
International Comparison of Social Support Policies on Long-Term Care in Workplaces in Aging Societies


Abstract
:1. Introduction
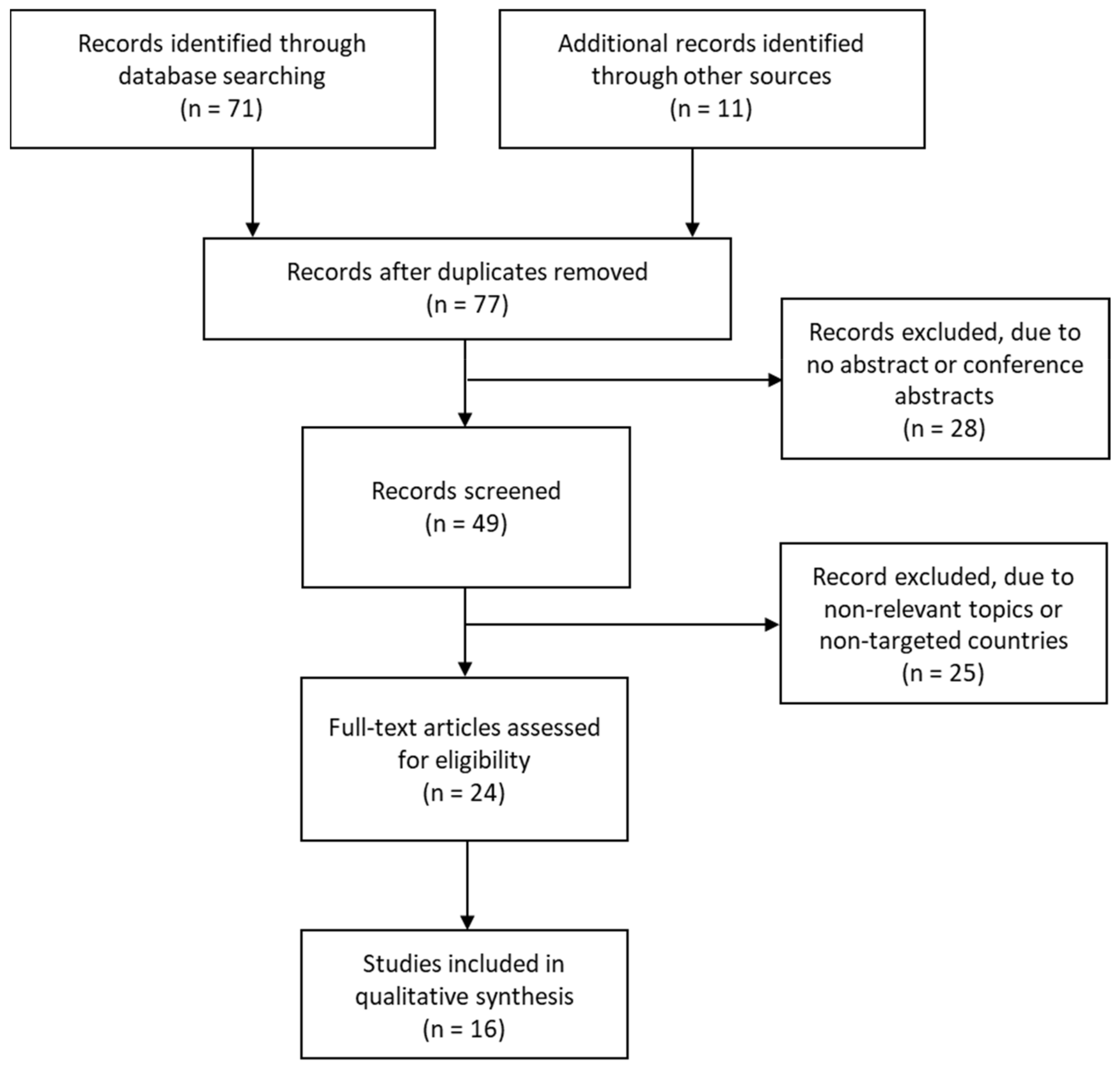
2. Materials and Methods
3. Results
3.1. Basic Information and Occupational Health Standards in Each Country
3.2. LTC Support Systems for Employees Who Take Care of Family Members and Relatives, by Country
3.2.1. Canada
3.2.2. France
3.2.3. Germany
3.2.4. Japan
3.2.5. Sweden
3.2.6. The UK
3.2.7. The USA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Organisation for Economic Co-Operation and Development (OECD) Statistics. Available online: https://stats.oecd.org/ (accessed on 9 December 2021).
- Spasova, S.; Baeten, R.; Coster, S.; Ghailani, D.; Peña-Casas, R.; Vanhercke, B. Challenges in Long-Term Care in Europe: A Study of National Policies, 2018; European Commission: Brussels, Belgium, 2018; Available online: https://ec.europa.eu/social/BlobServlet?docId=20225&langId=en (accessed on 6 December 2021).
- European Commission; Directorate-General for Employment; Social Affairs and Inclusion; Zigante, V. Informal Care in Europe: Exploring Formalisation, Availability and Quality; Publications Office of the European Union: Luxembourg, 2018; Available online: https://op.europa.eu/en/publication-detail/-/publication/96d27995-6dee-11e8-9483-01aa75ed71a1 (accessed on 9 December 2021).
- The Japan Institute for Labour Policy and Training (JIPAT). JIPAT Research Report No. 204: Combining Work and Care under the Re-Familization of Elderly Care in Japan; JIPAT: Tokyo, Japan, 2020; Available online: https://www.jil.go.jp/english/reports/jilpt_research/2020/no.204.html (accessed on 25 January 2022).
- European Commission. Executive Summary: Peer Review on ‘Work-Life Balance: Promoting Gender Equality in Informal Long-Term Care Provision; European Commission: Brussels, Germany, 2020; Available online: https://ec.europa.eu/social/BlobServlet?docId=23272&langId=en (accessed on 6 December 2021).
- Ministry of Health, Labour and Welfare (MHLW). Annual Health, Labour and Welfare Report—The Social Security System and People’s Work Styles in the Reiwa Era; MHLW: Tokyo, Japan, 2020; Available online: https://www.mhlw.go.jp/english/wp/wp-hw13/index.html (accessed on 25 January 2022).
- Vos, E.E.; de Bruin, S.R.; van der Beek, A.J.; Proper, K.I. “It’s Like Juggling, Constantly Trying to Keep All Balls in the Air": A Qualitative Study of the Support Needs of Working Caregivers Taking Care of Older Adults. Int. J. Environ. Res. Public Health 2021, 18, 5701. [Google Scholar] [CrossRef] [PubMed]
- Plöthner, M.; Schmidt, K.; de Jong, L.; Zeidler, J.; Damm, K. Needs and preferences of informal caregivers regarding outpatient care for the elderly: A systematic literature review. BMC Geriatr. 2019, 19, 82. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, F.; Rodrigues, R. Informal Carers: Who Takes Care of Them? Policy Brief 2010, 4, 1–16. [Google Scholar]
- Statistics Bureau of Japan. 2017 Employment Status Survey: Summary of the Results; Statistics Bureau of Japan: Tokyo, Japan, 2017; Available online: https://www.stat.go.jp/english/data/shugyou/pdf/sum2017.pdf (accessed on 30 November 2021).
- ICF. Peer Review on “Work-Life Balance: Promoting Gender Equality in Informal Long-Term Care Provision”; European Commission: Brussels, Belgium, 2020; Available online: https://ec.europa.eu/social/main.jsp?langId=en&catId=1024&furtherNews=yes&newsId=9841 (accessed on 6 December 2021).
- The Japan Institute for Labour Policy and Training (JIPAT). Survey on Family Care and Employment; JIPAT: Tokyo, Japan, 2020; Available online: https://www.jil.go.jp/institute/research/2020/documents/0200.pdf (accessed on 26 May 2020).
- Feinberg, L.F. Paid Family Leave: An Emerging Benefit for Employed Family Caregivers of Older Adults. J. Am. Geriatr. Soc. 2019, 67, 1336–1341. [Google Scholar] [CrossRef] [PubMed]
- Greenfield, J.C.; Hasche, L.; Bell, L.M.; Johnson, H. Exploring how workplace and social policies relate to caregivers’ financial strain. J. Gerontol. Soc. Work 2018, 61, 849–866. [Google Scholar] [CrossRef] [PubMed]
- Stall, N. We should care more about caregivers. Can. Med. Assoc. J. 2019, 191, E245–E246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. Department of Labor. Navigating the Demands of Work and Eldercare; U.S. Department of Labor: Washington, DC, USA, 2016. Available online: https://ecommons.cornell.edu/handle/1813/78429 (accessed on 25 January 2022).
- Schulz, R.; Beach, S.R.; Czaja, S.J.; Martire, L.M.; Monin, J.K. Family Caregiving for Older Adults. Annu. Rev. Psychol. 2020, 71, 635–659. [Google Scholar] [CrossRef] [PubMed]
- Cabinet Office. Annual Report on the Ageing Society 2021; Cabinet Office: Tokyo, Japan, 2021; Available online: https://www8.cao.go.jp/kourei/whitepaper/index-w.html (accessed on 19 January 2022).
- Meyer, K.; Rath, L.; Gassoumis, Z.; Kaiser, N.; Wilber, K. What Are Strategies to Advance Policies Supporting Family Caregivers? Promising Approaches From a Statewide Task Force. J. Aging Soc. Policy 2018, 31, 66–84. [Google Scholar] [CrossRef] [PubMed]
- Paraponaris, A.; Davin, B.; Verger, P. Formal and informal care for disabled elderly living in the community: An appraisal of French care composition and costs. Eur. J. Health Econ. 2011, 13, 327–336. [Google Scholar] [CrossRef] [PubMed]
- Detaille, S.I.; de Lange, A.; Engels, J.; Pijnappels, M.; Hutting, N.; Osagie, E.; Reig-Botella, A. Supporting Double Duty Caregiving and Good Employment Practices in Health Care Within an Aging Society. Front. Psychol. 2020, 11, 535353. [Google Scholar] [CrossRef] [PubMed]
- Longacre, M.L.; Valdmanis, V.G.; Handorf, E.A.; Fang, C.Y. Work Impact and Emotional Stress Among Informal Caregivers for Older Adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2016, 72, 522–531. [Google Scholar] [CrossRef] [PubMed]
- McCaffrey, N.; Gill, L.; Kaambwa, B.; Cameron, I.D.; Patterson, J.; Crotty, M.; Ratcliffe, J. Important features of home-based support services for older Australians and their informal carers. Health Soc. Care Community 2015, 23, 654–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eldh, A.C.; Carlsson, E. Seeking a balance between employment and the care of an ageing parent. Scand. J. Caring Sci. 2010, 25, 285–293. [Google Scholar] [CrossRef] [PubMed]
- McCann, S.; Evans, D. Informal care: The views of people receiving care. Health Soc. Care Community 2002, 10, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Plaisier, I.; van Groenou, M.B.; Keuzenkamp, S. Combining work and informal care: The importance of caring organisations. Hum. Resour. Manag. J. 2014, 25, 267–280. [Google Scholar] [CrossRef] [Green Version]
- Meyer, K.; Kaiser, N.; Benton, D.; Fitzpatrick, S.; Gassoumis, Z.; Wilber, K.; The California Task Force on Family Caregiving. Picking up the Pace of Change for California’s Family Caregivers: A Report from the California Task Force on Family Caregiving; USC Leonard Davis School of Gerontology: Los Angeles, CA, USA, 2018; Available online: http://tffc.usc.edu/2018/07/02/final-report-from-the-california-task-force-on-family-caregiving-2/ (accessed on 25 January 2022).
- Le Bihan, B. ESPN Thematic Report on Challenges in Long-Term Care: France; European Commission: Brussels, Belgium, 2018; Available online: https://ec.europa.eu/social/BlobServlet?docId=19847&langId=en (accessed on 6 December 2021).
- Henning-Smith, C.; Lahr, M. Rural-Urban Difference in Workplace Supports and Impacts for Employed Caregivers. J. Rural Health 2019, 35, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Van Groenou, M.I.B.; De Boer, A. Providing informal care in a changing society. Eur. J. Ageing 2016, 13, 271–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health, Labour and Welfare (MHLW). Overseas Situation Report 2019; MHLW: Tokyo, Japan, 2020. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Japan Institute for Labour Policy and Training (JIPAT). Databook of International Labour Statistics 2019; JIPAT: Tokyo, Japan, 2019; Available online: https://www.jil.go.jp/english/estatis/databook/2019/index.html (accessed on 20 May 2020).
- Employment and Social Development Canada. Hours of Work. Available online: https://www.canada.ca/en/employment-social-development/programs/employment-standards/work-hours.html (accessed on 24 January 2022).
- Ministry of Health, Labour and Welfare (MHLW). Overseas Situation Report 2018; MHLW: Tokyo, Japan, 2019. [Google Scholar]
- The Japan Institute for Labour Policy and Training (JIPAT). Childcare Leave Systems and Other Policies to Support Balancing Work and Childcare in Other Countries: Sweden, France, Germany, the United Kingdom, the United States, and South Korea; JIPAT: Tokyo, Japan, 2018; Available online: https://www.jil.go.jp/institute/siryo/2018/197.html (accessed on 28 May 2020).
- Ministry of Health, Labour and Welfare (MHLW). Overseas Situation Report 2020; MHLW: Tokyo, Japan, 2021. [Google Scholar]
- The Japan Institute for Labour Policy and Training (JIPAT). Childcare and Family Care Leave Systems in Europe; JIPAT: Tokyo, Japan, 2017; Available online: https://www.jil.go.jp/institute/siryo/2017/186.html (accessed on 28 May 2020).
- Social Protection Committee (SPC); European Commission (DG EMPL). 2021 Long-Term Care Report—Trends, Challenges and Opportunities in an Ageing Society: Country Profiles, Volume II; Publications Office of the European Union: Luxembourg, 2021. [Google Scholar] [CrossRef]
- Gerlinger, T. ESPN Thematic Report on Challenges in Long-Term Care: Germany; European Commission: Brussels, Belgium, 2018; Available online: https://ec.europa.eu/social/BlobServlet?docId=19848&langId=en (accessed on 6 December 2021).
- Schön, P.; Heap, J. ESPN Thematic Report on Challenges in Long-Term Care: Sweden; European Commission: Brussels, Belgium, 2018; Available online: https://ec.europa.eu/social/BlobServlet?docId=19870&langId=en (accessed on 27 November 2020).
- Ministry of Health, Labour and Welfare (MHLW). 2018 Edition Annual Health, Labour and Welfare Report -Achieve a Society in which Everyone Can Play an Active Role while Coping with Disabilities, Illnesses or Other Hardships; MHLW: Tokyo, Japan, 2018; Available online: https://www.mhlw.go.jp/english/wp/wp-hw12/dl/summary.pdf (accessed on 25 January 2022).
- Ministry of Health, Labour and Welfare (MHLW). General Survey on Working Conditions 2020; MHLW: Tokyo, Japan, 2021. [Google Scholar]
- Organisation for Economic Co-operation and Development (OECD). OECD Family Database; OECD: Paris, France, 2014. [Google Scholar]
- Cabinet Office. Opinion Poll on People’s Life; Cabinet Office: Tokyo, Japan, 2022. [Google Scholar]
- Statistical Bureau of Japan. 2017 Employment Status Survey; Statistical Bureau of Japan: Tokyo, Japan, 2017. [Google Scholar]
- Glendinning, C. ESPN Thematic Report on Challenges in Long-Term Care: United Kingdom; European Commission: Brussels, Belgium, 2018; Available online: https://ec.europa.eu/social/BlobServlet?docId=19873&langId=en (accessed on 6 December 2021).
- Tur-Sinai, A.; Teti, A.; Rommel, A.; Hlebec, V.; Yghemonos, S.; Lamura, G. Cross-national data on informal caregivers of older people with long-term care needs in the European population: Time for a more coordinated and comparable approach. J. Biosoc. Sci. 2022, 1–5. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Population (× 1,000,000) 1 | Working Age (15–64 Years Old) Population (%) 1 | Elderly (65+ Years Old) Population (%) 1 | Old Age Dependency Ratio 1 | Life Expectancy (LE) at Birth, Both Sex (Years) 2 | Healthy Life Expectancy (HALE) at Birth, Both Sex (Years) 3 | Difference between LE and HALE | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Year | 2020 | 2020 | Difference from 2005 | 2020 | Difference from 2005 | 2020 | 2040 | 2019 | 2019 | 2019 |
| Canada | 38.01 | 66.1 | Δ 3.2 | 18.0 | 5.5 | 0.274 | 0.384 | 82.2 | 71.3 | 10.9 |
| France | 67.35 | 61.6 | Δ 3.5 | 20.6 | 4.3 | 0.335 | 0.468 | 82.5 | 72.1 | 10.4 |
| Germany | 83.16 | 64.4 | Δ 2.4 | 21.9 | 3.0 | 0.340 | 0.477 | 81.7 | 70.9 | 10.8 |
| Japan | 125,71 | 59.3 | Δ 6.8 | 28.8 | 8.6 | 0.489 | 0.656 | 84.3 | 74.1 | 10.2 |
| Sweden | 10.35 | 62.2 | Δ 3.1 | 20.1 | 2.8 | 0.323 | 0.384 | 82.4 | 71.9 | 10.5 |
| UK | 67.08 | 63.5 | Δ 2.5 | 18.6 | 2.7 | 0.294 | 0.398 | 81.4 | 70.1 | 11.3 |
| USA | 329.48 | 64.8 | Δ 2.3 | 16.9 | 4.5 | 0.260 | 0.353 | 78.5 | 66.1 | 12.4 |
| Country [References] | Legal Working Hours and Average Hours Per Week Per Employed Person (2019–2020) | Overtime Work Hours, Wage, and % Employed Working 49 and More Hours Per Week (2019–2020) | Rest, Holidays and Special Leaves | Other Labor Standards |
|---|---|---|---|---|
| Canada [33,34,35] |
|
|
|
|
| France [33,35] |
|
|
|
|
| Germany [33,35] |
|
|
|
|
| Japan [33] |
|
|
|
|
| Sweden [31,36] |
|
|
|
|
| UK [33,35] |
|
|
|
|
| USA [33,35,37] |
|
|
|
|
| Country [References] | Law Related to LTC Leave and LTC Insurance System | LTC Leave and Allowance for Employees |
|---|---|---|
| Canada [15,35] |
|
|
| France [11,28,35] |
|
|
| Germany [8,11,35,39,40] |
|
|
| Japan [42] |
|
|
| Sweden [31,36,41] |
|
|
| UK [38] |
|
|
| USA [13,16,35] |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kanda, K.; Sakurazawa, H.; Yoshida, T. International Comparison of Social Support Policies on Long-Term Care in Workplaces in Aging Societies. Int. J. Environ. Res. Public Health 2022, 19, 3284. https://doi.org/10.3390/ijerph19063284
Kanda K, Sakurazawa H, Yoshida T. International Comparison of Social Support Policies on Long-Term Care in Workplaces in Aging Societies. International Journal of Environmental Research and Public Health. 2022; 19(6):3284. https://doi.org/10.3390/ijerph19063284
Chicago/Turabian StyleKanda, Koji, Hirofumi Sakurazawa, and Takahiko Yoshida. 2022. "International Comparison of Social Support Policies on Long-Term Care in Workplaces in Aging Societies" International Journal of Environmental Research and Public Health 19, no. 6: 3284. https://doi.org/10.3390/ijerph19063284
APA StyleKanda, K., Sakurazawa, H., & Yoshida, T. (2022). International Comparison of Social Support Policies on Long-Term Care in Workplaces in Aging Societies. International Journal of Environmental Research and Public Health, 19(6), 3284. https://doi.org/10.3390/ijerph19063284