
Anxiety Linked to COVID-19: A Systematic Review Comparing Anxiety Rates in Different Populations





Abstract
:1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Literature Search
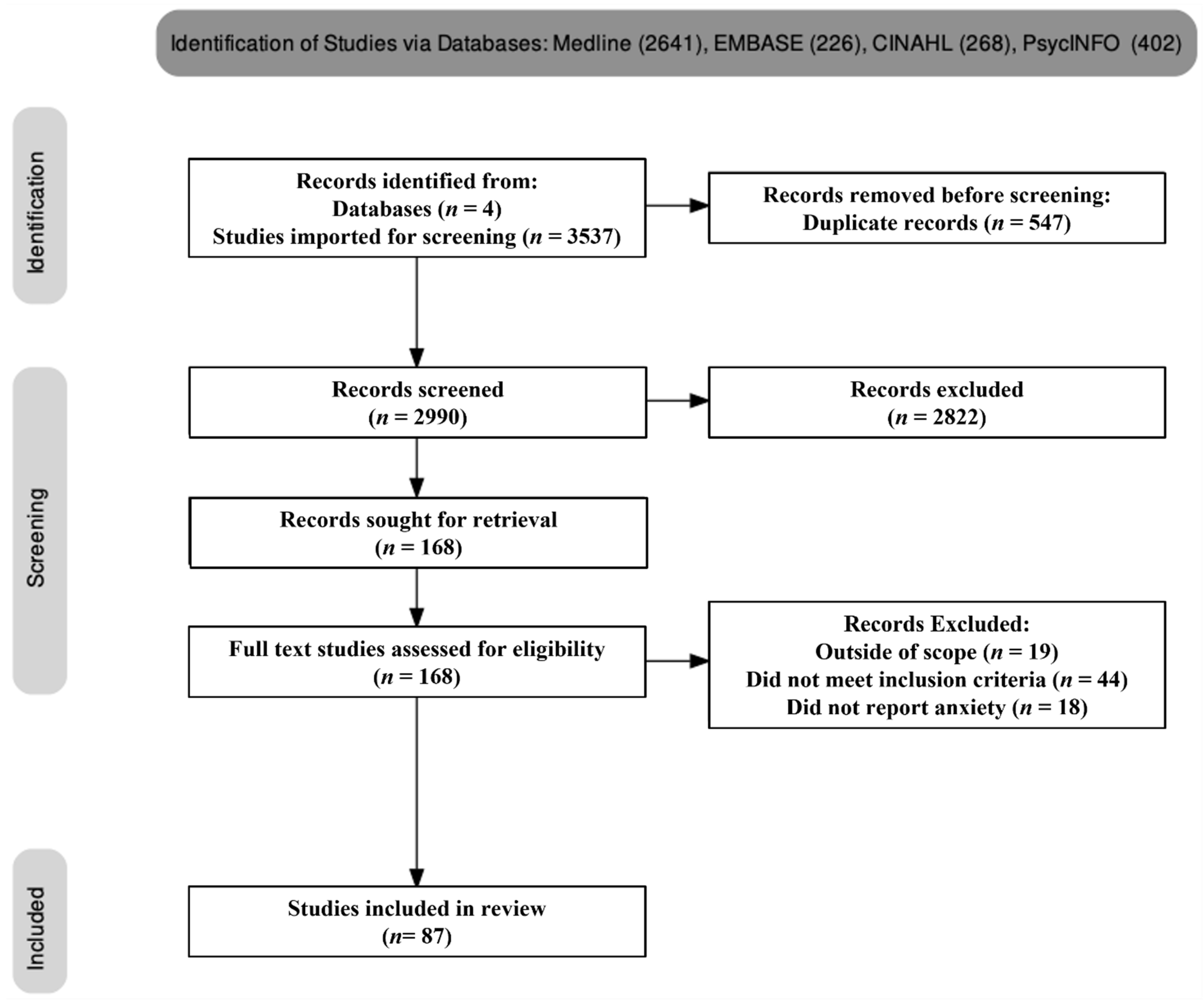
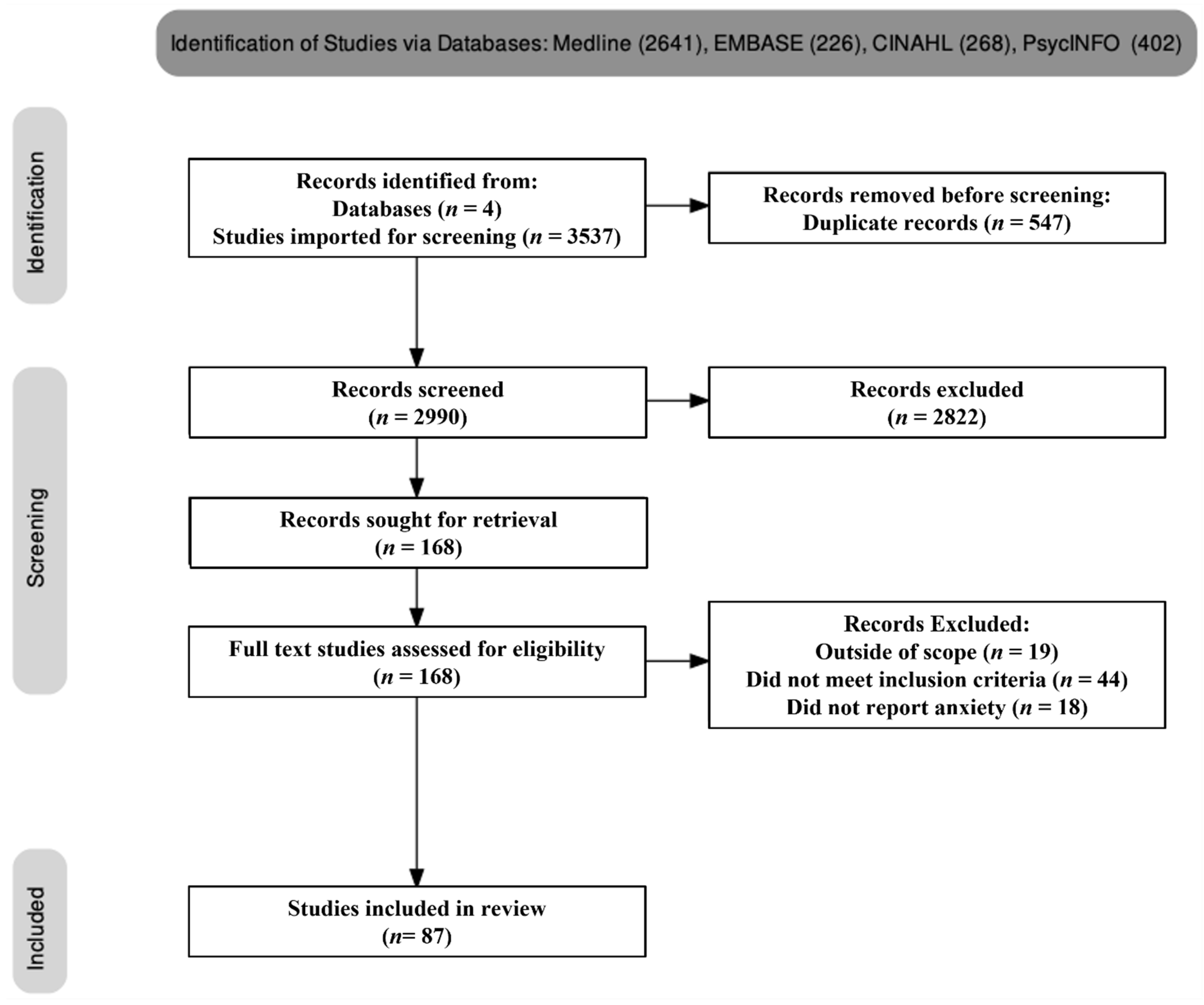
2.3. Study Selection
2.4. Quality Assessment
2.5. Data Extraction and Synthesis
3. Results
3.1. Study Characteristics
3.2. The General Population Group
3.3. Healthcare Worker Group
3.4. University Students
3.4.1. Other Adults of the General Population
Anxiety in Parents
Anxiety in Teachers
Anxiety in the Elderly Population
Anxiety in Police
Anxiety in Pregnant Women
4. Discussion
4.1. Anxiety before and after COVID-19
4.2. Anxiety in Different Populations during COVID-19
4.2.1. Anxiety in the General Population
4.2.2. Anxiety in Healthcare Workers
4.2.3. Anxiety in University Students
4.2.4. Anxiety in Other Adults of the General Population
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Publishing, Inc.: Arlington, VA, USA, 2013. [Google Scholar]
- Niles, A.N.; Dour, H.J.; Stanton, A.L.; Roy-Byrne, P.P.; Stein, M.B.; Sullivan, G.; Sherbourne, C.D.; Rose, R.D.; Craske, M.G. Anxiety and depressive symptoms and medical illness among adults with anxiety disorders. J. Psychosom. Res. 2015, 78, 109–115. [Google Scholar] [CrossRef] [Green Version]
- Roest Annelieke, M.; Martens Elisabeth, J.; de Jonge, P.; Denollet, J. Anxiety and Risk of Incident Coronary Heart Disease. J. Am. Coll. Cardiol. 2010, 56, 38–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 15 August 2021).
- Locatelli, I.; Trächsel, B.; Rousson, V. Estimating the basic reproduction number for COVID-19 in Western Europe. PLoS ONE 2021, 16, e0248731. [Google Scholar] [CrossRef] [PubMed]
- Alimohamadi, Y.; Taghdir, M.; Sepandi, M. Estimate of the Basic Reproduction Number for COVID-19: A Systematic Review and Meta-analysis. J. Prev. Med. Public Health 2020, 53, 151–157. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.-Y.; Yang, Y.-Z.; Zhang, X.-M.; Xu, X.; Dou, Q.-L.; Zhang, W.-W.; Cheng, A.S.K. The prevalence and influencing factors in anxiety in medical workers fighting COVID-19 in China: A cross-sectional survey. Epidemiol. Infect. 2020, 148, 1–17. [Google Scholar] [CrossRef]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef]
- Lee, A.M.; Wong, J.G.W.S.; McAlonan, G.M.; Cheung, V.; Cheung, C.; Sham, P.C.; Chu, C.-M.; Wong, P.-C.; Tsang, K.W.T.; Chua, S.E. Stress and psychological distress among SARS survivors 1 year after the outbreak. Can. J. Psychiatry 2007, 52, 233–240. [Google Scholar] [CrossRef] [Green Version]
- Lehmann, M.; Bruenahl, C.A.; Addo, M.M.; Becker, S.; Schmiedel, S.; Lohse, A.W.; Schramm, C.; Lowe, B. Acute Ebola virus disease patient treatment and health-related quality of life in health care professionals: A controlled study. J. Psychosom. Res. 2016, 83, 69–74. [Google Scholar] [CrossRef]
- Bendau, A.; Plag, J.; Kunas, S.; Wyka, S.; Strohle, A.; Petzold, M.B. Longitudinal changes in anxiety and psychological distress, and associated risk and protective factors during the first three months of the COVID-19 pandemic in Germany. Brain Behav. 2021, 11, e01964. [Google Scholar] [CrossRef]
- ABS. Labour Force, Australia. Available online: https://www.abs.gov.au/statistics/labour/employment-and-unemployment/labour-force-australia/jul-2020 (accessed on 3 September 2021).
- Pierce, M.; Hope, H.; Ford, T.; Hatch, S.; Hotopf, M.; John, A.; Kontopantelis, E.; Webb, R.; Wessely, S.; McManus, S.; et al. Mental health before and during the COVID-19 pandemic: A longitudinal probability sample survey of the UK population. Lancet Psychiatry 2020, 7, 883–892. [Google Scholar] [CrossRef]
- Wu, T.; Jia, X.; Shi, H.; Niu, J.; Yin, X.; Xie, J.; Wang, X. Prevalence of mental health problems during the COVID-19 pandemic: A systematic review and meta-analysis. J. Affect. Disord. 2021, 281, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Chou, K.-R.; Huang, Y.-J.; Wang, T.-S.; Liu, S.-Y.; Ho, L.-Y. Effects of a SARS prevention programme in Taiwan on nursing staff’s anxiety, depression and sleep quality: A longitudinal survey. Int. J. Nurs. Stud. 2006, 43, 215–225. [Google Scholar] [CrossRef] [PubMed]
- Lancee, W.J.; Maunder, R.G.; Goldbloom, D.S. Prevalence of Psychiatric Disorders Among Toronto Hospital Workers One to Two Years After the SARS Outbreak. Psychiatr. Serv. 2008, 59, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Mak, I.W.C.; Chu, C.M.; Pan, P.C.; Yiu, M.G.C.; Chan, V.L. Long-term psychiatric morbidities among SARS survivors. Gen. Hosp. Psychiatry 2009, 31, 318–326. [Google Scholar] [CrossRef]
- Bohlken, J.; Kostev, K.; Riedel-Heller, S.; Hoffmann, W.; Michalowsky, B. Effect of the COVID-19 pandemic on stress, anxiety, and depressive disorders in German primary care: A cross-sectional study. J. Psychiatr. Res. 2021, 143, 43–49. [Google Scholar] [CrossRef]
- Daly, M.; Sutin, A.R.; Robinson, E. Longitudinal changes in mental health and the COVID-19 pandemic: Evidence from the UK Household Longitudinal Study. Psychol. Med. 2020, 1, 1–10. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Dixon-Woods, M.; Fitzpatrick, R.; Roberts, K. Including qualitative research in systematic reviews: Opportunities and problems. J. Eval. Clin. Pr. 2001, 7, 125–133. [Google Scholar] [CrossRef]
- Turner, R.M.; Bird, S.M.; Higgins, J.P. The impact of study size on meta-analyses: Examination of underpowered studies in Cochrane reviews. PLoS ONE 2013, 8, e59202. [Google Scholar] [CrossRef]
- Munn, Z.; Tufanaru, C.; Aromataris, E. JBI’s Systematic Reviews: Data Extraction and Synthesis. AJN Am. J. Nurs. 2014, 114, 49–54. [Google Scholar] [CrossRef]
- Williams, N. The GAD-7 questionnaire. Occup. Med. 2014, 64, 224. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Fu, Z.; Bo, Q.; Mao, Z.; Ma, X.; Wang, C. The reliability and validity of PHQ-9 in patients with major depressive disorder in psychiatric hospital. BMC Psychiatry 2020, 20, 474. [Google Scholar] [CrossRef] [PubMed]
- Marteau, T.M.; Bekker, H. The development of a six-item short-form of the state scale of the Spielberger State—Trait Anxiety Inventory (STAI). Br. J. Clin. Psychol. 1992, 31, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Aharon, A.A.; Dubovi, I.; Ruban, A. Differences in mental health and health-related quality of life between the Israeli and Italian population during a COVID-19 quarantine. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2021, 30, 1675–1684. [Google Scholar] [CrossRef]
- Albagmi, F.M.; AlNujaidi, H.Y.; Al Shawan, D.S. Anxiety Levels Amid the COVID-19 Lockdown in Saudi Arabia. Int. J. Gen. Med. 2021, 14, 2161–2170. [Google Scholar] [CrossRef]
- Alshekaili, M.; Hassan, W.; Al Said, N.; Al Sulaimani, F.; Jayapal, S.K.; Al-Mawali, A.; Chan, M.F.; Mahadevan, S.; Al-Adawi, S. Factors associated with mental health outcomes across healthcare settings in Oman during COVID-19: Frontline versus non-frontline healthcare workers. BMJ Open 2020, 10, e042030. [Google Scholar] [CrossRef]
- Antonijevic, J.; Binic, I.; Zikic, O.; Manojlovic, S.; Tosic-Golubovic, S.; Popovic, N. Mental health of medical personnel during the COVID-19 pandemic. Brain Behav. 2020, 10, e01881. [Google Scholar] [CrossRef]
- Ausín, B.; González-Sanguino, C.; Castellanos, M.Á.; Muñoz, M. Gender-related differences in the psychological impact of confinement as a consequence of covid-19 in spain. J. Gend. Stud. 2020, 30, 29–38. [Google Scholar] [CrossRef]
- Batterham, P.J.; Calear, A.L.; McCallum, S.M.; Morse, A.R.; Banfield, M.; Farrer, L.M.; Gulliver, A.; Cherbuin, N.; Rodney Harris, R.M.; Shou, Y.; et al. Trajectories of depression and anxiety symptoms during the COVID-19 pandemic in a representative Australian adult cohort. Med. J. Aust. 2021, 214, 462–468. [Google Scholar] [CrossRef]
- Budimir, S.; Pieh, C.; Dale, R.; Probst, T. Severe Mental Health Symptoms during COVID-19: A Comparison of the United Kingdom and Austria. Healthcare 2021, 9, 191. [Google Scholar] [CrossRef]
- Cai, Q.; Feng, H.; Huang, J.; Wang, M.; Wang, Q.; Lu, X.; Xie, Y.; Wang, X.; Liu, Z.; Hou, B.; et al. The mental health of frontline and non-frontline medical workers during the coronavirus disease 2019 (COVID-19) outbreak in China: A case-control study. J. Affect. Disord. 2020, 275, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Canet-Juric, L.; Andres, M.L.; Del Valle, M.; Lopez-Morales, H.; Poo, F.; Galli, J.I.; Yerro, M.; Urquijo, S. A Longitudinal Study on the Emotional Impact Cause by the COVID-19 Pandemic Quarantine on General Population. Front. Psychol. 2020, 11, 565688. [Google Scholar] [CrossRef] [PubMed]
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Zhao, H.; Razin, D.; Song, T.; Wu, Y.; Ma, X.; HuerxidaAji; Wang, G.; Wang, M.; Yan, L. Anxiety levels during a second local COVID-19 pandemic breakout among quarantined people: A cross sectional survey in China. J. Psychiatr. Res. 2021, 135, 37–46. [Google Scholar] [CrossRef]
- Chew, N.W.S.; Ngiam, J.N.; Tan, B.Y.-Q.; Tham, S.-M.; Tan, C.Y.-S.; Jing, M.; Sagayanathan, R.; Chen, J.T.; Wong, L.Y.H.; Ahmad, A.; et al. Asian-Pacific perspective on the psychological well-being of healthcare workers during the evolution of the COVID-19 pandemic. BJPsych Open 2020, 6, e116. [Google Scholar] [CrossRef]
- Dawel, A.; Shou, Y.; Smithson, M.; Cherbuin, N.; Banfield, M.; Calear, A.L.; Farrer, L.M.; Gray, D.; Gulliver, A.; Housen, T.; et al. The Effect of COVID-19 on Mental Health and Wellbeing in a Representative Sample of Australian Adults. Front. Psychiatry 2020, 11, 579985. [Google Scholar] [CrossRef]
- Denning, M.; Goh, E.T.; Tan, B.; Kanneganti, A.; Almonte, M.; Scott, A.; Martin, G.; Clarke, J.; Sounderajah, V.; Markar, S.; et al. Determinants of burnout and other aspects of psychological well-being in healthcare workers during the COVID-19 pandemic: A multinational cross-sectional study. PLoS ONE 2021, 16, e0238666. [Google Scholar] [CrossRef]
- Di Blasi, M.; Gullo, S.; Mancinelli, E.; Freda, M.F.; Esposito, G.; Gelo, O.C.G.; Lagetto, G.; Giordano, C.; Mazzeschi, C.; Pazzagli, C.; et al. Psychological distress associated with the COVID-19 lockdown: A two-wave network analysis. J. Affect. Disord. 2021, 284, 18–26. [Google Scholar] [CrossRef]
- Di Giuseppe, M.; Zilcha-Mano, S.; Prout, T.A.; Perry, J.C.; Orru, G.; Conversano, C. Psychological Impact of Coronavirus Disease 2019 Among Italians During the First Week of Lockdown. Front. Psychiatry 2020, 11, 576597. [Google Scholar] [CrossRef]
- Di Mattei, V.E.; Perego, G.; Milano, F.; Mazzetti, M.; Taranto, P.; Di Pierro, R.; De Panfilis, C.; Madeddu, F.; Preti, E. The "Healthcare Workers’ Wellbeing (Benessere Operatori)" Project: A Picture of the Mental Health Conditions of Italian Healthcare Workers during the First Wave of the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 5267. [Google Scholar] [CrossRef]
- Fiorillo, A.; Sampogna, G.; Giallonardo, V.; Del Vecchio, V.; Luciano, M.; Albert, U.; Carmassi, C.; Carra, G.; Cirulli, F.; Dell’Osso, B.; et al. Effects of the lockdown on the mental health of the general population during the COVID-19 pandemic in Italy: Results from the COMET collaborative network. Eur. Psychiatry J. Assoc. Eur. Psychiatr. 2020, 63, e87. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J.R.; Tran, T.D.; Hammarberg, K.; Sastry, J.; Nguyen, H.; Rowe, H.; Popplestone, S.; Stocker, R.; Stubber, C.; Kirkman, M. Mental health of people in Australia in the first month of COVID-19 restrictions: A national survey. Med. J. Aust. 2020, 213, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Fu, W.; Wang, C.; Zou, L.; Guo, Y.; Lu, Z.; Yan, S.; Mao, J. Psychological health, sleep quality, and coping styles to stress facing the COVID-19 in Wuhan, China. Transl. Psychiatry 2020, 10, 225. [Google Scholar] [CrossRef] [PubMed]
- Fu, W.; Yan, S.; Zong, Q.; Anderson-Luxford, D.; Song, X.; Lv, Z.; Lv, C. Mental health of college students during the COVID-19 epidemic in China. J. Affect. Disord. 2021, 280, 7–10. [Google Scholar] [CrossRef]
- Gainer, D.M.; Nahhas, R.W.; Bhatt, N.V.; Merrill, A.; McCormack, J. Association Between Proportion of Workday Treating COVID-19 and Depression, Anxiety, and PTSD Outcomes in US Physicians. J. Occup. Environ. Med. 2021, 63, 89–97. [Google Scholar] [CrossRef]
- Garcia-Fernandez, L.; Romero-Ferreiro, V.; Lopez-Roldan, P.D.; Padilla, S.; Rodriguez-Jimenez, R. Mental Health in Elderly Spanish People in Times of COVID-19 Outbreak. Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2020, 28, 1040–1045. [Google Scholar] [CrossRef]
- Garcia-Fernandez, L.; Romero-Ferreiro, V.; Padilla, S.; David Lopez-Roldan, P.; Monzo-Garcia, M.; Rodriguez-Jimenez, R. Gender differences in emotional response to the COVID-19 outbreak in Spain. Brain Behav. 2021, 11, e01934. [Google Scholar] [CrossRef]
- Giardino, D.L.; Huck-Iriart, C.; Riddick, M.; Garay, A. The endless quarantine: The impact of the COVID-19 outbreak on healthcare workers after three months of mandatory social isolation in Argentina. Sleep Med. 2020, 76, 16–25. [Google Scholar] [CrossRef]
- Gundogmus, I.; Unsal, C.; Bolu, A.; Takmaz, T.; Okten, S.B.; Aydin, M.B.; Ucar, H.; Gunduz, A.; Kul, A.T. The comparison of anxiety, depression and stress symptoms levels of healthcare workers between the first and second COVID-19 peaks. Psychiatry Res. 2021, 301, 113976. [Google Scholar] [CrossRef]
- Hacimusalar, Y.; Kahve, A.C.; Yasar, A.B.; Aydin, M.S. Anxiety and hopelessness levels in COVID-19 pandemic: A comparative study of healthcare professionals and other community sample in Turkey. J. Psychiatr. Res. 2020, 129, 181–188. [Google Scholar] [CrossRef]
- Halperin, S.J.; Henderson, M.N.; Prenner, S.; Grauer, J.N. Prevalence of Anxiety and Depression Among Medical Students During the Covid-19 Pandemic: A Cross-Sectional Study. J. Med. Educ. Curric. Dev. 2021, 8, 2382120521991150. [Google Scholar] [CrossRef] [PubMed]
- Hammarberg, K.; Tran, T.; Kirkman, M.; Fisher, J. Sex and age differences in clinically significant symptoms of depression and anxiety among people in Australia in the first month of COVID-19 restrictions: A national survey. BMJ Open 2020, 10, e042696. [Google Scholar] [CrossRef] [PubMed]
- Hassannia, L.; Taghizadeh, F.; Moosazadeh, M.; Zarghami, M.; Taghizadeh, H.; Dooki, A.F.; Fathi, M.; Alizadeh-Navaei, R.; Hedayatizadeh-Omran, A.; Dehghan, N. Anxiety and Depression in Health Workers and General Population During COVID-19 in IRAN: A Cross-Sectional Study. Neuropsychopharmacol. Rep. 2021, 41, 40–49. [Google Scholar] [CrossRef] [PubMed]
- He, Q.; Ren, J.; Wang, G.; Zhang, J.; Xiang, J.; He, D. Psychological effects of the COVID-19 outbreak on nurses working in tertiary women’s and children’s hospitals from Sichuan, China: A cross-sectional study. Int. J. Disaster Risk Reduct. IJDRR 2021, 58, 102188. [Google Scholar] [CrossRef]
- Hennein, R.; Mew, E.J.; Lowe, S.R. Socio-ecological predictors of mental health outcomes among healthcare workers during the COVID-19 pandemic in the United States. PLoS ONE 2021, 16, e0246602. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Liu, F.; Teng, Z.; Chen, J.; Zhao, J.; Wang, X.; Wu, Y.; Xiao, J.; Wang, Y.; Wu, R. Public behavior change, perceptions, depression, and anxiety in relation to the COVID-19 outbreak. Open Forum Infect. Dis. 2020, 7, ofaa273. [Google Scholar] [CrossRef] [PubMed]
- IslamI, M.S.; Sujan, M.S.H.; Tasnim, R.; Sikder, M.T.; Potenza, M.N.; van Os, J. Psychological responses during the COVID-19 outbreak among university students in Bangladesh. PLoS ONE 2020, 15, e0245083. [Google Scholar] [CrossRef]
- Jacques-Avino, C.; Lopez-Jimenez, T.; Medina-Perucha, L.; de Bont, J.; Goncalves, A.Q.; Duarte-Salles, T.; Berenguera, A. Gender-based approach on the social impact and mental health in Spain during COVID-19 lockdown: A cross-sectional study. BMJ Open 2020, 10, e044617. [Google Scholar] [CrossRef]
- Jia, R.; Ayling, K.; Chalder, T.; Massey, A.; Broadbent, E.; Coupland, C.; Vedhara, K. Mental health in the UK during the COVID-19 pandemic: Cross-sectional analyses from a community cohort study. BMJ Open 2020, 10, e040620. [Google Scholar] [CrossRef]
- Jiang, W.; Liu, X.; Zhang, J.; Feng, Z. Mental health status of Chinese residents during the COVID-19 epidemic. BMC Psychiatry 2020, 20, 580. [Google Scholar] [CrossRef]
- Johnson, M.S.; Skjerdingstad, N.; Ebrahimi, O.V.; Hoffart, A.; Urnes Johnson, S. Mechanisms of parental distress during and after the first COVID-19 lockdown phase: A two-wave longitudinal study. PLoS ONE 2021, 16, e0253087. [Google Scholar] [CrossRef] [PubMed]
- Kantor, B.N.; Kantor, J. Mental Health Outcomes and Associations During the COVID-19 Pandemic: A Cross-Sectional Population-Based Study in the United States. Front. Psychiatry 2020, 11, 569083. [Google Scholar] [CrossRef] [PubMed]
- Karaivazoglou, K.; Konstantopoulou, G.; Kalogeropoulou, M.; Iliou, T.; Vorvolakos, T.; Assimakopoulos, K.; Gourzis, P.; Alexopoulos, P. Psychological distress in the Greek general population during the first COVID-19 lockdown. BJPsych Open 2021, 7, e59. [Google Scholar] [CrossRef] [PubMed]
- Khubchandani, J.; Sharma, S.; Webb, F.J.; Wiblishauser, M.J.; Bowman, S.L. Post-lockdown depression and anxiety in the USA during the COVID-19 pandemic. J. Public Health (Oxf. Engl.) 2021, 43, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Rackoff, G.N.; Zainal, N.H.; Schwob, J.T.; Newman, M.G.; Fitzsimmons-Craft, E.E.; Wilfley, D.E.; Shin, K.E.; Eisenberg, D.; Taylor, C.B. College Mental Health Before and During the COVID-19 Pandemic: Results From a Nationwide Survey. Cogn. Ther. Res. 2021, 46, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors Associated With Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef]
- Lei, L.; Huang, X.; Zhang, S.; Yang, J.; Yang, L.; Xu, M. Comparison of Prevalence and Associated Factors of Anxiety and Depression Among People Affected by versus People Unaffected by Quarantine During the COVID-19 Epidemic in Southwestern China. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2020, 26, e924609. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Miao, Y.; Zeng, X.; Tarimo, C.S.; Wu, C.; Wu, J. Prevalence and factors for anxiety during the coronavirus disease 2019 (COVID-19) epidemic among the teachers in China. J. Affect. Disord. 2020, 277, 153–158. [Google Scholar] [CrossRef]
- Li, W.W.; Li, Y.; Yu, H.; Miller, D.J.; Rouen, C.; Yang, F. Mental Health of Chinese People During the COVID-19 Pandemic: Associations With Infection Severity of Region of Residence and Filial Piety. Front. Psychol. 2021, 12, 633452. [Google Scholar] [CrossRef]
- Liu, Y.; Chen, H.; Zhang, N.; Wang, X.; Fan, Q.; Zhang, Y.; Huang, L.; Hu, B.; Li, M. Anxiety and depression symptoms of medical staff under COVID-19 epidemic in China. J. Affect. Disord. 2021, 278, 144–148. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, L.; Chen, L.; Zhang, X.; Bao, L.; Shi, Y. Mental Health Status of Paediatric Medical Workers in China During the COVID-19 Outbreak. Front. Psychiatry 2020, 11, 702. [Google Scholar] [CrossRef] [PubMed]
- Lu, P.; Li, X.; Lu, L.; Zhang, Y. The psychological states of people after Wuhan eased the lockdown. PLoS ONE 2020, 15, e0241173. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.; Wang, H.; Lin, Y.; Li, L. Psychological status of medical workforce during the COVID-19 pandemic: A cross-sectional study. Psychiatry Res. 2020, 288, 112936. [Google Scholar] [CrossRef]
- Luceno-Moreno, L.; Talavera-Velasco, B.; Garcia-Albuerne, Y.; Martin-Garcia, J. Symptoms of Posttraumatic Stress, Anxiety, Depression, Levels of Resilience and Burnout in Spanish Health Personnel during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 5514. [Google Scholar] [CrossRef] [PubMed]
- Mattila, E.; Peltokoski, J.; Neva, M.H.; Kaunonen, M.; Helminen, M.; Parkkila, A.-K. COVID-19: Anxiety among hospital staff and associated factors. Ann. Med. 2021, 53, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Meesala, N.; Harsha, G.; Kandikatla, P.; Karteekvarma, P.V.; Nadakuditi, S.R.; Kakaraparthi, S.K. Measuring the impact of COVID-19 on mental health as a preliminary procedure in primary care provision: A cross-sectional study using COVID-19 anxiety scale. J. Fam. Med. Prim. Care 2020, 9, 5554–5558. [Google Scholar] [CrossRef]
- Mosheva, M.; Hertz-Palmor, N.; Dorman Ilan, S.; Matalon, N.; Pessach, I.M.; Afek, A.; Ziv, A.; Kreiss, Y.; Gross, R.; Gothelf, D. Anxiety, pandemic-related stress and resilience among physicians during the COVID-19 pandemic. Depress. Anxiety 2020, 37, 965–971. [Google Scholar] [CrossRef]
- Ngoc Cong Duong, K.; Nguyen Le Bao, T.; Thi Lan Nguyen, P.; Vo Van, T.; Phung Lam, T.; Pham Gia, A.; Anuratpanich, L.; Vo Van, B. Psychological Impacts of COVID-19 During the First Nationwide Lockdown in Vietnam: Web-Based, Cross-Sectional Survey Study. JMIR Form. Res. 2020, 4, e24776. [Google Scholar] [CrossRef]
- Nkire, N.; Mrklas, K.; Hrabok, M.; Gusnowski, A.; Vuong, W.; Surood, S.; Abba-Aji, A.; Urichuk, L.; Cao, B.; Greenshaw, A.J.; et al. COVID-19 Pandemic: Demographic Predictors of Self-Isolation or Self-Quarantine and Impact of Isolation and Quarantine on Perceived Stress, Anxiety, and Depression. Front. Psychiatry 2021, 12, 553468. [Google Scholar] [CrossRef]
- Odriozola-Gonzalez, P.; Planchuelo-Gomez, A.; Irurtia, M.J.; de Luis-Garcia, R. Psychological effects of the COVID-19 outbreak and lockdown among students and workers of a Spanish university. Psychiatry Res. 2020, 290, 113108. [Google Scholar] [CrossRef]
- Ozamiz-Etxebarria, N.; Berasategi Santxo, N.; Idoiaga Mondragon, N.; Dosil Santamaria, M. The Psychological State of Teachers During the COVID-19 Crisis: The Challenge of Returning to Face-to-Face Teaching. Front. Psychol. 2020, 11, 620718. [Google Scholar] [CrossRef] [PubMed]
- Ozamiz-Etxebarria, N.; Idoiaga Mondragon, N.; Dosil Santamaria, M.; Picaza Gorrotxategi, M. Psychological Symptoms During the Two Stages of Lockdown in Response to the COVID-19 Outbreak: An Investigation in a Sample of Citizens in Northern Spain. Front. Psychol. 2020, 11, 1491. [Google Scholar] [CrossRef] [PubMed]
- Pandey, D.; Bansal, S.; Goyal, S.; Garg, A.; Sethi, N.; Pothiyill, D.I.; Sreelakshmi, E.S.; Sayyad, M.G.; Sethi, R. Psychological impact of mass quarantine on population during pandemics-The COVID-19 Lock-Down (COLD) study. PLoS ONE 2020, 15, e0240501. [Google Scholar] [CrossRef] [PubMed]
- Passavanti, M.; Argentieri, A.; Barbieri, D.M.; Lou, B.; Wijayaratna, K.; Foroutan Mirhosseini, A.S.; Wang, F.; Naseri, S.; Qamhia, I.; Tangeras, M.; et al. The psychological impact of COVID-19 and restrictive measures in the world. J. Affect. Disord. 2021, 283, 36–51. [Google Scholar] [CrossRef]
- Pieh, C.; Budimir, S.; Delgadillo, J.; Barkham, M.; Fontaine, J.R.J.; Probst, T. Mental Health During COVID-19 Lockdown in the United Kingdom. Psychosom. Med. 2021, 83, 328–337. [Google Scholar] [CrossRef]
- Pieh, C.; Budimir, S.; Probst, T. The effect of age, gender, income, work, and physical activity on mental health during coronavirus disease (COVID-19) lockdown in Austria. J. Psychosom. Res. 2020, 136, 110186. [Google Scholar] [CrossRef]
- Planchuelo-Gomez, A.; Odriozola-Gonzalez, P.; Irurtia, M.J.; de Luis-Garcia, R. Longitudinal evaluation of the psychological impact of the COVID-19 crisis in Spain. J. Affect. Disord. 2020, 277, 842–849. [Google Scholar] [CrossRef]
- Robb, C.E.; de Jager, C.A.; Ahmadi-Abhari, S.; Giannakopoulou, P.; Udeh-Momoh, C.; McKeand, J.; Price, G.; Car, J.; Majeed, A.; Ward, H.; et al. Associations of Social Isolation with Anxiety and Depression During the Early COVID-19 Pandemic: A Survey of Older Adults in London, UK. Front. Psychiatry 2020, 11, 591120. [Google Scholar] [CrossRef]
- Rossi, R.; Socci, V.; Pacitti, F.; Mensi, S.; Di Marco, A.; Siracusano, A.; Di Lorenzo, G. Mental Health Outcomes Among Healthcare Workers and the General Population During the COVID-19 in Italy. Front. Psychol. 2020, 11, 608986. [Google Scholar] [CrossRef]
- Ruengorn, C.; Awiphan, R.; Wongpakaran, N.; Wongpakaran, T.; Nochaiwong, S.; Health, O.; Mental Health Care Evaluation Survey Research, G. Association of job loss, income loss, and financial burden with adverse mental health outcomes during coronavirus disease 2019 pandemic in Thailand: A nationwide cross-sectional study. Depress. Anxiety 2021, 38, 648–660. [Google Scholar] [CrossRef]
- Serafim, A.P.; Duraes, R.S.S.; Rocca, C.C.A.; Goncalves, P.D.; Saffi, F.; Cappellozza, A.; Paulino, M.; Dumas-Diniz, R.; Brissos, S.; Brites, R.; et al. Exploratory study on the psychological impact of COVID-19 on the general Brazilian population. PLoS ONE 2021, 16, e0245868. [Google Scholar] [CrossRef] [PubMed]
- Shen, M.; Xu, H.; Fu, J.; Wang, T.; Fu, Z.; Zhao, X.; Zhou, G.; Jin, Q.; Tong, G. Investigation of anxiety levels of 1637 healthcare workers during the epidemic of COVID-19. PLoS ONE 2020, 15, e0243890. [Google Scholar] [CrossRef] [PubMed]
- Sinawi, H.A.; Al Balushi, N.; Al-Mahrouqi, T.; Al Ghailani, A.; McCall, R.K.; Sultan, A.; Al Sabti, H.; Al Maniri, A.; Murthi Panchatcharam, S.; Al-Alawi, M. Predictors of psychological distress among the public in Oman amid coronavirus disease 2019 pandemic: A cross-sectional analytical study. Psychol. Health Med. 2021, 26, 131–144. [Google Scholar] [CrossRef]
- Solomou, I.; Constantinidou, F. Prevalence and Predictors of Anxiety and Depression Symptoms during the COVID-19 Pandemic and Compliance with Precautionary Measures: Age and Sex Matter. Int. J. Environ. Res. Public Health 2020, 17, 4924. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Goldberg, S.B.; Lin, D.; Qiao, S.; Operario, D. Psychiatric symptoms, risk, and protective factors among university students in quarantine during the COVID-19 pandemic in China. Glob. Health 2021, 17, 15. [Google Scholar] [CrossRef] [PubMed]
- Tang, F.; Liang, J.; Zhang, H.; Kelifa, M.M.; He, Q.; Wang, P. Covid-19 related depression and anxiety among quarantined respondents. Psychol. Health 2020, 36, 164–178. [Google Scholar] [CrossRef]
- van der Velden, P.G.; Contino, C.; Das, M.; van Loon, P.; Bosmans, M.W.G. Anxiety and depression symptoms, and lack of emotional support among the general population before and during the COVID-19 pandemic. A prospective national study on prevalence and risk factors. J. Affect. Disord. 2020, 277, 540–548. [Google Scholar] [CrossRef]
- Wang, C.; Song, W.; Hu, X.; Yan, S.; Zhang, X.; Wang, X.; Chen, W. Depressive, anxiety, and insomnia symptoms between population in quarantine and general population during the COVID-19 pandemic: A case-controlled study. BMC Psychiatry 2021, 21, 99. [Google Scholar] [CrossRef]
- Wang, X.; Tao, J.; Zhu, Q.; Wu, X.; Li, T.; Zhao, C.; Yang, W.; Wang, X.; Zhang, J.; Guan, N. Depression and anxiety symptoms to COVID-19 outbreak among the public, medical staff and patients during the initial phase of the pandemic: An online questionnaire survey by a WeChat Mini Program. BMJ Open 2021, 11, e046350. [Google Scholar] [CrossRef]
- Wang, Y.; Kala, M.P.; Jafar, T.H. Factors associated with psychological distress during the coronavirus disease 2019 (COVID-19) pandemic on the predominantly general population: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0244630. [Google Scholar] [CrossRef]
- Wanigasooriya, K.; Palimar, P.; Naumann, D.N.; Ismail, K.; Fellows, J.L.; Logan, P.; Thompson, C.V.; Bermingham, H.; Beggs, A.D.; Ismail, T. Mental health symptoms in a cohort of hospital healthcare workers following the first peak of the COVID-19 pandemic in the UK. BJPsych Open 2020, 7, e24. [Google Scholar] [CrossRef] [PubMed]
- Warren, A.M.; Zolfaghari, K.; Fresnedo, M.; Bennett, M.; Pogue, J.; Waddimba, A.; Zvolensky, M.; Carlbring, P.; Powers, M.B. Anxiety sensitivity, COVID-19 fear, and mental health: Results from a United States population sample. Cogn. Behav. Ther. 2021, 50, 204–216. [Google Scholar] [CrossRef]
- Wathelet, M.; Duhem, S.; Vaiva, G.; Baubet, T.; Habran, E.; Veerapa, E.; Debien, C.; Molenda, S.; Horn, M.; Grandgenevre, P.; et al. Factors Associated With Mental Health Disorders Among University Students in France Confined During the COVID-19 Pandemic. JAMA Netw. Open 2020, 3, e2025591. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Han, H.; Lin, T.; Chen, M.; Wu, J.; Du, X.; Su, G.; Wu, D.; Chen, F.; Zhang, Q.; et al. Prevalence and risk factors of mental distress in China during the outbreak of COVID-19: A national cross-sectional survey. Brain Behav. 2020, 10, e01818. [Google Scholar] [CrossRef] [PubMed]
- Yuan, L.; Zhu, L.; Chen, F.; Cheng, Q.; Yang, Q.; Zhou, Z.Z.; Zhu, Y.; Wu, Y.; Zhou, Y.; Zha, X. A Survey of Psychological Responses During the Coronavirus Disease 2019 (COVID-19) Epidemic among Chinese Police Officers in Wuhu. Risk Manag. Healthc. Policy 2020, 13, 2689–2697. [Google Scholar] [CrossRef]
- Zhang, L.; Wang, S.; Shen, J.; Wang, Y.; Huang, X.; Wu, F.; Zheng, X.; Zeng, P.; Qiu, D. The mental health of Chinese healthcare staff in non-epicenter of COVID-19: A cross-sectional study. Ann. Palliat. Med. 2020, 9, 4127–4136. [Google Scholar] [CrossRef]
- Zhang, X.-R.; Huang, Q.-M.; Wang, X.-M.; Cheng, X.; Li, Z.-H.; Wang, Z.-H.; Zhong, W.-F.; Liu, D.; Shen, D.; Chen, P.-L.; et al. Prevalence of anxiety and depression symptoms, and association with epidemic-related factors during the epidemic period of COVID-19 among 123,768 workers in China: A large cross-sectional study. J. Affect. Disord. 2020, 277, 495–502. [Google Scholar] [CrossRef]
- Zhou, Y.; Wang, W.; Sun, Y.; Qian, W.; Liu, Z.; Wang, R.; Qi, L.; Yang, J.; Song, X.; Zhou, X.; et al. The prevalence and risk factors of psychological disturbances of frontline medical staff in china under the COVID-19 epidemic: Workload should be concerned. J. Affect. Disord. 2020, 277, 510–514. [Google Scholar] [CrossRef]
- Zilver, S.J.M.; Broekman, B.F.P.; Hendrix, Y.M.G.A.; de Leeuw, R.A.; Mentzel, S.V.; van Pampus, M.G.; de Groot, C.J.M. Stress, anxiety and depression in 1466 pregnant women during and before the COVID-19 pandemic: A Dutch cohort study. J. Psychosom. Obstet. Gynaecol. 2021, 42, 108–114. [Google Scholar] [CrossRef]
- Huang, H.L.; Chen, R.C.; Teo, I.; Chaudhry, I.; Heng, A.L.; Zhuang, K.D.; Tan, H.K.; Tan, B.S. A survey of anxiety and burnout in the radiology workforce of a tertiary hospital during the COVID-19 pandemic. J. Med. Imaging Radiat. Oncol. 2021, 65, 139–145. [Google Scholar] [CrossRef]
- Johns, G.; Samuel, V.; Freemantle, L.; Lewis, J.; Waddington, L. The global prevalence of depression and anxiety among doctors during the covid-19 pandemic: Systematic review and meta-analysis. J. Affect. Disord. 2022, 298, 431–441. [Google Scholar] [CrossRef] [PubMed]
- Drazen, J.M.; Kanapathipillai, R.; Campion, E.W.; Rubin, E.J.; Hammer, S.M.; Morrissey, S.; Baden, L.R. Ebola and Quarantine. N. Engl. J. Med. 2014, 371, 2029–2030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reynolds, D.L.; Garay, J.R.; Deamond, S.L.; Moran, M.K.; Gold, W.; Styra, R. Understanding, compliance and psychological impact of the SARS quarantine experience. Epidemiol. Infect. 2008, 136, 997–1007. [Google Scholar] [CrossRef] [PubMed]
- Santabárbara, J.; Lasheras, I.; Lipnicki, D.M.; Bueno-Notivol, J.; Pérez-Moreno, M.; López-Antón, R.; De La Cámara, C.; Lobo, A.; Gracia-García, P. Prevalence of anxiety in the COVID-19 pandemic: An updated meta-analysis of community-based studies. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 109, 110207. [Google Scholar] [CrossRef]
- Sharma, K.; Saji, J.; Kumar, R.; Raju, A. Psychological and Anxiety/Depression Level Assessment among Quarantine People during Covid19 Outbreak. J. Drug Deliv. Ther. 2020, 10, 198–201. [Google Scholar] [CrossRef]
- Qian, M.; Wu, Q.; Wu, P.; Hou, Z.; Liang, Y.; Cowling, B.J.; Yu, H. Anxiety levels, precautionary behaviours and public perceptions during the early phase of the COVID-19 outbreak in China: A population-based cross-sectional survey. BMJ Open 2020, 10, e040910. [Google Scholar] [CrossRef] [PubMed]
- AIHW. COVID-19 Impact on Mental Health. Available online: https://www.aihw.gov.au/reports/mental-health-services/mental-health-services-in-australia/report-contents/mental-health-impact-of-covid-19 (accessed on 2 October 2021).
- Hou, F.; Bi, F.; Jiao, R.; Luo, D.; Song, K. Gender differences of depression and anxiety among social media users during the COVID-19 outbreak in China:a cross-sectional study. BMC Public Health 2020, 20, 1648. [Google Scholar] [CrossRef]
- Korkmaz, S.; Kazgan, A.; Çekiç, S.; Tartar, A.S.; Balcı, H.N.; Atmaca, M. The anxiety levels, quality of sleep and life and problem-solving skills in healthcare workers employed in COVID-19 services. J. Clin. Neurosci. 2020, 80, 131–136. [Google Scholar] [CrossRef]
- Shevlin, M.; McBride, O.; Murphy, J.; Miller, J.G.; Hartman, T.K.; Levita, L.; Mason, L.; Martinez, A.P.; McKay, R.; Stocks, T.V.A.; et al. Anxiety, depression, traumatic stress and COVID-19-related anxiety in the UK general population during the COVID-19 pandemic. BJPsych Open 2020, 6, e125. [Google Scholar] [CrossRef]
- Goularte, J.F.; Serafim, S.D.; Colombo, R.; Hogg, B.; Caldieraro, M.A.; Rosa, A.R. COVID-19 and mental health in Brazil: Psychiatric symptoms in the general population. J. Psychiatr. Res. 2021, 132, 32–37. [Google Scholar] [CrossRef]
- Zhao, H.; He, X.; Fan, G.; Li, L.; Huang, Q.; Qiu, Q.; Kang, Z.; Du, T.; Han, L.; Ding, L.; et al. COVID-19 infection outbreak increases anxiety level of general public in China: Involved mechanisms and influencing factors. J. Affect. Disord. 2020, 276, 446–452. [Google Scholar] [CrossRef] [PubMed]
- Nikčević, A.V.; Marino, C.; Kolubinski, D.C.; Leach, D.; Spada, M.M. Modelling the contribution of the Big Five personality traits, health anxiety, and COVID-19 psychological distress to generalised anxiety and depressive symptoms during the COVID-19 pandemic. J. Affect. Disord. 2021, 279, 578–584. [Google Scholar] [CrossRef] [PubMed]
- Ran, L.; Wang, W.; Ai, M.; Kong, Y.; Chen, J.; Kuang, L. Psychological resilience, depression, anxiety, and somatization symptoms in response to COVID-19: A study of the general population in China at the peak of its epidemic. Soc. Sci. Med. 2020, 262, 113261. [Google Scholar] [CrossRef]
- Kharroubi, S.; Saleh, F. Are Lockdown Measures Effective Against COVID-19? Front. Public Health 2020, 8, 549692. [Google Scholar] [CrossRef]
- Özdin, S.; Bayrak Özdin, Ş. Levels and predictors of anxiety, depression and health anxiety during COVID-19 pandemic in Turkish society: The importance of gender. Int. J. Soc. Psychiatry 2020, 66, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Rey, R.; Garrido-Hernansaiz, H.; Collado, S. Psychological Impact and Associated Factors During the Initial Stage of the Coronavirus (COVID-19) Pandemic Among the General Population in Spain. Front. Psychol. 2020, 11, 1540. [Google Scholar] [CrossRef]
- Chatmon, B.N. Males and Mental Health Stigma. Am. J. Men’s Health 2020, 14, 155798832094932. [Google Scholar] [CrossRef]
- Nagasu, M.; Muto, K.; Yamamoto, I. Impacts of anxiety and socioeconomic factors on mental health in the early phases of the COVID-19 pandemic in the general population in Japan: A web-based survey. PLoS ONE 2021, 16, e0247705. [Google Scholar] [CrossRef]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef]
- Pashazadeh, F.; Raoofi, S.; Rafiei, S.; Khani, S.; Hosseinifard, H.; Tajik, F.; Raoofi, N.; Ahmadi, S.; Aghalou, S.; Torabi, F.; et al. A systematic review of the prevalence of anxiety among the general population during the COVID-19 pandemic. J. Affect. Disord. 2021, 293, 391–398. [Google Scholar] [CrossRef]
- Zhao, Y.-J.; Jin, Y.; Rao, W.-W.; Li, W.; Zhao, N.; Cheung, T.; Ng, C.H.; Wang, Y.-Y.; Zhang, Q.-E.; Xiang, Y.-T. The prevalence of psychiatric comorbidities during the SARS and COVID-19 epidemics: A systematic review and meta-analysis of observational studies. J. Affect. Disord. 2021, 287, 145–157. [Google Scholar] [CrossRef] [PubMed]
- Prati, G.; Mancini, A.D. The psychological impact of COVID-19 pandemic lockdowns: A review and meta-analysis of longitudinal studies and natural experiments. Psychol. Med. 2021, 51, 201–211. [Google Scholar] [CrossRef]
- Bonanad, C.; García-Blas, S.; Tarazona-Santabalbina, F.; Sanchis, J.; Bertomeu-González, V.; Fácila, L.; Ariza, A.; Núñez, J.; Cordero, A. The Effect of Age on Mortality in Patients With COVID-19: A Meta-Analysis With 611,583 Subjects. J. Am. Med. Dir. Assoc. 2020, 21, 915–918. [Google Scholar] [CrossRef] [PubMed]
- Khademi, F.; Moayedi, S.; Golitaleb, M.; Karbalaie, N. The COVID-19 pandemic and death anxiety in the elderly. Int. J. Ment. Health Nurs. 2021, 30, 346–349. [Google Scholar] [CrossRef] [PubMed]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Setiawati, Y.; Wahyuhadi, J.; Joestandari, F.; Maramis, M.M.; Atika, A. Anxiety and Resilience of Healthcare Workers During COVID-19 Pandemic in Indonesia. J. Multidiscip. Healthc. 2021, 14, 1–8. [Google Scholar] [CrossRef]
- Cheng, C.; Cheung, M.W.L. Psychological responses to outbreak of severe acute respiratory syndrome: A prospective, multiple time-point study. J. Personal. 2005, 73, 261–285. [Google Scholar] [CrossRef]
- Dai, Y.; Hu, G.; Xiong, H.; Qiu, H.; Yuan, X. Psychological impact of the coronavirus disease 2019 (COVID-19) outbreak on healthcare workers in China. medRxiv 2020, 33, PMC7299004. [Google Scholar] [CrossRef] [Green Version]
- Rizun, M.; Strzelecki, A. Students’ Acceptance of the COVID-19 Impact on Shifting Higher Education to Distance Learning in Poland. Int. J. Environ. Res. Public Health 2020, 17, 6468. [Google Scholar] [CrossRef]
- Arslan, G.; Yıldırım, M.; Aytaç, M. Subjective vitality and loneliness explain how coronavirus anxiety increases rumination among college students. Death Stud. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- Alemany-Arrebola, I.; Rojas-Ruiz, G.; Granda-Vera, J.; Mingorance-Estrada, Á.C. Influence of COVID-19 on the Perception of Academic Self-Efficacy, State Anxiety, and Trait Anxiety in College Students. Front. Psychol. 2020, 11, 570017. [Google Scholar] [CrossRef] [PubMed]
- Zhan, H.; Zheng, C.; Zhang, X.; Yang, M.; Zhang, L.; Jia, X. Chinese College Students’ Stress and Anxiety Levels Under COVID-19. Front. Psychiatry 2021, 12, 615390. [Google Scholar] [CrossRef] [PubMed]
- Allen, R.; Jerrim, J.; Sims, S. How Did the Early Stages of the COVID-19 Pandemic Affect Teacher Wellbeing; Working Paper No. 20-15; Centre for Education Policy and Equalising Opportunities (CEPEO): London, UK, 2020. [Google Scholar]
- Wakui, N.; Abe, S.; Shirozu, S.; Yamamoto, Y.; Yamamura, M.; Abe, Y.; Murata, S.; Ozawa, M.; Igarashi, T.; Yanagiya, T.; et al. Causes of anxiety among teachers giving face-to-face lessons after the reopening of schools during the COVID-19 pandemic: A cross-sectional study. BMC Public Health 2021, 21, 1050. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Zellweger-Zähner, T.; Schneider, M.; Junker, C.; Lengeler, C.; Antes, G. Language bias in randomised controlled trials published in English and German. Lancet 1997, 350, 326–329. [Google Scholar] [CrossRef]
- Prince, M.; Patel, V.; Saxena, S.; Maj, M.; Maselko, J.; Phillips, M.R.; Rahman, A. No health without mental health. Lancet 2007, 370, 859–877. [Google Scholar] [CrossRef]

{kind=link}
| Database | Search Terms | Search Limiters | Result |
|---|---|---|---|
| EMBASE (Ovid) | (Coronavirus OR COVID-19) AND (Anxiety) | Journal Article English 2020–2021 No Medline Results | 226 |
| Medline (Ovid) | (Coronavirus OR COVID-19) AND (Anxiety) | Journal Article English 2020–2021 | 2641 |
| CINAHL (EBSCO) | (Coronavirus OR COVID-19) AND (Anxiety) | Journal Article English 2020–2021 No Expanders | 268 |
| PsycINFO (EBSCO) | (Coronavirus OR COVID-19) AND (Anxiety) | Journal Article English 2020–2021 No Expanders | 402 |
| Reference | Study Design | Population Type | Country | Sample Size | Assessment Tools | Prevalence of Anxiety (%) |
|---|---|---|---|---|---|---|
| Aharon et al., 2020 [27] | Cross-sectional | General population | Israel and Italy | 1015 | PHQ-4, SF-8 | 50.2% of Italian and 42.2% of Israelis |
| Albagmi et al., 2012 [28] | Cross-sectional | General population | Saudi Arabia | 3017 | GAD-7 | 80% (mild), 11.4% (moderate), 8.2% (severe) |
| Alshekaili et al., 2020 [29] | Cross-sectional | Healthcare workers | Oman | 1139 | DASS-21 | 34.1% |
| Antonijevic et al., 2020 [30] | Cross-sectional | Healthcare workers | Serbia | 1678 | GAD-7 | 43.31% (minimal), 30.9% (mild), 12.99% (moderate),12.8% (severe). |
| Ausin et al., 2020 [31] | longitudinal | General population | Spain | 1041 | GAD-2 | N/A |
| Batterham et al., 2021 [32] | longitudinal | General population | Australia | 1296 | GAD-7, PHQ-9 | 77% |
| Bendau et al., 2020 [11] | Longitudinal | General population | Germany | 2376 | GAD-2, PHQ-4 | N/A |
| Budimir et al., 2021 [33] | Cross-sectional | General population | Austria and UK | 2011 | GAD-7 | 18.9% UK and 6% Austria |
| Cai et al., 2020 [34] | case-control | Healthcare workers | China | 2346 | BAI | Frontline 15.7%, non-frontline 7.4% |
| Canet-Juric et al., 2020 [35] | longitudinal | General population | Argentina | 6057 | STAI | N/A |
| Cao et al., 2020 [36] | Cluster Sampling | University Students | China | 7143 | GAD-7 | Mild (21.3%), moderate (2.7%), severe (0.9%) |
| Chen et al., 2021 [37] | Cross-sectional | General population (quarantined) | China | 1837 | STAI | 16.3% |
| Chew et al., 2020 [38] | Cross-sectional | Healthcare workers | India, Indonesia, Singapore, Malaysia and Vietnam | 1146 | DASS-21 | India (0.8%), Singapore (3.6%), Vietnam (6.7%), Indonesia (6.8%) and Malaysia (14.9%) |
| Dawel et al., 2020 [39] | longitudinal | General population | Australia | 1296 | GAD-7, PHQ-9, WHO-5 | N/A |
| Denning et al., 2021 [40] | Cross-sectional | Healthcare workers | UK, Poland and Singapore | 3537 | HADS | 20% |
| Di Blasi et al., 2021 [41] | longitudinal | General population | Italy | 1129 | DASS-21 | N/A |
| Di Giuseppe et al., 2020 [42] | Cross-sectional | General population | Italy | 5683 | SCL-90 | 51.1% |
| Di Mattei et al., 2021 [43] | Baseline assessment | Healthcare workers | Italy | 1055 | DASS-21 | 69.4% |
| Fiorillo et al., 2020 [44] | longitudinal | General population | Italy | 20,720 | DASS-21, GHQ | Moderate (16.7%) and severe or extremely severe (17.6%) |
| Fisher et al., 2020 [45] | Cross-sectional | General Population | Australia | 13,829 | GAD-7, PHQ-9 | 21% |
| Fu et al., 2020 [46] | Cross-sectional | General population | China | 1242 | GAD-7, PHQ-9 | 27.6% |
| Fu et al., 2021 [47] | Cross-sectional | University students | China | 89,588 | GAD-7 | 41.1% |
| Gainer et al., 2021 [48] | Cross-sectional | Healthcare workers | US | 1724 | GAD-7, PHQ-9 | 36.5% |
| Garcia-Fernandez et al., 2020 [49] | Cross-sectional | Elderly population | Spain | 1639 | HARS | N/A |
| Garcia-Fernandez et al., 2020 [50] | Cross-sectional | General population | Spain | 1635 | HARS | N/A |
| Giardino et al., 2020 [51] | Cross-sectional | Healthcare workers | Argentina | 1059 | DASS-18 | 76.5% |
| Gundogmus et al., 2021 [52] | longitudinal | Healthcare Workers | Turkey | 2460 | DASS-21 | 29.6% |
| Hacimusalar et al., 2020 [53] | Cross-sectional | Healthcare, non-healthcare | Turkey | 2156 | STAI | 89.5% |
| Halperin et al., 2021 [54] | Cross-sectional | University students | US | 1428 | GAD-7, PHQ-9 | 30.6% |
| Hammarberg et al., 2020 [55] | Cross-sectional | General population | Australia | 13,762 | GAD-7 | 21.8% females, 14.2% males |
| Hassannia et al., 2021 [56] | Cross-sectional | Healthcare workers and general population | Iran | 2045 | HADS | 65.6% |
| He et al., 2021 [57] | Cross-sectional | Healthcare workers | China | 1971 | GAD-7 | 29.3% |
| Hennein et al., 2021 [58] | Cross-sectional | Healthcare workers | US | 1092 | GAD-7 | 15.6% |
| Huang et al., 2021 [59] | Cross-sectional | Healthcare workers | Singapore | 1638 | GAD-7 | 12.5% |
| Islaml et al., 2020 [60] | Cross-sectional | University students | Bangladesh | 3122 | DASS-21 | Mild anxiety (71.5%), moderate (63.6%), severe (40.3%) and very severe (27.5%). |
| Jacques-Avino et al., 2020 [61] | Cross-sectional | General population | Spain | 7053 | GAD-7 | 31.2% females, 17.7% males |
| Jia et al., 2020 [62] | Cross-sectional | General population | UK | 3097 | GAD-7 | 57% (26% moderate to severe anxiety) |
| Jiang et al., 2020 [63] | Cross-sectional | General population | China | 60,199 | SAI | Mild (33.21%), moderate (41.27%) and severe (22.99%). |
| Johnson et al., 2021 [64] | longitudinal | Parents | Norway | 2868 | GAD-7 | N/A |
| Kantor and Kantor, 2020 [65] | Cross-sectional | General population | US | 1005 | GAD-7 | 52.1% mild, 26.8% anxiety disorder |
| Karaivazoglou et al., 2021 [66] | Cross-sectional | General population | Greece | 1443 | HADS | 20% |
| Khubchandani et al. 2021 [67] | Cross-sectional | General population | US | 1978 | GAD-2, PHQ-4 | 42% |
| Kim et al., 2021 [68] | longitudinal | University Students | US | 8613 | GAD | No significant changes were found in the rates of anxiety from before the pandemic. |
| Lai et al., 2020 [69] | Cross-sectional | Healthcare workers | China | 1257 | GAD-7 | 44.6% |
| Lei et al., 2020 [70] | Cross-sectional | General population | China | 1593 | SAS | 8.3% |
| Li et al., 2020 [71] | Cross-sectional | Teachers | China | 88,611 | GAD-7 | 13.67% |
| Li et al., 2021 [72] | Cross-sectional | General population | China | 1201 | DASS-21 | 34.2% |
| Liu et al., 2021 [73] | Cross-sectional | Healthcare workers | China | 1090 | GAD-7 | 13.3% |
| Liu et al., 2020 [74] | Cross-sectional | Healthcare workers (paediatric) | China | 2031 | DASS-21 | 18.3% |
| Lu et al., 2020a [75] | Cross-sectional | General population and frontline workers | China | 1417 | GAD-7 | 52.1% of the general public and 56% of frontline workers |
| Lu et al., 2020b [76] | Cross-sectional | Healthcare workers | China | 2299 | HAMA | 22.6% of medical staff showed mild to moderate anxiety and 2.9% were severe |
| Luceno-Moreno et al., 2020 [77] | Cross-sectional | Healthcare workers | Spain | 1422 | HADS | 58.6% healthcare workers presented with an anxiety disorder. |
| Mattila et al., 2020 [78] | Cross-sectional | Healthcare workers | Finland | 1995 | GAD-7 | 30% mild anxiety, 10% moderate and 5% severe anxiety. |
| Meesala et al., 2021 [79] | Cross-sectional | General population | India | 1346 | CAS-7 | N/A |
| Mosheva et al., 2020 [80] | Cross-sectional | Healthcare workers | Israel | 1106 | PROMIS | 52.8% |
| Ngoc Cong Duong et al., 2020 [81] | Cross-sectional | General population | Vietnam | 1385 | DASS-21 | 14.1% |
| Nkire et al., 2021 [82] | Cross-sectional | General population | Canada | 6041 | GAD-7 | 46.7% |
| Odriozola-Gonzalez et al., 2020 [83] | Cross-sectional | University students and workers. | Spain | 2530 | DASS-21, IES | 21.34% |
| Ozamiz-Etxebarria et al., 2021 [84] | Cross-sectional | Teachers | Spain | 1633 | DASS-21 | 49.5% (8.1% extreme severe and 7.6% severe) |
| Ozamiz-Etxebarria et al., 2020 [85] | longitudinal | General population | Spain | 1933 | DASS-21 | 26.9% |
| Pandey et al., 2020 [86] | Cross-sectional | General population | India | 1395 | DASS-21 | Anxiety prevalence was 22.4% in the second week and 26.6% in the third week of lockdowns |
| Passavanti et al., 2021 [87] | Cross-sectional | General population | Australia, Iran, China, Ecuador, Italy, Norway and the US | 1612 | DASS-21 | 44.7% (5.2% mild, 17.4% moderate, 5.8% severe and 16.3% extremely severe). |
| Pieh et al., 2021 [88] | Cross-sectional | General population | UK | 1006 | GAD-7 | 39% |
| Peih et al., 2020 [89] | Cross-sectional | General population | Austria | 1005 | GAD-7 | 19% |
| Planchuelo-Gomez et al., 2020 [90] | longitudinal | General population | Spain | 4724 | DASS-21 | 49.66% |
| Robb et al., 2020 [91] | Cross-sectional | Elderly population | UK | 7127 | HADS | N/A |
| Rossi et al., 2020 [92] | Cross-sectional | Healthcare workers and general population | Italy | 24,050 | GAD-7 | 21.25% in the general population, 18.05% in second line healthcare workers and 20.55% in frontline workers. |
| Ruengorn et al., 2020 [93] | Cross-sectional | General population | Thailand | 2303 | GAD-7 | 56.9% |
| Serafim et al., 2021 [94] | Cross-sectional | General population | Brazil | 3000 | DASS-21 | 39.7% |
| Shen et al., 2020 [95] | Cross-sectional | Healthcare Workers | China | 1637 | SAS | 10.02% |
| Sinawi et al., 2021 [96] | Cross-sectional | General Population | Oman | 1538 | GAD-7 | 22% |
| Solomou et al., 2020 [97] | Cohort study | General population | Cyprus | 1642 | GAD-7 | 41% mild, 23.1% moderate-severe |
| Sun et al., 2021 [98] | Cross-sectional | University Students | China | 1912 | GAD-7 | 34.73% |
| Tang et al., 2020 [99] | Cross-sectional | General population | China | 1389 | GAD-7 | 70.78% |
| Van der Velden et al., 2020 [100] | Longitudinal | General population | Holland | 3983 | GAD-7 | No significant anxiety found |
| Wang et al., 2021a [101] | Case-control | General population | China | 1674 | ADS | 27% in quarantined, 11.2% in general population |
| Wang et al., 2021b [102] | Cross-sectional | Healthcare workers | China | 1063 | GAD-7 | 48.7% in patients, 25.7% general population, 13.3% healthcare |
| Wang et al., 2020 [103] | Cross-sectional | General, covid and health | China | 49,015 | DASS-21 | 10.02% |
| Wanigasooriya et al., 2021 [104] | Cross-sectional | Healthcare workers | UK | 2638 | PHQ-4 | 34.31% |
| Warren et al., 2021 [105] | Cross-sectional | General population | United States | 5023 | PHQ-4 | 14.4% |
| Wathelet et al., 2020 [106] | Cross-sectional | University Students | France | 69,054 | STAI | 27.47% |
| Wu et al., 2020 [107] | Cross-sectional | General population | China | 24,789 | STAI | 51.6% |
| Yuan et al., 2020 [108] | Cross-sectional | Police | China | 3517 | HADS | 8.79% |
| Zhang et al., 2020a [109] | Cross-sectional | Healthcare workers | China | 2143 | GAD-7 | 14.23% |
| Zhang et al., 2020b [110] | Cross-sectional | General population | China | 123,768 | GAD-7 | 3.4% |
| Zhou et al., 2020 [111] | Cross-sectional | Healthcare workers | China | 1705 | SAS | 45.4% |
| Zilver et al., 2021 [112] | Cohort study | Pregnant women | Holland | 1466 | GAD-7 | 19.5% |
| Population Type | No. of Papers | Sample Size | Anxiety Prevalence | Main Findings |
|---|---|---|---|---|
| General Population | 47 | 423,341 | 34% | Those in epicentres or those with higher exposure to COVID-19 are more at risk of developing anxiety. Quarantine had mass adverse effects on mental health with females, younger people, the elderly, and lower SES disproportionality impacted. |
| Healthcare Workers | 25 | 43,387 | 36% | Increased working demands of COVID-19 have resulted in increased anxiety and burnout, especially in frontline workers. Health anxiety is highly prevalent with fears of infecting others. Females, trainee staff, and those with pre-existing conditions were most effected. |
| University Students | 8 | 183,390 | 34.7% | Worry regarding academics resulted in a marked increase in anxiety, especially during periods of lockdowns and when compared to pre-pandemic times. Financial instability and stigma accessing aid may have contributed to this. Females were also identified as having higher anxiety than males. |
| Other Groups: | Elderly (2) Teachers (2) Parents (1) Pregnant (1) Police (1) | 106,861 | N/A | The other groups affected all exemplify groups within society that are vulnerable, with females experiencing more anxiety than males in all groups apart from the elderly population, where no difference was seen. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saeed, H.; Eslami, A.; Nassif, N.T.; Simpson, A.M.; Lal, S. Anxiety Linked to COVID-19: A Systematic Review Comparing Anxiety Rates in Different Populations. Int. J. Environ. Res. Public Health 2022, 19, 2189. https://doi.org/10.3390/ijerph19042189
Saeed H, Eslami A, Nassif NT, Simpson AM, Lal S. Anxiety Linked to COVID-19: A Systematic Review Comparing Anxiety Rates in Different Populations. International Journal of Environmental Research and Public Health. 2022; 19(4):2189. https://doi.org/10.3390/ijerph19042189
Chicago/Turabian StyleSaeed, Hafsah, Ardalan Eslami, Najah T. Nassif, Ann M. Simpson, and Sara Lal. 2022. "Anxiety Linked to COVID-19: A Systematic Review Comparing Anxiety Rates in Different Populations" International Journal of Environmental Research and Public Health 19, no. 4: 2189. https://doi.org/10.3390/ijerph19042189
APA StyleSaeed, H., Eslami, A., Nassif, N. T., Simpson, A. M., & Lal, S. (2022). Anxiety Linked to COVID-19: A Systematic Review Comparing Anxiety Rates in Different Populations. International Journal of Environmental Research and Public Health, 19(4), 2189. https://doi.org/10.3390/ijerph19042189