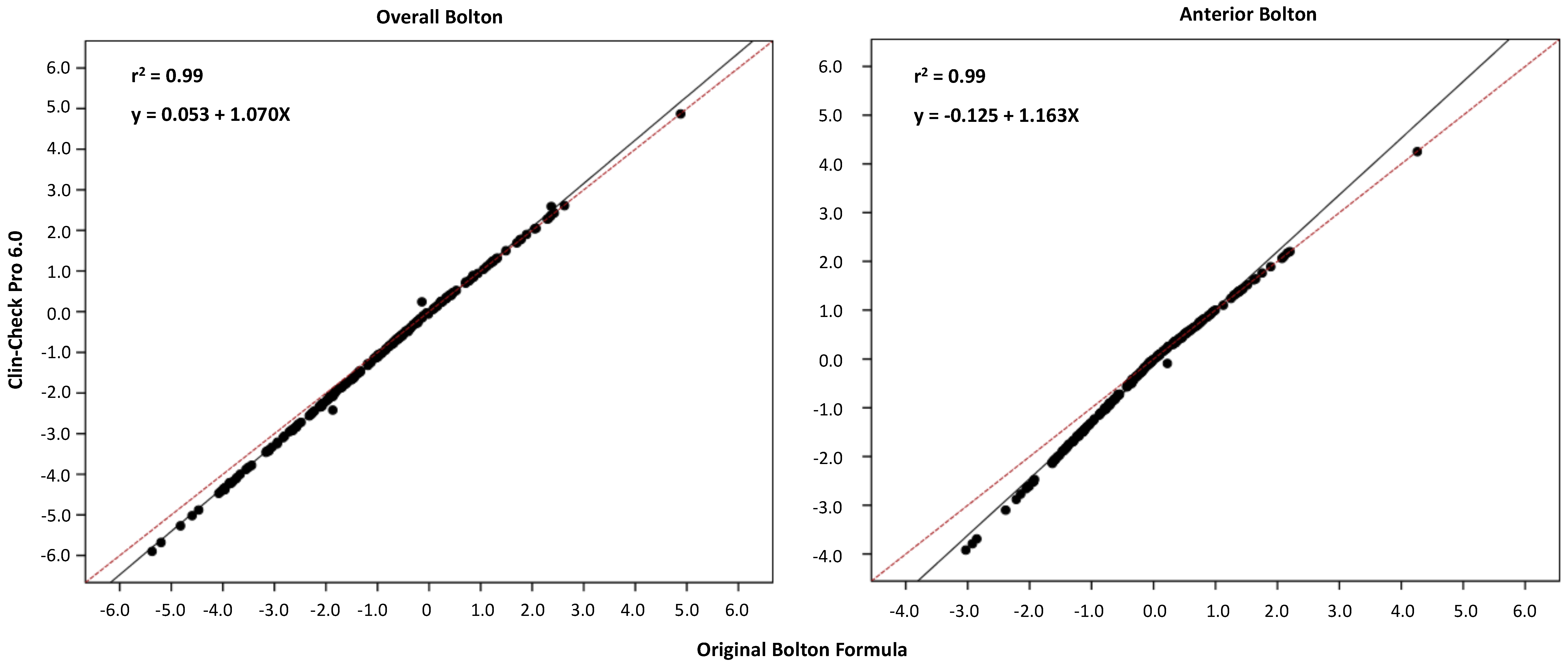
4.3. Agreement between the Manual Method and Clin-Check Pro 6.0 Software
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Daniele, G.; Matilde, S.-S.A.; María, M.; Rafael, R.V.; Milagros, A.M. Sex estimation by tooth dimension in a contemporary Spanish population. Forensic Sci. Int. 2020, 317, 110549. [Google Scholar] [CrossRef] [PubMed]
- Machado, V.; Botelho, J.; Pereira, D.; Vasques, M.; Fernandes-Retto, P.; Proença, L.; Mendes, J.J.; Delgado, A. Bolton ratios in Portuguese subjects among different malocclusion groups. J. Clin. Exp. Dent. 2018, 10, e864–e868. [Google Scholar] [CrossRef] [PubMed]
- Santoro, M.; Ayoub, M.E.; Pardi, V.A.; Cangialosi, T.J. Mesiodistal crown dimensions and tooth size discrepancy of the permanent dentition of Dominican Americans. Angle Orthod. 2000, 70, 303–307. [Google Scholar] [CrossRef]
- Bernabé, E.; Major, P.W.; Flores-Mir, C. Tooth-width ratio discrepancies in a sample of Peruvian adolescents. Am. J. Orthod. Dentofac. Orthop. 2004, 125, 361–365. [Google Scholar] [CrossRef] [PubMed]
- Cavalcante, R.C.; de Lucas Corso, P.F.C.; dos Santos Trento, G.; Antonini, F.; Rebellato, N.L.B.; da Costa, D.J.; Scariot, R.; Klüppel, L.E. Segmental orthognathic surgery for Bolton discrepancy correction. Oral Maxillofac. Surg. Cases 2018, 4, 108–114. [Google Scholar] [CrossRef]
- De Luca Canto, G.; Pachêco-Pereira, C.; Lagravere, M.O.; Flores-Mir, C.; Major, P.W. Intra-arch dimensional measurement validity of laser-scanned digital dental models compared with the original plaster models: A systematic review. Orthod. Craniofac. Res. 2015, 18, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Rossini, G.; Parrini, S.; Castroflorio, T.; Deregibus, A.; Debernardi, C.L. Diagnostic accuracy and measurement sensitivity of digital models for orthodontic purposes: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Fleming, P.S.; Marinho, V.; Johal, A. Orthodontic measurements on digital study models compared with plaster models: A systematic review. Orthod. Craniofac. Res. 2011, 14, 1–16. [Google Scholar] [CrossRef]
- Align Technology Announces Second Quarter 2020 Financial Results1 Millionth Invisalign Patient Milestone in APAC—Tokyo, Japan. Available online: https://www.biospace.com/article/releases/align-technology-announces-second-quarter-2020-financial-results1-millionth-invisalign-patient-milestone-in-apac-tokyo-japan/ (accessed on 28 February 2021).
- Koretsi, V.; Tingelhoff, L.; Proff, P.; Kirschneck, C. Intra-observer reliability and agreement of manual and digital orthodontic model analysis. Eur. J. Orthod. 2018, 40, 52–57. [Google Scholar] [CrossRef]
- Koretsi, V.; Kirschbauer, C.; Proff, P.; Kirschneck, C. Reliability and intra-examiner agreement of orthodontic model analysis with a digital caliper on plaster and printed dental models. Clin. Oral Investig. 2019, 23, 3387–3396. [Google Scholar] [CrossRef]
- Bolton, W.A. The clinical application of a tooth-size analysis. Am. J. Orthod. 1962, 48, 504–529. [Google Scholar] [CrossRef]
- Reuschl, R.P.; Heuer, W.; Stiesch, M.; Wenzel, D.; Dittmer, M.P. Reliability and validity of measurements on digital study models and plaster models. Eur. J. Orthod. 2016, 38, 22–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naidu, D.; Freer, T.J. Validity, reliability, and reproducibility of the iOC intraoral scanner: A comparison of tooth widths and Bolton ratios. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Quimby, M.L.; Vig, K.W.L.; Rashid, R.G.; Firestone, A.R. The accuracy and reliability of measurements made on computer-based digital models. Angle Orthod. 2004, 74, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Soto-Álvarez, C.; Fonseca, G.M.; Viciano, J.; Alemán, I.; Rojas-Torres, J.; Zúñiga, M.H.; López-Lázaro, S. Reliability, reproducibility and validity of the conventional buccolingual and mesiodistal measurements on 3D dental digital models obtained from intra-oral 3D scanner. Arch. Oral Biol. 2020, 109. [Google Scholar] [CrossRef]
- Sousa, M.V.S.; Vasconcelos, E.C.; Janson, G.; Garib, D.; Pinzan, A. Accuracy and reproducibility of 3-dimensional digital model measurements. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 269–273. [Google Scholar] [CrossRef]
- Grünheid, T.; Patel, N.; De Felippe, N.L.; Wey, A.; Gaillard, P.R.; Larson, B.E. Accuracy, reproducibility, and time efficiency of dental measurements using different technologies. Am. J. Orthod. Dentofac. Orthop. 2014, 145, 157–164. [Google Scholar] [CrossRef]
- Camardella, L.T.; Ongkosuwito, E.M.; Penning, E.W.; Kuijpers-Jagtman, A.M.; Vilella, O.V.; Breuning, K.H. Accuracy and reliability of measurements performed using two different software programs on digital models generated using laser and computed tomography plaster model scanners. Korean J. Orthod. 2020, 50, 13–25. [Google Scholar] [CrossRef]
- Roberts, C.T.; Richmond, S. The design and analysis of reliability studies for the use of epidemiological and audit indices in orthodontics. Br. J. Orthod. 1997, 24, 139–147. [Google Scholar] [CrossRef]
- Santoro, M.; Galkin, S.; Teredesai, M.; Nicolay, O.F.; Cangialosi, T.J. Comparison of measurements made on digital and plaster models. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 101–105. [Google Scholar] [CrossRef]
- Uysal, T.; Sari, Z. Intermaxillary tooth size discrepancy and mesiodistal crown dimensions for a Turkish population. Am. J. Orthod. Dentofac. Orthop. 2005, 128, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Yuen, K.K.W.; So, L.L.Y.; Tang, E.L.K. Mesiodistal crown diameters of the primary and permanent teeth in southern Chinese—A longitudinal study. Eur. J. Orthod. 1997, 19, 721–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajshekar, M.; Julian, R.; Williams, A.M.; Tennant, M.; Forrest, A.; Walsh, L.J.; Wilson, G.; Blizzard, L. The reliability and validity of measurements of human dental casts made by an intra-oral 3D scanner, with conventional hand-held digital callipers as the comparison measure. Forensic Sci. Int. 2017, 278, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Bootvong, K.; Liu, Z.; McGrath, C.; Hägg, U.; Wong, R.W.K.; Bendeus, M.; Yeung, S. Virtual model analysis as an alternative approach to plaster model analysis: Reliability and validity. Eur. J. Orthod. 2010, 32, 589–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watanabe-Kanno, G.A.; Abrão, J.; Miasiro, H.M.; Sánchez-Ayala, A.; Lagravère, M.O. Reproducibility, reliability and validity of measurements obtained from Cecile3 digital models. Braz. Oral Res. 2009, 23, 288–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goonewardene, R.W.; Goonewardene, M.S.; Razza, J.M.; Murray, K. Accuracy and validity of space analysis and irregularity index measurements using digital models. Aust. Orthod. J. 2008, 24, 83–90. [Google Scholar]
- Asquith, J.; Gillgrass, T.; Mossey, P. Three-dimensional imaging of orthodontic models: A pilot study. Eur. J. Orthod. 2007, 29, 517–522. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Intra-Examiner Reliability | Inter-Examiner Reliability | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tooth (FDI) | Δ (SD) | 95% CI | p | Dahlberg Error (mm) | CV (%) | ICC | Δ (SD) | 95% CI | p | Dahlberg Error (mm) | CV (%) | ICC |
| 1.1 | −0.03 (−0.09) | −0.09/0.04 | 0.336 | 0.06 | 0.76 | 0.98 | −0.01 (0.14) | −0.12/0.09 | 0.798 | 0.1 | 1.13 | 0.96 |
| 1.2 | 0.01 (−0.14) | −0.09/0.10 | 0.912 | 0.09 | 1.4 | 0.98 | 0.11 (0.25) | −0.08/0.29 | 0.211 | 0.18 | 2.75 | 0.92 |
| 1.3 | 0.06 (0.14) | −0.04/0.16 | 0.218 | 0.1 | 1.35 | 0.93 | 0.07 (0.24) | −0.1/0.24 | 0.39 | 0.17 | 2.22 | 0.80 |
| 1.4 | 0.01 (0.12) | −0.07/0.09 | 0.811 | 0.08 | 1.11 | 0.96 | 0.01 (0.12) | −0.08/0.09 | 0.894 | 0.08 | 1.1 | 0.96 |
| 1.5 | −0.03 (0.14) | −0.13/0.07 | 0.553 | 0.1 | 1.46 | 0.97 | −0.04 (0.15) | 0.15/0.07 | 0.422 | 0.1 | 1.55 | 0.97 |
| 1.6 | 0.11 (0.19) | −0.03/0.24 | 0.103 | 0.14 | 1.39 | 0.93 | 0.24 (0.3) | 0.03/0.45 | 0.031 * | 0.26 | 2.5 | 0.83 |
| 2.1 | −0.04 (0.13) | −0.13/0.05 | 0.385 | 0.09 | 1.06 | 0.97 | −0.07 (0.22) | −0.23/0.09 | 0.343 | 0.16 | 1.83 | 0.94 |
| 2.2 | 0.01 (0.13) | −0.08/0.10 | 0.776 | 0.09 | 1.3 | 0.97 | 0.07 (0.28) | −0.13/0.27 | 0.455 | 0.19 | 2.89 | 0.88 |
| 2.3 | −0.03 (0.13) | −0.12/0.06 | 0.449 | 0.09 | 1.15 | 0.95 | 0.02 (0.22) | −0.14/0.18 | 0.777 | 0.15 | 1.9 | 0.83 |
| 2.4 | 0.02 (0.12) | −0.07/0.10 | 0.667 | 0.08 | 1.16 | 0.97 | −0.01 (0.21) | −0.15/0.14 | 0.917 | 0.14 | 1.95 | 0.91 |
| 2.5 | −0.03 (0.14) | −0.13/0.07 | 0.491 | 0.1 | 1.44 | 0.98 | −0.04 (0.21) | −0.19/0.01 | 0.52 | 0.14 | 2.12 | 0.94 |
| 2.6 | 0.04 (0.14) | −0.06/0.14 | 0.374 | 0.1 | 0.97 | 0.96 | 0.04 (0.26) | −0.15/0.23 | 0.667 | 0.18 | 1.73 | 0.88 |
| 3.1 | −0.03 (0.14) | −0.12/0.07 | 0.547 | 0.09 | 1.75 | 0.93 | −0.03 (0.15) | −0.14/0.08 | 0.527 | 0.1 | 1.92 | 0.91 |
| 3.2 | 0.02 (0.11) | −0.06/0.10 | 0.556 | 0.07 | 1.27 | 0.96 | −0.02 (0.14) | −0.12/0.09 | 0.73 | 0.1 | 1.64 | 0.94 |
| 3.3 | −0.06 (0.11) | −0.14/0.02 | 0.103 | 0.09 | 1.29 | 0.96 | −0.06 (0.14) | −0.15/0.02 | 0.118 | 0.09 | 1.34 | 0.96 |
| 3.4 | −0.05 (0.14) | −0.15/0.05 | 0.289 | 0.1 | 1.4 | 0.91 | −0.05 (0.14) | −0.15/0.05 | 0.268 | 0.1 | 1.4 | 0.91 |
| 3.5 | 0.06 (0.13) | −0.03/0.15 | 0.188 | 0.1 | 1.35 | 0.98 | −0.04 (0.45) | −0.36/0.28 | 0.788 | 0.3 | 4.17 | 0.80 |
| 3.6 | 0.11 (0.20) | −0.03/0.25 | 0.121 | 0.16 | 1.42 | 0.95 | 0.15 (0.25) | −0.04/0.32 | 0.095 | 0.19 | 1.78 | 0.92 |
| 4.1 | 0.01 (0.09) | −0.05/0.07 | 0.755 | 0.06 | 1.14 | 0.95 | 0.02 (0.11) | −0.06/0.09 | 0.635 | 0.07 | 1.42 | 0.92 |
| 4.2 | 0.04 (0.14) | −0.06/0.14 | 0.384 | 0.1 | 1.71 | 0.94 | 0.03 (0.21) | −0.12/0.18 | 0.692 | 0.14 | 2.43 | 0.89 |
| 4.3 | −0.02 (0.13) | −0.11/0.08 | 0.702 | 0.09 | 1.29 | 0.95 | −0.04 (0.26) | −0.23/0.15 | 0.661 | 0.18 | 2.63 | 0.82 |
| 4.4 | 0.04 (0.13) | −0.05/0.14 | 0.353 | 0.09 | 1.32 | 0.96 | 0.05 (0.17) | −0.07/0.18 | 0.354 | 0.12 | 1.71 | 0.93 |
| 4.5 | 0 (0.16) | −0.12/0.11 | 0.938 | 0.11 | 1.48 | 0.96 | −0.06 (0.22) | −0.21/0.10 | 0.432 | 0.15 | 2.07 | 0.93 |
| 4.6 | 0.06 (0.10) | −0.01/0.13 | 0.095 | 0.08 | 0.72 | 0.98 | 0.11 (0.15) | 0.01/0.21 | 0.040 * | 0.12 | 1.13 | 0.96 |
| Total | 0.01 (0.14) | −0.01/0.03 | 0.199 | 0.1 | 1.28 | 0.99 | 0.01 (0.21) | 0.13 0.08 | 0.110 | 0.15 | 1.97 | 0.99 |
| Tooth (FDI) | Δ (SD) | 95% CI | p | Dahlberg Error (mm) | CV (%) | ICC |
|---|---|---|---|---|---|---|
| 1.1 | 0.00 (0.11) | −0.01/0.02 | 0.767 | 0.08 | 0.86 | 0.98 |
| 1.2 | 0.00 (0.09) | −0.01/0.02 | 0.642 | 0.07 | 0.97 | 0.98 |
| 1.3 | −0.01 (0.11) | −0.02/0.01 | 0.335 | 0.08 | 0.99 | 0.97 |
| 1.4 | 0.01 (0.12) | −0.01/0.03 | 0.280 | 0.09 | 1.20 | 0.96 |
| 1.5 | 0.01 (0.11) | −0.01/0.02 | 0.280 | 0.08 | 1.17 | 0.96 |
| 1.6 | 0.04 (0.22) | 0.01/0.07 | 0.019 * | 0.16 | 1.46 | 0.93 |
| 2.1 | 0.00 (0.10) | −0.02/0.01 | 0.719 | 0.07 | 0.82 | 0.99 |
| 2.2 | 0.01 (0.12) | −0.01/0.02 | 0.491 | 0.08 | 1.20 | 0.97 |
| 2.3 | 0.01 (0.14) | −0.01/0.03 | 0.459 | 0.10 | 1.26 | 0.95 |
| 2.4 | −0.01 (0.12) | −0.02/0.01 | 0.502 | 0.08 | 1.15 | 0.97 |
| 2.5 | 0.01 (0.13) | 0.00/0.03 | 0.099 | 0.09 | 1.29 | 0.95 |
| 2.6 | 0.02 (0.21) | −0.01/0.05 | 0.211 | 0.15 | 1.39 | 0.93 |
| 3.1 | −0.02 (0.23) | −0.05/0.01 | 0.208 | 0.16 | 3.10 | 0.83 |
| 3.2 | −0.01 (0.12) | −0.03/0.01 | 0.255 | 0.08 | 1.39 | 0.96 |
| 3.3 | −0.02 (0.13) | −0.03/0.00 | 0.098 | 0.09 | 1.35 | 0.96 |
| 3.4 | 0.00 (0.10) | −0.01/0.01 | 0.984 | 0.07 | 1.03 | 0.97 |
| 3.5 | 0.03 (0.23) | 0.09/0.06 | 0.061 | 0.16 | 2.24 | 0.86 |
| 3.6 | −0.01 (0.15) | −0.03/0.01 | 0.540 | 0.11 | 0.95 | 0.97 |
| 4.1 | −0.01 (0.08) | −0.02/0.01 | 0.277 | 0.06 | 1.08 | 0.97 |
| 4.2 | −0.01 (0.09) | −0.02/0.00 | 0.206 | 0.07 | 1.11 | 0.97 |
| 4.3 | −0.01 (0.14) | −0.03/0.01 | 0.239 | 0.10 | 1.42 | 0.96 |
| 4.4 | 0.00 (0.10) | −0.02/0.01 | 0.751 | 0.07 | 1.01 | 0.97 |
| 4.5 | 0.01 (0.11) | −0.01/0.02 | 0.519 | 0.08 | 1.10 | 0.96 |
| 4.6 | −0.01 (0.15) | −0.03/0.01 | 0.557 | 0.11 | 0.94 | 0.97 |
| Total | 0.002 (0.14) | −0.002/0.006 | 0.400 | 0.10 | 1.31 | 0.99 |
| Overall Bolton | −0.09 (0.74) | −0.19/0.01 | 0.084 | 0.53 | -- | 0.91 |
| Anterior Bolton | −0.05 (0.48) | −0.11/0.02 | 0.173 | 0.34 | -- | 0.93 |
| Translation (BL) | Rotation (MD) | Angulation (MD) | |||||
|---|---|---|---|---|---|---|---|
| Tooth (FDI) | ICC (95% CI) | p | ICC (95% CI) | p | ICC (95% CI) | p | r2 |
| 1.3 | 0.004 (−0.011/0.019) | 0.59 | 0.002 (0.000/0.003) | 0.039 * | 0.002 (−0.003/0.007) | 0.374 | 4.50% |
| 1.4 | 0.001 (−0.018/0.020) | 0.936 | 0.005 (0.001/0.008) | 0.007 ** | −0.001 (−0.006/0.004) | 0.663 | 4.00% |
| 1.5 | 0.011 (−0.001/0.023) | 0.078 | 0.003 (0.000/0.005) | 0.030 * | −0.002 (−0.006/0.002) | 0.312 | 5.60% |
| 1.6 | −0.026 (−0.066/0.014) | 0.204 | 0.011 (0.006/0.016) | <0.001 *** | −0.003 (−0.014/0.009) | 0.674 | 8.40% |
| 2.1 | 0.001 (−0.008/0.010) | 0.809 | 0.000 (−0.001/0.002) | 0.642 | 0.008 (0.003/0.013) | <0.001 *** | 6.10% |
| 2.3 | 0.035 (0.016/0.053) | <0.001 *** | −0.001 (−0.003/0.001) | 0.393 | 0.009 (0.003/0.015) | 0.005 ** | 13.00% |
| 3.4 | 0.017 (0.001/0.033) | 0.043 * | −0.001 (−0.003/0.001) | 0.164 | 0.002 (−0.002/0.005) | 0.357 | 2.70% |
| 3.5 | 0.056 (0.017/0.096) | 0.006 ** | 0.002 (−0.002/0.006) | 0.359 | 0.006 (−0.005/0.017) | 0.254 | 6.90% |
| 4.5 | −0.004 (−0.021/0.012) | 0.618 | 0.001 (−0.001/0.003) | 0.509 | 0.004 (0.000/0.009) | 0.047 * | 2.40% |
| 4.6 | −0.021 (−0.050/0.008) | 0.162 | 0.009 (0.003/0.015) | 0.005 ** | 0.006 (−0.001/0.014) | 0.109 | 5.30% |
| Agreement between Methods | ||||||
|---|---|---|---|---|---|---|
| Tooth (FDI) | Δ (SD) | 95% CI | p | Dahlberg Error (mm) | CV (%) | ICC |
| 1.1 | −0.18 (0.28) | −0.25/−0.10 | <0.001 *** | 0.24 | 2.74 | 0.86 |
| 1.2 | −0.16 (0.23) | −0.22/−0.10 | <0.001 *** | 0.20 | 2.91 | 0.90 |
| 1.3 | −0.16 (0.20) | −0.22/−0.11 | <0.001 *** | 0.18 | 2.31 | 0.85 |
| 1.4 | −0.14 (0.19) | −0.19/−0.09 | <0.001 *** | 0.17 | 2.33 | 0.89 |
| 1.5 | −0.18 (0.20) | −0.24/−0.13 | <0.001 *** | 0.19 | 2.74 | 0.89 |
| 1.6 | −0.65 (0.39) | 0.75/−0.54 | <0.001 *** | 0.53 | 4.97 | 0.24 |
| 2.1 | −0.16 (0.17) | −0.21/−0.11 | <0.001 *** | 0.17 | 1.91 | 0.92 |
| 2.2 | −0.18 (0.22) | −0.24/−0.10 | <0.001 *** | 0.20 | 2.97 | 0.88 |
| 2.3 | −0.14 (0.24) | −0.20/−0.07 | <0.001 *** | 0.20 | 2.52 | 0.80 |
| 2.4 | −0.11 (0.30) | −0.19/−0.03 | 0.011 * | 0.22 | 3.10 | 0.80 |
| 2.5 | −0.18 (0.18) | 0.23/−0.13 | <0.001 *** | 0.18 | 2.63 | 0.85 |
| 2.6 | −0.60 (0.30) | −0.69/−0.52 | <0.001 *** | 0.48 | 4.46 | 0.37 |
| 3.1 | −0.02 (0.25) | −0.09/0.05 | 0.570 | 0.18 | 3.29 | 0.76 |
| 3.2 | −0.14 (0.20) | −0.19/−0.09 | <0.001 *** | 0.17 | 2.88 | 0.82 |
| 3.3 | −0.16 (0.29) | −0.24/−0.08 | <0.001 *** | 0.23 | 3.22 | 0.75 |
| 3.4 | −0.11 (0.22) | −0.17/−0.05 | 0.001 ** | 0.17 | 2.39 | 0.84 |
| 3.5 | −0.18 (0.29) | 0.26/0.10 | <0.001 *** | 0.24 | 3.26 | 0.78 |
| 3.6 | −0.31 (0.26) | −0.38/−0.24 | <0.001 *** | 0.29 | 2.58 | 0.82 |
| 4.1 | −0.09 (0.15) | −0.13/−0.05 | <0.001 *** | 0.12 | 2.24 | 0.87 |
| 4.2 | −0.09 (0.25) | −0.16/0.02 | 0.001 ** | 0.18 | 3.09 | 0.78 |
| 4.3 | −0.14 (0.25) | −0.21/−0.07 | <0.001 *** | 0.20 | 2.97 | 0.79 |
| 4.4 | −0.11 (0.21) | −0.16/−0.05 | <0.001 *** | 0.17 | 2.33 | 0.85 |
| 4.5 | −0.14 (0.27) | −0.21/−0.06 | <0.001 *** | 0.21 | 2.86 | 0.82 |
| 4.6 | −0.19 (0.27) | −0.26/−0.12 | <0.001 *** | 0.23 | 2.08 | 0.87 |
| Total | −0.19 (0.28) | −0.20/−0.17 | <0.001 *** | 0.24 | 3.15 | 0.98 |
| Overall Bolton | 0.95 (1.93) | 0.53/1.37 | <0.001 *** | 1.26 | -- | 0.59 |
| Anterior Bolton | 0.29 (0.86) | 0.05/0.52 | 0.018 * | 0.64 | -- | 0.93 |
| Clin-Check Pro 6.0 Software/Original Bolton Formula | r2 | Slope [CI 95%] | Constant [CI 95%] |
|---|---|---|---|
| Overall Bolton | 0.99 | 1.070 [1.065, 1.075] | −0.053 [−0.063, −0.043] |
| Anterior Bolton | 0.99 | 1.163 [1.150, 1.176] | −0.125 [−0.140, −0.111] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adobes Martin, M.; Lipani, E.; Bernes Martinez, L.; Alvarado Lorenzo, A.; Aiuto, R.; Garcovich, D. Reliability of Tooth Width Measurements Delivered by the Clin-Check Pro 6.0 Software on Digital Casts: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 3581. https://doi.org/10.3390/ijerph19063581
Adobes Martin M, Lipani E, Bernes Martinez L, Alvarado Lorenzo A, Aiuto R, Garcovich D. Reliability of Tooth Width Measurements Delivered by the Clin-Check Pro 6.0 Software on Digital Casts: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(6):3581. https://doi.org/10.3390/ijerph19063581
Chicago/Turabian StyleAdobes Martin, Milagros, Erica Lipani, Laura Bernes Martinez, Alfonso Alvarado Lorenzo, Riccardo Aiuto, and Daniele Garcovich. 2022. "Reliability of Tooth Width Measurements Delivered by the Clin-Check Pro 6.0 Software on Digital Casts: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 6: 3581. https://doi.org/10.3390/ijerph19063581
APA StyleAdobes Martin, M., Lipani, E., Bernes Martinez, L., Alvarado Lorenzo, A., Aiuto, R., & Garcovich, D. (2022). Reliability of Tooth Width Measurements Delivered by the Clin-Check Pro 6.0 Software on Digital Casts: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 19(6), 3581. https://doi.org/10.3390/ijerph19063581