
Aging with HIV: Increased Risk of HIV Comorbidities in Older Adults



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Aim
2.2. Sample and Data Collection
2.3. Ethics Considerations
2.4. Data Analysis
3. Results
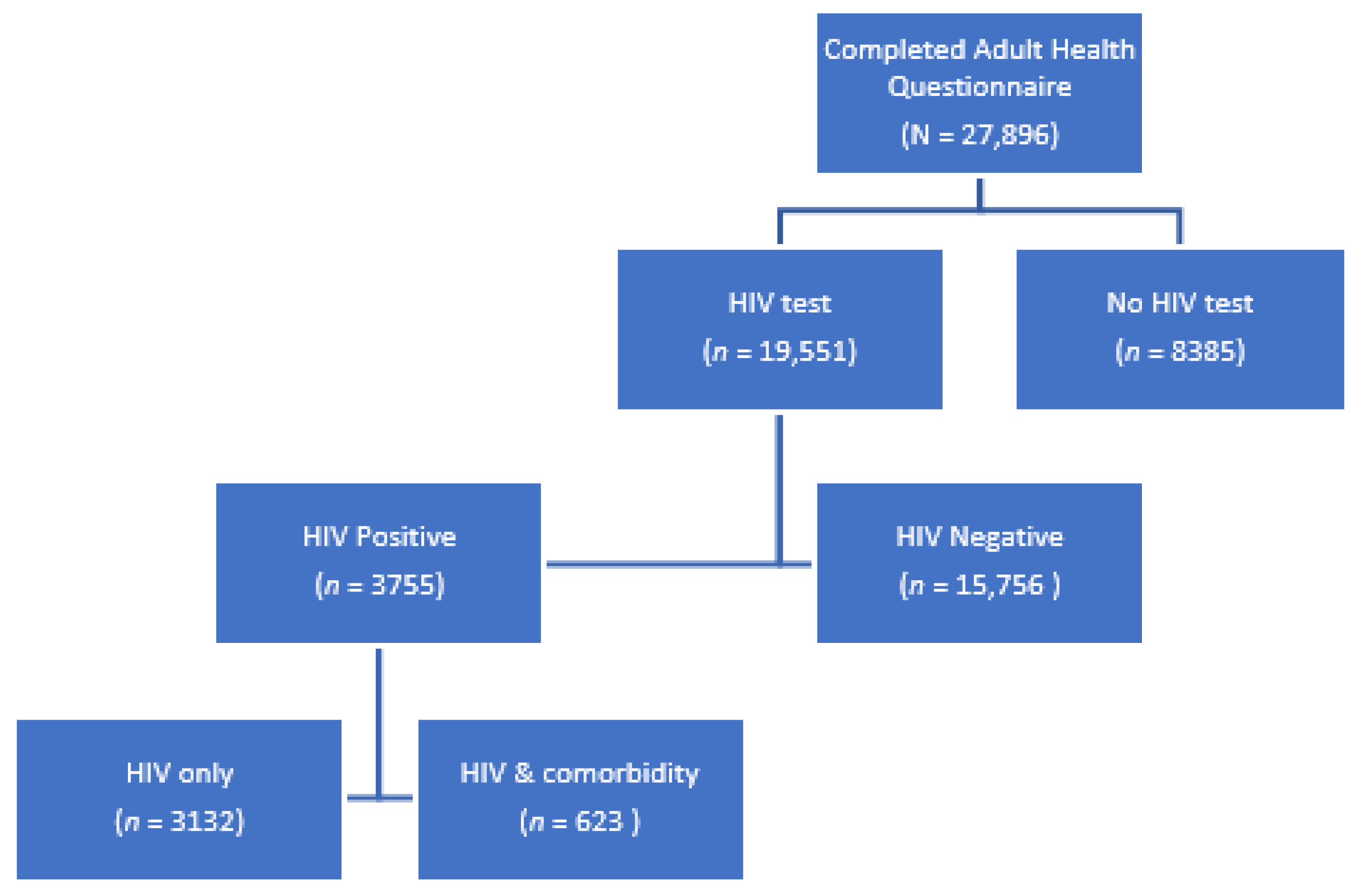
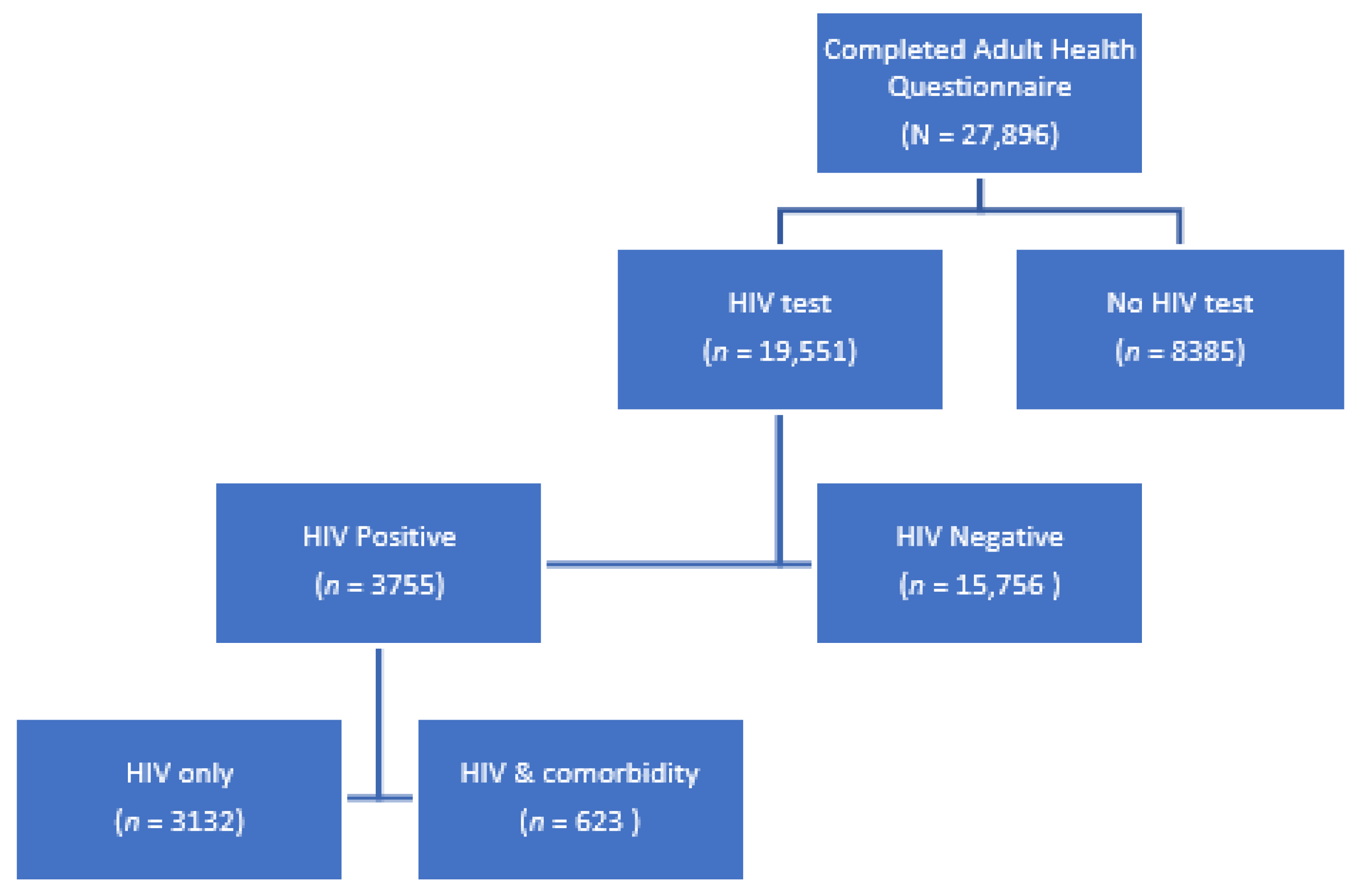
3.1. Sample Description
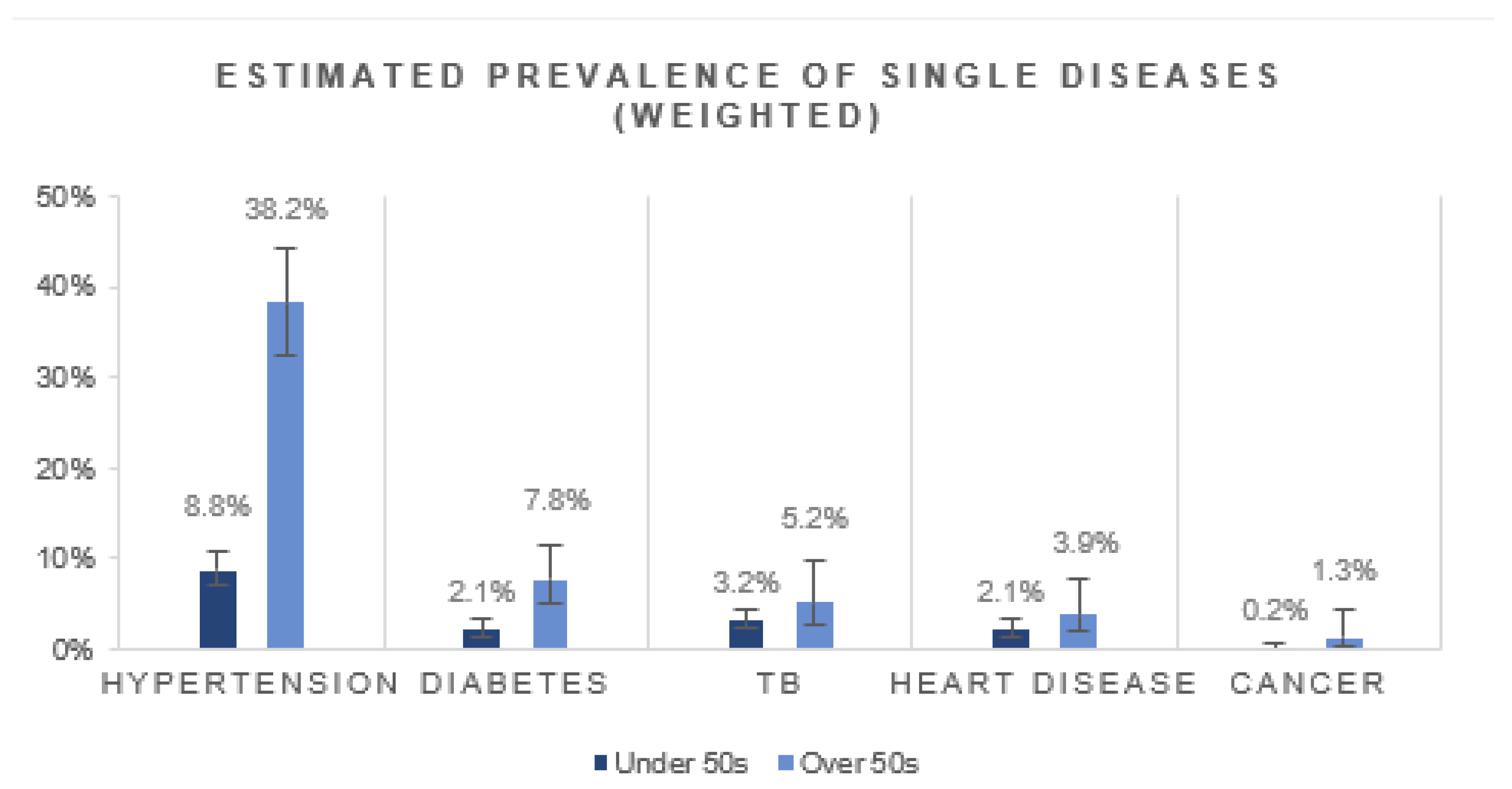
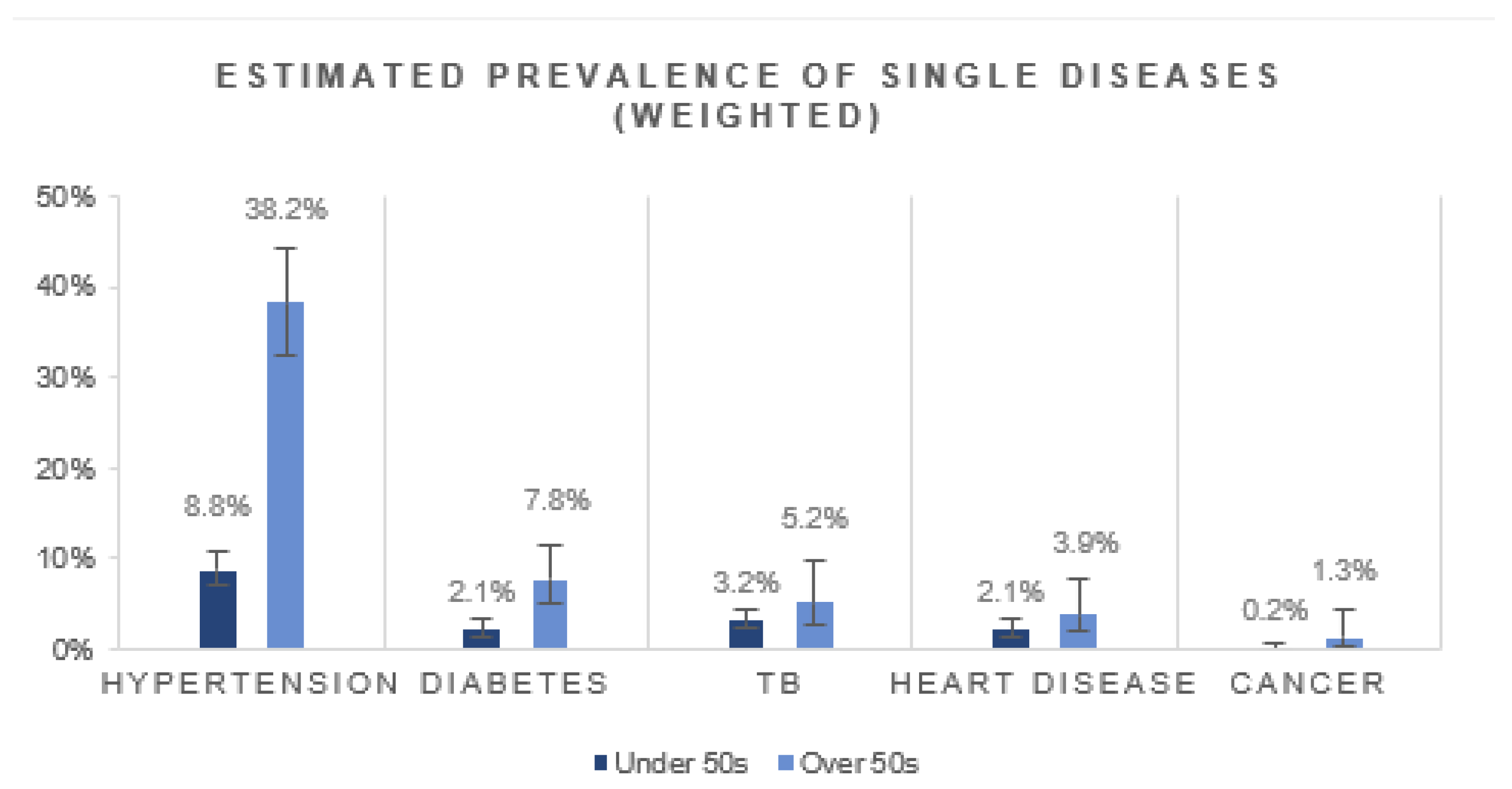
3.2. Prevalence of Comorbidities in Those with HIV
3.3. Factors Associated with Having HIV Comorbidity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Simbayi, L.; Zuma, K.; Moyo, S.; Marinda, E.; Mabaso, M.; Ramlagan, S.; North, A.; Mohlabane, N.; Dietrich, C.; Naidoo, I.; et al. South African National HIV Prevalence, Incidence, Behaviour and Communication Survey, 2017; Report No.: 978-0-7969-2444-5; HSRC Press: Cape Town, South Africa, 2019. [Google Scholar]
- UNAIDS. Country Factsheets: South Africa 2020. 2021. Available online: https://www.unaids.org/en/regionscountries/countries/southafrica (accessed on 20 September 2021).
- UNAIDS. 90-90-90 An Ambitious Treatment Target to Help End the AIDS Epidemic. Available online: https://www.unaids.org/sites/default/files/media_asset/90-90-90_en.pdf (accessed on 6 December 2021).
- AVERT. HIV and AIDS in South Africa. 2020. Available online: https://www.avert.org/professionals/hiv-around-world/sub-saharan-africa/south-africa (accessed on 28 July 2021).
- Marinda, E.; Simbayi, L.; Zuma, K.; Zungu, N.; Moyo, S.; Kondlo, L.; Jooste, S.; Nadol, P.; Igumbor, E.; Dietrich, C. Towards achieving the 90–90–90 HIV targets: Results from the south African 2017 national HIV survey. BMC Public Health 2020, 20, 1375. [Google Scholar] [CrossRef]
- Teeraananchai, S.; Kerr, S.; Amin, J.; Ruxrungtham, K.; Law, M. Life expectancy of HIV-positive people after starting combination antiretroviral therapy: A meta-analysis. HIV Med. 2017, 18, 256–266. [Google Scholar] [CrossRef]
- Haregu, T.N.; Oldenburg, B.; Sestwe, G.; Elliott, J.; Nanayakkara, V. Epidemiology of comorbidity of HIV/AIDS and non-communicable diseases in developing countries: A systematic review. J. Glob. Health Care Syst. 2012, 2, 1–12. [Google Scholar]
- Pillay-van Wyk, V.; Msemburi, W.; Laubscher, R.; Dorrington, R.E.; Groenewald, P.; Glass, T.; Nojilana, B.; Joubert, J.D.; Matzopoulos, R.; Prinsloo, M. Mortality trends and differentials in South Africa from 1997 to 2012: Second National Burden of Disease Study. Lancet Glob. Health 2016, 4, e642–e653. [Google Scholar] [CrossRef] [Green Version]
- Levitt, N.S.; Steyn, K.; Dave, J.; Bradshaw, D. Chronic noncommunicable diseases and HIV-AIDS on a collision course: Relevance for health care delivery, particularly in low-resource settings—Insights from South Africa. Am. J. Clin. Nutr. 2011, 94, 1690S–1696S. [Google Scholar] [CrossRef] [Green Version]
- Wong, E.B.; Olivier, S.; Gunda, R.; Koole, O.; Surujdeen, A.; Gareta, D.; Munatsi, D.; Modise, T.H.; Dreyer, J.; Nxumalo, S.; et al. Convergence of infectious and non-communicable disease epidemics in rural South Africa: A cross-sectional, population-based multimorbidity study. Lancet Glob. Health 2021, 9, e967–e976. [Google Scholar] [CrossRef]
- van Heerden, A.; Barnabas, R.V.; Norris, S.A.; Micklesfield, L.K.; van Rooyen, H.; Celum, C. High prevalence of HIV and non-communicable disease (NCD) risk factors in rural KwaZulu-Natal, South Africa. J. Int. AIDS Soc. 2017, 20, e25012. [Google Scholar] [CrossRef] [Green Version]
- Chang, A.Y.; Gómez-Olivé, F.X.; Payne, C.; Rohr, J.K.; Manne-Goehler, J.; Wade, A.N.; Wagner, R.G.; Montana, L.; Tollman, S.; Salomon, J.A. Chronic multimorbidity among older adults in rural South Africa. BMJ Glob. Health 2019, 4, e001386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oni, T.; Berkowitz, N.; Kubjane, M.; Goliath, R.; Levitt, N.S.; Wilkinson, R.J. Trilateral overlap of tuberculosis, diabetes and HIV-1 in a high-burden African setting: Implications for TB control. Eur. Respir. J. 2017, 50, 1700004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pourcher, V.; Gourmelen, J.; Bureau, I.; Bouee, S. Comorbidities in people living with HIV: An epidemiologic and economic analysis using a claims database in France. PLoS ONE 2020, 15, e0243529. [Google Scholar] [CrossRef] [PubMed]
- Maciel, R.A.; Klück, H.M.; Durand, M.; Sprinz, E. Comorbidity is more common and occurs earlier in persons living with HIV than in HIV-uninfected matched controls, aged 50 years and older: A cross-sectional study. Int. J. Infect. Dis. 2018, 70, 30–35. [Google Scholar] [CrossRef] [Green Version]
- Marcus, J.L.; Leyden, W.A.; Alexeeff, S.E.; Anderson, A.N.; Hechter, R.C.; Hu, H.; Lam, J.O.; Towner, W.J.; Yuan, Q.; Horberg, M.A. Comparison of overall and comorbidity-free life expectancy between insured adults with and without HIV infection, 2000–2016. JAMA Netw. Open 2020, 3, e207954. [Google Scholar] [CrossRef] [PubMed]
- Calcagno, A.; Nozza, S.; Muss, C.; Celesia, B.; Carli, F.; Piconi, S.; De Socio, G.; Cattelan, A.; Orofino, G.; Ripamonti, D. Ageing with HIV: A multidisciplinary review. Infection 2015, 43, 509–522. [Google Scholar] [CrossRef] [PubMed]
- Pathai, S.; Lawn, S.D.; Gilbert, C.E.; McGuinness, D.; McGlynn, L.; Weiss, H.A.; Port, J.; Christ, T.; Barclay, K.; Wood, R.; et al. Accelerated biological ageing in HIV-infected individuals in South Africa: A case-control study. AIDS 2013, 27, 2375–2384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tavoschi, L.; Dias, J.G.; Pharris, A.; Schmid, D.; Sasse, A.; Van Beckhoven, D.; Varleva, T.; Blazic, T.N.; Hadjihannas, L.; Koliou, M. New HIV diagnoses among adults aged 50 years or older in 31 European countries, 2004–2015: An analysis of surveillance data. Lancet HIV 2017, 4, e514–e521. [Google Scholar] [CrossRef] [Green Version]
- Autenrieth, C.S.; Beck, E.J.; Stelzle, D.; Mallouris, C.; Mahy, M.; Ghys, P. Global and regional trends of people living with HIV aged 50 and over: Estimates and projections for 2000–2020. PLoS ONE 2018, 13, e0207005. [Google Scholar] [CrossRef]
- Havlir, D.; Lockman, S.; Ayles, H.; Larmarange, J.; Chamie, G.; Gaolathe, T.; Iwuji, C.; Fidler, S.; Kamya, M.; Floyd, S. What do the Universal Test and Treat trials tell us about the path to HIV epidemic control? J. Int. AIDS Soc. 2020, 23, e25455. [Google Scholar] [CrossRef] [Green Version]
- Guaraldi, G.; Milic, J.; Mussini, C. Aging with HIV. Curr. HIV/AIDS Rep. 2019, 16, 475–481. [Google Scholar] [CrossRef]
- Xu, Y.; Chen, X.; Wang, K. Global prevalence of hypertension among people living with HIV: A systematic review and meta-analysis. J. Am. Soc. Hypertens. 2017, 11, 530–540. [Google Scholar] [CrossRef]
- Nduka, C.; Stranges, S.; Sarki, A.; Kimani, P.; Uthman, O. Evidence of increased blood pressure and hypertension risk among people living with HIV on antiretroviral therapy: A systematic review with meta-analysis. J. Hum. Hypertens. 2016, 30, 355–362. [Google Scholar] [CrossRef]
- Rozanova, J.; Zeziulin, O.; Rich, K.M.; Altice, F.L.; Kiriazova, T.; Zaviryukha, I.; Sosidko, T.; Gulati, K.; Carroll, C.; Shenoi, S.V. An expanding HIV epidemic among older adults in Ukraine: Implications for patient-centered care. PLoS ONE 2021, 16, e0256627. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Olivé, F.X.; Houle, B.; Rosenberg, M.; Kabudula, C.; Mojola, S.; Rohr, J.K.; Clark, S.; Angotti, N.; Schatz, E.; Kahn, K. Brief Report: HIV incidence among older adults in a rural South African setting: 2010–2015. J. Acquir. Immune Defic. Syndr. (1999) 2020, 85, 18. [Google Scholar] [CrossRef] [PubMed]
- Guaraldi, G.; Zona, S.; Brothers, T.D.; Carli, F.; Stentarelli, C.; Dolci, G.; Santoro, A.; Beghetto, B.; Menozzi, M.; Mussini, C. Aging with HIV vs. HIV seroconversion at older age: A diverse population with distinct comorbidity profiles. PLoS ONE 2015, 10, e0118531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGettrick, P.; Barco, E.A.; Mallon, P.W. Ageing with HIV. Healthcare; Multidisciplinary Digital Publishing Institute: Basel, Switzerland, 2018. [Google Scholar]
- Negin, J.; Martiniuk, A.; Cumming, R.G.; Naidoo, N.; Phaswana-Mafuya, N.; Madurai, L.; Williams, S.; Kowal, P. Prevalence of HIV and chronic comorbidities among older adults. AIDS 2012, 26, S55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Justice, A.C.; Gordon, K.S.; Romero, J.; Edelman, E.J.; Garcia, B.J.; Jones, P.; Khoo, S.; Re, V.L., III; Rentsch, C.T.; Tate, J.P. Polypharmacy-associated risk of hospitalisation among people ageing with and without HIV: An observational study. Lancet Healthy Longev. 2021, 2, e639–e650. [Google Scholar] [CrossRef]
- Wyman, M.F.; Shiovitz-Ezra, S.; Bengel, J. Ageism in the health care system: Providers, patients, and systems. In Contemporary Perspectives on Ageism; Springer: Cham, Switzerland, 2018; pp. 193–212. [Google Scholar]
- World Health Organization. Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection: Recommendations for a Public Health Approach; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Roomaney, R.A.; van Wyk, B.; Turawa, E.B.; Pillay-van Wyk, V. Multimorbidity in South Africa: A systematic review of prevalence studies. BMJ Open 2021, 11, e048676. [Google Scholar]
- Xu, X.; Mishra, G.D.; Jones, M. Evidence on multimorbidity from definition to intervention: An overview of systematic reviews. Ageing Res. Rev. 2017, 37, 53–68. [Google Scholar] [CrossRef] [Green Version]
- Pregibon, D. Logistic regression diagnostics. Ann. Stat. 1981, 9, 705–724. [Google Scholar] [CrossRef]
- Zungu, N.P.; Mabaso, M.L.; Kumalo, F.; Sigida, S.; Mlangeni, L.; Wabiri, N.; Chasela, C. Prevalence of non-communicable diseases (NCDs) and associated factors among HIV positive educators: Findings from the 2015/6 survey of Health of Educators in Public Schools in South Africa. PLoS ONE 2019, 14, e0209756. [Google Scholar] [CrossRef] [Green Version]
- Naidoo, V.A.; Martinson, N.A.; Moodley, P.; Joyimbana, W.; Mothlaoleng, K.; Abraham, P.; Otwombe, K.; Variava, E. HIV Prevalence and Morbidity in Older Inpatients in a High HIV Prevalence Setting. AIDS Res. Hum. Retrovir. 2020, 36, 186–192. [Google Scholar] [CrossRef]
- Ciccacci, F.; Tolno, V.T.; Doro Altan, A.M.; Liotta, G.; Orlando, S.; Mancinelli, S.; Palombi, L.; Marazzi, M.C. Noncommunicable diseases burden and risk factors in a cohort of HIV+ elderly patients in Malawi. AIDS Res. Hum. Retrovir. 2019, 35, 1106–1111. [Google Scholar] [CrossRef] [PubMed]
- Kendall, C.E.; Wong, J.; Taljaard, M.; Glazier, R.H.; Hogg, W.; Younger, J.; Manuel, D.G. A cross-sectional, population-based study measuring comorbidity among people living with HIV in Ontario. BMC Public Health 2014, 14, 161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, K.M.; Parker, W.-a.; Mchiza, Z.J.; Sewpaul, R.; Labadarios, D.; Rosen, S.; Stokes, A. Quantifying unmet need for hypertension care in South Africa through a care cascade: Evidence from the SANHANES, 2011-2012. BMJ Glob. Health 2017, 2, e000348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, B.; Goudge, J.; Ataguba, J.E.; McIntyre, D.; Nxumalo, N.; Jikwana, S.; Chersich, M. Inequities in access to health care in South Africa. J. Public Health Policy 2011, 32, S102–S123. [Google Scholar] [CrossRef] [PubMed]
- Peer, N. The converging burdens of infectious and non-communicable diseases in rural-to-urban migrant Sub-Saharan African populations: A focus on HIV/AIDS, tuberculosis and cardio-metabolic diseases. Trop. Dis. Travel Med. Vaccines 2015, 1, 6. [Google Scholar] [CrossRef] [Green Version]
- Godongwana, M.; De Wet-Billings, N.; Milovanovic, M. The comorbidity of HIV, hypertension and diabetes: A qualitative study exploring the challenges faced by healthcare providers and patients in selected urban and rural health facilities where the ICDM model is implemented in South Africa. BMC Health Serv. Res. 2021, 21, 647. [Google Scholar] [CrossRef]
- UNAIDS. Global AIDS Update 2021. Confronting Inequalities: Lessons for Pandemic Responses from 40 Years of AIDS. 2021. Available online: https://www.unaids.org/sites/default/files/media_asset/2021-global-aids-update_en.pdf (accessed on 10 February 2022).
- Richterman, A.; Sax, P.E. Antiretroviral therapy in older people with HIV. Curr. Opin. HIV AIDS 2020, 15, 118–125. [Google Scholar] [CrossRef]
- Mann, S.C.; Castillo-Mancilla, J.R. HIV, aging, and adherence: An update and future directions. Curr. Opin. HIV AIDS 2020, 15, 134–141. [Google Scholar] [CrossRef]
- Kandala, N.-B.; Nnanatu, C.C.; Dukhi, N.; Sewpaul, R.; Davids, A.; Reddy, S.P. Mapping the Burden of Hypertension in South Africa: A Comparative Analysis of the National 2012 SANHANES and the 2016 Demographic and Health Survey. Int. J. Environ. Res. Public Health 2021, 18, 5445. [Google Scholar] [CrossRef]
- National Department of Health; Statistics South Africa; South African Medical Research Council; ICF. South Africa Demographic and Health Survey 2016; NDoH; Stats SA; SAMRC; ICF: Pretoria, South Africa; Rockville, MA, USA, 2019.

{kind=link}
{kind=link}
| Variable | % (n) | p-Value * | ||
|---|---|---|---|---|
| Total (N = 3755) | Under 50s (n = 3066) | Over 50s (n = 688) | ||
| Age (Median years and IQR) | 36 (29–46) | 33 (28–40) | 56 (53–61) | - |
| Female | 73.4 (2754) | 73.9 (2266) | 80.0 (487) | 0.115 |
| Urban location | 45.6 (1712) | 45.7 (1402) | 45.1 (310) | 0.750 |
| Province | <0.001 | |||
| Eastern Cape | 7.4 (277) | 7.5 (230) | 6.8 (47) | |
| Free State | 4.7 (177) | 4.2 (130) | 6.8 (47) | |
| Gauteng | 13.9 (523) | 13.9 (427) | 14.0 (96) | |
| KwaZulu-Natal | 38.4 (1442) | 38.6 (1184) | 37.5 (258) | |
| Limpopo | 5.1 (193) | 4.5 (137) | 8.1 (56) | |
| Mpumalanga | 15.6 (585) | 16.0 (490) | 13.7 (94) | |
| Northern Cape | 3.4 (126) | 3.5 (108) | 2.6 (18) | |
| North-West | 7.2 (269) | 7.2 (220) | 7.1 (49) | |
| Western Cape | 4.3 (163) | 4.6 (140) | 3.3 (23) | |
| Employed/Self-employed | 27.9 (987) | 28.9 (836) | 23.6 (151) | 0.007 |
| Education level | <0.001 | |||
| Primary or less | 23.9 (688) | 18.4 (446) | 52.9 (241) | |
| Secondary complete | 70.6 (2036) | 76.0 (1844) | 42.1 (192) | |
| Tertiary | 5.6 (161) | 5.7 (138) | 5.0 (23) | |
| Number of Comorbidities | Weighted % (95% CI) | ||
|---|---|---|---|
| Total | Under 50s | Over 50s | |
| HIV only | 82.2 (80.0–84.3) | 87.0 (84.6–89.0) | 55.9 (49.7–61.9) |
| 1 comorbidity | 14.8 (12.9–16.9) | 11.1 (9.2–13.2) | 35.5 (29.9–41.6) |
| 2 comorbidities | 2.4 (1.7–3.4) | 1.6 (1.0–2.6) | 7.2 (4.6–11.0) |
| 3 + comorbidities | 0.5 (0.3–1.0) | 0.4 (0.1–0.9) | 1.4 (0.4–4.1) |
| HIV and comorbidity | 17.8 (15.7–20.0) | 13.0 (11.0–15.4) | 44.1 (38.1–50.3) |
| Variable | Unadjusted Odds Ratios (95% CI) | Adjusted Odds Ratios (95% CI) |
|---|---|---|
| Age over 50 years (Reference: Under 50s) | 5.3 (3.8–7.3) | 4.7 (3.1–7.0) |
| Sex (Reference: Male) | 1.4 (1.0–2.0) | 1.6 (1.11–2.4) |
| Urban (Reference: Rural) | 1.9 (1.4–2.5) | 2.6 (1.8–3.7) |
| Education (Reference: Primary) | ||
| Secondary | 0.6 (0.4–0.9) | 0.7 (0.5–1.1) |
| Tertiary | 1.1 (0.5–2.7) | 1.4 (0.5–3.6) |
| Employed (Reference: Not employed) | 0.6 (0.4–0.9) | 0.6 (0.4–0.9) |
| Current alcohol use (Reference: No current alcohol use) | 1.0 (0.7–1.4) | 1.1 (0.8–1.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roomaney, R.A.; van Wyk, B.; Pillay-van Wyk, V. Aging with HIV: Increased Risk of HIV Comorbidities in Older Adults. Int. J. Environ. Res. Public Health 2022, 19, 2359. https://doi.org/10.3390/ijerph19042359
Roomaney RA, van Wyk B, Pillay-van Wyk V. Aging with HIV: Increased Risk of HIV Comorbidities in Older Adults. International Journal of Environmental Research and Public Health. 2022; 19(4):2359. https://doi.org/10.3390/ijerph19042359
Chicago/Turabian StyleRoomaney, Rifqah Abeeda, Brian van Wyk, and Victoria Pillay-van Wyk. 2022. "Aging with HIV: Increased Risk of HIV Comorbidities in Older Adults" International Journal of Environmental Research and Public Health 19, no. 4: 2359. https://doi.org/10.3390/ijerph19042359
APA StyleRoomaney, R. A., van Wyk, B., & Pillay-van Wyk, V. (2022). Aging with HIV: Increased Risk of HIV Comorbidities in Older Adults. International Journal of Environmental Research and Public Health, 19(4), 2359. https://doi.org/10.3390/ijerph19042359