
Association between Happiness and Economic Status among Older Adults in Two Myanmar Regions


 ,
,
Abstract
1. Introduction
2. Materials and Methods
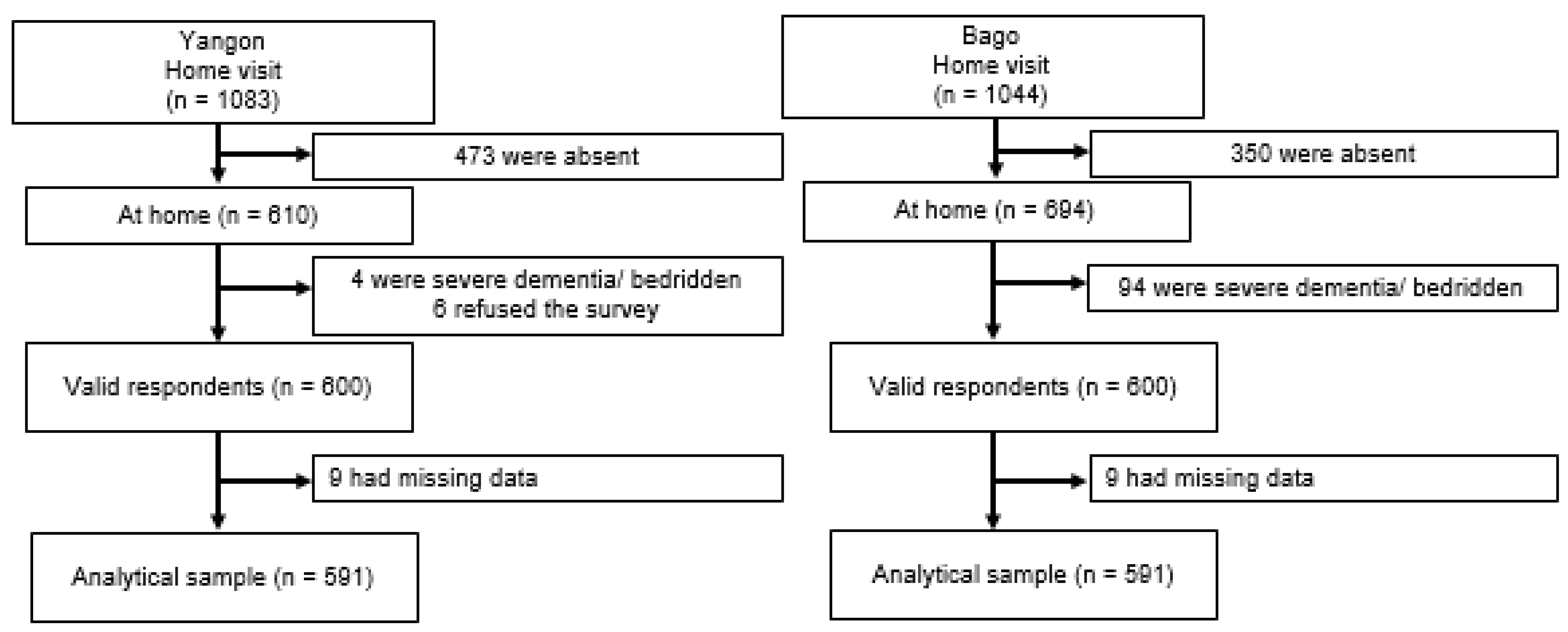
2.1. Study Design and Participants
2.2. Study Tools
2.3. Dependent Variable
2.4. Independent Variables
2.5. Confounding Variables
2.6. Statistical Analysis
3. Results
3.1. Characteristics of Happy and Unhappy Respondents
3.2. Associations between Objective/Subjective ES and Happiness
4. Discussion
5. Conclusions
6. Implications and Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Steptoe, A.; Deaton, A.; Stone, A.A. Subjective Wellbeing, Health, and Ageing. Lancet 2015, 385, 640–648. [Google Scholar] [CrossRef]
- Radermacher, W.J. Recent and Future Developments Related to “GDP and Beyond”. Rev. Income Wealth 2015, 61, 18–24. [Google Scholar] [CrossRef]
- Dolan, P.; White, M.P. How Can Measures of Subjective Well-Being Be Used to Inform Public Policy? Perspectives on Psychological Science. J. Assoc. Psychol. Sci. 2007, 2, 71–85. [Google Scholar]
- Veenhoven, R. Healthy Happiness: Effects of Happiness on Physical Health and the Consequences for Preventive Health Care. J. Happiness Stud. 2008, 9, 449–469. [Google Scholar] [CrossRef]
- Chei, C.-L.; Lee, J.M.-L.; Ma, S.; Malhotra, R. Happy Older People Live Longer. Age Ageing 2018, 47, 860–866. [Google Scholar] [CrossRef]
- Liu, B.; Floud, S.; Pirie, K.; Green, J.; Peto, R.; Beral, V. Does Happiness Itself Directly Affect Mortality? The Prospective UK Million Women Study. Lancet 2016, 387, 874–881. [Google Scholar] [CrossRef]
- Chida, Y.; Steptoe, A. Positive Psychological Well-Being and Mortality: A Quantitative Review of Prospective Observational Studies. Psychosom. Med. 2008, 70, 741–756. [Google Scholar] [CrossRef]
- Ostir, G.V.; Markides, K.S.; Black, S.A.; Goodwin, J.S. Emotional Well-Being Predicts Subsequent Functional Independence and Survival. J. Am. Geriatr. Soc. 2000, 48, 473–478. [Google Scholar] [CrossRef]
- Pressman, S.D.; Cohen, S. Does Positive Affect Influence Health? Psychol. Bull. 2005, 131, 925–971. [Google Scholar] [CrossRef]
- Koopmans, T.A.; Geleijnse, J.M.; Zitman, F.G.; Giltay, E.J. Effects of Happiness on All-Cause Mortality during 15 Years of Follow-Up: The Arnhem Elderly Study. J. Happiness Stud. 2010, 11, 113–124. [Google Scholar] [CrossRef]
- Moskowitz, J.T.; Epel, E.S.; Acree, M. Positive Affect Uniquely Predicts Lower Risk of Mortality in People with Diabetes. Health Psychol. 2008, 27, S73–S82. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, E.M.; Rogers, R.G.; Wadsworth, T. Happiness and Longevity in the United States. Soc. Sci. Med. 2015, 145, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Schiffrin, H.H.; Nelson, S.K. Stressed and Happy? Investigating the Relationship between Happiness and Perceived Stress. J. Happiness Stud. 2010, 11, 33–39. [Google Scholar] [CrossRef]
- Fredrickson, B.L. The Value of Positive Emotions: The Emerging Science of Positive Psychology Is Coming to Understand Why it’s Good to Feel Good. Am. Sci. 2003, 91, 330–335. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhou, L.; Fu, C.; Wang, Y.; Liu, Q.; Wu, H.; Zhang, R.; Zheng, L. Socio-Economic Factors Related with the Subjective Well-Being of the Rural Elderly People Living Independently in China. Int. J. Equity Health 2015, 14, 5. [Google Scholar] [CrossRef]
- Sasaki, I.; Kondo, K.; Kondo, N.; Aida, J.; Ichikawa, H.; Kusumi, T.; Sueishi, N.; Imanaka, Y. Are Pension Types Associated with Happiness in Japanese Older people?: JAGES Cross-Sectional Study. PLoS ONE 2018, 13, e0197423. [Google Scholar] [CrossRef]
- Sun, S.; Chen, J.; Johannesson, M.; Kind, P.; Burström, K. Subjective Well-Being and Its Association with Subjective Health Status, Age, Sex, Region, and Socio-Economic Characteristics in a Chinese Population Study. J. Happiness Stud. 2015, 17, 833–873. [Google Scholar] [CrossRef]
- Tran, N.L.T.; Wassmer, R.W.; Lascher, E.L. The Health Insurance and Life Satisfaction Connection. J. Happiness Stud. 2017, 18, 409–426. [Google Scholar] [CrossRef]
- Keng, S.-H.; Wu, S.-Y. Living Happily Ever after? The Effect of Taiwan’s National Health Insurance on the Happiness of the Elderly. J. Happiness Stud. 2014, 15, 783–808. [Google Scholar] [CrossRef]
- Ergin, I.; Mandiracioglu, A. Demographic and Socioeconomic Inequalities for Self-Rated Health and Happiness in Elderly: The Situation for Turkey Regarding World Values Survey between 1990 and 2013. Arch. Gerontol. Geriatr. 2015, 61, 224–230. [Google Scholar] [CrossRef]
- Kye, S.Y.; Park, K. Health-Related Determinants of Happiness in Korean Adults. Int. J. Public Health 2014, 59, 731–738. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.H.; Abdin, E.; Shahwan, S.; Zhang, Y.; Sambasivam, R.; Vaingankar, J.A.; Mahendran, R.; Chua, H.C.; Chong, S.A.; Subramaniam, M. Happiness and Cognitive Impairment among Older Adults: Investigating the Mediational Roles of Disability, Depression, Social Contact Frequency, and Loneliness. Int. J. Environ. Res. Public Health 2019, 16, 4954. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, R.; Okumiya, K.; Norboo, T.; Tsering, N.; Wada, T.; Fujisawa, M.; Imai, H.; Nose, M.; Ishimoto, Y.; Kimura, Y.; et al. Health and Happiness among Community-Dwelling Older Adults in Domkhar Valley, Ladakh, India. Geriatr. Gerontol. Int. 2017, 17, 480–486. [Google Scholar] [CrossRef]
- Yiengprugsawan, V.; Seubsman, S.-A.; Sleigh, A.C. Unhappiness and Mortality: Evidence from a Middle-Income Southeast Asian Setting. Biopsychosoc. Med. 2014, 8, 18. [Google Scholar] [CrossRef] [PubMed]
- Hsu, H.-C.; Chang, W.-C.; Chong, Y.-S.; An, J.S. Happiness and Social Determinants across Age Cohorts in Taiwan. J. Health Psychol. 2016, 21, 1828–1839. [Google Scholar] [CrossRef]
- Oshio, T.; Urakawa, K. The Association between Perceived Income Inequality and Subjective Well-Being: Evidence from a Social Survey in Japan. Soc. Indic. Res. 2014, 116, 755–770. [Google Scholar] [CrossRef]
- Tay, L.; Kuykendall, L. Promoting Happiness: The Malleability of Individual and Societal Subjective Wellbeing. Int. J. Psychol. 2013, 48, 159–176. [Google Scholar] [CrossRef]
- Read, S.; Grundy, E.; Foverskov, E. Socio-Economic Position and Subjective Health and Well-Being among Older People in Europe: A Systematic Narrative Review. Aging Ment. Health 2016, 20, 529–542. [Google Scholar] [CrossRef]
- Peiró, A. Happiness, Satisfaction and Socio-Economic Conditions: Some International Evidence. J. Socio-Econ. 2006, 35, 348–365. [Google Scholar] [CrossRef]
- Lu, L.; Kao, S.-F. Striving for Positive Aging among Chinese Older People: Effects of Life Stress and Control Beliefs in a Longitudinal Study. Int. J. Aging Hum. Dev. 2017, 86, 382–400. [Google Scholar] [CrossRef]
- Oluwafunmilade, A.A.; Rojas, B.M.; Darboe, A.; Beogo, I. Socioeconomic Differential in Self-Assessment of Health and Happiness in 5 African Countries: Finding from World Value Survey. PLoS ONE 2017, 12, e0188281. [Google Scholar] [CrossRef]
- Amorim, S.M.; França, L.H.D.F.P.; Valentini, F. Predictors of Happiness among Retired from Urban and Rural Areas in Brazil. Psicologia Reflexão Crítica 2017, 30, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Carrillo, G.; Alonso-Ferres, M.; Moya, M.; Valor-Segura, I. Socioeconomic Status and Psychological Well-Being: Revisiting the Role of Subjective Socioeconomic Status. Front. Psychol. 2020, 11, 1303. [Google Scholar] [CrossRef] [PubMed]
- Adler, N.E.; Epel, E.S.; Castellazzo, G.; Ickovics, J.R. Relationship of Subjective and Objective Social Status with Psychological and Physiological Functioning: Preliminary Data in Healthy, White Women. Health Psychol. 2000, 19, 586. [Google Scholar] [CrossRef] [PubMed]
- HelpAge International. Ageing Population in Myanmar: Trends in Ageing and Health Myanmar. Available online: https://ageingasia.org/Ageing-Population-myanmar/ (accessed on 18 August 2020).
- HelpAge International. Improving Basic Mental Health Services in Myanmar’s Primary Health Care System. 2019. Available online: http://themimu.info/sites/themimu.info/files/assessment_file_attachments/Mental_health_policy_brief_FINAL.Pdf (accessed on 17 March 2021).
- Myanmar Profile. Institute for Health Metrics and Evaluation. University of Washington. 2018. Available online: http://www.healthdata.org/Myanmar (accessed on 17 March 2021).
- Sasaki, Y.; Shobugawa, Y.; Nozaki, I.; Takagi, D.; Nagamine, Y.; Funato, M.; Chihara, Y.; Shirakura, Y.; Lwin, K.T.; Zin, P.E.; et al. Association between Depressive Symptoms and objective/Subjective Socioeconomic Status among Older Adults of Two Regions in Myanmar. PLoS ONE 2021, 16, e0245489. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y. Report of the Special Rapporteur on the Situation of Human Rights in Myanmar; UN Human Rights Commission: New York, NY, USA, 2015; p. 9. [Google Scholar]
- Health in Myanmar. Ministry of Health, The Republic of the Union of Mynmar 2014. Available online: https://themimu.info/sites/themimu.info/files/documents/Report_Health_in_Myanmar_2014_MOH.Pdf (accessed on 17 March 2021).
- Htet, A.S.; Bjertness, M.B.; Sherpa, L.Y.; Kjøllesdal, M.K.; Oo, W.M.; Meyer, H.E.; Stigum, H.; Bjertness, E. Urban-Rural Differences in the Prevalence of Non-Communicable Diseases Risk Factors among 25–74 Years Old Citizens in Yangon Region, Myanmar: A Cross Sectional Study. BMC Public Health 2016, 16, 1225. [Google Scholar] [CrossRef] [PubMed]
- Selth, A. Modern Burma Studies: A Survey of the Field. Mod. Asian Stud. 2010, 44, 401–440. [Google Scholar] [CrossRef]
- Rezaee, M.; Hedayati, A.; Naghizadeh, M.M.; Farjam, M.; Sabet, H.R.; Paknahad, M. Correlation between Happiness and Depression According to Beck Depression and Oxford Happiness Inventory among University Students. Galen Med. J. 2016, 5, 75–81. [Google Scholar] [CrossRef]
- Deng, Y.; Paul, D.R. The Relationships between Depressive Symptoms, Functional Health Status, Physical Activity, and the Availability of Recreational Facilities: A Rural-Urban Comparison in Middle-Aged and Older Chinese Adults. Int. J. Behav. Med. 2018, 25, 322–330. [Google Scholar] [CrossRef]
- World Health Organization. The WHO STEPS Surveillance Manual. 2017. Available online: https://www.who.int/ncds/surveillance/steps/STEPS_Manual.Pdf (accessed on 28 July 2020).
- Win, H.H.; Nyunt, T.W.; Lwin, K.T.; Zin, P.E.; Nozaki, I.; Bo, T.Z.; Sasaki, Y.; Takagi, D.; Nagamine, Y.; Shobugawa, Y. Cohort Profile: Healthy and Active Ageing in Myanmar (JAGES in Myanmar 2018): A Prospective Population-Based Cohort Study of the Long-Term Care Risks and Health Status of Older Adults in Myanmar. BMJ Open 2020, 10, e042877. [Google Scholar] [CrossRef]
- Japan Gerontological Evaluation Study. Available online: https://www.jages.Net/?_layoutmode=off&lang=english (accessed on 30 July 2020).
- Acquadro, C.; Conway, K.; Giroudet, C.; Mear, I. Linguistic Validation Manual for Health Outcome Assessments; Mapi Institute: Lyon, France, 2012. [Google Scholar]
- Jitapunkul, S.; Pillay, I.; Ebrahim, S. The Abbreviated Mental Test: Its Use and Validity. Age Ageing 1991, 20, 332–336. [Google Scholar] [CrossRef] [PubMed]
- MacKenzie, D.M.; Copp, P.; Shaw, R.J.; Goodwin, G.M. Brief Cognitive Screening of the Elderly: A Comparison of the Mini-Mental State Examination (MMSE), Abbreviated Mental Test (AMT) and Mental Status Questionnaire (MSQ). Psychol. Med. 1996, 26, 427–430. [Google Scholar] [CrossRef] [PubMed]
- Krueger, A.; Schkade, D. The Reliability of Subjective Well-Being Measures. Reliab. Subj. Well Being Meas. 2007, 92, 1833–1845. [Google Scholar] [CrossRef]
- Lee, Y.; Hofferth, S.L.; Flood, S.M.; Fisher, K. Reliability, Validity, and Variability of the Subjective Well-Being Questions in the 2010 American Time Use Survey. Soc. Indic. Res. 2016, 126, 1355–1373. [Google Scholar] [CrossRef][Green Version]
- Diener, E.; Wirtz, D.; Tov, W.; Kim-Prieto, C.; Choi, D.-W.; Oishi, S.; Biswas-Diener, R. New Well-Being Measures: Short Scales to Assess Flourishing and Positive and Negative Feelings. Soc. Indic. Res. 2010, 97, 143–156. [Google Scholar] [CrossRef]
- Matsubayashi, K.; Kimura, S.; Iwasaki, T.; Okumiya, K.; Hamada, T.; Fujisawa, M.; Takeuchi, K.; Kawamoto, A.; Ozawa, T. Evaluation of Subjective Happiness in the Elderly Using a Visual Analogue Scale of Happiness in Correlation with Depression Scale. Nippon Ronen Igakkai Zasshi. Jpn. J. Geriatr. 1992, 29, 811–816. [Google Scholar] [CrossRef]
- Filmer, D.; Pritchett, L.H. Estimating Wealth Effects without Expenditure data—Or Tears: An Application to Educational Enrollments in States of India. Demography 2001, 38, 115–132. [Google Scholar] [CrossRef]
- Shimai, S.; Yamamiya, Y.; Fukuda, S. Subjective Happiness among Japanese Adults: An Upward Tendency Associated with age. Nihon Koshu Eisei Zasshi 2018, 65, 553–562. [Google Scholar] [CrossRef]
- Moeini, B.; Barati, M.; Farhadian, M.; Ara, M.H. The Association between Social Support and Happiness among Elderly in Iran. Korean J. Fam. Med. 2018, 39, 260–265. [Google Scholar] [CrossRef]
- Rizvi, M.A.K.; Hossain, M.Z. Relationship between Religious Belief and Happiness: A Systematic Literature Review. J. Relig. Health 2016, 56, 1561–1582. [Google Scholar] [CrossRef]
- Myanmar Living Conditions Survey 2017: Socio-Economic Report Myanmar’s Central Statistical Organization of the Ministry of Planning, Finance and Industry, The World Bank, United Nations Development Programme. 2020. Available online: http://documents.worldbank.org/curated/en/151001580754918086/pdf/Myanmar-Living-Conditions-Survey-2017-Socio-Economic-Report.Pdf (accessed on 26 March 2021).
- Choragudi, U. Surveys Shows Inequality a Serious Problem in Myanmar. Mizzima. 2020. Available online: https://www.bnionline.net/en/news/survey-shows-inequality-serious-problem-myanmar (accessed on 15 February 2020).
- Barua, A.; Ghosh, M.K.; Kar, N.; Basilio, M.A. Prevalence of Depressive Disorders in the Elderly. Ann. Saudi Med. 2011, 31, 620–624. [Google Scholar] [CrossRef] [PubMed]
- Wada, T. Depression of Community-Dwelling Elderly in Three Asian Countries: Myanmar, Indonesia, and Japan. Kyoto Work. Pap. Area Stud. G-COE Ser. 2009, 18, 1–11. [Google Scholar]
- Williams, J.; Allen, L.; Wickramasinghe, K.; Mikkelsen, B.; Roberts, N.; Townsend, N. A Systematic Review of Associations between Non-Communicable Diseases and Socioeconomic Status within Low- and Lower-Middle-Income Countries. J. Glob. Health 2018, 8, 020409. [Google Scholar] [CrossRef] [PubMed]
- Hosseinpoor, A.R.; Bergen, N.; Mendis, S.; Harper, S.; Verdes, E.; Kunst, A.; Chatterji, S. Socioeconomic Inequality in the Prevalence of Noncommunicable Diseases in Low- and Middle-Income Countries: Results from the World Health Survey. BMC Public Health 2012, 12, 474. [Google Scholar] [CrossRef] [PubMed]
- Tang, K.L.; Rashid, R.; Godley, J.; Ghali, W.A. Association between Subjective Social Status and Cardiovascular Disease and Cardiovascular Risk Factors: A Systematic Review and Meta-Analysis. BMJ Open 2016, 6, e010137. [Google Scholar] [CrossRef]
- Adjaye-Gbewonyo, K.; Kawachi, I. Use of the Yitzhaki Index as a Test of Relative Deprivation for Health Outcomes: A Review of Recent Literature. Soc. Sci. Med. 2012, 75, 129–137. [Google Scholar] [CrossRef]
- Wilkinson, R.G. Socioeconomic Determinants of Health: Health Inequalities: Relative or Absolute Material Standards? BMJ Clin. Res. Ed. 1997, 314, 591. [Google Scholar] [CrossRef]
- Caner, A.; Yiğit, Y.C. Relative Deprivation and Its Association with Health Indicators: Lower Inequality May Not Improve Health. SSM Popul. Health 2019, 7, 100381. [Google Scholar] [CrossRef]
- Smith, H.J.; Pettigrew, T.F.; Pippin, G.M.; Bialosiewicz, S. Relative Deprivation: A Theoretical and Meta-Analytic Review. Personality and Social Psychology Review. Off. J. Soc. Personal. Soc. Psychol. Inc. 2012, 16, 203–232. [Google Scholar] [CrossRef]
- Kawachi, I.; Kennedy, B.P. Income Inequality and Health: Pathways and Mechanisms. Health Serv. Res. 1999, 34, 215–227. [Google Scholar]
- Ziersch, A.M.; Baum, F.; Darmawan, I.G.N.; Kavanagh, A.M.; Bentley, R.J. Social Capital and Health in Rural and Urban Communities in South Australia. Aust. N. Z. J. Public Health 2009, 33, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Riva, M.; Bambra, C.; Curtis, S.; Gauvin, L. Collective Resources or Local Social Inequalities? Examining the Social Determinants of Mental Health in Rural Areas. Eur. J. Public Health 2010, 21, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Sommanustweechai, A.; Putthasri, W.; Nwe, M.L.; Aung, S.T.; Theint, M.M.; Tangcharoensathien, V.; Wynn, S.S. Community Health Worker in Hard-to-Reach Rural Areas of Myanmar: Filling Primary Health Care Service Gaps. Hum. Resour. Health 2016, 14, 64. [Google Scholar] [CrossRef] [PubMed]
- Li, L.W.; Liu, J.; Xu, H.; Zhang, Z. Understanding Rural–Urban Differences in Depressive Symptoms among Older Adults in China. J. Aging Health 2016, 28, 341–362. [Google Scholar] [CrossRef]
- Ziarko, M.; Mojs, E.; Kaczmarek, L.D.; Warchol-Biedermann, K.; Malak, R.; Lisinski, P.; Samborski, W. Do Urban and Rural Residents Living in Poland Differ in Their Ways of Coping with Chronic Diseases? Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 4227–4234. [Google Scholar]
- Knodel, J. The Situation of Older Persons in Myanmar: Results from the 2012 Survey of Older Persons; HelpAge International: London, UK, 2013. [Google Scholar]
- Teerawichitchainan, B.; Knodel, J. Economic Status and Old-Age Health in Poverty-Stricken Myanmar. J. Aging Health 2015, 27, 1462–1484. [Google Scholar] [CrossRef]
- Knodel, J.; Teerawichitchainan, B. Aging in Myanmar. Gerontology 2017, 57, 599–605. [Google Scholar] [CrossRef]
- Teerawichitchainan, B.; Knodel, J. Long-Term Care Needs in the Context of Poverty and Population Aging: The Case of Older Persons in Myanmar. J. Cross Cult. Gerontol. 2018, 33, 143–162. [Google Scholar] [CrossRef]
- Spoorenberg, T. Provisional Results of the 2014 Census of Myanmar: The Surprise That wasn’t. Asian Popul. Stud. 2015, 11, 4–6. [Google Scholar] [CrossRef]
- Schnittker, J.; Baćak, V. The Increasing Predictive Validity of Self-Rated Health. PLoS ONE 2014, 9, e84933. [Google Scholar] [CrossRef]
- Latham, K.; Peek, C.W. Self-Rated Health and Morbidity Onset among Late Midlife U.S. Adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2012, 68, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Pan, A.; Sun, Q.; Okereke, O.I.; Rexrode, K.M.; Hu, F.B. Depression and Risk of Stroke Morbidity and Mortality: A Meta-Analysis and Systematic Review. JAMA 2011, 306, 1241–1249. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, Y.; Shobugawa, Y.; Nozaki, I.; Takagi, D.; Nagamine, Y.; Funato, M.; Chihara, Y.; Shirakura, Y.; Lwin, K.; Zin, P.; et al. Rural–Urban Differences in the Factors Affecting Depressive Symptoms among Older Adults of Two Regions in Myanmar. Int. J. Environ. Res. Public Health 2021, 18, 2818. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| N | Mean | ±SD | p-Value | ||
|---|---|---|---|---|---|
| Happiness score | 1200 | 6.58 | 2.01 | ||
| Objective SES | Middle/High | 718 | 6.80 | 1.88 | <0.001 |
| (wealth index) | Low | 480 | 6.24 | 2.14 | |
| Subjective SES | Average or more | 953 | 6.83 | 1.89 | <0.001 |
| (self-rated economic status) | Difficult/Very difficult | 247 | 5.62 | 2.14 | |
| Sex | Male | 483 | 6.86 | 2.00 | <0.001 |
| Female | 717 | 6.38 | 2.02 | ||
| Age | 60–69 | 670 | 6.61 | 2.00 | 0.25 |
| 70–79 | 380 | 6.61 | 2.04 | ||
| 80+ | 150 | 6.32 | 2.06 | ||
| Subjective health status | Excellent/Good | 354 | 7.10 | 1.89 | <0.001 |
| Fair/Poor | 846 | 6.36 | 2.01 | ||
| Illness during preceding year | No | 582 | 6.75 | 2.08 | <0.01 |
| Yes | 615 | 6.41 | 1.92 | ||
| Depressive symptoms | GDS < 5 | 921 | 6.89 | 1.89 | <0.001 |
| GDS ≥ 5 | 265 | 5.48 | 2.01 | ||
| Education | No school | 104 | 5.72 | 1.94 | <0.001 |
| Monastic | 292 | 6.47 | 1.98 | ||
| Some/Finished primary | 417 | 6.55 | 2.06 | ||
| Middle school or higher | 387 | 6.92 | 1.91 | ||
| Region | Yangon | 600 | 6.71 | 1.86 | <0.05 |
| Bago | 600 | 6.45 | 2.13 | ||
| Marital status | Married | 642 | 6.77 | 1.93 | <0.001 |
| Widow/Divorced/Never | 558 | 6.35 | 2.07 | ||
| Living status | Alone | 68 | 6.04 | 2.45 | <0.05 |
| Not alone | 1132 | 6.61 | 1.97 | ||
| Social Support | |||||
| Receiving emotional support | No | 176 | 6.60 | 2.14 | 0.85 |
| Yes | 1024 | 6.57 | 1.98 | ||
| Providing emotional support | No | 196 | 6.54 | 2.13 | 0.78 |
| Yes | 1004 | 6.58 | 1.98 | ||
| Receiving instrumental support | No | 27 | 6.11 | 2.24 | 0.22 |
| Yes | 1173 | 6.59 | 2.00 | ||
| Providing instrumental support | No | 268 | 6.57 | 2.15 | 0.98 |
| Yes | 932 | 6.58 | 1.96 | ||
| Religion | Buddhism | 1147 | 6.57 | 1.99 | 0.47 |
| Other | 53 | 6.77 | 2.32 | ||
| Frequency of religious visits | Less than once per week | 617 | 6.40 | 1.99 | <0.05 |
| Once per week or more | 583 | 6.76 | 2.01 |
| Happiness | OR | SE | 95%CI | p-Value | AOR | SE | 95%CI | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yangon & Bago | n = 1198 | n = 1182 | ||||||||||
| Objective ES | Middle/High | 1.00 | 1.00 | |||||||||
| (wealth index) | Low | 0.74 | 0.08 | 0.59 | 0.92 | 0.01 | 0.69 | 0.10 | 0.52 | 0.91 | 0.01 | |
| Subjective ES | Average or more | 1.00 | 1.00 | |||||||||
| (self-rated ES) | Difficult/Very difficult | 0.33 | 0.48 | 0.25 | 0.44 | 0.00 | 0.46 | 0.07 | 0.35 | 0.62 | 0.00 | |
| Pseudo = 0.0191 | Pseudo = 0.0459 | |||||||||||
| n = 591 (Yangon) | n = 599 | n = 591 | ||||||||||
| Objective ES | Middle/High | 1.00 | 1.00 | |||||||||
| (wealth index) | Low | 0.52 | 0.14 | 0.31 | 0.87 | 0.01 | 0.54 | 0.15 | 0.32 | 0.93 | 0.03 | |
| Subjective ES | Average or more | 1.00 | 1.00 | |||||||||
| (self-rated ES) | Difficult/Very difficult | 0.46 | 0.11 | 0.29 | 0.75 | 0.00 | 0.55 | 0.14 | 0.34 | 0.91 | 0.02 | |
| Pseudo = 0.0100 | Pseudo = 0.0359 | |||||||||||
| n = 591 (Bago) | n = 599 | n = 591 | ||||||||||
| Objective ES | Middle/High | 1.00 | 1.00 | |||||||||
| (wealth index) | Low | 0.76 | 0.12 | 0.55 | 1.04 | 0.08 | 0.73 | 0.12 | 0.53 | 1.01 | 0.06 | |
| Subjective ES | Average or more | 1.00 | 1.00 | |||||||||
| (self-rated ES) | Difficult/Very difficult | 0.29 | 0.05 | 0.20 | 0.41 | 0.00 | 0.43 | 0.08 | 0.30 | 0.62 | 0.00 | |
| Pseudo = 0.0191 | Pseudo = 0.0643 | |||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sasaki, Y.; Shobugawa, Y.; Nozaki, I.; Takagi, D.; Nagamine, Y.; Funato, M.; Chihara, Y.; Shirakura, Y.; Lwin, K.T.; Zin, P.E.; et al. Association between Happiness and Economic Status among Older Adults in Two Myanmar Regions. Int. J. Environ. Res. Public Health 2022, 19, 3216. https://doi.org/10.3390/ijerph19063216
Sasaki Y, Shobugawa Y, Nozaki I, Takagi D, Nagamine Y, Funato M, Chihara Y, Shirakura Y, Lwin KT, Zin PE, et al. Association between Happiness and Economic Status among Older Adults in Two Myanmar Regions. International Journal of Environmental Research and Public Health. 2022; 19(6):3216. https://doi.org/10.3390/ijerph19063216
Chicago/Turabian StyleSasaki, Yuri, Yugo Shobugawa, Ikuma Nozaki, Daisuke Takagi, Yuiko Nagamine, Masafumi Funato, Yuki Chihara, Yuki Shirakura, Kay Thi Lwin, Poe Ei Zin, and et al. 2022. "Association between Happiness and Economic Status among Older Adults in Two Myanmar Regions" International Journal of Environmental Research and Public Health 19, no. 6: 3216. https://doi.org/10.3390/ijerph19063216
APA StyleSasaki, Y., Shobugawa, Y., Nozaki, I., Takagi, D., Nagamine, Y., Funato, M., Chihara, Y., Shirakura, Y., Lwin, K. T., Zin, P. E., Bo, T. Z., Sone, T., & Win, H. H. (2022). Association between Happiness and Economic Status among Older Adults in Two Myanmar Regions. International Journal of Environmental Research and Public Health, 19(6), 3216. https://doi.org/10.3390/ijerph19063216