1. Introduction
The field of healthcare in the United States (U.S.) has long been considered hazardous because of unhealthful or error-prone environments, high mortality rates, and the unnecessary loss of valuable lives and assets [
1]. The inconsistency between highly advanced medical technologies and less developed medical practices leads to disappointment among patients expecting to receive high-quality healthcare, and to frequent vulnerability to medical errors and adverse events (AEs) [
1]. AEs not associated with specific diseases include unfavorable outcomes of faulty diagnoses or inappropriate treatments, rather than resulting from medical errors, carelessness, or low-level care [
2].
Research has shown that U.S. healthcare institutions lack many of the innovations required to eliminate prevalent risk [
2,
3,
4,
5,
6]. The Institute of Medicine (IOM) report “
To Err Is Human: Building a Safer Health System” has brought international attention to the issue of patient safety. By highlighting the amount of harm done, the IOM encourages healthcare institutions to improve the quality of their healthcare practices and thus increase patient safety. Increasing awareness of patient safety creates a culture ensuring that patients encounter fewer risks while receiving healthcare [
7]. Globally, attention has shifted to making a culture of patient safety a cornerstone of effective healthcare policy.
Patient safety is defined as “freedom from accidental or preventable injuries produced by medical care” [
8], and increased attention has been directed to evaluating safety levels in healthcare organizations [
9,
10,
11]. Increased safety culture awareness has improved healthcare services and led to more favorable outcomes. However, studies and reviews [
12,
13,
14,
15,
16,
17] have found that, globally, large numbers of patients remain vulnerable to avoidable risks and continue to be subjected to below-average levels of healthcare [
18], with a rate of AE occurrence between 3% and 17%. For example, in the United Kingdom, a report of the Mid-Staffordshire NHS Foundation Trust has revealed several points of weakness in patient care safety [
19]. Ample evidence of wide-ranging errors and failures has been found worldwide [
20].
These errors and failures lead to large losses in healthcare assets, costing the U.S. USD 19 billion per year due to hospital overstays, unnecessary time off work, and legal action [
21]. Therefore, improving patient safety is an investment in healthcare provision. Policymakers can be assured that the financial gains made by improving patient safety far outweigh the losses [
22].
This study sought to highlight the possibilities of establishing institutional healthcare that prioritizes patient safety. In safe and well-established healthcare systems, defects or problems should be detected and addressed in a timely manner, and healthcare services should be continually upgraded and improved to ensure the successful advancement of patient safety [
23]. The findings of this study should assist in standardizing medical safety practices to yield more effective and efficient healthcare systems [
24,
25].
The primary objective of the study was to conduct a patient safety culture (PSC) evaluation by probing the 12 areas assessed by the Hospital Survey of Patient Safety Culture (HSOPSC). The research relied on the development of a model indicating the effects of hospital settings on the respondents. Healthcare workers’ perceptions of PSC and the effects of their awareness of safety culture were thoroughly evaluated.
The research hypotheses were aimed at testing the correlations among potential latent variables, among which PSC was prominent. The latent variable of PSC consists of ten factors: (1) teamwork within the hospital unit, (2) organizational learning and continual improvement, (3) staffing, (4) nonpunitive response to error, (5) communication openness, (6) supervisor/manager expectations and actions promoting safety, (7) feedback and communication regarding errors, (8) management support for patient safety, (9) teamwork across hospital units, and (10) handoffs and transitions. Moreover, the frequency of events reported and overall perceptions of patient safety affect PSC. The study measured the effects of personal and hospital predictors on perceptions of PSC and outcomes in hospital settings. Previous research has indicated that the HSOPSC is considered reliable and valid in the U.S. [
5,
24,
26,
27] and internationally [
14,
23,
28,
29,
30,
31,
32]. However, no study has examined second-order HSPSC factors. This study was aimed at addressing this gap.
Previous research has indicated that respondent characteristics, such as staff position [
33,
34], and hospital characteristics, such as teaching status [
27,
35,
36,
37] and geographic region [
29,
30,
31,
32], significantly influence the perceptions of PSC, frequency of event reporting, and overall perceptions of safety. Because no study has examined the relationships between personal and hospital characteristics, this study was aimed at addressing this gap.
Moreover, PSC has been found to affect the frequency of event reporting and overall perceptions of safety [
5,
24,
26,
27,
38].
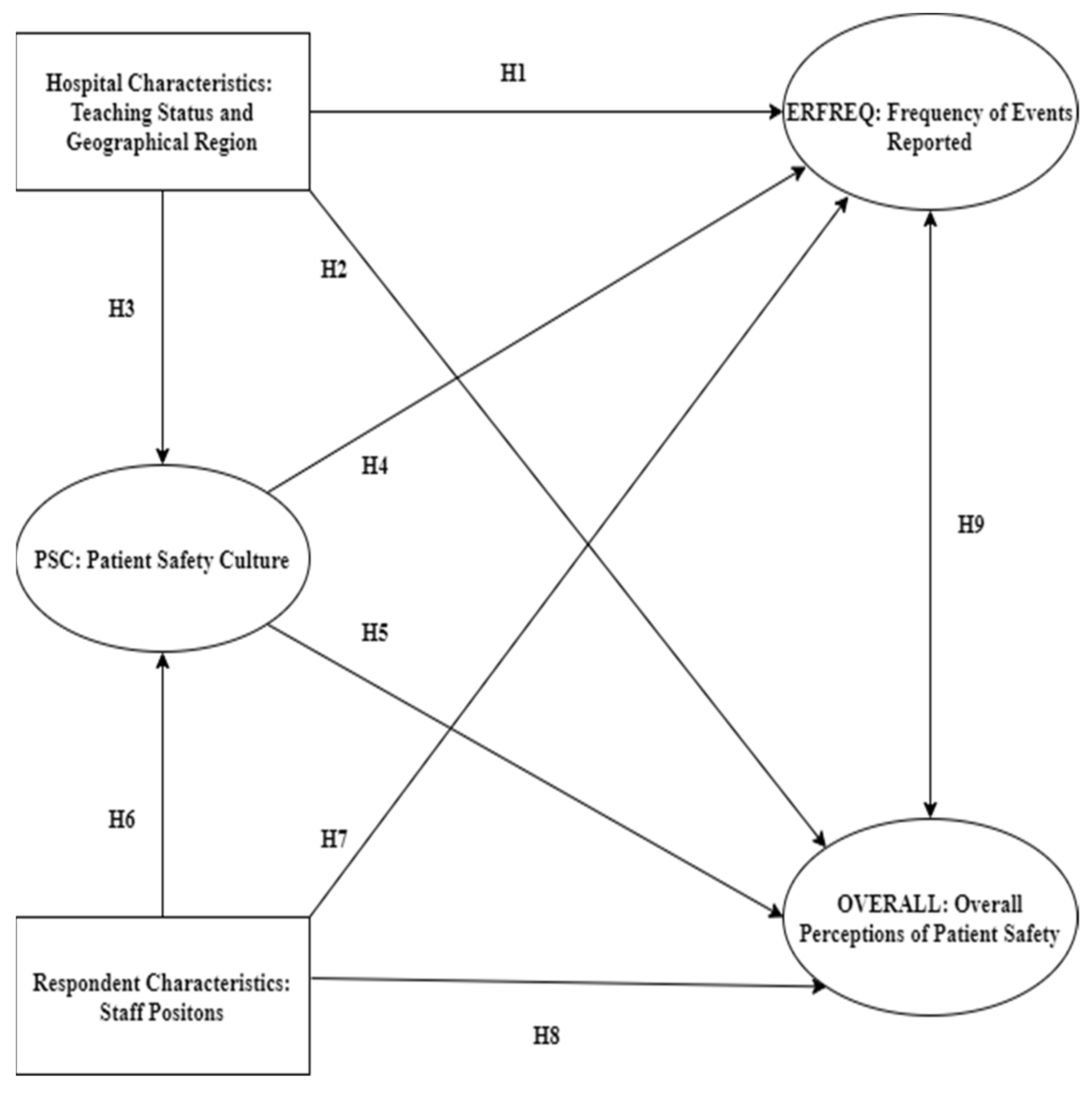
In view of the above discussion, the relationships among hospital characteristics, respondent characteristics, the frequency of reported error events (ERFREQ), and overall perceptions of patient safety (OVERALL) were explored, on the basis of the following nine hypotheses (
Figure 1).
Hypothesis 1. (H1): Hospital characteristics have a significant influence on ERFREQ.
Hypothesis 2. (H2): Hospital characteristics have a significant influence on OVERALL.
Hypothesis 3. (H3): Hospital characteristics have a significant influence on PSC.
Hypothesis 4. (H4): PSC is related to ERFREQ.
Hypothesis 5. (H5): PSC is related to OVERALL.
Hypothesis 6. (H6): Respondent characteristics have a significant influence on perceived PSC.
Hypothesis 7. (H7): Respondent characteristics have a significant influence on ERFREQ.
Hypothesis 8. (H8): Respondent characteristics have a significant influence on OVERALL.
Hypothesis 9. (H9): OVERALL and ERFREQ are significantly associated.
4. Discussion
4.1. This Study
The purpose of this study was to investigate the extent of the relationships among the perceptions of PSC, overall perceptions of patient safety, frequency of event reporting, and hospital and respondent characteristics, among medical and administrative staff in U.S. hospitals. The results revealed four aspects underlying these relationships.
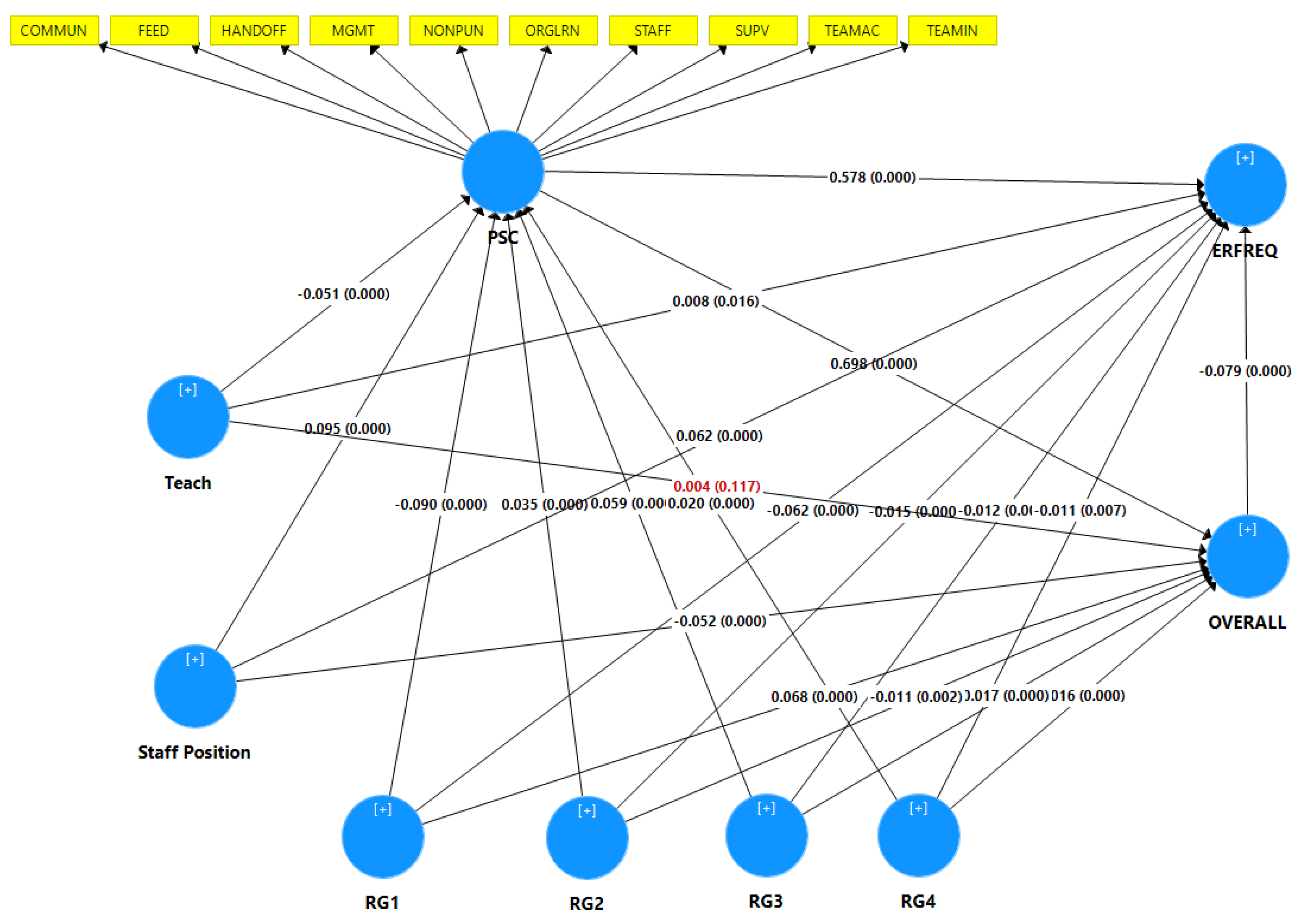
First, PSC is a shared value among institutional staff regarding the operation of and interactions between work units and systems, which together produce institutional behavioral norms that promote safety [
51]. The results indicated that the perception of PSC has a significant relationship with overall perceptions of patient safety and the frequency of event reporting. The strong correlations indicated that PSC as a higher order construct was valid and reliable for the model, and HOC was used to reduce the number of path model relationships. PSC is associated with procedural efficiency, adequate staffing, managerial support for nurses, and good relationships among staff [
52,
53,
54]. In general, successful hospitals and transparent health systems are those that apply systematic solutions to enhance patient safety [
55]. PSC significantly influences safety outcomes, including reporting frequency and overall perceptions of patient safety [
51,
56,
57].
Second, as predicted, hospital characteristics, including region and teaching status, significantly influenced PSC, ERFREQ, and the overall perceptions of participants. The staff in U.S. hospitals had high perception in four of the five regions. Only the staff in hospitals in the Northeast region had low perception of PSC and ERFREQ. However, staff in the Northeast region had higher overall perceptions of patient safety than the staff in other U.S. hospitals. These variations in perception might have occurred because of the diversity of populations, culture, and work experience; therefore, each region should be investigated individually. Wagner [
32] has found similar variations in PSC between hospitals in the U.S. and those in the Netherlands and Taiwan, whereas Eiras [
29] has found differences in perceptions of PSC among hospitals in northern, central, and southern Portugal. Moreover, staff in teaching hospitals had higher perception of ERFREQ and lower perception of PSC than did nonteaching staff, but teaching status did not influence staff perception regarding overall perceptions of patient safety. These variations can arise from a blaming culture, and educational programs and their availability in health systems. Rather than blaming individuals, a hospital with a positive PSC is open and fair to staff, and learns from its mistakes [
52,
53]. Güneş [
35] has also found no relationship between PSC and hospital type, whereas Ammouri [
36] has found that nurses in teaching hospitals are more perceptive of PSC.
Third, participants in this study were divided into medical and nonmedical staff to improve the general understanding of perceptions of PSC. The results revealed that medical staff had higher perceptions of ERFREQ and PSC than nonmedical staff but lower overall perceptions of patient safety than nonmedical staff. These findings implied that hospital administrators/managers differ in their perceptions of the volume and efficacy of error reporting, and their contribution to PSC. These findings are consistent with other research findings suggesting that positive safety settings are associated with increased reporting of medication errors and greater willingness of professionals to advocate for patient safety [
27,
38,
56,
58].
Finally, overall perceptions of patient safety showed a significantly negative relationship with the frequency of event reporting. This negative relationship might be due to many reasons, such as the use of self-reported surveys and a blaming culture. Therefore, hospital executives must create cultures in which employees learn from their mistakes, which may increase reporting errors. This finding is consistent with research indicating negative relationships between overall safety culture and patient safety outcomes. For example, hospitals with positive PSC scores have lower rates of in-hospital complications or AEs [
27]. In addition, another study has found that a higher safety culture is associated with lower rates of hospital-acquired pressure ulcers [
59], and fewer medication or dislodgement errors [
60].
4.2. Limitations
The present study has several important limitations. The study design included several limitations inherent to the use of secondary data. This was a cross-sectional study including only hospitals that independently administered the survey in the database according to AHRQ’s requirements. The submitting hospitals are not representative of all U.S. hospitals, because they are not a random sample; only approximately 10% of all hospitals chose to participate. Estimates based on this self-selected group might yield biased population estimates, and precise estimates cannot be computed from such a self-selected group. Another limitation was the way in which the surveys were conducted: verification that each hospital followed AHRQ’s data collection procedures could not be obtained, because the investigators overseeing survey distribution were not required to undergo any training. Moreover, another limitation is that the surveys were administered with a variety of methods. Hospitals used paper surveys, Web-based surveys, and a combination thereof. These different modes of administration might potentially have resulted in differences in survey responses; more research is needed to determine whether and how different administration modes affect the results. Finally, this study measured only the subjective overall perception of patient safety, and the frequency of event reporting, both of which were based on only the respondents’ perceptions as an estimate of reporting, rather than actual measurements.
4.3. Future Work
We recommend that nonteaching hospitals develop education and training programs for medical and nonmedical staff, collect and statistically analyze error data, and redesign systems to improve PSC, all which can directly decrease the rates of medical errors. This study focused on the perceptions of medical and nonmedical staff. We suggest that future research should focus on nonmedical staff. Hospital administrators and mangers can improve PSC by understanding hospital settings and developing policies and care practices that support programs such as Team Strategies and Tools to Enhance Performance and Patient Safety (TeamSTEPPS®). TeamSTEPPS® is a set of evidence-based teamwork tools designed to improve patient outcomes by optimizing interprofessional team functions.
Furthermore, future research should also explore other hospital and respondent characteristics, such as bed size, ownership, and work experience, to establish their effects on perceptions of PSC. This study measured only the subjective overall perception of patient safety and the frequency of event reporting. A future study could include both subjective and objective patient safety indicators. A longitudinal study design including more healthcare professionals and practitioners would be beneficial to increase data reliability.


 ,
, 




{kind=link}
{kind=link}