
The Her Tribe and His Tribe Aboriginal-Designed Empowerment Programs

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Program Design
2.3. Outcome Measures
2.4. Yarning Circles
2.5. Safety and Wellbeing Protocol
2.6. Data Analysis
2.7. Ethics and Methodology
3. Results
3.1. Yarning Circles
‘We all connected as mothers or as women, but we all had the same issues and just being in a place that it’s okay to feel like that because everybody has been through that moment or felt like that before or could understand I could just talk to somebody even if it was an aunty or another women that has a young child the same age. I could just get some comfort to say, it is okay and I’m doing a good job’.(Yarning Group 3 Participant, Her Tribe)
3.2. Post Hoc Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- During the last 30 days, about how often did you feel tired out for no good reason?
- During the last 30 days, about how often did you feel nervous?
- During the last 30 days, about how often did you feel so nervous that nothing could calm you down?
- During the last 30 days, about how often did you feel hopeless?
- During the last 30 days, about how often did you feel restless or fidgety?
- During the last 30 days, about how often did you feel so restless you could not sit still?
- During the last 30 days, about how often did you feel depressed?
- During the last 30 days, about how often did you feel that everything was an effort?
- During the last 30 days, about how often did you feel so sad that nothing could cheer you up?
- During the last 30 days, about how often did you feel worthless?
References
- Australian Bureau of Statistics (ABS). Body Mass Index by Age, Indigenous Status and Sex, 2012–13—Australia. 2014. Available online: https://www.abs.gov.au/ausstats/abs@.nsf/PrimaryMainFeatures/4727.0.55.006?OpenDocument (accessed on 1 April 2021).
- Australian Bureau of Statistics (ABS). Health Risk Factors—Diet, Body Mass, Blood Pressure, Physical Activity. National Aboriginal and Torres Strait Islander Health Survey, 2018–19. 2019. Available online: https://www.abs.gov.au/statistics/people/aboriginal-and-torres-strait-islander-peoples/national-aboriginal-and-torres-strait-islander-health-survey/2018-19 (accessed on 19 October 2020).
- Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework.1.18.Social and Emotional Wellbeing. Available online: https://www.indigenoushpf.gov.au/measures/1-18-social-emotional-wellbeing (accessed on 1 April 2021).
- Bize, R.; Johnson, J.A.; Plotnikoff, R.C. Physical activity level and health-related quality of life in the general adult population: A systematic review. Prev. Med. 2007, 45, 401–415. [Google Scholar] [CrossRef] [PubMed]
- Mammen, G.; Faulkner, G. Physical activity and the prevention of depression: A systematic review of prospective studies. Am. J. Prev. Med. 2013, 45, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Spanier, P.A.; Allison, K.R. General social support and physical activity: An analysis of the Ontario Health Survey. Can. J. Public Health 2001, 92, 210–213. [Google Scholar] [CrossRef] [PubMed]
- Chekroud, S.R.; Gueorguieva, R.; Zheutlin, A.B.; Paulus, M.; Krumholz, H.M.; Krystal, J.H.; Chekroud, A.M. Association between physical exercise and mental health in 1·2 million individuals in the USA between 2011 and 2015: A cross-sectional study. Lancet Psychiatry 2018, 5, 739–746. [Google Scholar] [CrossRef]
- Schuch, F.B.; Vancampfort, D.; Firth, J.; Rosenbaum, S.; Ward, P.B.; Silva, E.S.; Hallgren, M.; De Leon, A.P.; Dunn, A.L.; Deslandes, A.C.; et al. Physical activity and incident depression: A meta-analysis of prospective cohort studies. Am. J. Psychiatry 2018, 175, 631–648. [Google Scholar] [CrossRef] [PubMed]
- Macniven, R.; Canuto, K.; Wilson, R.; Bauman, A.; Evans, J. The impact of physical activity and sport on social outcomes among Aboriginal and Torres Strait Islander people: A systematic scoping review. J. Sci. Med. Sport 2019, 22, 1232–1242. [Google Scholar] [CrossRef] [PubMed]
- Gee, G. Resilience and Recovery from Trauma among Aboriginal Help Seeking Clients in an Urban Aboriginal Community Controlled Health Organisation. Ph.D. Thesis, University of Melbourne, Melbourne, Australia, 2016. [Google Scholar]
- Usher, K.; Jackson, D.; Walker, R.; Durkin, J.; Smallwood, R.; Robinson, M.; Sampson, U.N.; Adams, I.; Porter, C.; Marriott, R. Indigenous resilience in Australia: A scoping review using a reflective decolonizing collective dialogue. Front. Public Health 2021, 9, 162. [Google Scholar] [CrossRef] [PubMed]
- Ungar, M.; Liebenberg, L. Assessing Resilience Across Cultures Using Mixed Methods: Construction of the Child and Youth Resilience Measure. J. Mix. Methods Res. 2011, 5, 126–149. [Google Scholar] [CrossRef]
- Bessarab, D.; Ng’andu, B. Yarning about yarning as a legitimate method in Indigenous research. Int. J. Crit. Indig. Stud. 2010, 3, 37–50. [Google Scholar] [CrossRef] [Green Version]
- Kessler, R.C.; Andrew, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.-L.T.; Walters, E.E.; Zaslavksy, A.M. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef] [PubMed]
- Markwick, A.; Ansari, Z.; Sullivan, M.; McNeil, J. Social determinants and psychological distress among Aboriginal and Torres Strait islander adults in the Australian state of Victoria: A cross-sectional population-based study. Soc. Sci. Med. 2015, 128, 178–187. [Google Scholar] [CrossRef]
- Leger, L.A.; Lambert, J. A maximal multistage 20m shuttle run test to predict VO2 max. Eur. J. Appl. Physiol. 1982, 49, 1–5. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows, version 22.0; Released 2013; IBM Corp: Armonk, NY, USA, 2013. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge Academic: New York, NY, USA, 1988. [Google Scholar]
- Braun, V.; Clarke, C. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Flick, U. An introduction to Qualitative Research, 4th ed.Sage: London, UK, 2009. [Google Scholar]
- Rigney, L.I. Indigenous Australians: Addressing racism in education. Dulwich Cent. Newsl. 1995, 2, 5–15. [Google Scholar]
- Rigney, L.I. A First Perspective of Indigenous Australian Participation in Science: Framing Indigenous Research towards Indigenous Australian Intellectual Sovereignty; Aboriginal Research Institute; University of South Australia: Adelaide, Australia, 2001. [Google Scholar]
- Canuto, K.; Cargo, M.; Li, M.; D’Onise, K.; Esterman, A.; McDermott, R. Pragmatic randomised trial of a 12-week exercise and nutrition program for Aboriginal and Torres Strait Islander women: Clinical results immediate post and 3 months follow-up. BMC Public Health 2012, 12, 933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thorpe, A.; Anders, W.; Rowley, K. The community network: An Aboriginal community football club bringing people together. Aust. J. Prim. Health 2014, 20, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Onemda VicHealth Koori Health Unit. We Can Like Research in Koori Hands: A Community Report on Onemda Vichealth Koori Health Unit’s Research Workshops in 2007; Onemda VicHealth Koori Health Unit., The University of Melbourne: Melbourne, Australia, 2008. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Her Tribe Program | His Tribe Program | |||||
|---|---|---|---|---|---|---|
| Week | Topic | Themes | Speaker | Topic | Themes | Speaker |
| 1 | Getting in to your groove | Team Bonding Fitness Test | Program leader | Fitness…The Black Way! | Team Bonding Fitness Testing | Aboriginal fitness promotion |
| 2 | Today’s Warriors | Resilience Motivation | Kokoda Trek Leader | Talking Nutrition | Diet and lifestyle | Nutritionist AFL Players |
| 3 | It’s Never Too Late | Determination Overcoming challenges Goal Setting | Aboriginal Ultra Marathon Runner | Tackling the Beast | Resilience Suicide prevention | Aboriginal mental health |
| 4 | Destination Arnold | Goal setting Determination Inspiration | Aboriginal Body Builder | The Premiership Race | Exercise promotion Diet | Aboriginal AFL Players |
| 5 | Eagle, Look out! | Community Building Wellbeing | No speaker | Soaring with Bunjil | Physical/mental barriers Connecting with country | No speaker |
| 6 | Receiving the Gold | Resilience Commitment | Aboriginal psychologist | You are in Control | Gambling prevention Fitness testing | Gambling prevention speaker |
| 7 | Tough Mudder Champion | Fitness testing Overcoming Challenges | Tough Mudder Competitor | Over the Hurdles | Coming togetherTeamwork | Aboriginal Psychologist |
| 8 | Women’s Circles | Peer leadership Self-Esteem | Aboriginal domestic violence survivor and educator | Receiving the Gold | Self determination | Aboriginal boxer and fitness trainer |
| 9 | Her Time–Caring for yourself | Yoga Self-Care | Aboriginal Yoga Teacher | Sporting Stars | Northcote Sporting Competition | No speaker |
| 10 | I am not the problem | Self-Determination Leadership | Aboriginal Community Leader | Your Inner Ninja * | Health and fitness choices Overcoming adversity | ‘Deadly Ninja’ success |
| 11 | Chasing Goals Balancing Family | Fitness testing Goal Setting self and family wellbeing | Aboriginal Jui-Jitsu Champion | |||
| 12 | First 1000 Days | Education Women’s Health | Aboriginal academic leader | |||
| 13 | Throwback Thursday | Northcote Sporting Competition | No speaker | |||
| 14 | Women’s Circle | Community care Relationships Connectedness | Aboriginal Woman and community champion | |||
| 15 | Breaking Ground | Trauma Resilience Culture | Aboriginal community champion | |||
| 16 | Graduation | Fitness Testing | No speaker | |||
| Her Tribe Participants (n = 86) | His Tribe Participants (n = 31) | |||
|---|---|---|---|---|
| Total | Percentage * | Total | Percentage | |
| Indigenous status/affiliation | ||||
| Aboriginal | 74 | 86.0 | 31 | 100 |
| Torres Strait Islander | 1 | 1.2 | 0 | 0 |
| Aboriginal and Torres Strait Islander | 2 | 2.3 | 0 | 0 |
| Bi-cultural heritage | 3 | 3.5 | 0 | 0 |
| Identified as Koori (clan/language group within Victoria) | 47 | 58.8 | 16 | 51.6 |
| Non-Koori (identified clan/language group outside Victoria or did not answer) | 33 | 41.3 | 15 | 48.4 |
| Age (years), Mean (SD) | 35.7 (SD 12.1) | 40.3 (SD 13.0) | ||
| Employment | ||||
| Yes | 61 | 70.9 | 23 | 74.2 |
| No | 19 | 22.1 | 8 | 25.8 |
| Financial security Enough money for basic living expenses | ||||
| Yes | 72 | 83.7 | 27 | 87.1 |
| No | 8 | 9.3 | 4 | 12.9 |
| Education ** | ||||
| Completed year 7–11 | 38 | 44.0 | 18 | 58.1 |
| Completed year 12 | 42 | 49.0 | 13 | 41.9 |
| Completed a tertiary degree | 26 | 30.0 | 9 | 29.0 |
| Outcomes | Her Tribe Pre- and Post-Program Comparisons | |||||
|---|---|---|---|---|---|---|
| Pre M (SD) | Post M (SD) | Mean Diff | 95% CI | t | Cohen’s d | |
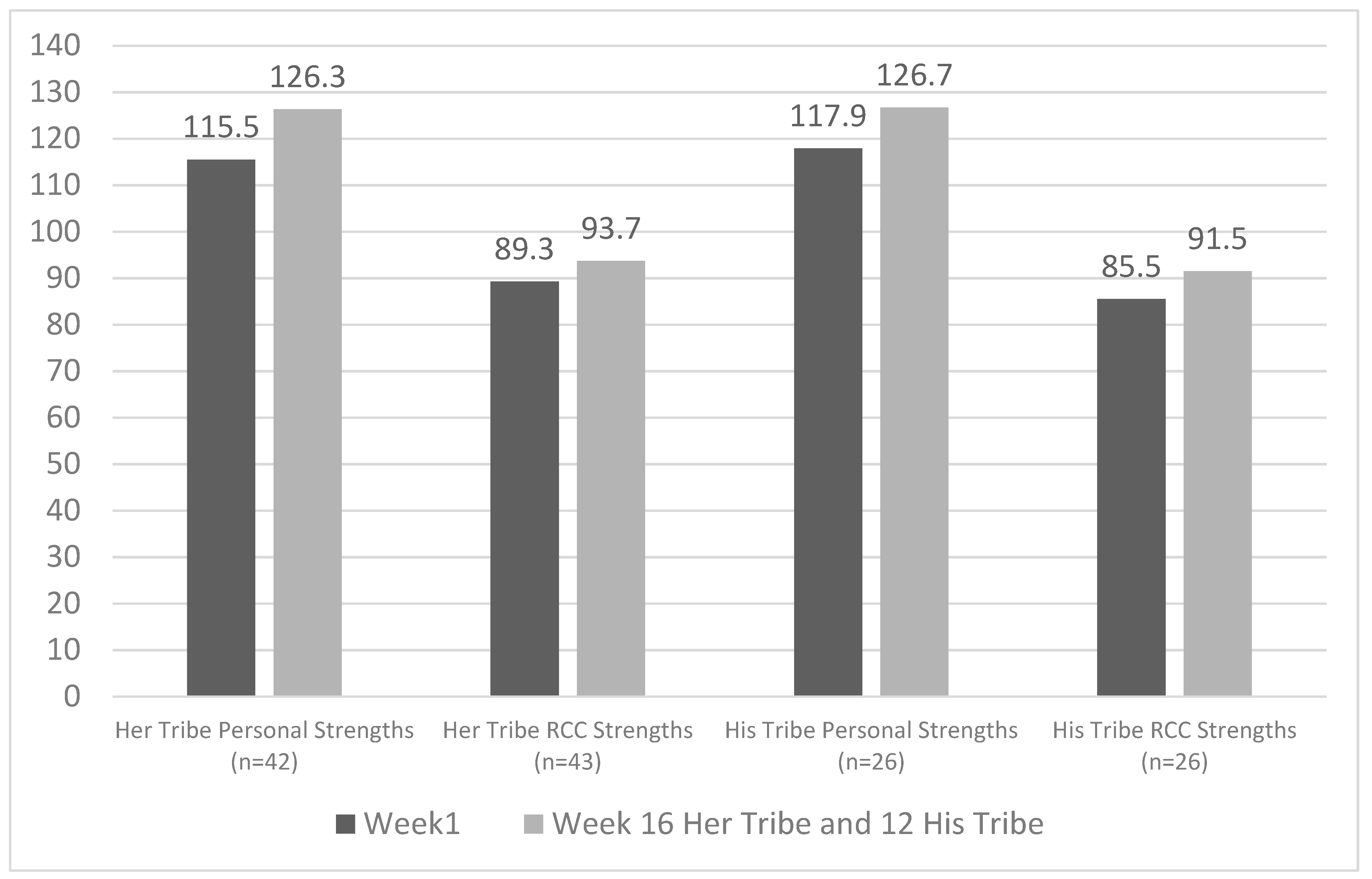
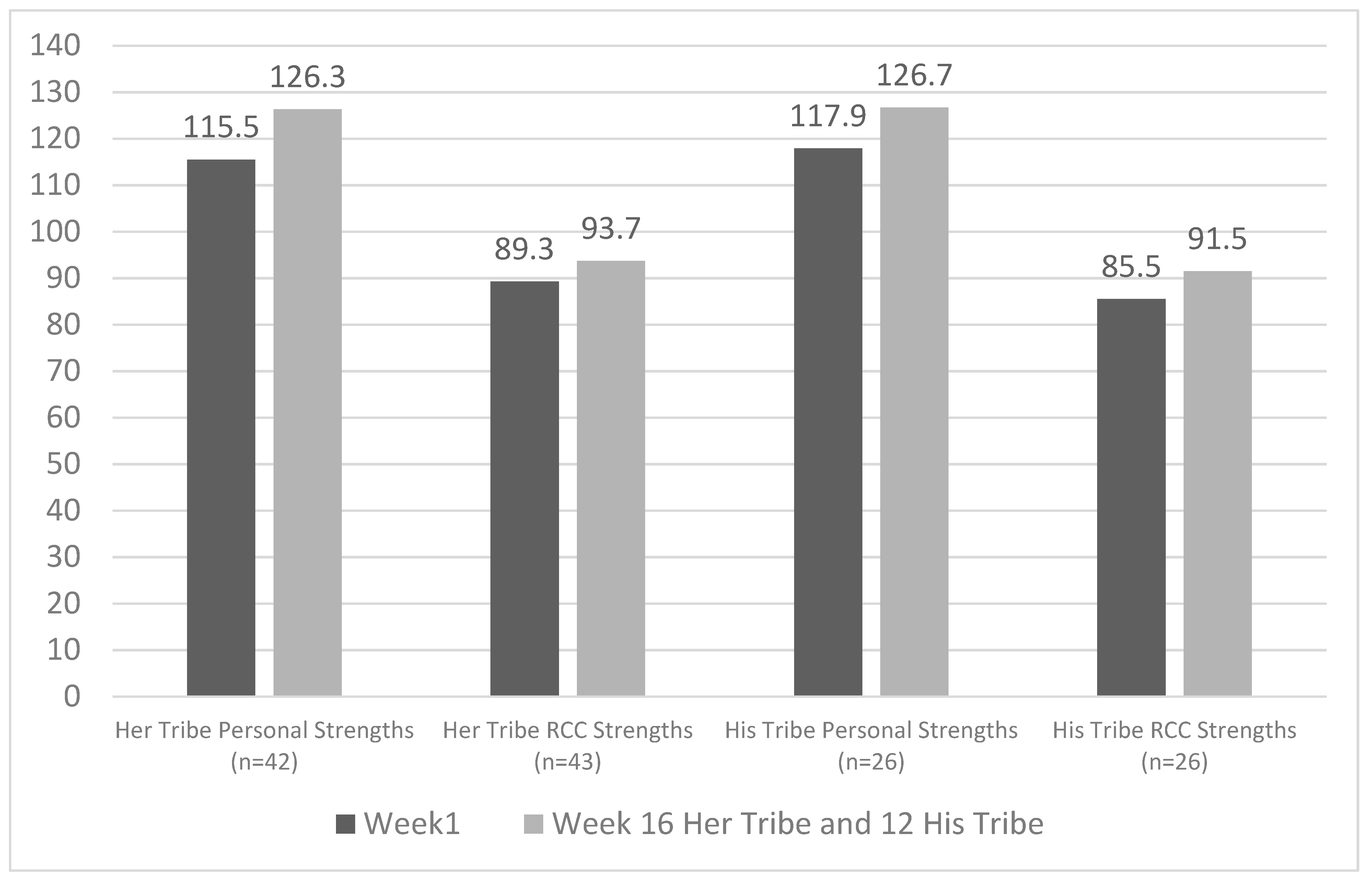
| Personal Strengths (n = 42) | 115.52 (17.13) | 126.26 (17.40) | 10.74 | 5.77, 15.70 | 4.37 *** | 0.67 |
| RRC Strengths (n = 43) | 89.30 (13.04) | 93.67 (12.07) | 4.37 | 1.00, 7.73 | 2.62 * | 0.40 |
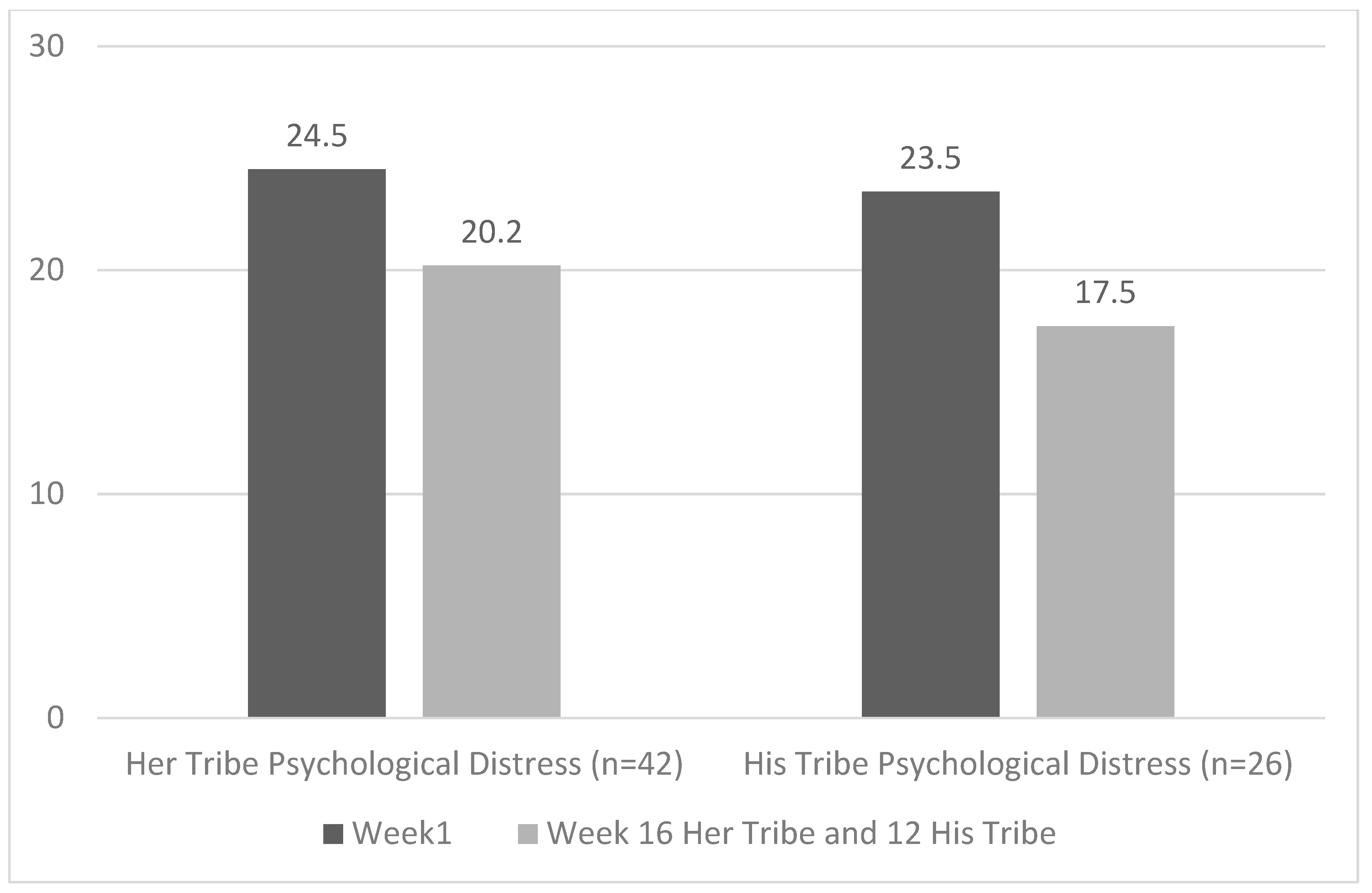
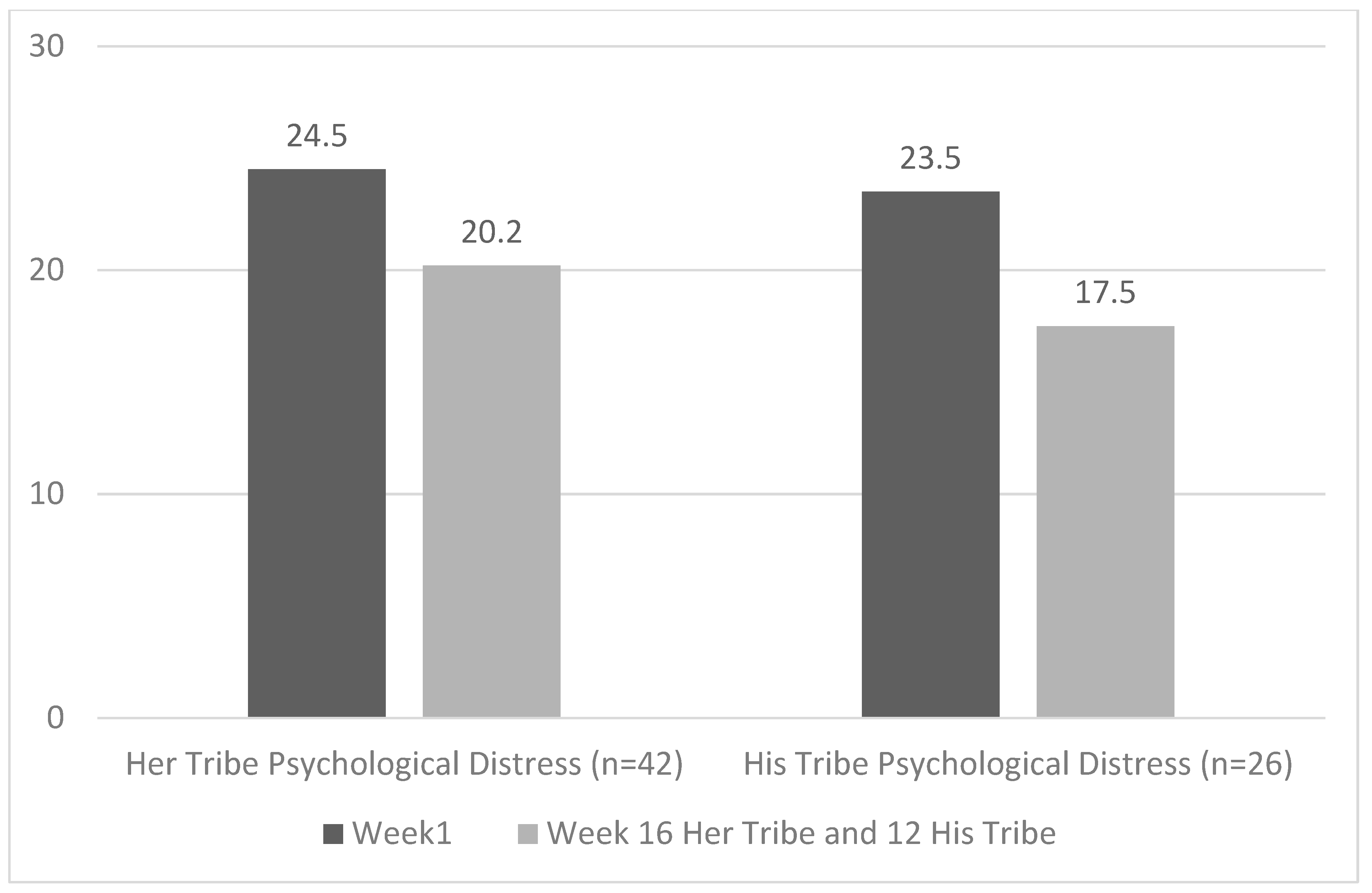
| Psychological Distress (n = 42) | 24.50 (8.10) | 20.19 (7.21) | 4.31 | −6.48, −2.14 | −4.00 *** | −0.61 |
| Aerobic (n = 18) | 3.94 (0.61) | 5.76 (0.77) | 1.81 | 1.15, 2.49 | 5.89 *** | 1.53 |
| Weight (n = 14) | 73.26 (16.72) | 71.97 (16.23) | 1.29 | −2.82, 0.24 | 1.78 | −0.41 |
| Outcomes | Her Tribe Post-Program and 6-Month Follow up Comparisons | |||||
|---|---|---|---|---|---|---|
| Post M (SD) | Follow up M (SD) | Mean Diff | 95% CI | t | Cohen’s d | |
| Personal Strengths (n = 37) | 125.05 (17.71) | 125.08 (14.83) | 0.03 | −3.61, 3.66 | 0.02 | 0.00 |
| RCC Strengths (n = 37) | 93.43 (12.55) | 94.05 (9.62) | 0.62 | −1.98, 3.22 | 0.48 | 0.08 |
| Psychological Distress (n = 36) | 20.81 (8.37) | 20.36 (8.62) | 0.44 | −2.50, 1.61 | −0.44 | −0.07 |
| His Tribe Pre- and Post-Program Comparison | ||||||
|---|---|---|---|---|---|---|
| Pre M (SD) | Post M (SD) | Mean Diff | 95% CI | t | Cohen’s d | |
| Personal Strengths (n = 26) | 117.85 (14.32) | 126.66 (13.72) | 8.81 | 3.76, 13.86 | 3.59 *** | 0.69 |
| RCC Strengths (n = 26) | 85.53 (11.87) | 91.46 (10.90) | 5.92 | 2.00, 9.84 | 3.11 ** | 0.60 |
| Psychological Distress (n = 26) | 23.50 (9.47) | 17.50 (6.09) | 6.00 | −9.56, −2.44 | −3.48 ** | −0.67 |
| Aerobic (n = 6) | 6.22 (3.15) | 6.20 (2.87) | 0.02 | −1.33, 1.30 | −0.03 | −0.12 |
| Weight (n = 14) | 89.57 (12.58) | 89.12 (11.39) | 0.45 | −1.75, 0.85 | −0.75 | −0.19 |
| His Tribe Post-Program and 6-Month Follow up Comparisons | ||||||
|---|---|---|---|---|---|---|
| Pre M (SD) | Post M (SD) | Mean Diff | 95% CI | t | Cohen’s d | |
| Personal Strengths (n = 10) | 134.10 (25.82) | 130.30 (12.18) | 3.80 | −17.0, 9.47 | −0.65 | −0.20 |
| RCC Strengths (n = 10) | 92.40 (10.23) | 91.40 (10.61) | 1.0 | −5.91, 3.91 | −0.46 | −0.14 |
| Psychological Distress (n = 10) | 18.90 (5.16) | 17.70 (4.85) | 1.20 | −2.01, 4.41 | −0.85 | −0.26 |
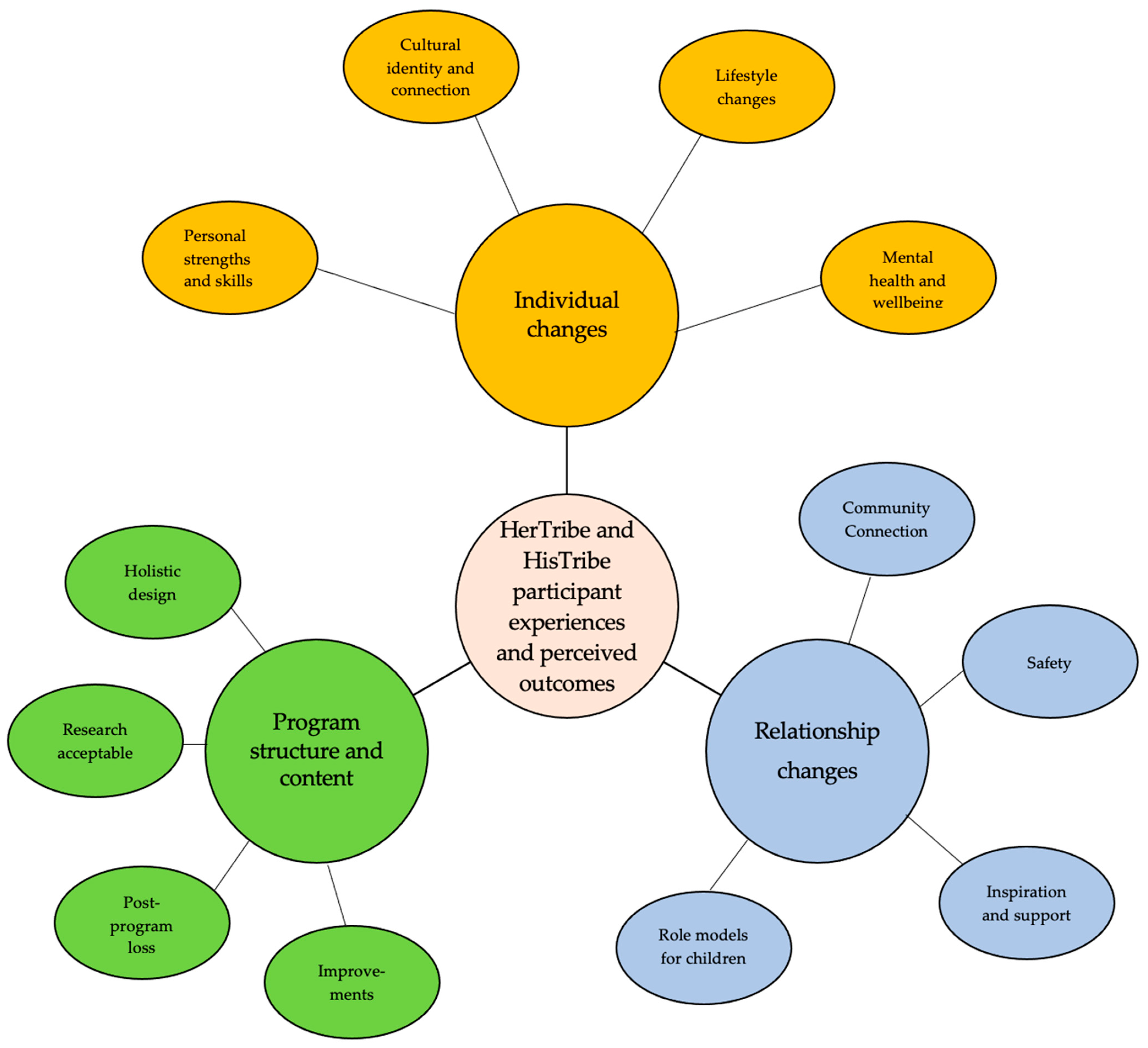
| Individual Changes | Quotes: Her Tribe Participants (3 Yarning Circles–YC1, 2, 3) | Quotes: His Tribe Participants (1Yarning Group: 10 Participants) |
|---|---|---|
| Personal strengths and skills | How many times did I say “I’m not doing that, I can’t do that”? and then I went and did it (YC1) | I’ve got more energy that in my twenties, like a lot more energy and mentally as well, I feel a lot better (P4) |
| Lifestyle changes | I think the biggest thing was the education as well. Now I don’t eat the Macas. I have the understanding of what it does, sort of thing, or sugary drinks (YC2) | I maintained sort of a fitness regime after the program (P3). Same here but I still gotta’ get the nutrition right (P1) |
| Mental health and SEWB | It really made me think about my mental health as well, a lot with the pre-talks before the exercise. And really inspired me to change my mental and physical health (P4) It was like holistic I think, and that was the big thing for me because there’s being physically fit but for me mentally fit was just as, if not more, important (P13) | I’ve had several issues with mental health…and that really… to realise that you’re not the only one out there (P10) It was good always meeting…a really positive thing, it was rare for me that I got depressed in-between that time I was coming (P5) |
| Cultural identity and connection | They were threatening to suspend me (from another program) because I was ‘too white’ to be Aboriginal. I had so much shame after that… now it’s like I’ve got community, that’s big’ (YC2) | Not just coming together as men, but just spiritually healing for everyone, whether you were hurting or not (P7). |
| Relationship Changes | Quotes: Her Tribe participants (3 Yarning Circles–YC1, 2, 3) | Quotes: His Tribe participants (1Yarning Group: 10 participants) |
| Community connection | I also made a lot of friendships out of it, like people that I see in community now that I never knew before, but I see them all the time now at events (P4) | I thought it was a good place for connection. I don’t think men connect enough. So, ah, to have more spaces where we can create that sort of environment (P6) |
| Safety | I felt in a safe environment and for me that safety was…. it was an amazing part of it. Just being accepted (YC2) | Not made to feel unwelcome. A lot of times we all feel unwelcome, no matter where we go as men (P8) |
| Inspiration and support | It was really good to have other people around, and they’re there supporting the achievement you were making, but [I] didn’t realise they were there supporting me through other things as well (YC) | We grew as a group of men, help each other with each other’s problems… like us men, we usually [do, we] avoid the issue (P8) |
| Role models for children | I kept coming back because I loved it and it was good that I could bring my kids and then show them, be a good role model for them (P1) | We get to meet each other’s little kids… it brings everyone a bit closer… the kids see that person and are like “I know you!” (P6) |
| Program Structure and Content | Quotes: Her Tribe Participants (3 Yarning Circles–YC1, 2, 3) | Quotes: His Tribe Participants (1Yarning Group: 10 Participants) |
|---|---|---|
| Holistic design | I like the way it was run, have the speakers come in and then go out, and do the work out (YC1) | We all helped each other and to see some of the Elders….they’re leaders…and you look over at Uncle pumping it out, and you’re like “I better not slacken off!” (P10) |
| Improvements | Make it a normal thing every week (P8) | One thing I didn’t like is turn up and have a feed and then you sit down and talk ….. you’ve had the feed, settled, then to try and get up and to do the exercise. I think exercise first and then the meals (P4) |
| Post-program loss | It was by far the best thing in my week. There was a post Her Tribe depression. It wasn’t like that extreme but it was like you really longed for it… that’s what made it so important, belonging..’(YC2) | Shortly after it… [the program finishing] I could feel that, like, my mental health dropping (P3) I felt the drop [in mental health] after (P6). |
| Research acceptable | At the start I was a bit like, not iffy, but it was a bit like “oh ok, so what parts and all that?”… but that quickly got away. I sort of came to realise it was going to be different. It actually turned from “oh how are you going to use this? to empowering because you’re actually a part of it sort of thing”. | No problems (P1) |
| Participant feedback | ARRQ Feedback Her Tribe participants | ARRQ feedback His Tribe participants |
| When I did it today, it was like, 80% of it was over the right-hand side [positive scores] rather than the left and that was a bit, I was like “wow, things have changed a bit”. (YC2) Made me think about the positives that I don’t often stop and think about. Completing this questionnaire makes me realise how resilient I am and how strong I am in my identity, culture and values’. (ARRQ written feedback) The questionnaire helped me reflect and think about how I have overcome adversity and how much I need to strengthen my connection to country and mob for my own wellbeing. (ARRQ written feedback) | It’s a good measurement tool… before and after... indicates what value the program was (P7) Participating in His Tribe positively impacted on my wellbeing. The questionnaire reflects these results. (ARRQ written feedback) The questionnaire gave me an opportunity to reflect on my life and identify issues in my personal life and in the community. (ARRQ written feedback) |
| Outcomes | Her Tribe Pre- and Post-Program Sub-Scale Comparisons | |||||
|---|---|---|---|---|---|---|
| Pre M (SD) | Post M (SD) | Mean Diff | 95% CI | t | Cohen’s d | |
| Safety (n = 43) | 20.53 (4.13) | 21.93 (3.84) | 1.40 | 2.47, 0.32 | 2.62 ** | 3.56 |
| Community connection (n = 44) | 16.57 (2.68) | 17.83 (2.19) | 1.27 | 2.06, 0.48 | 3.25 *** | 2.64 |
| Positive Emotions (n = 45) | 15.69 (3.22) | 17.06 (2.83) | 1.38 | 2.28, 0.47 | 3.07 ** | 3.06 |
| Self-Worth (n = 44) | 7.45 (1.82) | 8.27 (1.83) | 0.80 | 1.34, 0.30 | 3.16 *** | 1.74 |
| Outcomes | His Tribe Pre- and Post-Program Sub-Scale Comparisons | |||||
|---|---|---|---|---|---|---|
| Pre M (SD) | Post M (SD) | Mean Diff | 95% CI | t | Cohen’s d | |
| Safety (n = 26) | 19.27 (3.97) | 21.65 (3.46) | 2.38 | 3.76, 1.00 | 3.57 *** | 3.51 |
| Community connection (n = 26) | 17.23 (2.77) | 18.38 (2.02) | 1.15 | 1.91, 0.39 | 3.11 ** | 1.95 |
| Positive emotions (n = 26) | 12.04 (1.77) | 17.23 (2.41) | 5.19 | 6.14, 4.24 | 11.27 *** | 2.42 |
| Self-worth (n = 44) | 7.65 (1.41) | 8.65 (1.35) | 1.67 | 1.68, 0.32 | 3.05 ** | 1.73 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gee, G.; Sheridan, S.; Charles, L.; Dayne, L.; Joyce, L.; Stevens, J.; Paradies, Y.; Hulbert, C.; Haslam, N.; Thorpe, R.; et al. The Her Tribe and His Tribe Aboriginal-Designed Empowerment Programs. Int. J. Environ. Res. Public Health 2022, 19, 2381. https://doi.org/10.3390/ijerph19042381
Gee G, Sheridan S, Charles L, Dayne L, Joyce L, Stevens J, Paradies Y, Hulbert C, Haslam N, Thorpe R, et al. The Her Tribe and His Tribe Aboriginal-Designed Empowerment Programs. International Journal of Environmental Research and Public Health. 2022; 19(4):2381. https://doi.org/10.3390/ijerph19042381
Chicago/Turabian StyleGee, Graham, Sarah Sheridan, Lena Charles, Lana Dayne, Lisa Joyce, Jack Stevens, Yin Paradies, Carol Hulbert, Nick Haslam, Reg Thorpe, and et al. 2022. "The Her Tribe and His Tribe Aboriginal-Designed Empowerment Programs" International Journal of Environmental Research and Public Health 19, no. 4: 2381. https://doi.org/10.3390/ijerph19042381
APA StyleGee, G., Sheridan, S., Charles, L., Dayne, L., Joyce, L., Stevens, J., Paradies, Y., Hulbert, C., Haslam, N., Thorpe, R., Thorpe, L., Thorpe, A., Stewart, P., Austin, L., Lyons, L., Belfrage, M., Warber, R., Paxton, A., & Thompson, L. (2022). The Her Tribe and His Tribe Aboriginal-Designed Empowerment Programs. International Journal of Environmental Research and Public Health, 19(4), 2381. https://doi.org/10.3390/ijerph19042381