
Povidone-Iodine as a Pre-Procedural Mouthwash to Reduce the Salivary Viral Load of SARS-CoV-2: A Systematic Review of Randomized Controlled Trials

 ,
,  , ,
, ,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol
2.2. Focused Question
“In patients diagnosed with COVID-19 (P), does the use of PVP-I mouthwashes (I) compared to not prescribing them (C) reduce the viral load present in saliva (O)?”
2.3. Eligibility Criteria
2.3.1. Inclusion Criteria
2.3.2. Exclusion Criteria
2.4. Information Sources and Search Strategy
2.5. Study Records
2.6. Risk of Bias Assessment
3. Results
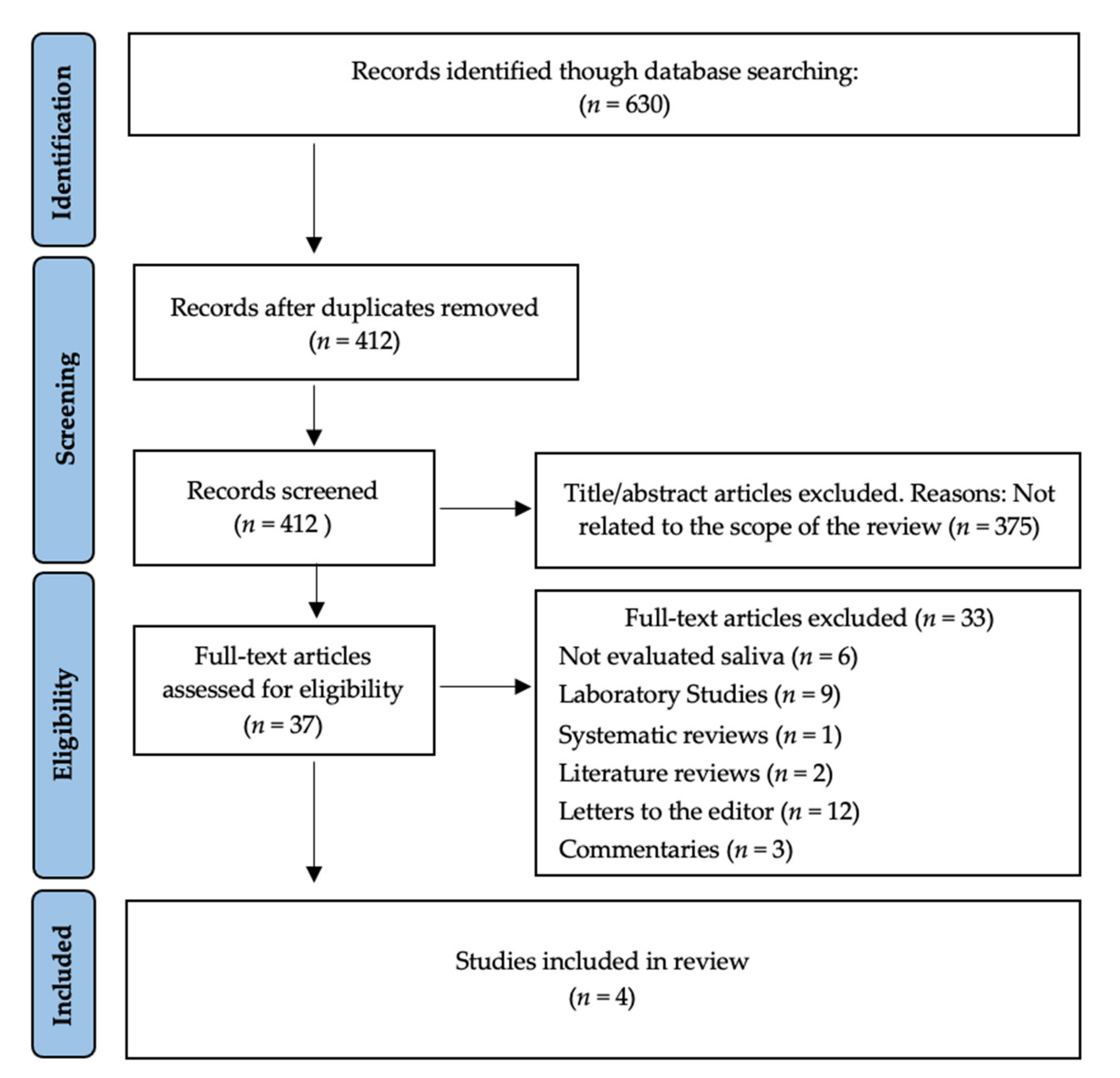
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk Bias Assessment
4. Discussion
4.1. Strengths and Limitations
4.2. Recommendations for Further Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Tellier, R. Aerosol Transmission of Influenza A Virus: A Review of New Studies. J. R. Soc. Interface 2009, 6, 783–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef] [PubMed]
- Jackson, T.; Deibert, D.; Wyatt, G.; Durand-Moreau, Q.; Adisesh, A.; Khunti, K.; Khunti, S.; Smith, S.; Chan, X.H.S.; Ross, L.; et al. Classification of Aerosol-Generating Procedures: A Rapid Systematic Review. BMJ Open Respir. Res. 2020, 7, e000730. [Google Scholar] [CrossRef] [PubMed]
- Li, R.W.K.; Leung, K.W.C.; Sun, F.C.S.; Samaranayake, L.P. Severe Acute Respiratory Syndrome (SARS) and the GDP. Part II: Implications for GDPs. Br. Dent. J. 2004, 197, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Ayeh, S.K.; Chidambaram, V.; Karakousis, P.C. Modes of Transmission of SARS-CoV-2 and Evidence for Preventive Behavioral Interventions. BMC Infect. Dis. 2021, 21, 496. [Google Scholar] [CrossRef]
- Xu, H.; Zhong, L.; Deng, J.; Peng, J.; Dan, H.; Zeng, X.; Li, T.; Chen, Q. High Expression of ACE2 Receptor of 2019-NCoV on the Epithelial Cells of Oral Mucosa. Int. J. Oral Sci. 2020, 12, 8. [Google Scholar] [CrossRef]
- Bennett, A.M.; Fulford, M.R.; Walker, J.T.; Bradshaw, D.J.; Martin, M.V.; Marsh, P.D. Microbial Aerosols in General Dental Practice. Br. Dent. J. 2000, 189, 664–667. [Google Scholar] [CrossRef]
- Liu, Y.; Ning, Z.; Chen, Y.; Guo, M.; Liu, Y.; Gali, N.K.; Sun, L.; Duan, Y.; Cai, J.; Westerdahl, D.; et al. Aerodynamic Analysis of SARS-CoV-2 in Two Wuhan Hospitals. Nature 2020, 582, 557–560. [Google Scholar] [CrossRef]
- Vergara-Buenaventura, A.; Castro-Ruiz, C. Use of Mouthwashes against COVID-19 in Dentistry. Br. J. Oral Maxillofac. Surg. 2020, 58, 924–927. [Google Scholar] [CrossRef]
- To, K.K.-W.; Tsang, O.T.-Y.; Leung, W.-S.; Tam, A.R.; Wu, T.-C.; Lung, D.C.; Yip, C.C.-Y.; Cai, J.-P.; Chan, J.M.-C.; Chik, T.S.-H.; et al. Temporal Profiles of Viral Load in Posterior Oropharyngeal Saliva Samples and Serum Antibody Responses during Infection by SARS-CoV-2: An Observational Cohort Study. Lancet Infect. Dis. 2020, 20, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Van der Valk, J.P.M.; in ’t Veen, J.C.C.M. SARS-Cov-2: The Relevance and Prevention of Aerosol Transmission. J. Occup. Environ. Med. 2021, 63, e395–e401. [Google Scholar] [CrossRef] [PubMed]
- Carrouel, F.; Conte, M.P.; Fisher, J.; Gonçalves, L.S.; Dussart, C.; Llodra, J.C.; Bourgeois, D. COVID-19: A Recommendation to Examine the Effect of Mouthrinses with β-Cyclodextrin Combined with Citrox in Preventing Infection and Progression. J. Clin. Med. 2020, 9, 1126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marui, V.C.; Souto, M.L.S.; Rovai, E.S.; Romito, G.A.; Chambrone, L.; Pannuti, C.M. Efficacy of Preprocedural Mouthrinses in the Reduction of Microorganisms in Aerosol. J. Am. Dent. Assoc. 2019, 150, 1015–1026.e1. [Google Scholar] [CrossRef] [PubMed]
- Guenezan, J.; Garcia, M.; Strasters, D.; Jousselin, C.; Lévêque, N.; Frasca, D.; Mimoz, O. Povidone Iodine Mouthwash, Gargle, and Nasal Spray to Reduce Nasopharyngeal Viral Load in Patients With COVID-19. JAMA Otolaryngol.–Head Neck Surg. 2021, 147, 400. [Google Scholar] [CrossRef]
- Rodríguez-Casanovas, H.J.; de la Rosa, M.; Bello-Lemus, Y.; Rasperini, G.; Acosta-Hoyos, A.J. Virucidal Activity of Different Mouthwashes Using a Novel Biochemical Assay. Healthcare 2021, 10, 63. [Google Scholar] [CrossRef]
- Chen, S.; Chen, J.W.; Guo, B.; Xu, C.C. Preoperative Antisepsis with Chlorhexidine Versus Povidone-Iodine for the Prevention of Surgical Site Infection: A Systematic Review and Meta-Analysis. World J. Surg. 2020, 44, 1412–1424. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- The Joanna Briggs Institute Checklist for Randomized Controlled Trials. Available online: http://joannabriggs.org/research/critical-appraisal-tools.html (accessed on 3 January 2022).
- Ferrer, M.D.; Barrueco, Á.S.; Martinez-Beneyto, Y.; Mateos-Moreno, M.V.; Ausina-Márquez, V.; García-Vázquez, E.; Puche-Torres, M.; Giner, M.J.F.; González, A.C.; Coello, J.M.S.; et al. Clinical Evaluation of Antiseptic Mouth Rinses to Reduce Salivary Load of SARS-CoV-2. Sci. Rep. 2021, 11, 24392. [Google Scholar] [CrossRef]
- Seneviratne, C.J.; Balan, P.; Ko, K.K.K.; Udawatte, N.S.; Lai, D.; Ng, D.H.L.; Venkatachalam, I.; Lim, K.S.; Ling, M.L.; Oon, L.; et al. Efficacy of Commercial Mouth-Rinses on SARS-CoV-2 Viral Load in Saliva: Randomized Control Trial in Singapore. Infection 2021, 49, 305–311. [Google Scholar] [CrossRef]
- Elzein, R.; Abdel-Sater, F.; Fakhreddine, S.; Hanna, P.A.; Feghali, R.; Hamad, H.; Ayoub, F. In Vivo Evaluation of the Virucidal Efficacy of Chlorhexidine and Povidone-Iodine Mouthwashes against Salivary SARS-CoV-2. A Randomized-Controlled Clinical Trial. J. Evid.-Based Dent. Pract. 2021, 21, 101584. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, P.; Melkonyan, A.; Meethil, A.; Saraswat, S.; Hall, D.L.; Cottle, J.; Wenzel, M.; Ayouty, N.; Bense, S.; Casanova, F.; et al. Estimating Salivary Carriage of Severe Acute Respiratory Syndrome Coronavirus 2 in Nonsymptomatic People and Efficacy of Mouthrinse in Reducing Viral Load: A Randomized Controlled Trial. J. Am. Dent. Assoc. 2021, 152, 903–908. [Google Scholar] [CrossRef] [PubMed]
- Letko, M.; Marzi, A.; Munster, V. Functional Assessment of Cell Entry and Receptor Usage for SARS-CoV-2 and Other Lineage B Betacoronaviruses. Nat. Microbiol. 2020, 5, 562–569. [Google Scholar] [CrossRef] [Green Version]
- Carrouel, F.; Gonçalves, L.S.; Conte, M.P.; Campus, G.; Fisher, J.; Fraticelli, L.; Gadea-Deschamps, E.; Ottolenghi, L.; Bourgeois, D. Antiviral Activity of Reagents in Mouth Rinses against SARS-CoV-2. J. Dent. Res. 2021, 100, 124–132. [Google Scholar] [CrossRef]
- Cavalcante-Leão, B.L.; de Araujo, C.; Basso, I.; Schroder, A.; Guariza-Filho, O.; Ravazzi, G.; Gonçalves, F.; Zeigelboim, B.; Santos, R.; Stechman-Neto, J. Is There Scientific Evidence of the Mouthwashes Effectiveness in Reducing Viral Load in Covid-19? A Systematic Review. J. Clin. Exp. Dent. 2021, 13, e179–e189. [Google Scholar] [CrossRef]
- Trougakos, I.P.; Stamatelopoulos, K.; Terpos, E.; Tsitsilonis, O.E.; Aivalioti, E.; Paraskevis, D.; Kastritis, E.; Pavlakis, G.N.; Dimopoulos, M.A. Insights to SARS-CoV-2 Life Cycle, Pathophysiology, and Rationalized Treatments That Target COVID-19 Clinical Complications. J. Biomed. Sci. 2021, 28, 9. [Google Scholar] [CrossRef]
- Huang, N.; Pérez, P.; Kato, T.; Mikami, Y.; Okuda, K.; Gilmore, R.C.; Conde, C.D.; Gasmi, B.; Stein, S.; Beach, M.; et al. SARS-CoV-2 Infection of the Oral Cavity and Saliva. Nat. Med. 2021, 27, 892–903. [Google Scholar] [CrossRef]
- Xu, C.; Wang, A.; Hoskin, E.R.; Cugini, C.; Markowitz, K.; Chang, T.L.; Fine, D.H. Differential Effects of Antiseptic Mouth Rinses on SARS-CoV-2 Infectivity In Vitro. Pathogens 2021, 10, 272. [Google Scholar] [CrossRef] [PubMed]
- Hassandarvish, P.; Tiong, V.; Mohamed, N.A.; Arumugam, H.; Ananthanarayanan, A.; Qasuri, M.; Hadjiat, Y.; Abubakar, S. In Vitro Virucidal Activity of Povidone Iodine Gargle and Mouthwash against SARS-CoV-2: Implications for Dental Practice. Br. Dent. J. 2020. [Google Scholar] [CrossRef]
- Bidra, A.S.; Pelletier, J.S.; Westover, J.B.; Frank, S.; Brown, S.M.; Tessema, B. Comparison of In Vitro Inactivation of SARS CoV-2 with Hydrogen Peroxide and Povidone-Iodine Oral Antiseptic Rinses. J. Prosthodont. 2020, 29, 599–603. [Google Scholar] [CrossRef] [PubMed]
- Anderson, D.E.; Sivalingam, V.; Kang, A.E.Z.; Ananthanarayanan, A.; Arumugam, H.; Jenkins, T.M.; Hadjiat, Y.; Eggers, M. Povidone-Iodine Demonstrates Rapid In Vitro Virucidal Activity Against SARS-CoV-2, The Virus Causing COVID-19 Disease. Infect. Dis. Ther. 2020, 9, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Pelletier, J.S.; Tessema, B.; Frank, S.; Westover, J.B.; Brown, S.M.; Capriotti, J.A. Efficacy of Povidone-Iodine Nasal and Oral Antiseptic Preparations Against Severe Acute Respiratory Syndrome-Coronavirus 2 (SARS-CoV-2). Ear Nose Throat J. 2021, 100, 192S–196S. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; Grover, V.; Singh, C.; Sharma, A.; Das, D.K.; Singh, P.; Thakur, K.G.; Ringe, R.P. Chlorhexidine: An Effective Anticovid Mouth Rinse. J. Indian Soc. Periodontol. 2021, 25, 86–88. [Google Scholar] [CrossRef] [PubMed]
- Frank, S.; Brown, S.M.; Capriotti, J.A.; Westover, J.B.; Pelletier, J.S.; Tessema, B. In Vitro Efficacy of a Povidone-Iodine Nasal Antiseptic for Rapid Inactivation of SARS-CoV-2. JAMA Otolaryngol.–Head Neck Surg. 2020, 146, 1054. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, M.; Yokoe, D.S.; Havlir, D.V. Asymptomatic Transmission, the Achilles’ Heel of Current Strategies to Control Covid-19. N. Engl. J. Med. 2020, 382, 2158–2160. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Author/Year | Sample Size | Time of Testing | Intervention/Duration of Rinses | Conclusions | |
|---|---|---|---|---|---|
| Control Group | Test Group(s) | ||||
| Chaudhary et al. [23] (2021) | 40 | Saliva samples for RT-PCR 1 were collected at 15 and 45 min 2 post-rinse. | Placebo (normal saline), 1%/ 60 s 3 | 1% HP 4, 0.12% CHX 5, 0.50% PVP-I 6.Rinsed with 15 mL 7/for 60 s. | All 4 mouthwashes reduced the salivary load by 61% through 89% at 15 min and by 70% through 97% at 45 min. |
| Elzein et al. [22] (2021) | 61 | Saliva was evaluated with RT-PCR at baseline and 5 min after rinsing. | Placebo (distilled water)/ 30 s. | 1% PVP-I and 0.20% CHX/30 s. | The Ct 8 of the intervention groups (CHX 0.20% and 1% PVP-I) was significantly different compared to the control group. |
| Ferrer et al. [20] (2021) | 84 | RT-PCR at baseline, 30, 60, and 120 min after mouth rinse | Placebo (distilled water)/ 1 min. | 2% PVP-I, 1% HP, 0.07% CPC 9, 0.12% CHX/1 min. | None of the mouthwashes evaluated presented a statistically significant change in the salivary viral load. |
| Seneviratne et al. [21] (2020) | 36 | Saliva samples for RT-PCR at baseline (pre-rinse), 5 min, and 3 and 6 h 10 post-rinsing. | Placebo (water)/ 30 s. | 0.5% PVP-I, 0.20% CHX, 0.075% CPC/30 s. | There were no differences in the reduction of salivary load in all intervention groups. When compared with the control group, PVP-I and CPC showed a significant decrease at 6 h. CPC also showed a significant reduction at 5 min. |
| Critical Appraisal Questions | Chaudhary et al. [23] (2021) | Seneviratne et al. [21] (2020) | Elzein et al. [22] (2021) | Ferrer et al. [20] (2021) |
|---|---|---|---|---|
|  | | | |
| | | | |
| |  | | |
| |  | | |
| | | | |
| | | | |
| | | | |
| | | | |
| | | | |
| | | | |
| | | | |
| | | | |
| | | | |
= yes, = no, = uncertain.Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcia-Sanchez, A.; Peña-Cardelles, J.-F.; Ordonez-Fernandez, E.; Montero-Alonso, M.; Kewalramani, N.; Salgado-Peralvo, A.-O.; Végh, D.; Gargano, A.; Parra, G.; Guerra-Guajardo, L.-I.; et al. Povidone-Iodine as a Pre-Procedural Mouthwash to Reduce the Salivary Viral Load of SARS-CoV-2: A Systematic Review of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2022, 19, 2877. https://doi.org/10.3390/ijerph19052877
Garcia-Sanchez A, Peña-Cardelles J-F, Ordonez-Fernandez E, Montero-Alonso M, Kewalramani N, Salgado-Peralvo A-O, Végh D, Gargano A, Parra G, Guerra-Guajardo L-I, et al. Povidone-Iodine as a Pre-Procedural Mouthwash to Reduce the Salivary Viral Load of SARS-CoV-2: A Systematic Review of Randomized Controlled Trials. International Journal of Environmental Research and Public Health. 2022; 19(5):2877. https://doi.org/10.3390/ijerph19052877
Chicago/Turabian StyleGarcia-Sanchez, Alvaro, Juan-Francisco Peña-Cardelles, Esther Ordonez-Fernandez, María Montero-Alonso, Naresh Kewalramani, Angel-Orión Salgado-Peralvo, Dániel Végh, Angélica Gargano, Gabriela Parra, Lourdes-Isabela Guerra-Guajardo, and et al. 2022. "Povidone-Iodine as a Pre-Procedural Mouthwash to Reduce the Salivary Viral Load of SARS-CoV-2: A Systematic Review of Randomized Controlled Trials" International Journal of Environmental Research and Public Health 19, no. 5: 2877. https://doi.org/10.3390/ijerph19052877
APA StyleGarcia-Sanchez, A., Peña-Cardelles, J.-F., Ordonez-Fernandez, E., Montero-Alonso, M., Kewalramani, N., Salgado-Peralvo, A.-O., Végh, D., Gargano, A., Parra, G., Guerra-Guajardo, L.-I., & Kozuma, W. (2022). Povidone-Iodine as a Pre-Procedural Mouthwash to Reduce the Salivary Viral Load of SARS-CoV-2: A Systematic Review of Randomized Controlled Trials. International Journal of Environmental Research and Public Health, 19(5), 2877. https://doi.org/10.3390/ijerph19052877