
A Scoping Review of the Health Impact of the COVID-19 Pandemic on Persons Experiencing Homelessness in North America and Europe



Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Data Charting and Synthesis
3. Results
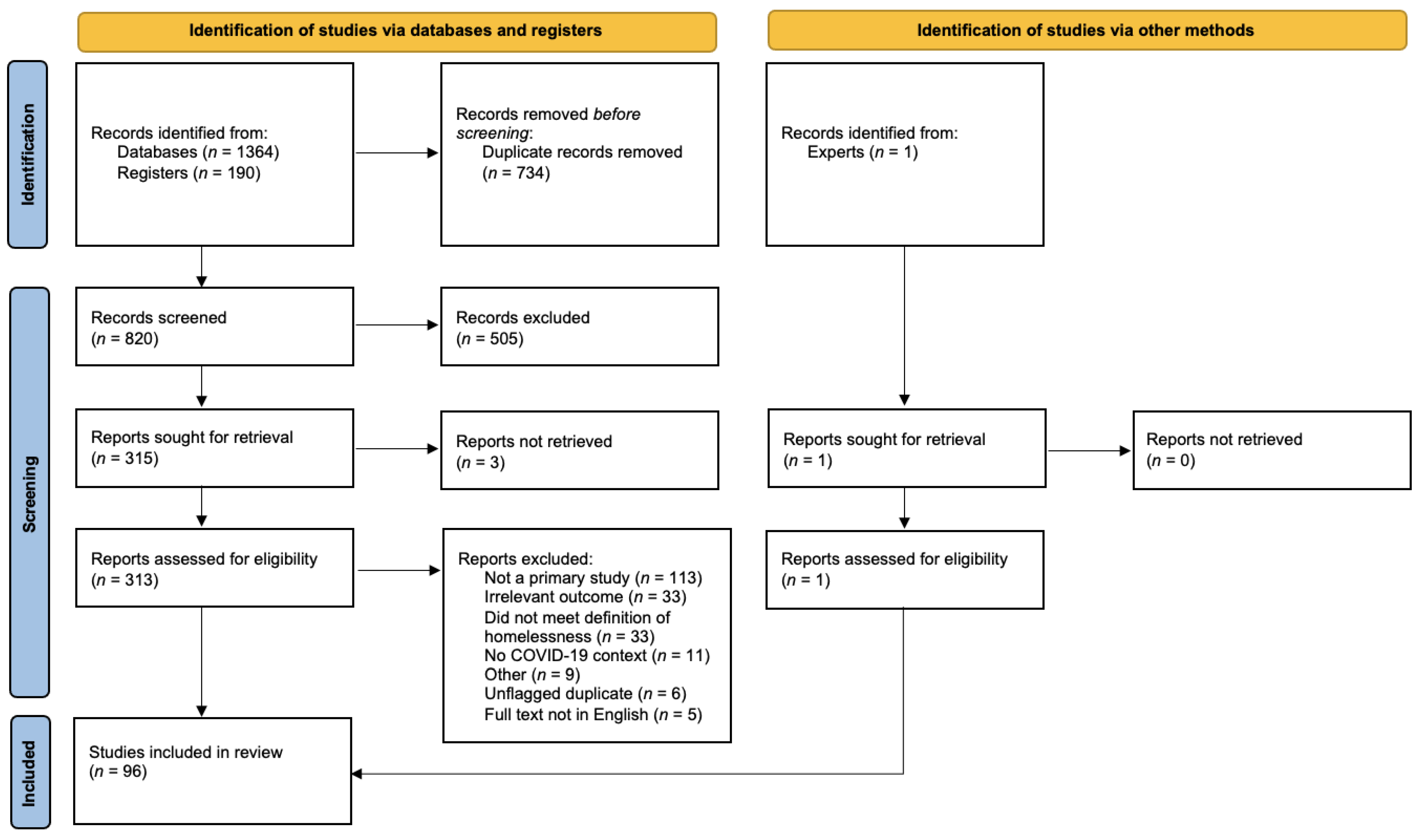
3.1. Screening Process
3.2. Overview of Included Studies
3.3. SARS-CoV-2 Infection and Morbidity
3.4. COVID-19-Related Hospitalisation
3.5. COVID-19-Related Mortality
3.6. Fear of COVID-19
3.7. COVID-19 Vaccine Acceptance
3.8. Housing
3.9. Access to Personal Hygiene and PPE
3.10. Access to Food
3.11. Substance Use
3.12. Mental Health
3.13. Access to Health Services
3.14. Other Health Impacts
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Detailed Search Strategy
| EMBASE |
| ‘coronavirus disease 2019’/exp OR ‘Severe acute respiratory syndrome coronavirus 2’/exp (‘2019 nCoV’ or 2019 nCoV or ‘2019-n ovel CoV’): ti,ab,kw (‘corona vir*’ or coronavir* or ‘neocorona vir*’ or neocoronavir*): ti,ab COVID: ti,ab,kw ‘COVID 19’: ti,ab (‘nCov 2019’ or ‘nCov 19’): ti,ab (‘SARS-CoV-2’ or ‘SARS-CoV2’ or SARSCoV2 or SARSCoV-2): ti,ab,kw (‘SARS coronavirus 2’ or ‘SARS-like coronavirus’ or ‘Severe Acute Respiratory Syndrome Coronavirus-2’): ti,ab,kw (‘2019 new coronavirus’ OR ‘2019 novel coronavirus’ OR ‘2019-ncov’ OR ‘hcov-19’ OR ‘human coronavirus 2019’ OR ‘sars coronavirus 2’ OR ‘SARS-CoV-2’ OR ‘sars2 (virus)’ OR ‘severe acute respiratory syndrome coronavirus 2’ OR ‘wuhan coronavirus’ OR ‘wuhan seafood market pneumonia virus’ OR ‘ncov-2019’ OR ‘novel 2019 coronavirus’ OR ‘novel coronavirus 2019’ OR ‘novel coronavirus-19’): ti,ab,kw #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 ‘homelessness’/exp OR ‘homeless person’/exp (homeless*): ti,ab (Rough NEAR/3 sleep*):ti,ab (‘Housing insecur*’): ti,ab #11 OR #12 OR #13 OR #14 #10 AND #15 |
| Medline |
| Coronavirus/ Coronavirus Infections/ COVID 19.rs. severe acute respiratory syndrome coronavirus 2.os. (2019 nCoV or 2019 nCoV or 2019 novel CoV). tw,kf. (corona vir* or coronavir* or neocorona vir* or neocoronavir*). tw,kf. COVID.mp. COVID 19. tw,kf. (nCov 2019 or nCov 19). tw,kf. (“SARS-CoV-2” or “SARS-CoV2” or SARSCoV2 or “SARSCoV-2”).mp. (“SARS coronavirus 2” or “SARS-like coronavirus” or “Severe Acute Respiratory Syndrome Coronavirus-2”).mp. or/1–11 exp Homeless Persons/ homeless*.mp (Rough adj3 sleep*).mp. (Housing insecur*).mp. or/13–16 12 AND 17 |
| CINAHL |
| (((MH “Coronavirus+”) or coronavirus* or covid) AND (wuhan or beijing or shanghai) OR (“novel coronavirus*” AND ((MH “China”) or China)) OR TI coronavirus * OR (((MH pneumonia) or pneumonia) AND Wuhan) OR ((D614 G or “COVID-19” or COVID-19 or “2019-nCoV” or “SARS-CoV-2” or (MH Coronavirus Infections))) AND ((MH “Coronavirus+”) or coronavirus* or COVID) AND (wuhan or beijing or shanghai) OR (“novel coronavirus*” AND ((MH “China”) or China)) OR TI coronavirus* OR (((MH pneumonia) or pneumonia) AND Wuhan) OR ((D614 G or “COVID-19” or COVID-19 or “2019-nCoV” or “SARS-CoV-2” or (MH Coronavirus Infections))) AND DT 20191201-20300101) (MH “Homeless Persons”) OR (MH “Homelessness”) TI (homeless*) OR AB (homeless *) TI (Rough N3 sleep*) OR AB (Rough N3 sleep*) TI (“Housing insecur*”) OR AB (“Housing insecur*”) S2 OR S3 OR S4 OR S5 S6 AND S1 |
| Web of Science |
| ((“Wuhan coronavirus” OR “COVID-19 *” OR “COVID-19*” OR “COVID-2019*” OR “coronavirus disease 2019” OR “SARS-CoV-2” OR “2019-nCoV” OR “2019 novel coronavirus” OR “severe acute respiratory syndrome coronavirus 2” OR “2019 novel coronavirus infection” OR “coronavirus disease 2019” OR “coronavirus disease-19” OR “SARS-CoV-2019” OR “SARS-CoV-19”) AND (homeless* OR (Rough NEAR/3 sleep*) OR (“Housing insecur*”))) |
| PsycINFO |
| (DE “COVID-19”) TI (coronavir* OR “corona virus*” OR “corona pandemic*” OR betacoronavir* OR covid19 OR COVID OR nCoV OR “novel CoV” OR “CoV 2” OR CoV2 OR sarscov2 OR sars2 OR 2019 nCoV OR “wuhan virus*”) OR AB (coronavir* OR “corona virus*” OR “corona pandemic*” OR betacoronavir* OR COVID-19 OR covid OR nCoV OR “novel CoV” OR “CoV 2” OR CoV2 OR sarscov2 OR sars2 OR 2019 nCoV OR “wuhan virus*”) TI (sars AND cov) OR AB (sars AND cov) TI ((wuhan OR hubei OR huanan) AND (“severe acute respiratory” OR pneumonia*) AND outbreak*) OR AB ((wuhan OR hubei OR huanan) AND (“severe acute respiratory” OR pneumonia*) AND outbreak*) S1 OR S2 OR S3 OR S4 DE “Homeless” OR DE “Homeless Mentally ill” TI (homeless*) OR AB (homeless*) TI (Rough N3 sleep*) OR AB (Rough N3 sleep*) TI (“Housing insecur*”) OR AB (“Housing insecur*”) S6 OR S7 OR S8 OR S9 S5 AND S10 |
| Google Scholar (10 pages) |
| coronavirus|“2019nCoV|novelnCoV|nCoV|coronavirus”|CoV|“COVID19”|COVID19|ncov|“SARS-CoV2|CoV 2”|“severe acute respiratory syndrome Coronavirus 2” “rough AROUND (3) sleeper|sleepers|sleeping” coronavirus|“2019nCoV|novelnCoV|nCoV|coronavirus”|CoV|“COVID19”|COVID19|ncov|“SARS-CoV2|CoV 2”|“severe acute respiratory syndrome Coronavirus 2” homeless|homelessness |
References
- Worldometer. Coronavirus Statistics. Available online: https://www.worldometers.info/coronavirus/ (accessed on 26 January 2022).
- Moghadas, S.M.; Vilches, T.N.; Zhang, K.; Wells, C.R.; Shoukat, A.; Singer, B.H.; Meyers, L.A.; Neuzil, K.M.; Langley, J.M.; Fitzpatrick, M.C.; et al. The Impact of Vaccination on Coronavirus Disease 2019 (COVID-19) Outbreaks in the United States. Clin. Infect. Dis. 2021, 73, 2257–2264. [Google Scholar] [CrossRef] [PubMed]
- Calderón-Larrañaga, A.; Dekhtyar, S.; Vetrano, D.L.; Bellander, T.; Fratiglioni, L. COVID-19: Risk accumulation among biologically and socially vulnerable older populations. Ageing Res. Rev. 2020, 63, 101149. [Google Scholar] [CrossRef] [PubMed]
- Tregoning, J.S.; Flight, K.E.; Higham, S.L.; Wang, Z.; Pierce, B.F. Progress of the COVID-19 vaccine effort: Viruses, vaccines and variants versus efficacy, effectiveness and escape. Nat. Rev. Immunol. 2021, 21, 626–636. [Google Scholar] [CrossRef] [PubMed]
- Leifheit, K.M.; Chaisson, L.H.; Medina, J.A.; Wahbi, R.N.; Shover, C.L. Elevated Mortality Among People Experiencing Homelessness With COVID-19. Open Forum Infect. Dis. 2021, 8, ofab301. [Google Scholar] [CrossRef]
- Perri, M.; Dosani, N.; Hwang, S.W. COVID-19 and people experiencing homelessness: Challenges and mitigation strategies. CMAJ 2020, 192, E716–E719. [Google Scholar] [CrossRef]
- Roederer, T.; Mollo, B.; Vincent, C.; Nikolay, B.; Llosa, A.E.; Nesbitt, R.; Vanhomwegen, J.; Rose, T.; Goyard, S.; Anna, F.; et al. Seroprevalence and risk factors of exposure to COVID-19 in homeless people in Paris, France: A cross-sectional study. Lancet Public Health 2021, 6, e202–e209. [Google Scholar] [CrossRef]
- Schrooyen, L.; Delforge, M.; Lebout, F.; Vanbaelen, T.; Lecompte, A.; Dauby, N. Homeless people hospitalized with COVID-19 in Brussels. Clin. Microbiol. Infect. 2021, 27, 151–152. [Google Scholar] [CrossRef]
- Tsai, J.; Wilson, M. COVID-19: A potential public health problem for homeless populations. Lancet Public Health 2020, 5, e186–e187. [Google Scholar] [CrossRef]
- Silva, D.S.; Smith, M.J. Social distancing, social justice, and risk during the COVID-19 pandemic. Can. J. Public Health 2020, 111, 459–461. [Google Scholar] [CrossRef]
- Montgomery, M.P.; Carry, M.G.; Garcia-Williams, A.G.; Marshall, B.; Besrat, B.; Bejarano, F.; Carlson, J.; Rutledge, T.; Mosites, E. Hand hygiene during the COVID-19 pandemic among people experiencing homelessness—Atlanta, Georgia, 2020. J. Community Psychol. 2021, 49, 2441–2453. [Google Scholar] [CrossRef]
- Rodriguez, N.M.; Lahey, A.M.; MacNeill, J.J.; Martinez, R.G.; Teo, N.E.; Ruiz, Y. Homelessness during COVID-19: Challenges, Responses, and Lessons Learned from Homeless Service Providers in Tippecanoe County, Indiana. BMC Public Health 2021, 21, 1657. [Google Scholar] [CrossRef] [PubMed]
- Allaria, C.; Loubière, S.; Mosnier, E.; Monfardini, E.; Auquier, P.; Tinland, A. “Locked down outside”: Perception of hazard and health resources in COVID-19 epidemic context among homeless people. SSM Popul. Health 2021, 15, 100829. [Google Scholar] [CrossRef] [PubMed]
- Farhoudian, A.; Radfar, S.R.; Mohaddes Ardabili, H.; Rafei, P.; Ebrahimi, M.; Khojasteh Zonoozi, A.; De Jong, C.A.J.; Vahidi, M.; Yunesian, M.; Kouimtsidis, C.; et al. A Global Survey on Changes in the Supply, Price, and Use of Illicit Drugs and Alcohol, and Related Complications During the 2020 COVID-19 Pandemic. Front. Psychiatry 2021, 12, 1134. [Google Scholar] [CrossRef]
- Ali, F.; Russell, C.; Nafeh, F.; Rehm, J.; LeBlanc, S.; Elton-Marshall, T. Changes in substance supply and use characteristics among people who use drugs (PWUD) during the COVID-19 global pandemic: A national qualitative assessment in Canada. Int. J. Drug Policy 2021, 93, 103237. [Google Scholar] [CrossRef] [PubMed]
- Glick, S.N.; Prohaska, S.M.; LaKosky, P.A.; Juarez, A.M.; Corcorran, M.A.; Des Jarlais, D.C. The Impact of COVID-19 on Syringe Services Programs in the United States. AIDS Behav. 2020, 24, 2466–2468. [Google Scholar] [CrossRef] [PubMed]
- Picchio, C.A.; Valencia, J.; Doran, J.; Swan, T.; Pastor, M.; Martró, E.; Colom, J.; Lazarus, J.V. The impact of the COVID-19 pandemic on harm reduction services in Spain. Harm Reduct. J. 2020, 17, 87. [Google Scholar] [CrossRef]
- Radfar, S.R.; De Jong, C.A.J.; Farhoudian, A.; Ebrahimi, M.; Rafei, P.; Vahidi, M.; Yunesian, M.; Kouimtsidis, C.; Arunogiri, S.; Massah, O.; et al. Reorganization of Substance Use Treatment and Harm Reduction Services During the COVID-19 Pandemic: A Global Survey. Front. Psychiatry 2021, 12, 349. [Google Scholar] [CrossRef]
- Vasylyeva, T.I.; Smyrnov, P.; Strathdee, S.; Friedman, S.R. Challenges posed by COVID-19 to people who inject drugs and lessons from other outbreaks. J. Int. AIDS Soc. 2020, 23, e25583. [Google Scholar] [CrossRef]
- Aguilar, L.; Vicente-Hernández, B.; Remón-Gallo, D.; García-Ullán, L.; Valriberas-Herrero, I.; Maciá-Casas, A.; Pérez-Madruga, A.; Garzón, M.Á.; Álvarez-Navares, A.; Roncero, C. A real-world ten-week follow-up of the COVID outbreak in an outpatient drug clinic in Salamanca (Spain). J. Subst. Abus. Treat 2021, 125, 108303. [Google Scholar] [CrossRef]
- Irwin, M.D.; Amanuel, Y.; Bickers, B.; Nguyen, M.A.; Russell, O.W. Impacts of the COVID-19 Pandemic on Preexisting Racial and Ethnic Disparities, and Results of an Integrated Safety Net Response in Arlington County, Virginia. Health Secur. 2021, 19, S62–S71. [Google Scholar] [CrossRef]
- O’Carroll, A.; Duffin, T.; Collins, J. Harm reduction in the time of COVID-19: Case study of homelessness and drug use in Dublin, Ireland. Int. J. Drug Policy 2021, 87, 102966. [Google Scholar] [CrossRef] [PubMed]
- Parkes, T.; Carver, H.; Masterton, W.; Falzon, D.; Dumbrell, J.; Grant, S.; Wilson, I. “You know, we can change the services to suit the circumstances of what is happening in the world”: A rapid case study of the COVID-19 response across city centre homelessness and health services in Edinburgh, Scotland. Harm Reduct. J. 2021, 18, 64. [Google Scholar] [CrossRef] [PubMed]
- Krawczyk, N.; Fawole, A.; Yang, J.; Tofighi, B. Early innovations in opioid use disorder treatment and harm reduction during the COVID-19 pandemic: A scoping review. Addict. Sci. Clin. Pract. 2021, 16, 68. [Google Scholar] [CrossRef]
- Parkes, T.; Carver, H.; Masterton, W.; Falzon, D.; Dumbrell, J.; Grant, S.; Wilson, I. ‘They already operated like it was a crisis, because it always has been a crisis’: A qualitative exploration of the response of one homeless service in Scotland to the COVID-19 pandemic. Harm Reduct. J. 2021, 18, 26. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.; Andrés, P.; Bullón, A.; Villegas, J.L.; de la Iglesia-Larrad, J.I.; Bote, B.; Prieto, N.; Roncero, C. COVID pandemic as an opportunity for improving mental health treatments of the homeless people. Int. J. Soc. Psychiatry 2021, 67, 335–343. [Google Scholar] [CrossRef]
- Levesque, J.; Loranger, N.; Sehn, C.; Johnson, S.; Pugh, D.; Babando, J. COVID-19 prevalence and infection control measures at homeless shelters and hostels in high-income countries: Protocol for a scoping review. YorkSpace 2021. [Google Scholar] [CrossRef]
- Mohsenpour, A.; Bozorgmehr, K.; Rohleder, S.; Stratil, J.; Costa, D. SARS-CoV-2 prevalence, transmission, health-related outcomes and control strategies in homeless shelters: Systematic review and meta-analysis. eClinicalMedicine 2021, 38, 101032. [Google Scholar] [CrossRef]
- Babando, J.; Quesnel, D.A.; Woodmass, K.; Lomness, A.; Graham, J.R. Responding to pandemics and other disease outbreaks in homeless populations: A review of the literature and content analysis. Health Soc. Care Community 2021, 30, 11–26. [Google Scholar] [CrossRef]
- Jang, H.S.; Shi, Y.; Keyes, L.; Dicke, L.A.; Kim, J. Responding to the Needs of the Homeless in the COVID-19 Pandemic: A Review of Initiatives in 20 Major U.S. Cities. Int. J. Public Adm. 2021, 44, 1006–1017. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19-11 March 2020; World Health Organization: Geneva, Switzerland, 2020.
- Samuels, E.A.; Karb, R.; Vanjani, R.; Trimbur, M.C.; Napoli, A. Congregate Shelter Characteristics and Prevalence of Asymptomatic SARS-CoV-2. medRxiv 2020. [Google Scholar] [CrossRef]
- Redditt, V.; Wright, V.; Rashid, M.; Male, R.; Bogoch, I. Outbreak of SARS-CoV-2 infection at a large refugee shelter in Toronto, April 2020: A clinical and epidemiologic descriptive analysis. CMAJ Open 2020, 8, E819–E824. [Google Scholar] [CrossRef] [PubMed]
- Aranda-Díaz, A.; Imbert, E.; Strieff, S.; Graham-Squire, D.; Evans, J.L.; Moore, J.; McFarland, W.; Fuchs, J.; Handley, M.A.; Kushel, M. Implementation of Rapid and Frequent SARS-CoV2 Antigen Testing and Response in Congregate Homeless Shelters. medRxiv 2021. [Google Scholar] [CrossRef]
- Jatt, L.P.; Winnett, A.; Graber, C.J.; Vallone, J.; Beenhouwer, D.O.; Goetz, M.B. Widespread severe acute respiratory coronavirus virus 2 (SARS-CoV-2) laboratory surveillance program to minimize asymptomatic transmission in high-risk inpatient and congregate living settings. Infect. Control Hosp. Epidemiol. 2020, 41, 1331–1334. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Ma, H.; Yiu, K.C.Y.; Calzavara, A.; Landsman, D.; Luong, L.; Chan, A.K.; Kustra, R.; Kwong, J.C.; Boily, M.-C.; et al. Heterogeneity in testing, diagnosis and outcome in SARS-CoV-2 infection across outbreak settings in the Greater Toronto Area, Canada: An observational study. CMAJ Open 2020, 8, E627–E636. [Google Scholar] [CrossRef] [PubMed]
- Kiran, T.; Craig-Neil, A.; Das, P.; Lockwood, J.; Wang, R.; Nathanielsz, N.; Rosenthal, E.; Snider, C.; Hwang, S.W. Factors associated with SARS-CoV-2 positivity in 20 homeless shelters in Toronto, Canada, from April to July 2020: A repeated cross-sectional study. CMAJ Open 2021, 9, E302–E308. [Google Scholar] [CrossRef] [PubMed]
- Le Bihan, C.; Faucherre, V.; Le Moing, V.; Mehenni, A.; Nantes, D.; Da Silva, A.; Jaume, C.; Lassalle, F.; Makinson, A. COVID-19: The forgotten cases of hidden exiles. Infect. Dis. Now 2021, 51, 387–390. [Google Scholar] [CrossRef]
- Yoon, J.C.; Montgomery, M.P.; Buff, A.M.; Boyd, A.T.; Jamison, C.; Hernandez, A.; Schmit, K.; Shah, S.; Ajoku, S.; Holland, D.P.; et al. Coronavirus Disease 2019 (COVID-19) Prevalences Among People Experiencing Homelessness and Homelessness Service Staff During Early Community Transmission in Atlanta, Georgia, April–May 2020. Clin. Infect. Dis. 2021, 73, e2978–e2984. [Google Scholar] [CrossRef]
- Marquez, H.; Ramers, C.; Northrup, A.; Tam, A.; Liu, J.; Rojas, S.; Klaman, S.; Khasira, M.; Madbak, J.; Matthews, E.; et al. Response to the Coronavirus Disease 2019 Pandemic Among People Experiencing Homelessness in Congregant Living Settings in San Diego, California. Clin. Infect. Dis. 2021, 73, e805–e807. [Google Scholar] [CrossRef]
- Ly, T.D.A.; Hoang, V.T.; Goumballa, N.; Louni, M.; Canard, N.; Dao, T.L.; Medkour, H.; Borg, A.; Bardy, K.; Esteves-Vieira, V.; et al. Variations in respiratory pathogen carriage among a homeless population in a shelter for men in Marseille, France, March-July 2020: Cross-sectional 1-day surveys. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 1579–1582. [Google Scholar] [CrossRef]
- Mosites, E.; Parker, E.M.; Clarke, K.E.N.; Gaeta, J.M.; Baggett, T.P.; Imbert, E.; Sankaran, M.; Scarborough, A.; Huster, K.; Hanson, M. Assessment of SARS-CoV-2 infection prevalence in homeless shelters—four US cities, March 27–April 15, 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, J.H.; Link, A.C.; McCulloch, D.; Brandstetter, E.; Newman, K.L.; Jackson, M.L.; Hughes, J.P.; Englund, J.A.; Boeckh, M.; Sugg, N. Characteristics of COVID-19 in homeless shelters: A community-based surveillance study. Ann. Intern. Med. 2021, 174, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Rincón, A.; Moreso, F.; López-Herradón, A.; Fernández-Robres, M.A.; Cidraque, I.; Nin, J.; Méndez, O.; López, M.; Pájaro, C.; Satorra, À. The keys to control a COVID-19 outbreak in a haemodialysis unit. Clin. Kidney J. 2020, 13, 542–549. [Google Scholar] [CrossRef] [PubMed]
- Karb, R.; Samuels, E.; Vanjani, R.; Trimbur, C.; Napoli, A. Homeless shelter characteristics and prevalence of SARS-CoV-2. West. J. Emerg. Med. 2020, 21, 1048. [Google Scholar] [CrossRef]
- Ly, T.D.A.; Nguyen, N.N.; Goumballa, N.; Louni, M.; Canard, N.; Dao, T.L.; Medkour, H.; Borg, A.; Bardy, K.; Esteves-Vieira, V. Screening of SARS-CoV-2 among homeless people, asylum-seekers and other people living in precarious conditions in Marseille, France, March–April 2020. Int. J. Infect. Dis. 2021, 105, 1–6. [Google Scholar] [CrossRef]
- Ghinai, I.; Davis, E.S.; Mayer, S.; Toews, K.-A.; Huggett, T.D.; Snow-Hill, N.; Perez, O.; Hayden, M.K.; Tehrani, S.; Landi, A.J. Risk factors for severe acute respiratory syndrome coronavirus 2 infection in homeless shelters in Chicago, Illinois—March–May, 2020. Open Forum Infect. Dis. 2020, 7, ofaa477. [Google Scholar] [CrossRef]
- Fields, V.L.; Kiphibane, T.; Eason, J.T.; Hafoka, S.F.; Lopez, A.S.; Schwartz, A.; Henry, A.; Tran, C.H.; Tate, J.E.; Kirking, H.L. Assessment of contact tracing for COVID-19 among people experiencing homelessness, Salt Lake County Health Department, March–May 2020. Ann. Epidemiol. 2021, 59, 50–55. [Google Scholar] [CrossRef]
- Baggett, T.P.; Keyes, H.; Sporn, N.; Gaeta, J.M. Prevalence of SARS-CoV-2 infection in residents of a large homeless shelter in Boston. JAMA 2020, 323, 2191–2192. [Google Scholar] [CrossRef]
- Cardenas, J.; Roach, J.; Kopelowicz, A. Prevalence of COVID 19 Positive Cases Presenting to a Psychiatric Emergency Room. Community Ment. Health J. 2021, 57, 1240–1243. [Google Scholar] [CrossRef]
- Ralli, M.; Morrone, A.; Arcangeli, A.; Ercoli, L. Asymptomatic patients as a source of transmission of COVID-19 in homeless shelters. Int. J. Infect. Dis. 2021, 103, 243–245. [Google Scholar] [CrossRef]
- Fuchs, J.D.; Carter, H.C.; Evans, J.; Graham-Squire, D.; Imbert, E.; Bloome, J.; Fann, C.; Skotnes, T.; Sears, J.; Pfeifer-Rosenblum, R. Assessment of a Hotel-Based COVID-19 Isolation and Quarantine Strategy for Persons Experiencing Homelessness. JAMA Netw. Open 2021, 4, e210490. [Google Scholar] [CrossRef] [PubMed]
- O’Shea, T.; Bodkin, C.; Mokashi, V.; Beal, K.; Wiwcharuk, J.; Lennox, R.; Guenter, D.; Smieja, M.; Bulir, D.; Chong, S. Pandemic Planning in Homeless Shelters: A Pilot Study of a Coronavirus Disease 2019 (COVID-19) Testing and Support Program to Mitigate the Risk of COVID-19 Outbreaks in Congregate Settings. Clin. Infect. Dis. 2021, 72, 1639–1641. [Google Scholar] [CrossRef] [PubMed]
- Tobolowsky, F.A.; Gonzales, E.; Self, J.L.; Rao, C.Y.; Keating, R.; Marx, G.E.; McMichael, T.M.; Lukoff, M.D.; Duchin, J.S.; Huster, K. COVID-19 outbreak among three affiliated homeless service sites—King County, Washington, 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 523. [Google Scholar] [CrossRef]
- Baggett, T.P.; Racine, M.W.; Lewis, E.; De Las Nueces, D.; O’Connell, J.J.; Bock, B.; Gaeta, J.M. Addressing COVID-19 among people experiencing homelessness: Description, adaptation, and early findings of a multiagency response in Boston. Public Health Rep. 2020, 135, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Sachdev, D.; Mara, E.; Hsu, L.; Scheer, S.; Rutherford, G.; Enanoria, W.; Gandhi, M. COVID-19 Susceptibility and Outcomes Among People Living With HIV in San Francisco. J. Acquir. Immune. Defic. Syndr. 2021, 86, 19–21. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, M.P.; Paulin, H.N.; Morris, A.; Speers, A.; Boyd, A.T.; Buff, A.M.; Mathews, D.; Wells, A.; Marchman, C.; Gaffga, N. Establishment of Isolation and Noncongregate Hotels During COVID-19 and Symptom Evolution Among People Experiencing Homelessness—Atlanta, Georgia, 2020. J. Public Health Manag. Pract. 2021, 27, 285–294. [Google Scholar] [CrossRef] [PubMed]
- Iacoella, C.; Ralli, M.; Maggiolini, A.; Arcangeli, A.; Ercoli, L. Acceptance of COVID-19 vaccine among persons experiencing homelessness in the City of Rome, Italy. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 3132–3135. [Google Scholar] [CrossRef]
- Brody, J.K.; Rajabiun, S.; Strupp Allen, H.J.; Baggett, T. Enhanced Telehealth Case Management Plus Emergency Financial Assistance for Homeless-Experienced People Living With HIV During the COVID-19 Pandemic. Am. J. Public Health 2021, 111, 835–838. [Google Scholar] [CrossRef]
- Loubiere, S.; Monfardini, E.; Allaria, C.; Mosnier, M.; Allibert, A.; Ninove, L.; Bosetti, T.; Farnarier, C.; Hamouda, I.; Auquier, P. Seroprevalence of SARS-CoV-2 antibodies among homeless people living rough, in shelters and squats: A large population-based study in France. PLoS ONE 2021, 16, e0255498. [Google Scholar] [CrossRef]
- Röthlin Eriksen, A.R.; Fogh, K.; Hasselbalch, R.B.; Bundgaard, H.; Nielsen, S.D.; Jørgensen, C.S.; Scharff, B.F.S.S.; Erikstrup, C.; Sækmose, S.G.; Holm, D.K.; et al. SARS-CoV-2 antibody prevalence among homeless people, sex workers and shelter workers in Denmark: A nationwide cross-sectional study. medRxiv 2021. [Google Scholar] [CrossRef]
- Routledge, I.; Epstein, A.; Takahashi, S.; Janson, O.; Hakim, J.; Duarte, E.; Turcios, K.; Vinden, J.; Sujishi, K.; Rangel, J.; et al. Citywide serosurveillance of the initial SARS-CoV-2 outbreak in San Francisco using electronic health records. Nat. Commun. 2021, 12, 3566. [Google Scholar] [CrossRef] [PubMed]
- Spinelli, M.A.; Lynch, K.L.; Yun, C.; Glidden, D.V.; Peluso, M.J.; Henrich, T.J.; Gandhi, M.; Brown, L.B. SARS-CoV-2 seroprevalence, and IgG concentration and pseudovirus neutralising antibody titres after infection, compared by HIV status: A matched case-control observational study. Lancet HIV 2021, 8, e334–e341. [Google Scholar] [CrossRef]
- Hickey, M.D.; Sergi, F.; Zhang, K.; Spinelli, M.A.; Black, D.; Sola, C.; Blaz, V.; Nguyen, J.Q.; Oskarsson, J.; Gandhi, M. Pragmatic randomized trial of a pre-visit intervention to improve the quality of telemedicine visits for vulnerable patients living with HIV. J. Telemed. Telecare 2020, 1357633X20976036. [Google Scholar] [CrossRef] [PubMed]
- Ralli, M.; Cedola, C.; Urbano, S.; Latini, O.; Shkodina, N.; Morrone, A.; Arcangeli, A.; Ercoli, L. Assessment of SARS-CoV-2 infection through rapid serology testing in the homeless population in the City of Rome, Italy. Preliminary results. J. Public Health Res. 2020, 9, 1986. [Google Scholar] [CrossRef]
- Krcmery, V.; Bucko, L.; Kimuli, A.; Jackulikova, M.; Kozon, V.; Olah, M.; Kovac, R.; Jancovic, M.; Holkova, J.; Mikolasova, G.; et al. Cohortation and testing of elderly homeless within COVID pademics in an urban environment—Example of a life island mission model. Acta Missiol. 2020, 1, 76–78. [Google Scholar]
- Husain, M.; Rachline, A.; Cousien, A.; Rolland, S.; Rouzaud, C.; Ferre, V.M.; Gomez, M.V.; Le Teurnier, M.; Wicky-Thisse, M.; Descamps, D.; et al. Impact of the COVID-19 pandemic on the homeless: Results from a retrospective closed cohort in France (March–May 2020). Clin. Microbiol. Infect. 2021, 27, 1520.e1–1520.e5. [Google Scholar] [CrossRef]
- Roland, M.; Ben Abdelhafidh, L.; Déom, V.; Vanbiervliet, F.; Coppieters, Y.; Racapé, J. SARS-CoV-2 screening among people living in homeless shelters in Brussels, Belgium. PLoS ONE 2021, 16, e0252886. [Google Scholar] [CrossRef]
- Storgaard, S.F.; Eiset, A.H.; Abdullahi, F.; Wejse, C. First wave of COVID-19 did not reach the homeless population in Aarhus. Dan. Med. J. 2020, 67, A08200594. [Google Scholar]
- Gombita, P.; Olah, M.; Kovac, R.; Jurasek, M.; Kosticova, M.; Taziarova, M.; Zabavova, S.; Haluskova, E.; Jackulikova, M.; Zemko, R. Senior Homeless Population was COVID-19 Free in 3 shelter communities after adapting the Life Island model (Note). Clin. Soc. Work Health Interv. 2020, 11, 78–79. [Google Scholar] [CrossRef]
- Komaromy, M.; Harris, M.; Koenig, R.M.; Tomanovich, M.; Ruiz-Mercado, G.; Barocas, J.A. Caring for COVID’s most vulnerable victims: A safety-net hospital responds. J. Gen. Intern. Med. 2020, 36, 1006–1010. [Google Scholar] [CrossRef]
- Imbert, E.; Kinley, P.M.; Scarborough, A.; Cawley, C.; Sankaran, M.; Cox, S.N.; Kushel, M.; Stoltey, J.; Cohen, S.; Fuchs, J.D. Coronavirus Disease 2019 Outbreak in a San Francisco Homeless Shelter. Clin. Infect. Dis. 2021, 73, 324–327. [Google Scholar] [CrossRef] [PubMed]
- Gaeta, J.M.; De Las Nueces, D.; Munson, D.G.; Barocas, J.A.; Walsh, K.E. Case 21–2020: A 66-year-old homeless man with COVID-19. N. Engl. J. Med. 2020, 383, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Barocas, J.A.; Gai, M.J.; White, L.F.; Faretra, D.; Sachs, K.; Komaromy, M. Implementation of a Recuperation Unit and Hospitalization Rates Among People Experiencing Homelessness With COVID-19. JAMA Netw. Open 2021, 4, e212826. [Google Scholar] [CrossRef] [PubMed]
- Cha, S.; Henry, A.; Montgomery, M.P.; Laws, R.L.; Pham, H.; Wortham, J.; Garg, S.; Kim, L.; Mosites, E.; Team, C.-N.S. Morbidity and Mortality among Adults Experiencing Homelessness Hospitalized with COVID-19. J. Infect. Dis. 2021, 224, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Ly, T.D.A.; Edouard, S.; Badiaga, S.; Tissot-Dupont, H.; Hoang, V.T.; Pommier de Santi, V.; Brouqui, P.; Raoult, D.; Gautret, P. Epidemiology of respiratory pathogen carriage in the homeless population within two shelters in Marseille, France, 2015–2017: Cross sectional 1-day surveys. Clin. Microbiol. Infect. 2019, 25, e241–e249. [Google Scholar] [CrossRef] [Green Version]
- Rozenfeld, Y.; Beam, J.; Maier, H.; Haggerson, W.; Boudreau, K.; Carlson, J.; Medows, R. A model of disparities: Risk factors associated with COVID-19 infection. Int. J. Equity Health 2020, 19, 126. [Google Scholar] [CrossRef]
- Rahi, M.; Le Pluart, D.; Beaudet, A.; Ismaël, S.; Parisey, M.; Poey, N.; Tarhini, H.; Lescure, F.-X.; Yazdanpanah, Y.; Deconinck, L. Sociodemographic characteristics and transmission risk factors in patients hospitalized for COVID-19 before and during the lockdown in France. BMC Infect. Dis. 2021, 21, 812. [Google Scholar] [CrossRef]
- Hsu, H.E.; Ashe, E.M.; Silverstein, M.; Hofman, M.; Lange, S.J.; Razzaghi, H.; Mishuris, R.G.; Davidoff, R.; Parker, E.M.; Penman-Aguilar, A. Race/ethnicity, underlying medical conditions, homelessness, and hospitalization status of adult patients with COVID-19 at an urban safety-net medical center—Boston, Massachusetts, 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 864. [Google Scholar] [CrossRef]
- Song, J.; Grey, C.N.B.; Davies, A.R. Creating an e-cohort of individuals with lived experience of homelessness and subsequent mortality in Wales, UK. J. Public Health 2021, fdab180. [Google Scholar] [CrossRef]
- Hajek, A.; Bertram, F.; Heinrich, F.; van Rüth, V.; Ondruschka, B.; Kretzler, B.; Schüler, C.; Püschel, K.; König, H.-H. Determinants of health care use among homeless individuals: Evidence from the Hamburg survey of homeless individuals. BMC Health Serv. Res. 2021, 21, 317. [Google Scholar] [CrossRef]
- Longchamps, C.; Ducarroz, S.; Crouzet, L.; Vignier, N.; Pourtau, L.; Allaire, C.; Colleville, A.-C.; El Aarbaoui, T.; Melchior, M.; ECHO Study Group. COVID-19 vaccine hesitancy among persons living in homeless shelters in France. Vaccine 2021, 39, 3315–3318. [Google Scholar] [CrossRef] [PubMed]
- Bertram, F.; Heinrich, F.; Fröb, D.; Wulff, B.; Ondruschka, B.; Püschel, K.; König, H.-H.; Hajek, A. Loneliness among Homeless Individuals during the First Wave of the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 3035. [Google Scholar] [CrossRef] [PubMed]
- Henwood, B.F.; Redline, B.; Lahey, J. Surveying Tenants of Permanent Supportive Housing in Skid Row about COVID-19. J. Health Care Poor Underserved 2020, 31, 1587–1594. [Google Scholar] [CrossRef]
- Finnigan, R. Self-reported impacts of the COVID-19 pandemic for people experiencing homelessness in Sacramento, California. J. Soc. Distress Homelessness 2021. [Google Scholar] [CrossRef]
- Kuhn, R.; Henwood, B.; Lawton, A.; Kleva, M.; Murali, K.; King, C.; Gelberg, L. COVID-19 vaccine access and attitudes among people experiencing homelessness from pilot mobile phone survey in Los Angeles, CA. PLoS ONE 2021, 16, e0255246. [Google Scholar] [CrossRef] [PubMed]
- Tucker, J.S.; D’Amico, E.J.; Pedersen, E.R.; Garvey, R.; Rodriguez, A.; Klein, D.J. Behavioral health and service usage during the COVID-19 pandemic among emerging adults currently or recently experiencing homelessness. J. Adolesc. Health 2020, 67, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Hajek, A.; Bertram, F.; van Rüth, V.; Kretzler, B.; Püschel, K.; Heinrich, F.; König, H.-H. Prevalence and factors associated with fear of COVID-19 among homeless individuals during the COVID-19 pandemic: Evidence from the hamburg survey of homeless individuals. Risk Manag. Healthc. Policy 2021, 14, 2689. [Google Scholar] [CrossRef]
- Moore, J.X.; Gilbert, K.L.; Lively, K.L.; Laurent, C.; Chawla, R.; Li, C.; Johnson, R.; Petcu, R.; Mehra, M.; Spooner, A. Correlates of COVID-19 vaccine hesitancy among a community sample of African Americans living in the Southern United States. Vaccines 2021, 9, 879. [Google Scholar] [CrossRef]
- Hsu, H.-T.; Petering, R.; Onasch-Vera, L. Implications of COVID-19 vaccine uptake among young adults experiencing homelessness: A brief report. J. Soc. Distress Homelessness 2021, 1–6. [Google Scholar] [CrossRef]
- Appa, A.; Rodda, L.N.; Cawley, C.; Zevin, B.; Coffin, P.O.; Gandhi, M.; Imbert, E. Drug Overdose Deaths Before and After Shelter-in-Place Orders During the COVID-19 Pandemic in San Francisco. JAMA Netw. Open 2021, 4, e2110452. [Google Scholar] [CrossRef]
- Ramaswamy, M.; Hemberg, J.; Faust, A.; Wickliffe, J.; Comfort, M.; Lorvick, J.; Cropsey, K. Criminal justice–involved women navigate COVID-19: Notes from the field. Health Educ. Behav. 2020, 47, 544–548. [Google Scholar] [CrossRef] [PubMed]
- Barbu, S.; Perez, S.; Silk, R.; Coyne, A. The Impact of COVID-19 on Homeless Service Providers & Homeless People: The Migrant Perspective; FEANTSA: Brussels, Belgium, 2021. [Google Scholar]
- Cironi, K.A.; Jones, A.T.; Hauser, E.M.; Olsen, J.W.; Kissinger, P.J. Human Immunodeficiency Virus and Hepatitis C Linkage-to-Care Initiative for New Orleans Residents Experiencing Homelessness During the COVID-19 Pandemic. Sex. Transm. Dis. 2021, 48, 595–600. [Google Scholar] [CrossRef]
- Leonardi, D.; Stefani, S. The pandemic and homeless people in the Turin area: The level of housing adequacy shapes experiences and well-being. Hous. Care Support 2021, 24, 93–104. [Google Scholar] [CrossRef]
- Pixley, C.L.; Henry, F.A.; DeYoung, S.E.; Settembrino, M.R. The role of homelessness community based organizations during COVID-19. J. Community Psychol. 2021, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Kelly, D.; Murphy, H.; Vadlamudi, R.; Kraut, R.; Dalessio, K.; Malani, A.N.; Glabach, M.; Marquez, J.L. Successful public health measures preventing coronavirus disease 2019 (COVID-19) at a Michigan homeless shelter. Infect. Control Hosp. Epidemiol. 2021, 42, 1155–1156. [Google Scholar] [CrossRef]
- Aitken, E. COVID-19: Opportunity to improve crisis responses to homelessness? J. R. Coll. Physicians Edinb. 2021, 51, S53–S62. [Google Scholar] [CrossRef]
- Brown, D.; Edwards, F.L. Sheltering the Homeless during COVID-19 in San Jose, California. Int. J. Public Adm. 2021, 44, 952–962. [Google Scholar] [CrossRef]
- National Social Inclusion Office. National COVID-19 Homeless Service User Experience Survey—Report of Findings; HSE: Dublin, Ireland, 2020.
- Fitzpatrick, S.; Watts, B.; Sims, R. Homelessness Monitor England 2020: COVID-19 Crisis Response Briefing; Crisis: London, UK, 2020. [Google Scholar]
- Wilkinson, R.; Mandal, S.; Phipps, E. Evaluation of Hepatitis C Test and Treat Interventions Targeted at Homeless Populations (Outside London) in England During the COVID-19 Pandemic. Clin. Liver Dis. 2021, 17, 90–94. [Google Scholar] [CrossRef]
- Scallan, E.; Bodkin, C.; Wiwcharuk, J.; O’Shea, T.; Lennox, R. Finding stability amidst the COVID-19 pandemic: The impact of emergency temporary housing for people who use drugs. Drug Alcohol Rev. 2021, 41, 7–8. [Google Scholar] [CrossRef]
- Riley, E.D.; Raven, M.C.; Dilworth, S.E.; Braun, C.; Imbert, E.; Doran, K.M. Using a “Big Events” framework to understand emergency department use among women experiencing homelessness or housing instability in San Francisco during the COVID-19 pandemic. Int. J. Drug Policy 2021, 97, 103405. [Google Scholar] [CrossRef]
- Ramírez-Cervantes, K.L.; Romero-Pardo, V.; Pérez-Tovar, C.; Martínez-Alés, G.; Quintana-Diaz, M. A medicalized hotel as a public health resource for the containment of COVID-19: More than a place for quarantining. J. Public Health 2021, 43, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.Y.; Palma, M.L.; Haley, C.; Watts, J.; Hinami, K. Rapid Creation of a Multiagency Alternate Care Site for COVID-19—Positive Individuals Experiencing Homelessness. Am. J. Public Health 2021, 111, 1227–1230. [Google Scholar] [CrossRef] [PubMed]
- Mehtani, N.J.; Ristau, J.T.; Snyder, H.; Surlyn, C.; Eveland, J.; Smith-Bernardin, S.; Knight, K.R. COVID-19: A catalyst for change in telehealth service delivery for opioid use disorder management. Subst. Abus. 2021, 42, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Redondo-Sama, G.; Matulic, V.; Munté-Pascual, A.; de Vicente, I. Social work during the COVID-19 crisis: Responding to urgent social needs. Sustainability 2020, 12, 8595. [Google Scholar] [CrossRef]
- Steer, K.J.D.; Klassen, D.C.; O’Gorman, C.M.; Webster, M.; Mitchell, M.; Krichevsky, L.; Christiansen, K.; Benham, J.L.; Schindler, R.S. Cups for COVID: Rapid implementation of a harm reduction initiative to support populations experiencing homelessness during the COVID-19 pandemic. Can. J. Public Health 2021, 112, 29–35. [Google Scholar] [CrossRef]
- Riley, E.D.; Dilworth, S.E.; Satre, D.D.; Silverberg, M.J.; Neilands, T.B.; Mangurian, C.; Weiser, S.D. Factors associated with symptoms of depression and anxiety among women experiencing homelessness and unstable housing during the COVID-19 pandemic. JAMA Netw. Open 2021, 4, e2117035. [Google Scholar] [CrossRef]
- Dempsey, D.; Pautz, H. Food Insecurity in Times of COVID-19—An Insight into a Deepening Crisis; UWS-Oxfam Partnership: Scotland, UK, 2021. [Google Scholar]
- Harris, M.; Johnson, S.; Mackin, S.; Saitz, R.; Walley, A.Y.; Taylor, J.L. Low barrier tele-buprenorphine in the time of COVID-19: A case report. J. Addict. Med. 2020, 14, e136–e138. [Google Scholar] [CrossRef]
- Hickey, M.D.; Imbert, E.; Glidden, D.V.; Del Rosario, J.B.; Chong, M.; Clemenzi-Allen, A.; Oskarsson, J.; Riley, E.D.; Gandhi, M.; Havlir, D.V. Viral suppression during COVID-19 among people with HIV experiencing homelessness in a low-barrier clinic-based program. AIDS 2021, 35, 517–519. [Google Scholar] [CrossRef]
- van Rüth, V.; König, H.H.; Bertram, F.; Schmiedel, P.; Ondruschka, B.; Püschel, K.; Heinrich, F.; Hajek, A. Determinants of health-related quality of life among homeless individuals during the COVID-19 pandemic. Public Health 2021, 194, 60–66. [Google Scholar] [CrossRef]
- Thomas, J.; Bowes, N.; Meyers, R.; Thirlaway, K. Mental well-being and physical activity of young people experiencing homelessness before and during COVID-19 lockdown: A longitudinal study. Ment. Health Phys. Act. 2021, 21, 100407. [Google Scholar] [CrossRef]
- Ferguson, J.M.; Jacobs, J.; Yefimova, M.; Greene, L.; Heyworth, L.; Zulman, D.M. Virtual care expansion in the Veterans Health Administration during the COVID-19 pandemic: Clinical services and patient characteristics associated with utilization. J. Am. Med. Inform. Assoc. 2021, 28, 453–462. [Google Scholar] [CrossRef]
- Spinelli, M.A.; Hickey, M.D.; Glidden, D.V.; Nguyen, J.Q.; Oskarsson, J.J.; Havlir, D.; Gandhi, M. Viral suppression rates in a safety-net HIV clinic in San Francisco destabilized during COVID-19. AIDS 2020, 34, 2328–2331. [Google Scholar] [CrossRef]
- O’Connell, J.J. Nontuberculous respiratory infections among the homeless. Semin. Respir. Infect. 1991, 6, 247–253. [Google Scholar]
- Thiberville, S.-d.; Salez, N.; Benkouiten, S.; Badiaga, S.; Charrel, R.; Brouqui, P. Respiratory viruses within homeless shelters in Marseille, France. BMC Res. Notes 2014, 7, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, R.T.; Hemati, K.; Riley, E.D.; Lee, C.T.; Ponath, C.; Tieu, L.; Guzman, D.; Kushel, M.B. Geriatric Conditions in a Population-Based Sample of Older Homeless Adults. Gerontologist 2017, 57, 757–766. [Google Scholar] [CrossRef]
- Seastres, R.J.; Hutton, J.; Zordan, R.; Moore, G.; Mackelprang, J.; Kiburg, K.V.; Sundararajan, V. Long-term effects of homelessness on mortality: A 15-year Australian cohort study. Aust. N. Z. J. Public Health 2020, 44, 476–481. [Google Scholar] [CrossRef]
- Benavides, A.D.; Nukpezah, J.A. How local governments are caring for the homeless during the COVID-19 pandemic. Am. Rev. Public Adm. 2020, 50, 650–657. [Google Scholar] [CrossRef]
- Conway, B.; Truong, D.; Wuerth, K. COVID-19 in homeless populations: Unique challenges and opportunities. Future Virol. 2020, 15, 331–334. [Google Scholar] [CrossRef]
- Richardson, J. Has homeless rough sleeping in the UK and Europe been solved in the wake of the COVID-19 pandemic? In Power, Media and the COVID-19 Pandemic: Framing Public Discourse; Price, S., Harbisher, B., Eds.; Routledge: London, UK, 2021. [Google Scholar]
- Brown, R.T.; Miao, Y.; Mitchell, S.L.; Bharel, M.; Patel, M.; Ard, K.L.; Grande, L.J.; Blazey-Martin, D.; Floru, D.; Steinman, M.A. Health outcomes of obtaining housing among older homeless adults. Am. J. Public Health 2015, 105, 1482–1488. [Google Scholar] [CrossRef]
- Schick, V.; Wiginton, L.; Crouch, C.; Haider, A.; Isbell, F. Integrated service delivery and health-related quality of life of individuals in permanent supportive housing who were formerly chronically homeless. Am. J. Public Health 2019, 109, 313–319. [Google Scholar] [CrossRef] [Green Version]
- Bean, K.F.; Shafer, M.S.; Glennon, M. The impact of housing first and peer support on people who are medically vulnerable and homeless. Psychiatr. Rehabil. J. 2013, 36, 48–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolf, J.; Burnam, A.; Koegel, P.; Sullivan, G.; Morton, S. Changes in subjective quality of life among homeless adults who obtain housing: A prospective examination. Soc. Psychiatry Psychiatr. Epidemiol. 2001, 36, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Driscoll, D.L.; Johnston, J.M.; Chapman, C.; Hedwig, T.; Shimer, S.; Barker, R.; Burke, N.; Baldwin, M.; Brown, R.A. Changes in the health status of newly housed chronically homeless: The Alaska Housing First program evaluation. J. Soc. Distress Homeless 2018, 27, 34–43. [Google Scholar] [CrossRef]
- Kirst, M.; Zerger, S.; Misir, V.; Hwang, S.; Stergiopoulos, V. The impact of a Housing First randomized controlled trial on substance use problems among homeless individuals with mental illness. Drug Alcohol Depend. 2015, 146, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Tsai, J.; Rosenheck, R.A. Homeless veterans in supported housing: Exploring the impact of criminal history. Psychol. Serv. 2013, 10, 452–458. [Google Scholar] [CrossRef]
- Martinez, T.E.; Burt, M.R. Impact of permanent supportive housing on the use of acute care health services by homeless adults. Psychiatr. Serv. 2006, 57, 992–999. [Google Scholar] [CrossRef]
- Sadowski, L.S.; Kee, R.A.; VanderWeele, T.J.; Buchanan, D. Effect of a housing and case management program on emergency department visits and hospitalizations among chronically ill homeless adults: A randomized trial. JAMA 2009, 301, 1771–1778. [Google Scholar] [CrossRef] [Green Version]
- Talevi, D.; Socci, V.; Carai, M.; Carnaghi, G.; Faleri, S.; Trebbi, E.; di Bernardo, A.; Capelli, F.; Pacitti, F. Mental health outcomes of the COVID-19 pandemic. Riv. Di Psichiatr. 2020, 55, 137–144. [Google Scholar] [CrossRef]
- Khan, K.S.; Mamun, M.A.; Griffiths, M.D.; Ullah, I. The mental health impact of the COVID-19 pandemic across different cohorts. Int. J. Ment. Health Addict. 2020, 20, 380–386. [Google Scholar] [CrossRef]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef]
- Fazel, S.; Khosla, V.; Doll, H.; Geddes, J. The prevalence of mental disorders among the homeless in western countries: Systematic review and meta-regression analysis. PLoS Med. 2008, 5, e225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlyle, M.; Leung, J.; Walter, Z.C.; Juckel, J.; Salom, C.; Quinn, C.A.; Davidson, L.; Ellem, R.; Newland, G.; Hides, L. Changes in Substance Use Among People Seeking Alcohol and Other Drug Treatment During the COVID-19 Pandemic: Evaluating Mental Health Outcomes and Resilience. Subst. Abus. 2021, 15, 11782218211061746. [Google Scholar] [CrossRef] [PubMed]
- Schecke, H.; Fink, M.; Bäuerle, A.; Skoda, E.-M.; Schweda, A.; Musche, V.; Dinse, H.; Weismüller, B.M.; Moradian, S.; Scherbaum, N. Changes in Substance Use and Mental Health Burden among Women during the Second Wave of COVID-19 in Germany. Int. J. Environ. Res. Public Health 2021, 18, 9728. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Ebbert, J.O.; Rosedahl, J.K.; Philpot, L.M. Changes in substance use among young adults during a respiratory disease pandemic. SAGE Open Med. 2020, 8, 2050312120965321. [Google Scholar] [CrossRef]
- Doraiswamy, S.; Abraham, A.; Mamtani, R.; Cheema, S. Use of telehealth during the COVID-19 pandemic: Scoping review. J. Med. Internet. Res. 2020, 22, e24087. [Google Scholar] [CrossRef]
- Koonin, L.M.; Hoots, B.; Tsang, C.A.; Leroy, Z.; Farris, K.; Jolly, B.; Antall, P.; McCabe, B.; Zelis, C.B.R.; Tong, I. Trends in the use of telehealth during the emergence of the COVID-19 pandemic—United States, January–March 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1595. [Google Scholar] [CrossRef]
- Pierce, B.S.; Perrin, P.B.; Tyler, C.M.; McKee, G.B.; Watson, J.D. The COVID-19 telepsychology revolution: A national study of pandemic-based changes in US mental health care delivery. Am. Psychol. 2021, 76, 14. [Google Scholar] [CrossRef]
- McInnes, D.K.; Li, A.E.; Hogan, T.P. Opportunities for engaging low-income, vulnerable populations in health care: A systematic review of homeless persons’ access to and use of information technologies. Am. J. Public Health 2013, 103 (Suppl. 2), e11–e24. [Google Scholar] [CrossRef]
- Lowrie, R.; Stock, K.; Lucey, S.; Knapp, M.; Williamson, A.; Montgomery, M.; Lombard, C.; Maguire, D.; Allan, R.; Blair, R. Pharmacist led homeless outreach engagement and non-medical independent prescribing (Rx)(PHOENIx) intervention for people experiencing homelessness: A non-randomised feasibility study. Int. J. Equity Health 2021, 20, 19. [Google Scholar] [CrossRef]
- Jagpal, P.; Saunders, K.; Plahe, G.; Russell, S.; Barnes, N.; Lowrie, R.; Paudyal, V. Research priorities in healthcare of persons experiencing homelessness: Outcomes of a national multi-disciplinary stakeholder discussion in the United Kingdom. Int. J. Equity Health 2020, 19, 86. [Google Scholar] [CrossRef]
- Crock, E. Access to healthcare services for people living with HIV experiencing homelessness-a literature review. Aust. J. Adv. Nurs. 2016, 34, 42–51. [Google Scholar] [CrossRef]
- Christiani, A.; Hudson, A.L.; Nyamathi, A.; Mutere, M.; Sweat, J. Attitudes of homeless and drug-using youth regarding barriers and facilitators in delivery of quality and culturally sensitive health care. J. Child Adolesc. Psychiatr. Nurs. 2008, 21, 154–163. [Google Scholar] [CrossRef] [PubMed]
- Ramsay, N.; Hossain, R.; Moore, M.; Milo, M.; Brown, A. Health care while homeless: Barriers, facilitators, and the lived experiences of homeless individuals accessing health care in a Canadian regional municipality. Qual. Health Res. 2019, 29, 1839–1849. [Google Scholar] [CrossRef] [PubMed]
- Taylor, H.C.; Stuttaford, M.C.; Broad, B.; Vostanis, P. Listening to service users: Young homeless people’s experiences of a new mental health service. J. Child Health Care 2007, 11, 221–230. [Google Scholar] [CrossRef]
- Wittman, F.; Polcin, D.; Sheridan, D. The architecture of recovery: Two kinds of housing assistance for chronic homeless persons with substance use disorders. Drugs Alcohol Today 2017, 17, 157–167. [Google Scholar] [CrossRef] [Green Version]
- Barile, J.P.; Pruitt, A.S.; Parker, J.L. Identifying and understanding gaps in services for adults experiencing homelessness. J. Community Appl. Soc. Psychol. 2020, 30, 262–277. [Google Scholar] [CrossRef]
- Hjemsæter, A.J.; Bramness, J.G.; Drake, R.; Skeie, I.; Monsbakken, B.; Benth, J.Š.; Landheim, A.S. Mortality, cause of death and risk factors in patients with alcohol use disorder alone or poly-substance use disorders: A 19-year prospective cohort study. BMC Psychiatry 2019, 19, 101. [Google Scholar] [CrossRef] [Green Version]
- Torchalla, I.; Strehlau, V.; Li, K.; Krausz, M. Substance use and predictors of substance dependence in homeless women. Drug Alcohol Depend. 2011, 118, 173–179. [Google Scholar] [CrossRef]
- Tsai, J.; Kasprow, W.J.; Rosenheck, R.A. Alcohol and drug use disorders among homeless veterans: Prevalence and association with supported housing outcomes. Addict. Behav. 2014, 39, 455–460. [Google Scholar] [CrossRef]
- Paudyal, V.; MacLure, K.; Forbes-McKay, K.; McKenzie, M.; MacLeod, J.; Smith, A.; Stewart, D. ‘If I die, I die, I don’t care about my health’: Perspectives on self-care of people experiencing homelessness. Health Soc. Care Community 2020, 28, 160–172. [Google Scholar] [CrossRef]
- Maroko, A.R.; Hopper, K.; Gruer, C.; Jaffe, M.; Zhen, E.; Sommer, M. Public restrooms, periods, and people experiencing homelessness: An assessment of public toilets in high needs areas of Manhattan, New York. PLoS ONE 2021, 16, e0252946. [Google Scholar] [CrossRef] [PubMed]
- Vora, S. The Experiences of Menstruation by Homeless Women: A Preliminary Report; Empowering Women: Devon, UK, 2018. [Google Scholar]
- Douglas, M.; Katikireddi, S.V.; Taulbut, M.; McKee, M.; McCartney, G. Mitigating the wider health effects of COVID-19 pandemic response. BMJ 2020, 369, m1557. [Google Scholar] [CrossRef] [PubMed]
- Hartley, D.M.; Perencevich, E.N. Public health interventions for COVID-19: Emerging evidence and implications for an evolving public health crisis. JAMA 2020, 323, 1908–1909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marçal, K.E.; Fowler, P.J.; Hovmand, P.S.; Cohen, J. Understanding Mechanisms Driving Family Homeless Shelter Use and Child Mental Health. J. Soc. Serv. Res. 2021, 47, 473–485. [Google Scholar] [CrossRef]
- Lima, N.N.R.; de Souza, R.I.; Feitosa, P.W.G.; de Sousa Moreira, J.L.; da Silva, C.G.L.; Neto, M.L.R. People experiencing homelessness: Their potential exposure to COVID-19. Psychiatry Res 2020, 288, 112945. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.-C.; Strong, C.; Pakpour, A.H.; Griffiths, M.D.; Lin, C.-Y. Factors related to preventive COVID-19 infection behaviors among people with mental illness. J. Formos. Med. Assoc. 2020, 119, 1772–1780. [Google Scholar] [CrossRef]
- Harper, C.A.; Satchell, L.P.; Fido, D.; Latzman, R.D. Functional fear predicts public health compliance in the COVID-19 pandemic. Int. J. Ment. Health Addict. 2021, 19, 1875–1888. [Google Scholar] [CrossRef]
- Lee, M.; You, M. Psychological and Behavioral Responses in South Korea During the Early Stages of Coronavirus Disease 2019 (COVID-19). Int. J. Environ. Res. Public Health 2020, 17, 2977. [Google Scholar] [CrossRef]
- Yıldırım, M.; Geçer, E.; Akgül, Ö. The impacts of vulnerability, perceived risk, and fear on preventive behaviours against COVID-19. Psychol. Health Med. 2021, 26, 35–43. [Google Scholar] [CrossRef]
- Sanchez, M.C. Creating Access Individuals with Disabilities who are Experiencing Homelessness. Captone Projects and Master’s Theses. 2019. Available online: https://digitalcommons.csumb/edu/caps_thes_all/515 (accessed on 6 January 2022).
- Petrovich, J.C.; Roark Murphy, E.; Hardin, L.K.; Koch, B.R. Creating safe spaces: Designing day shelters for people experiencing homelessness. J. Soc. Distress Homeless 2017, 26, 65–72. [Google Scholar] [CrossRef]
- Ballard, A.M.; Hoover, A.T.; Rodriguez, A.V.; Caruso, B.A. Emphasizing choice and autonomy in personal hygiene, menstrual health, and sexual health product distribution to people experiencing homelessness in Atlanta, Georgia during COVID-19. Health Promot. Pract. 2021, 22, 764–766. [Google Scholar] [CrossRef] [PubMed]
- Moffa, M.; Cronk, R.; Fejfar, D.; Dancausse, S.; Padilla, L.A.; Bartram, J. A systematic scoping review of environmental health conditions and hygiene behaviors in homeless shelters. Int. J. Hyg. Environ. Health 2019, 222, 335–346. [Google Scholar] [CrossRef] [PubMed]
- Pleace, N.; Baptista, I.; Benjaminsen, L.; Busch-Geertsema, V.; O’Sullivan, E.; Teller, N. European Homelessness and COVID 19; FEANSTA: York, UK, 2021. [Google Scholar]
- Stephenson, J. National Academies Report Advises on Allocation Priorities for a COVID-19 Vaccine. JAMA Health Forum 2020, 1, e201288. [Google Scholar] [CrossRef]
- Buechler, C.R.; Ukani, A.; Elsharawi, R.; Gable, J.; Petersen, A.; Franklin, M.; Chung, R.; Bell, J.; Manly, A.; Hefzi, N.; et al. Barriers, beliefs, and practices regarding hygiene and vaccination among the homeless during a hepatitis A outbreak in Detroit, MI. Heliyon 2020, 6, e03474. [Google Scholar] [CrossRef] [PubMed]
- Story, A.; Aldridge, R.W.; Gray, T.; Burridge, S.; Hayward, A.C. Influenza vaccination, inverse care and homelessness: Cross-sectional survey of eligibility and uptake during the 2011/12 season in London. BMC Public Health 2014, 14, 44. [Google Scholar] [CrossRef] [Green Version]
- Nowalk, M.P.; Zimmerman, R.K.; Shen, S.; Jewell, I.K.; Raymund, M. Barriers to Pneumococcal and Influenza Vaccination in Older Community-Dwelling Adults (2000–2001). J. Am. Geriatr. Soc. 2004, 52, 25–30. [Google Scholar] [CrossRef]
- Doroshenko, A.; Hatchette, J.; Halperin, S.A.; MacDonald, N.E.; Graham, J.E. Challenges to immunization: The experiences of homeless youth. BMC Public Health 2012, 12, 338. [Google Scholar] [CrossRef] [Green Version]
- Buccieri, K.; Gaetz, S. Ethical Vaccine Distribution Planning for Pandemic Influenza: Prioritizing Homeless and Hard-to-Reach Populations. Public Health Ethics 2013, 6, 185–196. [Google Scholar] [CrossRef]
- Metcalfe, S.E.; Sexton, E.H. An Academic-Community Partnership to Address the Flu Vaccination Rates of the Homeless. Public Health Nurs. 2014, 31, 175–182. [Google Scholar] [CrossRef]
- Bowen, E.A.; Lahey, J.; Rhoades, H.; Henwood, B.F. Food Insecurity Among Formerly Homeless Individuals Living in Permanent Supportive Housing. Am. J. Public Health 2019, 109, 614–617. [Google Scholar] [CrossRef]
- Crawford, B.; Yamazaki, R.; Franke, E.; Amanatidis, S.; Ravulo, J.; Steinbeck, K.; Ritchie, J.; Torvaldsen, S. Sustaining dignity? Food insecurity in homeless young people in urban Australia. Health Promot. J. Aust. 2014, 25, 71–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dachner, N.; Tarasuk, V. Homeless “squeegee kids”: Food insecurity and daily survival. Soc. Sci. Med. 2002, 54, 1039–1049. [Google Scholar] [CrossRef]
- Prayogo, E.; Chater, A.; Chapman, S.; Barker, M.; Rahmawati, N.; Waterfall, T.; Grimble, G. Who uses foodbanks and why? Exploring the impact of financial strain and adverse life events on food insecurity. J. Public Health 2018, 40, 676–683. [Google Scholar] [CrossRef] [PubMed]
- Tong, M.; Tieu, L.; Lee, C.T.; Ponath, C.; Guzman, D.; Kushel, M. Factors associated with food insecurity among older homeless adults: Results from the HOPE HOME study. J. Public Health 2019, 41, 240–249. [Google Scholar] [CrossRef]
- Fitzpatrick, K.M.; Harris, C.; Drawve, G.; Willis, D.E. Assessing Food Insecurity among US Adults during the COVID-19 Pandemic. J. Hunger. Environ. Nutr. 2021, 16, 1–18. [Google Scholar] [CrossRef]
- Loopstra, R. Vulnerability to Food Insecurity since the COVID-19 Lockdown; The Food Foundation: London, UK, 2020. [Google Scholar]
- Morales, D.X.; Morales, S.A.; Beltran, T.F. Racial/Ethnic Disparities in Household Food Insecurity During the COVID-19 Pandemic: A Nationally Representative Study. J. Racial Ethn. Health Disparities 2021, 8, 1300–1314. [Google Scholar] [CrossRef]
- Ranta, R.; Mulrooney, H. Pandemics, food (in) security, and leaving the EU: What does the COVID-19 pandemic tell us about food insecurity and Brexit. Soc. Sci. Humanit. Open 2021, 3, 100125. [Google Scholar] [CrossRef]
- Lakhani, N. ‘A Perfect Storm’: US Facing Hunger Crisis as Demand for Food Banks Soars; The Gaurdian: London, UK, 2020. [Google Scholar]
- Leddy, A.M.; Weiser, S.D.; Palar, K.; Seligman, H. A conceptual model for understanding the rapid COVID-19–related increase in food insecurity and its impact on health and healthcare. Am. J. Clin. Nutr. 2020, 112, 1162–1169. [Google Scholar] [CrossRef]
- McPherson, C. Young People, Food Insecurity and COVID-19: A Qualitative Study in Edinburgh and London; Institute for Social Policy, Housing, Equalities Research: Edinburgh, Scotland, 2020. [Google Scholar]
- Miewald, C.; Ostry, A. A warm meal and a bed: Intersections of housing and food security in Vancouver’s Downtown Eastside. Hous. Stud. 2014, 29, 709–729. [Google Scholar] [CrossRef]
- Piquero, A.R.; Jennings, W.G.; Jemison, E.; Kaukinen, C.; Knaul, F.M. Domestic violence during the COVID-19 pandemic-Evidence from a systematic review and meta-analysis. J. Crim. Justice 2021, 74, 101806. [Google Scholar] [CrossRef]
- Boserup, B.; McKenney, M.; Elkbuli, A. Alarming trends in US domestic violence during the COVID-19 pandemic. Am. J. Emerg. Med. 2020, 38, 2753–2755. [Google Scholar] [CrossRef] [PubMed]
- Bradbury-Jones, C.; Isham, L. The pandemic paradox: The consequences of COVID-19 on domestic violence. J. Clin. Nurs. 2020, 29, 2047–2049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rauhaus, B.M.; Sibila, D.; Johnson, A.F. Addressing the Increase of Domestic Violence and Abuse During the COVID-19 Pandemic: A Need for Empathy, Care, and Social Equity in Collaborative Planning and Responses. Am. Rev. Public Adm. 2020, 50, 668–674. [Google Scholar] [CrossRef]
- Jasinski, J.L.; Wesely, J.K.; Mustaine, E.; Wright, J.D. The Experience of Violence in the Lives of Homeless Women: A Research Report; National Institute of Justice: Washington, DC, USA, 2005.
- Pittman, B.; Nelson-Dusek, S.; Gerrard, M.D.; Shelton, E. Homelessness in Minnesota: Detailed findings from the 2018 Minnesota Homeless Study; Wilder Research Center: St Paul, MN, USA, 2020; pp. 11–371. [Google Scholar]
- Bassuk, E.L.; DeCandia, C.J.; Beach, C.A.; Berman, F. America’s Youngest Outcasts: A Report Card on Child Homelessness; National Center on Family Homelessness: Waltham, MA, USA, 2014. [Google Scholar]
- Bretherton, J.; Mayock, P. Women’s Homelessness: European Evidence Review; FEANSTA: Brussels, Belgium, 2021. [Google Scholar]

{kind=link}
| Country | Study Design | ||
|---|---|---|---|
| U.S. | 51 | Cross-sectional | 30 |
| U.K. | 9 | Unspecified * | 7 |
| France | 9 | Longitudinal | 4 |
| Canada | 6 | Mixed methods | 4 |
| Spain | 5 | Pilot | 4 |
| Italy | 4 | Case study | 4 |
| Germany | 4 | Qualitative | 3 |
| Denmark | 2 | Report | 3 |
| Belgium | 2 | Case report | 2 |
| Multiple | 2 | Case series | 2 |
| Slovakia | 1 | Retrospective | 2 |
| Ireland | 1 | Cross-sectional seroprevalence | 2 |
| Primary Population of Interest | Analytical observational | 1 | |
| PEH | 74 | Community-based participatory research | 1 |
| General patient populations | 6 | Cross-sectional community-based | 1 |
| People living with HIV | 5 | Cross-sectional community-based surveillance | 1 |
| Multiple vulnerable groups | 3 | Cross-sectional multicentre cohort | 1 |
| COVID-19 patients | 3 | Cross-sectional retrospective chart review | 1 |
| Persons using drugs | 2 | Descriptive | 1 |
| U.S. Veterans | 1 | Disease prevention protocol | 1 |
| African Americans in Southern U.S. | 1 | Interrupted time series | 1 |
| Criminal justice-involved women | 1 | Longitudinal ecological | 1 |
| Publication Type | Matched-case control observational | 1 | |
| Journal article | 48 | Nationwide cross-sectional seroprevalence | 1 |
| Brief report | 8 | Nonconcurrent cohort | 1 |
| Research letter | 6 | Nonrandomised observational pre/post | 1 |
| Short communication | 4 | Nonrandomised pre/post | 1 |
| Case study | 4 | Observational retrospective | 1 |
| Preprint | 4 | Point prevalence | 1 |
| Report | 4 | Population-based prospective | 1 |
| Letter to the editor | 3 | Population-based retrospective e-cohort | 1 |
| Research note | 2 | Pragmatic randomised controlled trial | 1 |
| Weekly report | 2 | Prospective | 1 |
| Notes from the field | 2 | Qualitative exploratory | 1 |
| Rapid communication | 1 | Quality improvement program | 1 |
| Practice full report | 1 | Rapid case study | 1 |
| Case report | 1 | Repeated cross-sectional | 1 |
| Brief research report | 1 | Retrospective chart audit | 1 |
| Concise communication | 1 | Retrospective cohort | 1 |
| Short report | 1 | Retrospective cross-sectional | 1 |
| Research brief | 1 | Retrospective serological | 1 |
| Review | 1 | ||
| Briefing report | 1 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corey, J.; Lyons, J.; O’Carroll, A.; Stafford, R.; Ivers, J.-H. A Scoping Review of the Health Impact of the COVID-19 Pandemic on Persons Experiencing Homelessness in North America and Europe. Int. J. Environ. Res. Public Health 2022, 19, 3219. https://doi.org/10.3390/ijerph19063219
Corey J, Lyons J, O’Carroll A, Stafford R, Ivers J-H. A Scoping Review of the Health Impact of the COVID-19 Pandemic on Persons Experiencing Homelessness in North America and Europe. International Journal of Environmental Research and Public Health. 2022; 19(6):3219. https://doi.org/10.3390/ijerph19063219
Chicago/Turabian StyleCorey, Julia, James Lyons, Austin O’Carroll, Richie Stafford, and Jo-Hanna Ivers. 2022. "A Scoping Review of the Health Impact of the COVID-19 Pandemic on Persons Experiencing Homelessness in North America and Europe" International Journal of Environmental Research and Public Health 19, no. 6: 3219. https://doi.org/10.3390/ijerph19063219
APA StyleCorey, J., Lyons, J., O’Carroll, A., Stafford, R., & Ivers, J.-H. (2022). A Scoping Review of the Health Impact of the COVID-19 Pandemic on Persons Experiencing Homelessness in North America and Europe. International Journal of Environmental Research and Public Health, 19(6), 3219. https://doi.org/10.3390/ijerph19063219