
Association between Depression Severity and Physical Function among Chinese Nursing Home Residents: The Mediating Role of Different Types of Leisure Activities


Abstract
:1. Introduction
2. Research Hypotheses
3. Materials and Methods
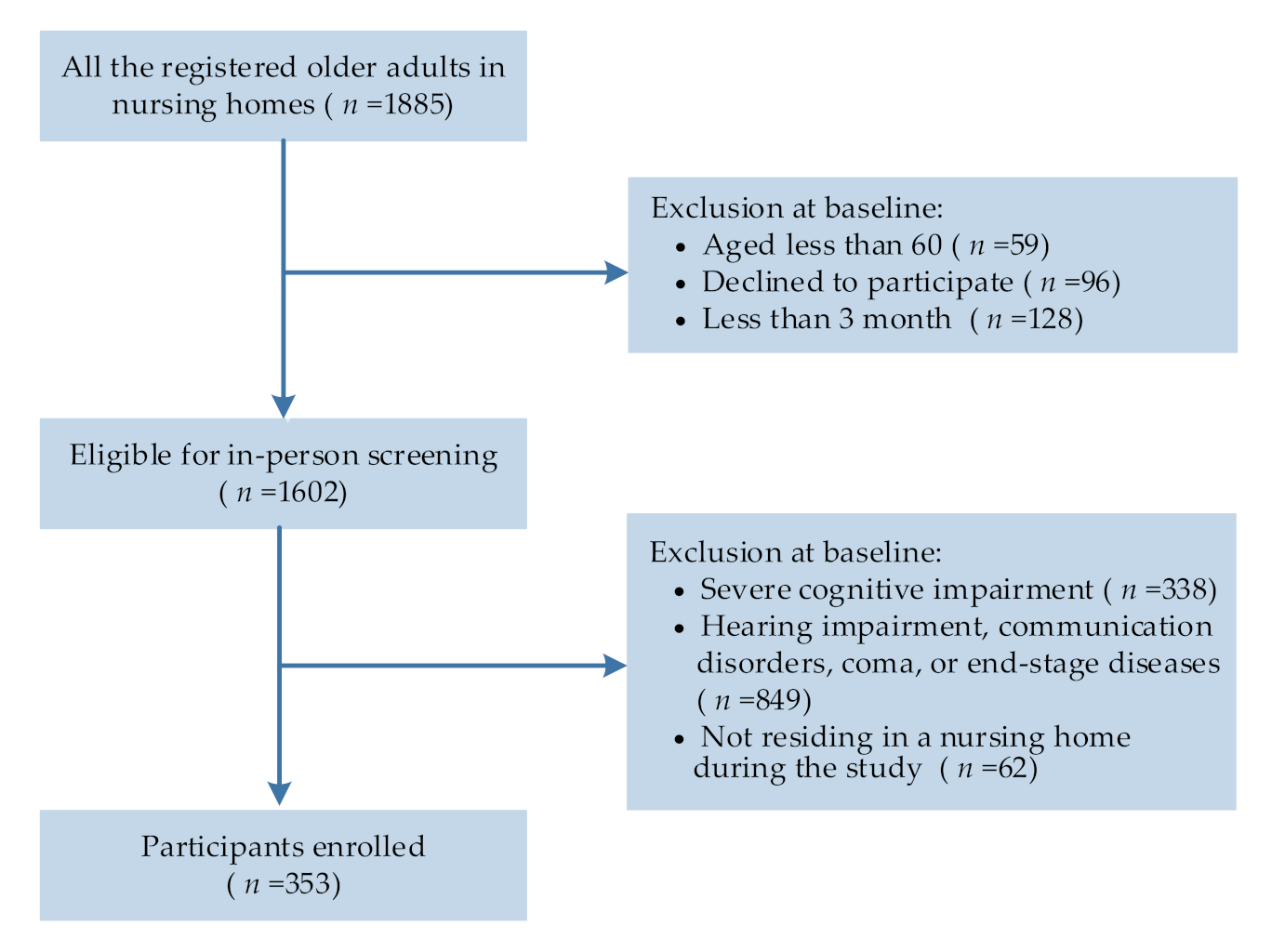
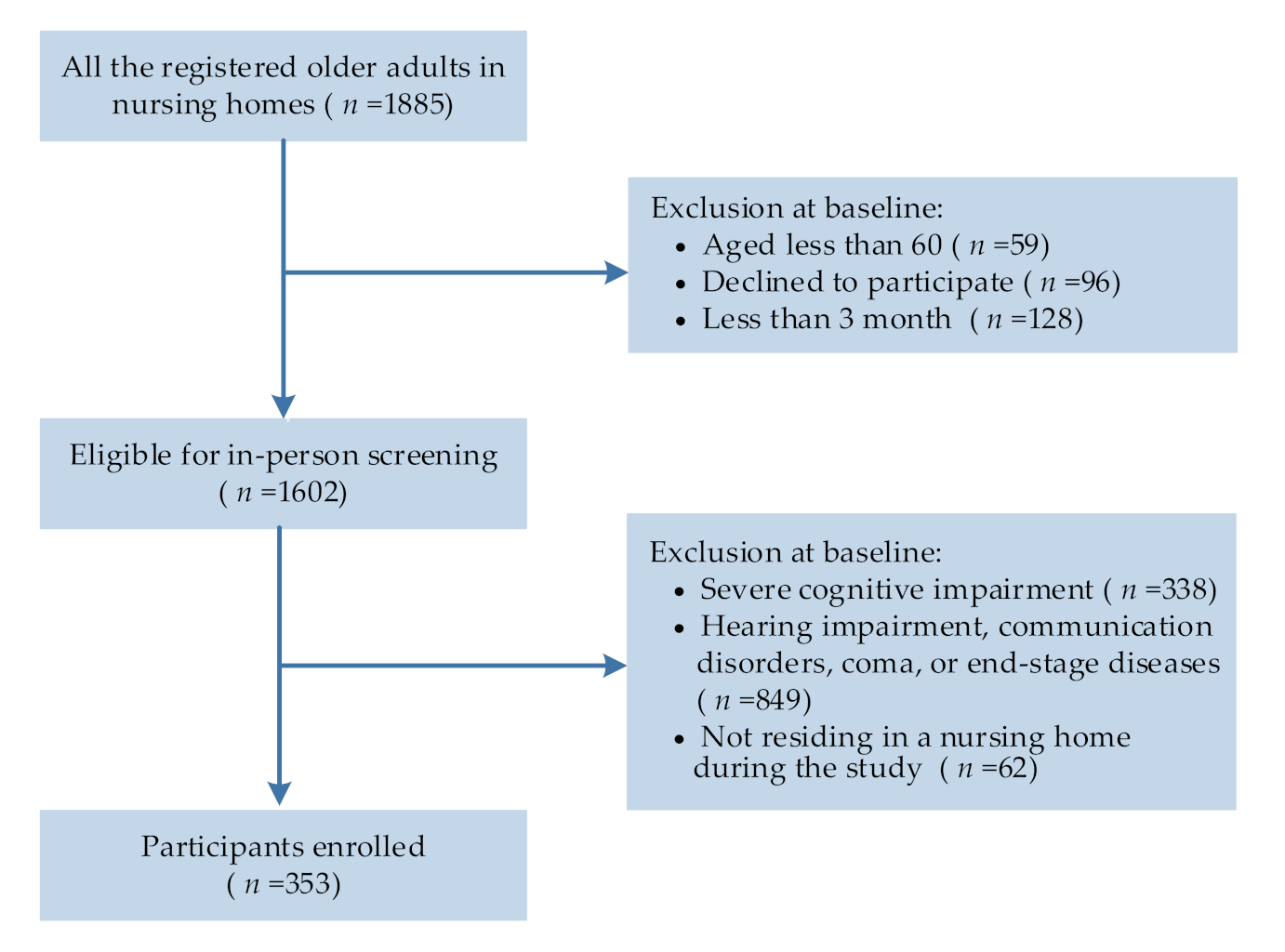
3.1. Participants
3.2. Measures
3.2.1. Exposures: Depression
3.2.2. Mediators: Active and Passive Leisure Activities
3.2.3. Outcome: Physical Function
3.3. Covariates
3.4. Data Analyses
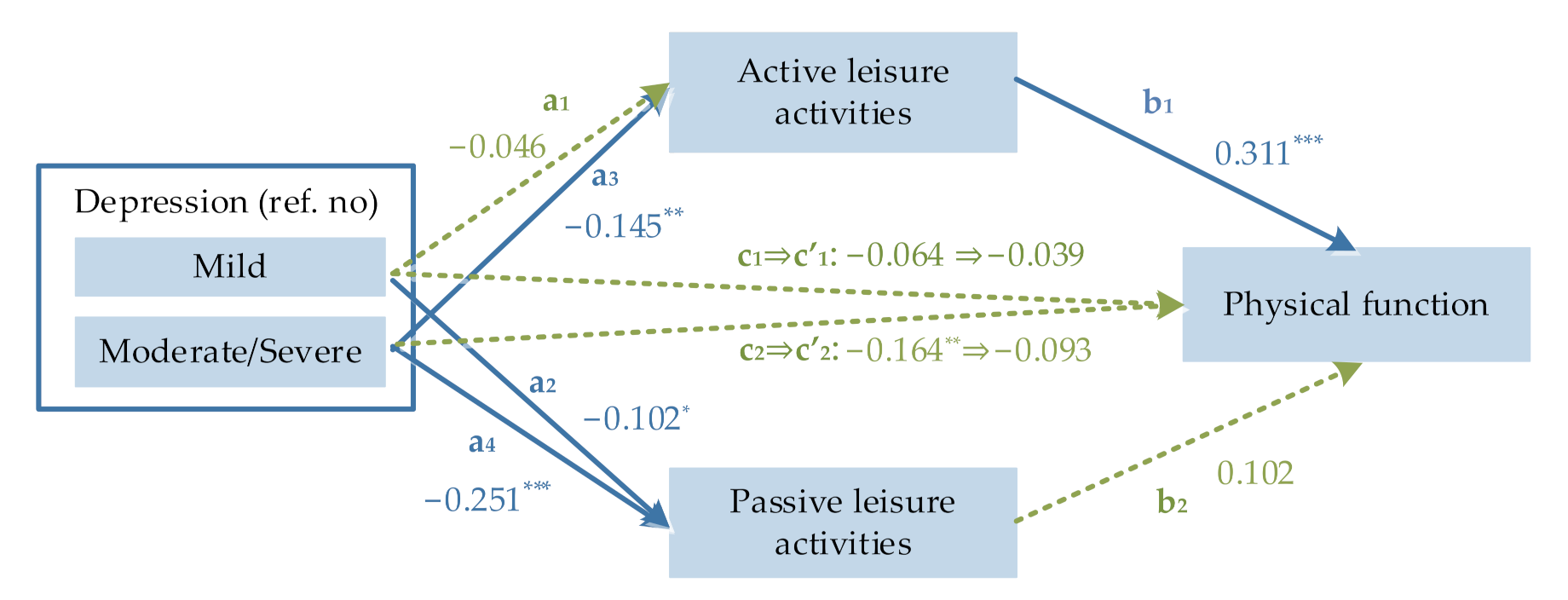
4. Results
5. Discussion
Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bulletin of the Seventh National Census (No. 7). Available online: http://www.stats.gov.cn/xxgk/sjfb/zxfb2020/202105/t20210511_1817195.html (accessed on 5 November 2021).
- Coelho-Junior, H.J.; Calvani, R.; Picca, A.; Gonçalves, I.O.; Landi, F.; Bernabei, R.; Cesari, M.; Uchida, M.C.; Marzetti, E. Association between dietary habits and physical function in brazilian and italian older women. Nutrients 2020, 12, 1635. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.M.; Ferrucci, L.; Pieper, C.F.; Leveille, S.G.; Markides, K.S.; Ostir, G.V.; Studenski, S.; Berkman, L.F.; Wallace, R.B. Lower extremity function and subsequent disability: Consistency across studies, predictive models, and value of gait speed alone compared with the short physical performance battery. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2000, 55, M221–M231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosano, C.; Simonsick, E.M.; Harris, T.B.; Kritchevsky, S.B.; Brach, J.; Visser, M.; Yaffe, K.; Newman, A.B. Association between physical and cognitive function in healthy elderly: The health, aging and body composition study. Neuroepidemiology 2005, 24, 8–14. [Google Scholar] [CrossRef] [PubMed]
- McDermott, M.M.; Liu, K.; Ferrucci, L.; Tian, L.; Guralnik, J.M.; Liao, Y.; Criqui, M.H. Decline in functional performance predicts later increased mobility loss and mortality in peripheral arterial disease. J. Am. Coll. Cardiol. 2011, 57, 962–970. [Google Scholar] [CrossRef] [Green Version]
- de Souto Barreto, P.; Lapeyre-Mestre, M.; Mathieu, C.; Piau, C.; Bouget, C.; Cayla, F.; Vellas, B.; Rolland, Y. A multicentric individually-tailored controlled trial of education and professional support to nursing home staff: Research protocol and baseline data of the IQUARE study. J. Nutr. Health Aging 2013, 17, 173–178. [Google Scholar] [CrossRef]
- Cronin-Stubbs, D.; de Leon, C.F.; Beckett, L.A.; Field, T.S.; Glynn, R.J.; Evans, D.A. Six-year effect of depressive symptoms on the course of physical disability in community-living older adults. Arch. Intern. Med. 2000, 160, 3074–3080. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, T.; French, S.D.; Belanger, E.; Guerra, R.O.; Zunzunegui, M.V.; Auais, M. Gender differences in trajectories of lower extremity function in older adults: Findings from the international mobility in aging study. J. Am. Med. Dir. Assoc. 2019, 20, 1199–1205.e4. [Google Scholar] [CrossRef]
- Gomes, C.D.S.; Cavalcanti Maciel, A.C.; Falcao Freire, A.D.N.; Moreira, M.D.A.; Ribeiro, M.D.O.; Guerra, R.O. Depressive symptoms and functional decline in an elderly sample of urban center in northeastern Brazil. Arch. Gerontol. Geriatr. 2014, 58, 214–218. [Google Scholar] [CrossRef]
- Iwasa, H.; Yoshida, Y.; Kumagai, S.; Ihara, K.; Yoshida, H.; Suzuki, T. Depression status as a reliable predictor of functional decline among Japanese community-dwelling older adults: A 12-year population-based prospective cohort study. Int. J. Geriatr. Psych. 2009, 24, 1192–1200. [Google Scholar] [CrossRef]
- Penninx, B.; Deeg, D.J.H.; van Eijk, J.T.M.; Beekman, A.T.F.; Guralnik, J.M. Changes in depression and physical decline in older adults: A longitudinal perspective. J. Affect. Disord. 2000, 61, 1–12. [Google Scholar] [CrossRef]
- Zhao, D.; Li, J.; Fu, P.; Hao, W.; Yuan, Y.; Yu, C.; Jing, Z.; Wang, Y.; Zhou, C. What role does activity engagement play in the association between cognitive frailty and falls among older adults? Evidence from rural Shandong, China. Gerontology 2020, 66, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Corcoran, M.P.; Chui, K.K.H.; White, D.K.; Reid, K.F.; Kirn, D.; Nelson, M.E.; Sacheck, J.M.; Folta, S.C.; Fielding, R.A. Accelerometer assessment of physical activity and its association with physical function in older adults residing at assisted care facilities. J. Nutr. Health Aging 2016, 20, 752–758. [Google Scholar] [CrossRef] [PubMed]
- Yatsugi, H.; Chen, T.; Chen, S.; Liu, X.; Kishimoto, H. The Associations between Objectively Measured Physical Activity and Physical Function in Community-Dwelling Older Japanese Men and Women. Int. J. Environ. Res. Public Health 2022, 19, 369. [Google Scholar] [CrossRef] [PubMed]
- Hillsdon, M.M.; Brunner, E.J.; Guralnik, J.M.; Marmot, M.G. Prospective study of physical activity and physical function in early old age. Am. J. Prev. Med. 2005, 28, 245–250. [Google Scholar] [CrossRef]
- Sun, R. Double jeopardy versus double benefit: The role of age and leisure activities in the incidence of disability among Chinese older adults. J. Aging Health 2021, 33, 350–361. [Google Scholar] [CrossRef]
- Garcia-Esquinas, E.; Andrade, E.; Martinez-Gomez, D.; Felix Caballero, F.; Lopez-Garcia, E.; Rodriguez-Artalejo, F. Television viewing time as a risk factor for frailty and functional limitations in older adults: Results from 2 European prospective cohorts. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 54. [Google Scholar] [CrossRef] [Green Version]
- Cho, D.; Post, J.; Kim, S.K. Comparison of passive and active leisure activities and life satisfaction with aging. Geriat. Gerontol. Int. 2018, 18, 380–386. [Google Scholar] [CrossRef]
- Kelly, J.R. Life after Work: Retirement, Leisure, Recreation, and the Elderly; Praeger Publishers: New York, NY, USA, 1982. [Google Scholar]
- Fancourt, D.; Aughterson, H.; Finn, S.; Walker, E.; Steptoe, A. How leisure activities affect health: A narrative review and multi-level theoretical framework of mechanisms of action. Lancet Psychiatry 2021, 8, 329–339. [Google Scholar] [CrossRef]
- Da Silva, M.A.; Singh-Manoux, A.; Brunner, E.J.; Kaffashian, S.; Shipley, M.J.; Kivimaki, M.; Nabi, H. Bidirectional association between physical activity and symptoms of anxiety and depression: The Whitehall II study. Eur. J. Epidemiol. 2012, 27, 537–546. [Google Scholar] [CrossRef] [Green Version]
- Roshanaei-Moghaddam, B.; Katon, W.J.; Russo, J. The longitudinal effects of depression on physical activity. General hospital. Psychiatry 2009, 31, 306–315. [Google Scholar] [CrossRef]
- Fancourt, D.; Steptoe, A. Comparison of physical and social risk-reducing factors for the development of disability in older adults: A population-based cohort study. J. Epidemiol. Community Health 2019, 73, 906–912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holtfreter, K.; Reisig, M.D.; Turanovic, J.J. Depression and infrequent participation in social activities among older adults: The moderating role of high-quality familial ties. Aging Ment. Health 2017, 21, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. ‘Mini-mental state’. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Gao, J.; Li, M.; Wang, K. Relationship between loneliness and frailty among older adults in nursing homes: The mediating role of activity engagement. J. Am. Med. Dir. Assoc. 2019, 20, 759–764. [Google Scholar] [CrossRef] [PubMed]
- Perera, S.; Mody, S.H.; Woodman, R.C.; Studenski, S.A. Meaningful change and responsiveness in common physical performance measures in older adults. J. Am. Geriatr. Soc. 2006, 54, 743–749. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Ferrucci, L.; Darer, J.; Williamson, J.D.; Anderson, G. Untangling the concepts of disability, frailty, and comorbidity: Implications for improved targeting and care. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2004, 59, 255–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef]
- Hooper, D.; Coughlan, J.; Mullen, M. Structural equation modelling: Guidelines for determining model fit. Electron. J. Bus Res. Methods 2008, 6, 53–60. [Google Scholar] [CrossRef]
- Chen, L. Leisure activities and psychological wellbeing reduce the risk of cognitive impairment among older adults with hearing difficulty: A longitudinal study in China. Maturitas 2021, 148, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, R.D. Association between physical activity and mental disorders among adults in the United States. Prev. Med. 2003, 36, 698–703. [Google Scholar] [CrossRef]
- Shin, K.; You, S. Leisure type, leisure satisfaction and adolescents’ psychological wellbeing. J. Pac. Rim. Psychol. 2013, 7, 53–62. [Google Scholar] [CrossRef] [Green Version]
- Angulo, J.; El Assar, M.; Álvarez-Bustos, A.; Rodríguez-Mañas, L. Physical activity and exercise: Strategies to manage frailty. Redox Biol. 2020, 35, 101513. [Google Scholar] [CrossRef] [PubMed]
- Qi, M.; Li, P.; Moyle, W.; Weeks, B.; Jones, C. Physical activity, health-related quality of life, and stress among the Chinese adult population during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6494. [Google Scholar] [CrossRef] [PubMed]
- Cordes, T.; Schoene, D.; Kemmler, W.; Wollesen, B. Chair-based exercise interventions for nursing home residents: A systematic review. J. Am. Med. Dir. Assoc. 2021, 22, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Santos-Lozano, A.; Garatachea, N. Accelerometers: A physical activity assessment tool. Riv. Fisiopatol. Dello Sport 2013, 66 (Suppl. 2), 497–511. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristic | All (n = 353) | Depression Severity | p for Difference | ||
|---|---|---|---|---|---|
| No | Mild | Moderate/Severe | |||
| (n = 212) | (n = 70) | (n = 71) | |||
| Mean (Standard Deviations) or n (%) | |||||
| Age | 79.01 (8.80) | 79.22 (9.24) | 79.60 (7.61) | 77.80 (8.56) | 0.415 |
| Sex | 0.184 | ||||
| Female | 197 (55.8) | 110 (51.9) | 44 (62.9) | 43 (60.6) | |
| Male | 156 (44.2) | 102 (48.1) | 26 (37.1) | 28 (39.4) | |
| Years of education | 5.26 (4.84) | 6.42 (4.95) | 6.73 (4.79) | 5.32 (4.50) | 0.166 |
| Having a spouse | 0.250 | ||||
| Yes | 63 (17.8) | 180 (84.9) | 55 (78.6) | 55 (77.5) | |
| No | 290 (82.2) | 32 (15.1) | 15 (21.4) | 16 (22.5) | |
| Economic condition | 0.475 | ||||
| Good | 131 (37.1) | 128 (60.4) | 46 (65.7) | 48 (67.6) | |
| Poor | 222 (62.9) | 84 (39.6) | 24 (34.3) | 23 (32.4) | |
| Comorbidity | 0.152 | ||||
| Yes | 265 (75.1) | 152 (71.7) | 58 (82.9) | 55 (77.5) | |
| No | 88 (24.9) | 60 (28.3) | 12 (17.1) | 16 (22.5) | |
| Body mass index | 0.023 | ||||
| Underweight | 20 (32.0) | 8 (3.7) | 6 (8.6) | 6 (8.4) | |
| Normal | 113 (5.7) | 71 (33.5) | 18 (25.7) | 24 (33.8) | |
| Overweight | 120 (34.0) | 68 (32.1) | 21 (30.0) | 31 (43.7) | |
| Obese | 100 (28.3) | 65 (30.7) | 25 (35.7) | 10 (14.1) | |
| Leisure activities | |||||
| Active | 6.71 (2.53) | 6.99 (2.43) | 6.69 (2.70) | 5.89 (2.48) | 0.006 |
| Passive | 13.61 (3.73) | 14.27 (3.72) | 13.37 (3.29) | 11.87 (3.65) | <0.001 |
| Physical function | 3.70 (3.52) | 4.11 (3.57) | 3.56 (3.57) | 2.61 (3.07) | 0.007 |
| Effect | Mild Depression a | Moderate/Severe Depression a | |||
|---|---|---|---|---|---|
| Coefficient | 95% CI | Coefficient | 95% CI | Effect Size | |
| Total indirect effect (c) | −0.025 | −0.063, 0.015 | −0.070 ** | −0.119, −0.027 | 43% |
| Specific indirect effect (a × b) | |||||
| Active leisure activities | −0.014 | −0.051, 0.018 | −0.045 * | −0.083, −0.013 | 27% |
| Passive leisure activities | −0.010 | −0.033, 0.001 | −0.025 | −0.062, 0.003 | 15% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, M.; Wang, Y.; Wang, S.; Yang, Y.; Li, M.; Wang, K. Association between Depression Severity and Physical Function among Chinese Nursing Home Residents: The Mediating Role of Different Types of Leisure Activities. Int. J. Environ. Res. Public Health 2022, 19, 3543. https://doi.org/10.3390/ijerph19063543
Zhao M, Wang Y, Wang S, Yang Y, Li M, Wang K. Association between Depression Severity and Physical Function among Chinese Nursing Home Residents: The Mediating Role of Different Types of Leisure Activities. International Journal of Environmental Research and Public Health. 2022; 19(6):3543. https://doi.org/10.3390/ijerph19063543
Chicago/Turabian StyleZhao, Meng, Yaqi Wang, Shan Wang, Yuan Yang, Ming Li, and Kefang Wang. 2022. "Association between Depression Severity and Physical Function among Chinese Nursing Home Residents: The Mediating Role of Different Types of Leisure Activities" International Journal of Environmental Research and Public Health 19, no. 6: 3543. https://doi.org/10.3390/ijerph19063543
APA StyleZhao, M., Wang, Y., Wang, S., Yang, Y., Li, M., & Wang, K. (2022). Association between Depression Severity and Physical Function among Chinese Nursing Home Residents: The Mediating Role of Different Types of Leisure Activities. International Journal of Environmental Research and Public Health, 19(6), 3543. https://doi.org/10.3390/ijerph19063543