
Increased Urinary Cadmium Levels in Foreign-Born Asian Women—An NHANES Study of 9639 U.S. Participants

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
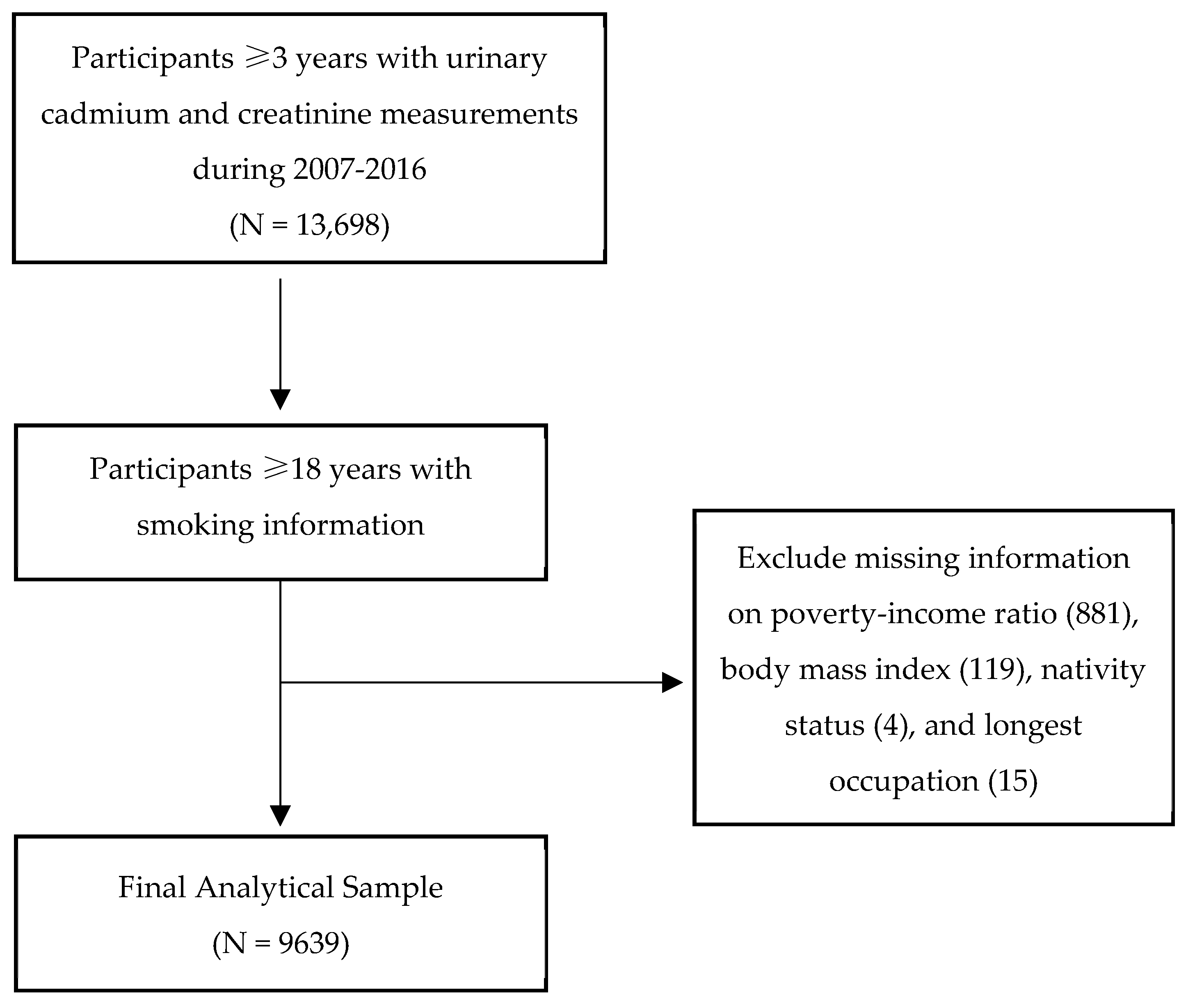
2.1. Data Source and Study Sample
2.2. Covariates
2.3. Outcome Measurements
2.4. Statistical Analysis
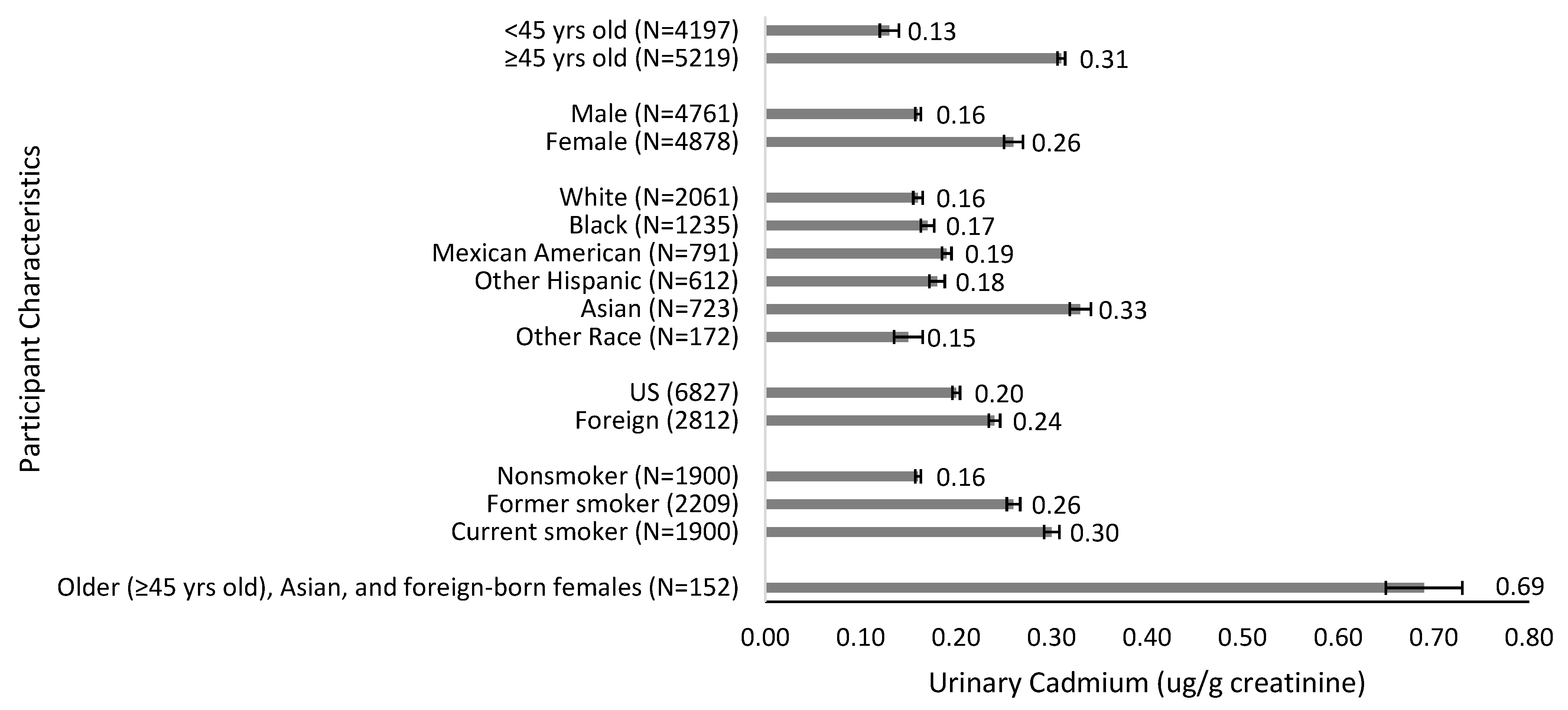
3. Results
ANOVA and Multivariable Regression Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Adams, S.V.; Newcomb, P.A.; Shafer, M.M.; Atkinson, C.; Bowles, E.J.A.; Newton, K.M.; Lampe, J.W. Sources of cadmium exposure among healthy premenopausal women. Sci. Total Environ. 2011, 409, 1632–1637. [Google Scholar] [CrossRef] [Green Version]
- What Are the U.S. Standards for Cadmium Exposure. Centers for Disease Control and Prevention. Available online: https://www.atsdr.cdc.gov/csem/cadmium/Safety-Standards.html (accessed on 24 January 2022).
- Buser, M.C.; Ingber, S.Z.; Raines, N.; Fowler, D.A.; Scinicariello, F. Urinary and blood cadmium and lead and kidney function: NHANES 2007–2012. Int. J. Hyg. Environ. Health 2016, 219, 261–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallagher, C.M.; Moonga, B.S.; Kovach, J.S. Cadmium, follicle-stimulating hormone, and effects on bone in women age 42–60 years, NHANES III. Environ. Res. 2010, 110, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Rani, A.; Kumar, A.; Lal, A.; Pant, M. Cellular mechanisms of cadmium-induced toxicity: A review. Int. J. Environ. Health Res. 2014, 24, 378–399. [Google Scholar] [CrossRef] [PubMed]
- Rafati Rahimzadeh, M.; Rafati Rahimzadeh, M.; Kazemi, S.; Moghadamnia, A.A. Cadmium toxicity and treatment: An update. Casp. J. Intern. Med. 2017, 8, 135–145. [Google Scholar] [CrossRef]
- Miao, H.; Ji, J.S. Trends of Blood Cadmium Concentration Among Workers and Non-Workers in the United States (NHANES 2003 to 2012). J. Occup. Environ. Med. 2019, 61, e503–e509. [Google Scholar] [CrossRef] [PubMed]
- Bulka, C.M.; Bommarito, P.A.; Fry, R.C. Predictors of toxic metal exposures among US women of reproductive age. J. Expo. Sci. Environ. Epidemiol. 2019, 29, 597–612. [Google Scholar] [CrossRef]
- Mijal, R.S.; Holzman, C.B. Blood cadmium levels in women of childbearing age vary by race/ethnicity. Environ. Res. 2010, 110, 505–512. [Google Scholar] [CrossRef] [Green Version]
- Järup, L.; Akesson, A. Current status of cadmium as an environmental health problem. Toxicol. Appl. Pharmacol. 2009, 238, 201–208. [Google Scholar] [CrossRef]
- NHANES—National Health and Nutrition Examination Survey Homepage. Available online: https://www.cdc.gov/nchs/nhanes/index.htm (accessed on 7 August 2021).
- About Adult BMI. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/healthyweight/assessing/bmi/adult_bmi/index.html (accessed on 27 August 2021).
- Wei, B.; Bernert, J.T.; Blount, B.C.; Sosnoff, C.S.; Wang, L.; Richter, P.; Pirkle, J.L. Temporal Trends of Secondhand Smoke Exposure: Nonsmoking Workers in the United States (NHANES 2001–2010). Environ. Health Perspect. 2016, 124, 1568–1574. [Google Scholar] [CrossRef]
- National Health and Nutrition Examination Survey (NHANES): Laboratory Procedures Manual. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/2011-2012/manuals/2011-12_laboratory_procedures_manual.pdf (accessed on 7 August 2021).
- Genchi, G.; Sinicropi, M.S.; Lauria, G.; Carocci, A.; Catalano, A. The Effects of Cadmium Toxicity. Int. J. Environ. Res. Public Health 2020, 17, 3782. [Google Scholar] [CrossRef]
- IARC. Summary of Data Reported and Evaluation. In IARC Monographs on the Evaluation of Carcinogenic Risks to Humas. Beryllium, Cadmium, Mercury, and Exposures in the Glass Manufacturing Industry; International Agency for Cancer Research, World Health Organization: Geneva, Switzerland, 1997; Volume 58. [Google Scholar]
- Jain, R.B. Factors affecting the variability in the observed levels of cadmium in blood and urine among former and current smokers aged 20–64 and ≥65 years. Environ. Sci. Pollut. Res. Int. 2017, 24, 8837–8851. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, C.M.; Chen, J.J.; Kovach, J.S. The relationship between body iron stores and blood and urine cadmium concentrations in US never-smoking, non-pregnant women aged 20–49 years. Environ. Res. 2011, 111, 702–707. [Google Scholar] [CrossRef] [PubMed]
- Vahter, M.; Berglund, M.; Akesson, A.; Lidén, C. Metals and women’s health. Environ. Res. 2002, 88, 145–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.D.; Cherrington, N.J.; Klaassen, C.D. Intestinal absorption of cadmium is associated with divalent metal transporter 1 in rats. Toxicol. Sci. 2002, 68, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Aoki, Y.; Yee, J.; Mortensen, M.E. Blood cadmium by race/hispanic origin: The role of smoking. Environ. Res. 2017, 155, 193–198. [Google Scholar] [CrossRef] [Green Version]
- Meharg, A.A.; Norton, G.; Deacon, C.; Williams, P.; Adomako, E.E.; Price, A.; Zhu, Y.; Li, G.; Zhao, F.-J.; McGrath, S.; et al. Variation in rice cadmium related to human exposure. Environ. Sci. Technol. 2013, 47, 5613–5618. [Google Scholar] [CrossRef]
- Kim, K.; Melough, M.M.; Vance, T.M.; Noh, H.; Koo, S.I.; Chun, O.K. Dietary Cadmium Intake and Sources in the US. Nutrients 2018, 11, 2. [Google Scholar] [CrossRef] [Green Version]
- Hutton, M. Sources of cadmium in the environment. Ecotoxicol. Environ. Saf. 1983, 7, 9–24. [Google Scholar] [CrossRef]
- Elghany, N.A.; Schumacher, M.C.; Slattery, M.L.; West, D.W.; Lee, J.S. Occupation, cadmium exposure, and prostate cancer. Epidemiology 1990, 1, 107–115. [Google Scholar] [CrossRef]
- Lo, J.C.; Chandra, M.; Lee, C.; Darbinian, J.A.; Ramaswamy, M.; Ettinger, B. Bone Mineral Density in Older U.S. Filipino, Chinese, Japanese, and White Women. J. Am. Geriatr. Soc. 2020, 68, 2656–2661. [Google Scholar] [CrossRef] [PubMed]
- Riederer, A.M.; Belova, A.; George, B.J.; Anastas, P.T. Urinary cadmium in the 1999–2008 U.S. National Health and Nutrition Examination Survey (NHANES). Environ. Sci. Technol. 2013, 47, 1137–1147. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Gao, P.; Snyder, M.P. The Exposome in the Era of the Quantified Self. Annu. Rev. Biomed. Data Sci. 2021, 4, 255–277. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Occupation Category | Occupation Types |
|---|---|
| White-collar | Management occupations, legal occupations |
| Science and education | Computer and mathematical occupations, architecture and engineering occupations, life physical, science and social science, education training and library occupations |
| Health-related | Health care practitioner technical occupations, health support, personal care service occupations |
| Sales, finance, business-related | Business, financial operations occupations, arts design entertainment sports media occupations, sales and related occupations |
| Office, administrative support | Community social services occupations, office and administrative support occupations |
| Food preparation and service | Food preparation service occupations |
| Blue collar | Protective services, building and cleaning maintenance occupations, farming fishing forestry occupations, construction extraction occupations, installation repair maintenance occupations, production occupations, transportation material moving occupations, armed forces |
| Characteristics | Overall (N = 9639) | Cadmium (µg/g Creatinine) | ||
|---|---|---|---|---|
| N(%) | Geometric Mean | Range | p-Value | |
| Time-Period | <0.001 a | |||
| 2007–2008 | 1934 (19%) | 0.24 | 0.01–4.04 | |
| 2009–2010 | 2111 (20%) | 0.23 | 0.01–3.57 | |
| 2011–2012 | 1805 (20%) | 0.21 | 0.02–7.56 | |
| 2013–2014 | 1925 (21%) | 0.17 | 0.01–5.49 | |
| 2015–2016 | 1864 (21%) | 0.18 | 0.01–2.73 | |
| Age Group | <0.001 a | |||
| Median (Range) | 45 yrs (18–80) | |||
| <45 yrs | 4197 (47%) | 0.13 | 0.01–7.56 | |
| ≥45 yrs | 5219 (53%) | 0.31 | 0.01–5.49 | |
| Nativity | <0.001 a | |||
| US | 6827 (82%) | 0.20 | 0.01–7.56 | |
| Foreign | 2812 (18%) | 0.24 | 0.01–5.49 | |
| Race/Ethnicity (2007–2016) | <0.001 a | |||
| White | 3933 (66%) | 0.21 | 0.01–7.56 | |
| Black | 2029 (12%) | 0.20 | 0.01–3.57 | |
| Mexican American | 1524 (9%) | 0.17 | 0.01–5.49 | |
| Other Hispanic | 1059 (6%) | 0.18 | 0.01–3.16 | |
| Other b | 1094 (8%) | 0.27 | 0.01–4.47 | |
| Race/Ethnicity (2011–2016) c | <0.001 a | |||
| White | 2061 (65%) | 0.16 | 0.01–7.56 | |
| Black | 1235 (11%) | 0.17 | 0.01–2.69 | |
| Mexican American | 791 (9%) | 0.19 | 0.01–5.49 | |
| Other Hispanic | 612 (6%) | 0.18 | 0.01–2.58 | |
| Asian | 723 (5%) | 0.33 | 0.02–4.47 | |
| Other d | 172 (3%) | 0.15 | 0.01–0.91 | |
| Gender | <0.001 a | |||
| Male | 4761 (48%) | 0.16 | 0.01–5.49 | |
| Female | 4878 (52%) | 0.26 | 0.01–7.56 | |
| Income Level | <0.001 a | |||
| Poverty | 2873 (22%) | 0.22 | 0.01–5.49 | |
| Low | 2342 (19%) | 0.21 | 0.01–5.90 | |
| Middle | 2289 (27%) | 0.21 | 0.01–4.47 | |
| High | 2135 (33%) | 0.20 | 0.01–7.56 | |
| Body Mass Index Category | <0.001 a | |||
| Median (Range) | 27 kg/m2 (13–83) | |||
| Underweight | 290 (3%) | 0.30 | 0.02–3.84 | |
| Normal | 2781 (30%) | 0.21 | 0.01–4.47 | |
| Overweight | 3104 (33%) | 0.21 | 0.01–7.56 | |
| Obese | 3464 (35%) | 0.20 | 0.01–4.04 | |
| Smoking Status | <0.001 a | |||
| Nonsmoker | 5530 (56%) | 0.16 | 0.01–7.56 | |
| Former smoker | 2209 (24%) | 0.26 | 0.01–5.49 | |
| Current smoker | 1900 (20%) | 0.30 | 0.01–5.90 | |
| Longest Occupation e,f | <0.001 a | |||
| Never worked | 392 (4%) | 0.18 | 0.02–4.04 | |
| White-collar | 549 (9%) | 0.20 | 0.01–5.90 | |
| Science and education | 658 (11%) | 0.20 | 0.01–4.47 | |
| Health-related | 826 (11%) | 0.24 | 0.01–4.22 | |
| Sales, finance, business | 1057 (15%) | 0.20 | 0.01–7.56 | |
| Office, administrative | 980 (13%) | 0.24 | 0.02–3.57 | |
| Food preparation and services | 548 (6%) | 0.18 | 0.02–3.72 | |
| Blue-collar | 2736 (31%) | 0.22 | 0.01–5.49 | |
| Characteristics | Odds Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Time-Period | |||
| 2007–2008 | 1 | ||
| 2009–2010 | 0.88 | 0.71–1.09 | 0.23 |
| 2011–2012 | 0.72 | 0.57–0.90 | 0.005 |
| 2013–2014 | 0.47 | 0.39–0.57 | <0.001 |
| Age Group | |||
| <45 yrs | 1 | ||
| ≥45 yrs | 8.87 | 7.48–10.53 | <0.001 |
| Nativity | |||
| US | 1 | ||
| Foreign | 1.83 | 1.48–2.26 | <0.001 |
| Race/Ethnicity a | |||
| White | 1 | ||
| Black | 1.17 | 0.91–1.52 | 0.21 |
| Asian | 4.52 | 3.10–6.61 | <0.001 |
| Mexican American | 1 | 0.62–1.62 | 0.99 |
| Other Hispanic | 0.81 | 0.55–1.18 | 0.26 |
| Other b | 1.12 | 0.52–2.44 | 0.76 |
| Gender | |||
| Male | 1 | ||
| Female | 4.32 | 3.59–5.21 | <0.001 |
| Income Level | |||
| High | 1 | ||
| Poverty | 1.35 | 1.08–1.68 | 0.01 |
| Low | 1.17 | 0.95–1.44 | 0.14 |
| Middle | 1.18 | 0.97–1.44 | 0.09 |
| Body Mass Index Category | |||
| Underweight | 1 | ||
| Normal | 0.96 | 0.62–1.47 | 0.84 |
| Overweight | 0.81 | 0.53–1.25 | 0.33 |
| Obese | 0.66 | 0.42–1.03 | 0.07 |
| Smoking Status | |||
| Nonsmoker | 1 | ||
| Former smoker | 3.23 | 2.65–3.95 | <0.001 |
| Current smoker | 5.74 | 4.69–7.02 | <0.001 |
| Longest Occupation c,d | |||
| Never worked | 1 | ||
| White-collar | 0.97 | 0.61–1.53 | 0.89 |
| Science and education | 0.88 | 0.59–1.32 | 0.54 |
| Health-related | 0.93 | 0.61–1.40 | 0.71 |
| Sales, Finance, business | 0.99 | 0.70–1.42 | 0.97 |
| Office, administrative | 0.997 | 0.71–1.39 | 0.99 |
| Food preparation and services | 0.74 | 0.52–1.06 | 0.10 |
| Blue-collar | 1.37 | 0.95–1.98 | 0.09 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milki, A.; Wong, D.; Chan, C.; Sooklal, S.; Kapp, D.S.; Mann, A.K. Increased Urinary Cadmium Levels in Foreign-Born Asian Women—An NHANES Study of 9639 U.S. Participants. Int. J. Environ. Res. Public Health 2022, 19, 2170. https://doi.org/10.3390/ijerph19042170
Milki A, Wong D, Chan C, Sooklal S, Kapp DS, Mann AK. Increased Urinary Cadmium Levels in Foreign-Born Asian Women—An NHANES Study of 9639 U.S. Participants. International Journal of Environmental Research and Public Health. 2022; 19(4):2170. https://doi.org/10.3390/ijerph19042170
Chicago/Turabian StyleMilki, Anthony, Deanna Wong, Chloe Chan, Sarita Sooklal, Daniel S. Kapp, and Amandeep K. Mann. 2022. "Increased Urinary Cadmium Levels in Foreign-Born Asian Women—An NHANES Study of 9639 U.S. Participants" International Journal of Environmental Research and Public Health 19, no. 4: 2170. https://doi.org/10.3390/ijerph19042170
APA StyleMilki, A., Wong, D., Chan, C., Sooklal, S., Kapp, D. S., & Mann, A. K. (2022). Increased Urinary Cadmium Levels in Foreign-Born Asian Women—An NHANES Study of 9639 U.S. Participants. International Journal of Environmental Research and Public Health, 19(4), 2170. https://doi.org/10.3390/ijerph19042170