
Patient with Phenylketonuria and Intellectual Disability—Problem Not Always Caused Exclusively by Insufficient Metabolic Control (Coexistence of PKU and Alazami Syndrome)

 , ,
, , 
{kind=link}
{kind=link}
Abstract
:1. Introduction
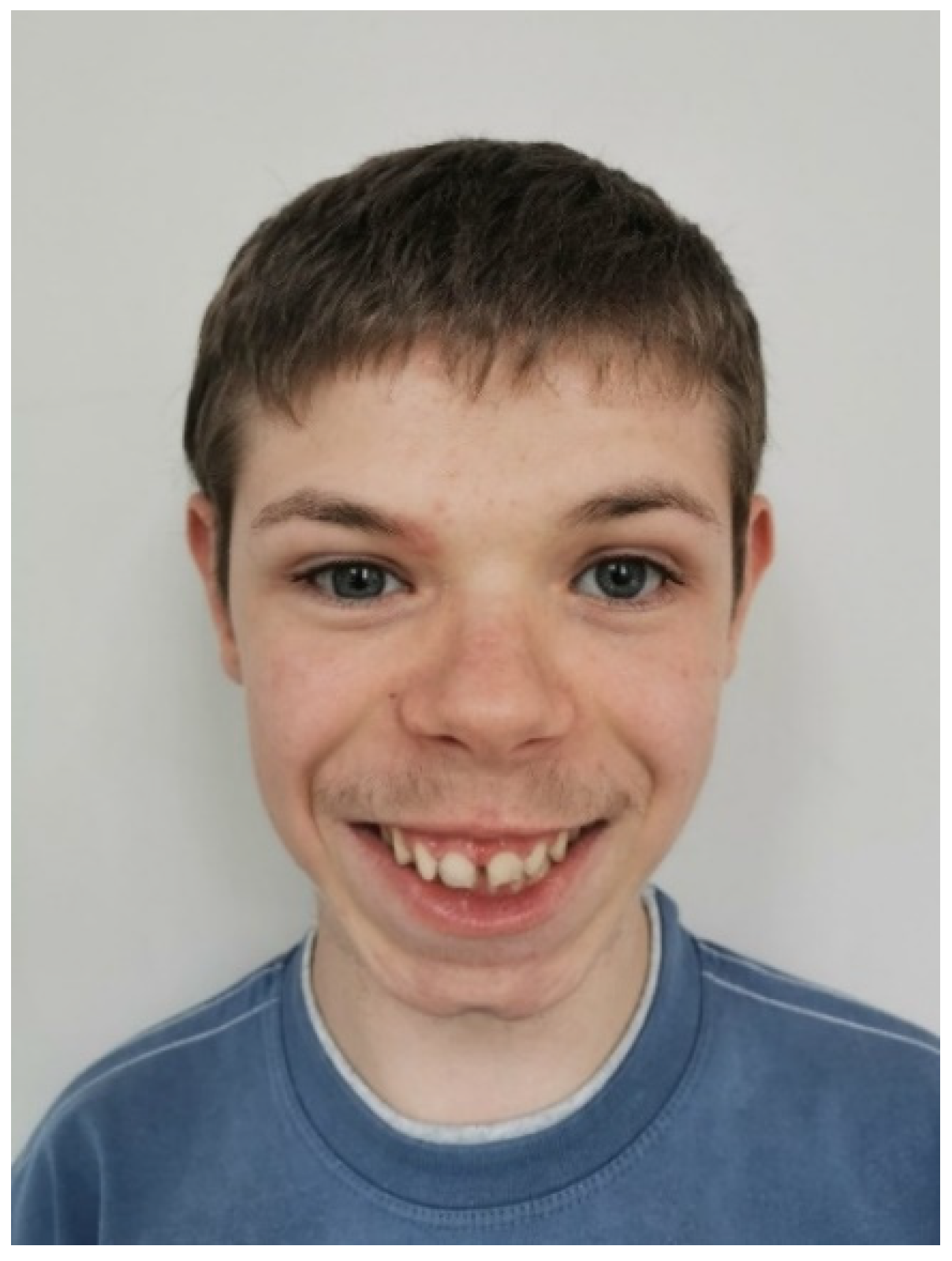
2. A Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Hillert, A.; Anikster, Y.; Belanger-Quintana, A.; Burlina, A.; Burton, B.K.; Carducci, C.; Chiesa, A.E.; Christodoulou, J.; Đorđević, M.; Desviat, L.R.; et al. The Genetic Landscape and Epidemiology of Phenylketonuria. Am. J. Hum. Genet. 2020, 107, 234–250. [Google Scholar] [CrossRef]
- Van Wegberg, A.M.J.; Macdonald, A.; Ahring, K.; BéLanger-Quintana, A.; Blau, N.; Bosch, A.M.; Burlina, A.; Campistol, J.; Feillet, F.; Giżewska, M.; et al. The complete European guidelines on phenylketonuria: Diagnosis and treatment. Orphanet J. Rare Dis. 2017, 12, 162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wesonga, E.; Shimony, J.S.; Rutlin, J.; Grange, R.K.; White, D.A. Relationship between age and white matter integrity in children with phenylketonuria. Mol. Genet. Metab. Rep. 2016, 7, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Szajewska, H.; Horvath, A. Żywienie i Leczenie Żywieniowe Dzieci i Młodzieży, 1st ed.; Medycyna Praktyczna: Kraków, Poland, 2017; pp. 279–281. [Google Scholar]
- Dateki, S.; Kitajima, T.; Kihara, T.; Watanabe, S.; Yoshiura, K.-I.; Moriuchi, H. Novel compound heterozygous variants in the LARP7 gene in a patient with Alazami syndrome. Hum. Genome Var. 2018, 5, 18014. [Google Scholar] [CrossRef] [PubMed]
- Alazami, A.M.; Al-Owain, M.; Alzahrani, F.; Shuaib, T.; Al-Shamrani, H.; Al-Falki, Y.H.; Al-Qahtani, S.M.; Alsheddi, T.; Colak, D.; Alkuraya, F.S. Loss of function mutation in LARP7, chaperone of 7SK ncRNA, causes a syndrome of facial dysmorphism, intellectual disability, and primordial dwarfism. Hum. Mutat. 2012, 33, 1429–1434. [Google Scholar] [CrossRef] [PubMed]
- Gana, S.; Plumari, M.; Rossi, E.; Saracino, A.; Iorio, M.; Zanaboni, M.P.; Orcesi, S.; Valente, E.M. Alazami syndrome: Phenotypic expansion and clinical resemblance to Smith–Lemli–Opitz syndrome. Am. J. Med. Genet. Part A 2020, 182, 2722–2726. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Kong, R.; Zhu, J.; Sun, H.; Chang, S. Unraveling the conformational determinants of LARP7 and 7SK small nuclear RNA by theoretical approaches. Mol. Biosyst. 2016, 12, 2613–2621. [Google Scholar] [CrossRef] [PubMed]
- Wojcik, M.H.; Linnea, K.; Stoler, J.M.; Rappaport, L. Updating the neurodevelopmental profile of Alazami syndrome: Illustrating the role of developmental assessment in rare genetic disorders. Am. J. Med. Genet. Part A 2019, 179, 1565–1569. [Google Scholar] [CrossRef] [PubMed]
- Imbert-Bouteille, M.; Them, F.T.M.; Thevenon, J.; Guignard, T.; Gatinois, V.; Riviere, J.-B.; Boland, A.; Meyer, V.; Deleuze, J.-F.; Sanchez, E.; et al. LARP7 variants and further delineation of the Alazami syndrome phenotypic spectrum among primordial dwarfisms: 2 sisters. Eur. J. Med. Genet. 2019, 62, 161–166. [Google Scholar] [CrossRef]
- Das, S.; Godbole, K.; Abraham, S.S.C.; Ganesan, P.; Kamdar, P.; Danda, S. Alazami syndrome: Report of three Indian patients with phenotypic spectrum from adolescence to adulthood. Am. J. Med. Genet. Part A 2021, 185, 1606–1609. [Google Scholar] [CrossRef]
- Smith, I.; Beasley, M.G.; Ades, E.A. Intelligence and quality of dietary treatment in phenylketonuria. Arch. Dis. Child. 1990, 65, 472–478. [Google Scholar] [CrossRef]
- Christ, S.E.; Huijbregts, S.; de Sonneville, L.; White, D. Executive function in early-treated phenylketonuria: Profile and underlying mechanisms. Mol. Genet. Metab. 2010, 99, S22–S32. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, A.; Ahring, K.; Almeida, M.F.; Belanger-Quintana, A.; Blau, N.; Burlina, A.; Cleary, M.; Coskum, T.; Dokoupil, K.; Evans, S.; et al. The challenges of managing coexistent disorders with phenylketonuria: 30 cases. Mol. Genet. Metab. 2015, 116, 242–251. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patalan, M.; Leśniak, A.; Bernatowicz, K.; Romanowska, H.; Krzywińska-Zdeb, E.; Walczak, M.; Giżewska, M. Patient with Phenylketonuria and Intellectual Disability—Problem Not Always Caused Exclusively by Insufficient Metabolic Control (Coexistence of PKU and Alazami Syndrome). Int. J. Environ. Res. Public Health 2022, 19, 2574. https://doi.org/10.3390/ijerph19052574
Patalan M, Leśniak A, Bernatowicz K, Romanowska H, Krzywińska-Zdeb E, Walczak M, Giżewska M. Patient with Phenylketonuria and Intellectual Disability—Problem Not Always Caused Exclusively by Insufficient Metabolic Control (Coexistence of PKU and Alazami Syndrome). International Journal of Environmental Research and Public Health. 2022; 19(5):2574. https://doi.org/10.3390/ijerph19052574
Chicago/Turabian StylePatalan, Michał, Alicja Leśniak, Krzysztof Bernatowicz, Hanna Romanowska, Elżbieta Krzywińska-Zdeb, Mieczysław Walczak, and Maria Giżewska. 2022. "Patient with Phenylketonuria and Intellectual Disability—Problem Not Always Caused Exclusively by Insufficient Metabolic Control (Coexistence of PKU and Alazami Syndrome)" International Journal of Environmental Research and Public Health 19, no. 5: 2574. https://doi.org/10.3390/ijerph19052574
APA StylePatalan, M., Leśniak, A., Bernatowicz, K., Romanowska, H., Krzywińska-Zdeb, E., Walczak, M., & Giżewska, M. (2022). Patient with Phenylketonuria and Intellectual Disability—Problem Not Always Caused Exclusively by Insufficient Metabolic Control (Coexistence of PKU and Alazami Syndrome). International Journal of Environmental Research and Public Health, 19(5), 2574. https://doi.org/10.3390/ijerph19052574