Abstract
Introduction: Paracetamol is the most commonly used antipyretic and analgesic in pregnancy. It is also increasingly used off-label in the neonatal intensive care unit. Despite the frequent use of paracetamol, concerns have been raised regarding the high variability in neonatal dosing regimens and the long-term safety of early life exposure. Objective: To investigate the available evidence on the long-term safety of prenatal and neonatal paracetamol exposure. Methods: We conducted a systematic search of the electronic databases Ovid Medline, Ovid Embase and Web of Science from inception to August 2021 for original research studies of any design that described the use of paracetamol in the prenatal or neonatal (within the first four weeks of life) periods and examined the occurrence of neurodevelopmental, atopic or reproductive adverse outcomes at or beyond birth. Results: We identified 1313 unique articles and included 30 studies in the final review. Of all studies, 27 (90%), two (7%) and one (3%) were on the long-term safety of prenatal, neonatal and both prenatal and neonatal exposure, respectively. Thirteen (46%), 11 (39%) and four (15%) studies examined neurodevelopmental, atopic and reproductive outcomes. Eleven (100%), 11 (100%), and three (27%) studies on prenatal exposure reported adverse neurodevelopmental, atopic and reproductive outcomes. Only one study found a possible correlation between neonatal paracetamol exposure and long-term adverse outcomes. Conclusions: The available evidence, although limited, suggests a possible association between prenatal paracetamol exposure and an increased risk of neurodevelopmental, atopic and reproductive adverse outcomes. There is an immediate need for robust data on the long-term safety of paracetamol exposure in the prenatal and neonatal periods.
1. Introduction
Paracetamol, the most frequently used drug in pregnancy, is now one of the most common medications used off-label in the neonatal intensive care unit (NICU). Besides its antipyretic and analgesic properties, paracetamol promotes the closure of persistent patent ductus arteriosus (PDA) [1]. In 2010, paracetamol was the fifteenth most commonly used medication in NICUs in the United States. However, a recent study of European NICUs found that it is now the third most frequently administered drug, prescribed to over 65% of extremely preterm neonates [2].
The opioid-sparing effects of paracetamol and its comparable effectiveness to non-steroidal anti-inflammatory drugs (NSAIDs) in the closure of PDAs are the main drivers of its increasing use in the NICU [3,4,5]. Animal models have shown degenerative and necrotic changes in pulmonary, reproductive and nervous systems following exposure to paracetamol during the period of embryogenesis or organogenesis [6]. Over the past 20 years, growing human epidemiological data have also raised concern regarding early life exposure to paracetamol and an increased risk of neurodevelopmental, atopic and reproductive adverse outcomes [7]. Paracetamol’s analgesic and antipyretic effects are mediated through activation of descending serotonergic pathways, inhibition of prostaglandin synthesis and effects on cannabinoids receptors through its active metabolites [8,9,10]. The non-selective inhibition of peripheral cyclooxygenase and the interference with the cannabinoid receptors are among paracetamol’s mechanisms of action that could explain how such causal association could be biologically plausible [11]. We, therefore, aimed to conduct this review to systematically collate and assess the entirety of primary research on the long-term safety of prenatal and neonatal (within the first four weeks of life) exposure to paracetamol.
2. Materials and Methods
2.1. Protocol and Registration
The Joanna Briggs Institute Manual for Evidence Synthesis [12] and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [13] guided the conduct and reporting of this review, respectively. The protocol for this review was submitted for registration to the international database of prospectively registered systematic reviews (PROSPERO, registration ID CRD42020212364) and was published [14].
2.2. Search Strategy
We developed a systematic search strategy with a professional librarian and searched the electronic databases Ovid Medline (1946 to August 2021), Ovid Embase (1974 to August 2021) and Web of Science (1900 to August 2021) (Table 1). We hand-searched the bibliographies of included studies for additional references. Using Google Scholar, we also searched for articles not commercially published, such as conference abstracts, dissertations and policy documents. We did not apply any language or design limitations.

Table 1.
Ovid Medline, Ovid Embase and Web of Science search strategies.
2.3. Eligibility Criteria
We included original research studies of any design that described the use of paracetamol in the prenatal or neonatal (within the first four weeks of life) periods and examined the occurrence of neurodevelopmental, atopic or reproductive adverse outcomes. Studies were eligible for inclusion irrespective of the indication, dose, administration frequency and duration of paracetamol treatment. In the studies with a control group, we used the provided intervention(s), placebo or standard practice as the comparator. In studies with no comparator group, we collected the observational report of the long-term safety of paracetamol during the study period. Neurodevelopmental, atopic and reproductive adverse outcomes were any neurodevelopmental, atopic or reproductive disorders described by the authors of the primary studies, respectively. We excluded animal studies and duplicate studies.
2.4. Study Selection Process and Data Extraction
Following the database searches, using Covidence as the primary screening and data extraction tool, two reviewers (K.S. and R.P.) screened all articles independently at the title and abstract level. The same reviewers then assessed all full-text articles for eligibility. After identifying the studies to be included in the final review, the same reviewers extracted the data independently, using a prespecified standardized data extraction form [10]. We resolved any discrepancies in the study selection and data extraction processes through discussion with a third reviewer (S.S.Z).
2.5. Risk of Bias Assessment and Assessment of Evidence Certainty
Two reviewers (K.S and R.P) performed a qualitative assessment of the included studies, using standardized risk-of-bias assessment tools appropriate for each study design. These included the Newcastle–Ottawa Quality Assessment Scale for Cohort Studies [15], the modified tool for assessing the Quality of Modern Cross-Sectional Ecologic Studies [16,17,18] and the Cochrane Collaboration Risk of Bias 2 (RoB 2) tool for randomized controlled trials (RCTs) [19]. The same reviewers used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach [20] to rate the certainty of the evidence, with adaptations by Murad et al. [21] to account for the absence of a single effect estimate. Any discrepancies were resolved through discussion with a third reviewer (S.S.Z.).
2.6. Synthesis Methods
We did not conduct a quantitative synthesis, due to the considerable heterogeneity of the included studies, methodologically, statistically and clinically. We performed a narrative synthesis of the study results based on the timing of exposure (prenatal or neonatal) and the primary outcome of interest (neurodevelopmental, atopic or reproductive adverse outcomes).
3. Results
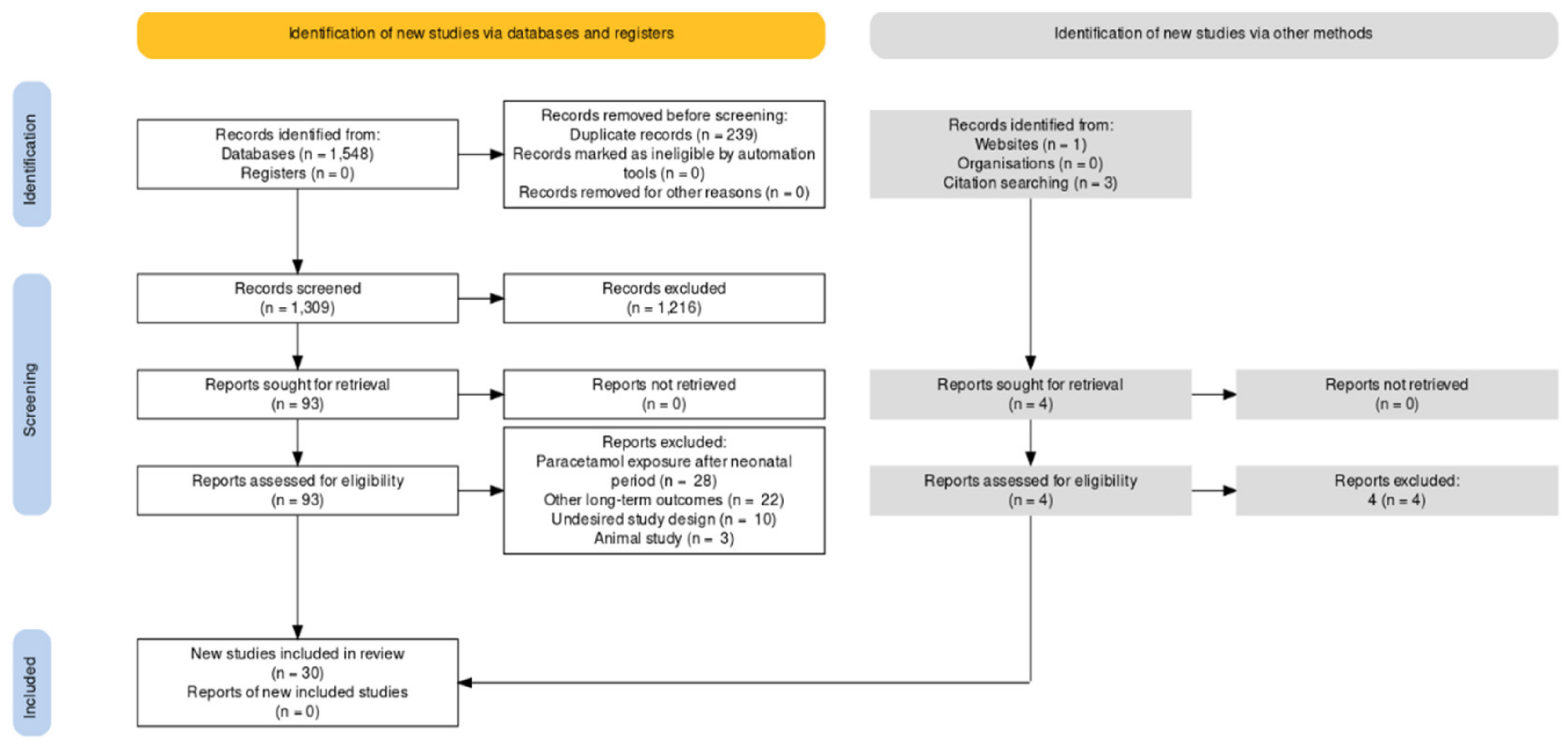
We identified a total of 1552 articles. After removing duplicates, we screened 1313 studies at the title and abstract level and 97 at the full-text level. Title- and abstract-screening assessed the following: is the study about prenatal or neonatal exposure to paracetamol? Full-text screening assessed the following: does the study examine neurodevelopmental, atopic or reproductive outcomes? We included 30 studies in the final review (Figure 1) [22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51].
Figure 1.
PRISMA flow diagram of the study’s selection process.
3.1. Characteristics of Included Studies
Of the 30 included studies, 13 (43%) were published within the last five years [24,25,26,27,29,31,34,36,37,45,47,50,51] and 21 (70%) within the last ten years [12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,29,33,34,35,36,37,39,42,43,44,45,46,48,50,51]. Studies on the long-term safety of prenatal exposure to paracetamol comprised the majority of the included studies (n = 27, 90%) [23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49], with two studies reporting on the long-term safety of neonatal exposure to paracetamol (7%) [50,51] and one (3%) reporting on both timings of exposure [22]. Observational epidemiologic and cohort studies were the most common study designs (27, 90%) [23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49]. The study by Persky et al. was an RCT that randomized pregnant women to receive health education alone or health education plus education on reducing household asthma triggers. Education on paracetamol as a risk factor for the development of asthma was not discussed, and the authors collected maternal self-report of medication use in pregnancy and compared the occurrence of respiratory endpoints at one year of life among children of women who used and who did not use paracetamol during pregnancy [40]. As maternal paracetamol use was not randomized, we treated this study as an observational cohort for the purpose of our review. Two RCTs (7%) were included in the review [50,51]. The remaining study (3%) used an ecologic design [22] (Table 2 and Table 3; Supplementary Tables S1 and S2).
Table 2.
Characteristics of included studies on the long-term safety of prenatal paracetamol exposure.
Table 3.
Characteristics of included studies on the long-term safety of neonatal paracetamol exposure.
3.2. Prenatal Exposure
For the studies that reported the long-term safety of prenatal paracetamol exposure, 13 (46%) [22,23,24,25,26,27,28,29,30,31,32,33,34], 11 (39%) [35,36,37,38,39,40,41,42,43,44,49] and four (15%) [45,46,47,48] focused on neurodevelopmental, atopic and reproductive adverse outcomes, respectively.
3.2.1. Neurodevelopmental Adverse Outcomes
Of the 13 studies that examined the occurrence of neurodevelopmental adverse outcomes, 12 (92%) were observational cohort studies [23,24,25,26,27,28,29,30,31,32,33,34]. The other study (8%) used an ecologic design [22]. Of the 12 cohort studies, 10 used self-reported questionnaires [23,24,27,28,29,30,31,32,33,34] and two used umbilical cord and maternal plasma biomarkers [25,26] to assess prenatal exposure to paracetamol. Behavioral, performance, intelligence, executive and psychomotor function problems, autism spectrum disorder (ASD), attention deficit hyperactivity disorder (ADHD) and cerebral palsy (CP) were the neurodevelopmental outcomes assessed. Impaired neurodevelopment was reported in 11 studies, with specific reports of increased conduct problems (relative risk (RR) 1.35, 95% confidence interval (CI) 1.13–1.6), ADHD (odds ratio (OR) 1.88, 95% CI 1.18–3.00 and RR 1.13, 95% CI 1.01–1.27), hyperactivity symptoms (RR 1.22, 95% CI 1.04–1.43), motor milestone delays (OR 1.35, 95% CI 1.07–1.70) and hyperkinetic disorders (OR 1.37, 95% CI 1.19–1.59) among children with prenatal paracetamol exposure [23,24,25,26,27,28,29,30,32,33,34].
The ecologic study investigated the risk of prenatal paracetamol exposure and ASD using the national statistics on maternal use of paracetamol and the occurrence of ASD in nine countries. This study showed that each country’s average prenatal paracetamol use correlated with its ASD prevalence (r = 0.80, 95% CI 0.22–0.47) [22].
3.2.2. Atopic Adverse Outcomes
Eleven studies investigated prenatal exposure to paracetamol and the risk of atopic adverse outcomes, using observational cohort (n = 10, 91%) [35,37,38,39,40,41,42,43,44,49] or epidemiologic (n = 1, 9%) [36] designs. The associations between paracetamol exposure and the occurrence of atopic adverse outcomes were identified via self-report (questionnaires, n = 8, 73% [36,37,38,40,41,42,43,49], interviews, n = 2, 18% [39,44]) and prescription records (n = 1, 9%) [35]. The study by Sordillo et al. also used serum levels of IgE as a marker of atopic adverse outcomes [43]. All studies (n = 11, 100%) reported an independent association between prenatal exposure to paracetamol and the risk of atopic adverse outcomes in childhood [35,36,37,38,39,40,41,42,43,44,49].
3.2.3. Reproductive Adverse Outcomes
Four cohort studies investigated prenatal exposure to paracetamol and the risk of reproductive adverse outcomes [45,46,47,48]. All studies used maternal self-administered questionnaires to identify the trimester-based exposure to paracetamol. The occurrence of reproductive adverse outcomes was assessed via physical examination (n = 3, 75%) [46,47,48] and parent or child self-report (n = 1, 25%) [45]. Anogenital distance (AGD) (n = 2, 50%) [46,47], hypospadias or cryptorchidism (n = 1, 25%) [48] and the timing of pubertal development (n = 1, 25%) [45] were the target outcome variables. Three studies (75%) found a strong relationship between prenatal exposure to paracetamol and the development of reproductive adverse outcomes [45,46,48]. One of the two cohort studies that examined the association between prenatal analgesic exposure and AGD in offspring did not find a significant association between prenatal paracetamol exposure alone and the risk of shorter AGD at three months of age. However, the combined exposure to paracetamol and NSAIDs was significantly associated with reduced AGD at three months of age (AGD −4.1 mm; 95% CI 6.4–1.7) [47].
3.3. Neonatal Outcomes
Three studies examined long-term safety outcomes among neonates exposed to paracetamol [22,50,51]. Two studies (67%) focused on neurodevelopmental adverse outcomes only [22,51]. The other study (33%) examined neurodevelopmental and atopic adverse outcomes [51].
Neurodevelopmental and Atopic Adverse Outcomes
The first study used an ecologic design to investigate the country-level association between the rate of circumcision as an index of early life exposure to paracetamol and the rate of ASD. A strong correlation (r = 0.98) was found between circumcision and rate of autism for countries with data after 1995 [22]. The second study was a follow-up of an RCT that examined neurodevelopmental outcomes among neonates who received paracetamol or ibuprofen for PDA closure at 25 to 30 weeks’ gestation. There were no significant differences in neurodevelopmental impairment according to the Bayley Scales of Infant Development the Mental Developmental Index or the Psychomotor Developmental Index at 18 and 24 months of age [50]. The third study that focused on neurodevelopmental and atopic adverse outcomes was an RCT that examined paracetamol compared to a placebo for PDA closure in neonates 23 to 31 weeks’ gestation. There was no significant difference in neurodevelopmental or atopic outcomes between the two groups at two and five years of age [51].
3.4. Risk-of-Bias Assessment and Assessment of Evidence Certainty
3.4.1. Risk-of-Bias Assessment
The risk of bias of the included observational epidemiologic and cohort studies [19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45] was assessed using the Newcastle–Ottawa Quality Assessment Scale for Cohort Studies [15]. All but three of the included observational studies received a rating between seven and nine, indicating a low risk of bias (Supplementary Table S3).
We used the RoB 2 tool [19] to determine the risk of bias of the included RCTs [46,47]. We rated the risk of bias of the included RCTs as low and with some concerns (Supplementary Figure S1).
To assess the quality of the ecologic study by Bauer et al. [18], we used the modified tool for assessing the Quality of Modern Cross-Sectional Ecologic Studies [16,17,18] (Supplementary Table S4). The study received a rating of 17, indicating high study quality.
3.4.2. Assessment of Evidence Certainty
We rated the certainty of the evidence on the long-term safety of prenatal paracetamol exposure as low. This was due to the observational design of the included studies and serious imprecision and inconsistency (Supplementary Tables S5 and S6).
We rated the certainty of the evidence on the long-term safety of neonatal paracetamol exposure as moderate. This was due to very serious imprecision and serious inconsistency of the included studies (Supplementary Tables S7 and S8).
4. Discussion
4.1. Summary of Findings
The results of the current systematic review suggest that prenatal exposure to paracetamol is associated with an increased risk of neurodevelopmental, atopic and reproductive adverse outcomes, independent of the timing and cumulative dosing of exposure. The ecologic study that examined the association between neonatal paracetamol exposure and neurodevelopmental adverse outcomes also demonstrated a correlation between neonatal exposure to paracetamol and neurodevelopmental adverse outcomes. However, neither of the two available RCTs on neonatal exposure to paracetamol showed an increased risk of neurodevelopmental or atopic adverse outcomes. Although two of the three available studies on neonatal exposure were RCTs, they were limited in their assessment of long-term safety outcomes, due to their small sample sizes. Furthermore, the exposure to paracetamol was limited to four days in duration and 200 mg/kg of cumulative dosing. In contrast, among the studies examining prenatal exposure, the duration of exposure and cumulative dosing were often more remarkable.
4.2. Comparison with Other Research
Studies on transplacental transfer of paracetamol have shown that paracetamol crosses the placental barrier rapidly via passive diffusion with significantly faster maternal-to-fetal than fetal-to-maternal transfer, transferring up to 50% of the original dose [52]. Besides the free cross through the placenta, maternal use of paracetamol has also been shown to be associated with placental CpG methylation [53]. Several studies have linked adverse placental growth and function and poor fetal and long-term health outcomes to placental DNA methylation [54,55,56]. Although paracetamol is mainly metabolized in the liver, evidence has shown that a small amount of para-aminophenol produced from paracetamol metabolism combines with arachidonic acid to produce N-arachidonoylaminophenol (AM404) [57]. AM404 is an indirect agonist at the cannabinoid receptors and has a disruptive effect on the normal function of the endocannabinoid system, an identified factor in the pathophysiology of neurodevelopmental disorders [8]. The endocannabinoid system has an important role in regulating early brain development through neuronal migration and proliferation of progenitor cells [58]. Exposure to paracetamol in the early stages of brain development could interfere with variable neuroprotein dynamics in different areas of the brain, such as the hippocampus and cerebral cortex, causing variable degrees of impairment in neurodevelopmental pathways and long-term neurodevelopment [9,59].
Paracetamol use is also associated with decreased glutathione levels, resulting in increased oxidant-induced inflammation and enhancement of T-helper type-2 pathways. This could be the biological basis for a link between paracetamol and atopic adverse outcomes [10]. The available evidence also points toward paracetamol causing a perturbance in the hormonal process, such as steroidogenesis and depletion of sulfated sex hormones [60], providing the biological plausibility for the potential alteration in the development of the fetal reproductive system that is associated with paracetamol exposure.
Paracetamol is a drug with multidirectional mechanisms of action consisting of inhibition of cyclooxygenases, involvement in the endocannabinoid system, serotonergic pathways, potassium and calcium channels and ultimately L-arginine in the nitric oxide synthesis pathway [9]. All of these mechanisms have key roles in hemostatic function of several regulatory systems. This raises remarkable controversy over the use of paracetamol during critical periods of organogenesis.
4.3. Strengths and Limitations
Our systematic review aimed to examine the available research on prenatal and neonatal paracetamol exposure and long-term safety outcomes. Although we collected a considerable amount of evidence on prenatal exposure, most studies used observational designs. Thus, these studies are vulnerable to the limitations of observational data, including the inability to establish cause–effect relationships. In addition, although two of the studies that focused on neonatal exposure were RCTs, the conclusions that could be drawn from their results were limited, due to the studies’ small sample sizes.
In our review protocol, we indicated that we intended to collect data on neonatal pharmacokinetics (PK) and pharmacodynamics (PD). We also planned to evaluate the short-term adverse events associated with neonatal paracetamol exposure [14]. As the included studies did not report on PK, PD or short-term adverse events, we were unable to synthesize data on these secondary outcomes.
5. Conclusions
The available evidence suggests a possible association between prenatal exposure to paracetamol and an increased risk of neurodevelopmental, atopic and reproductive adverse outcomes. This is supported by the current knowledge of paracetamol’s mechanism of action and biologic plausibility. However, the evidence is limited to observational studies and prone to biases, such as confounding by indication. Our review did not find an association between neonatal exposure to paracetamol and neurodevelopmental, atopic or reproductive adverse outcomes. However, the lack of quantity of the available evidence limits our conclusions. Considering the recent increase in early life exposure to paracetamol and the possible risk of long-term adverse outcomes, as shown in this review, there is an immediate need for robust data from using more rigorous methodologies. Until further data are available, the currently existing information needs to be investigated by the safety advisory committees of drug-regulatory agencies so that timely and appropriate labeling updates can be made and accessed by consumers and healthcare providers.
Supplementary Materials
The following supporting information can be downloaded at. https://www.mdpi.com/article/10.3390/ijerph19042128/s1. Table S1: Characteristics of included studies on the long-term safety of prenatal paracetamol exposure. Table S2: Characteristics of included studies on the long-term safety of neonatal paracetamol exposure. Table S3: Risk-of-bias assessment of the included observational studies using the NOS. Table S4: Risk-of-bias assessment of the included ecologic study, using the modified tool for assessing the Quality of Modern Cross-Sectional Ecologic Studies. Table S5: Certainty of the evidence on the long-term safety of prenatal paracetamol exposure. Table S6: Summary of findings on the long-term safety of prenatal paracetamol exposure. Table S7: Certainty of the evidence on the long-term safety of neonatal paracetamol exposure, Table S8: Summary of findings on the long-term safety of neonatal paracetamol exposure. Figure S1: Risk-of-bias assessment summary—review of authors’ judgements about each risk-of-bias Item in RoB 2 for the included randomized controlled trials.
Author Contributions
Conceptualization, S.S.-Z. and J.v.d.A.; methodology, S.S.-Z.; data curation, R.P. and K.S.; writing—original draft preparation, R.P.; writing—review and editing, K.S., S.S.-Z. and J.v.d.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We thank Laura Banfield, the librarian at McMaster University Health Sciences Library, for her consultation in the development of our search strategies.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Schilling, A.; Corey, R.; Leonard, M.; Eghtesad, B. Acetaminophen: Old drug, new warnings. Clevel. Clin. J. Med. 2010, 77, 19–27. [Google Scholar] [CrossRef]
- Wright, C.J. Acetaminophen and the Developing Lung: Could There Be Lifelong Consequences? J. Pediatr. 2021, 235, 264–276.e1. [Google Scholar] [CrossRef] [PubMed]
- Allegaert, K. A Critical Review on the Relevance of Paracetamol for Procedural Pain Management in Neonates. Front. Pediatr. 2020, 8, 89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van den Bosch, G.E.; Dijk, M.V.; Tibboel, D.; de Graaff, J.C. Long-term Effects of Early Exposure to Stress, Pain, Opioids and Anaesthetics on Pain Sensitivity and Neurocognition. Curr. Pharm. Des. 2017, 23, 5879–5886. [Google Scholar] [CrossRef] [PubMed]
- Mitra, S.; Florez, I.D.; Tamayo, M.E.; Mbuagbaw, L.; Vanniyasingam, T.; Veroniki, A.A.; Zea, A.M.; Zhang, Y.; Sadeghirad, B.; Thabane, L. Association of Placebo, Indomethacin, Ibuprofen, and Acetaminophen with Closure of Hemodynamically Significant Patent Ductus Arteriosus in Preterm Infants: A Systematic Review and Meta-analysis. JAMA 2018, 319, 1221–1238. [Google Scholar] [CrossRef]
- Van den Anker, J.N.; Allegaert, K. Acetaminophen in the Neonatal Intensive Care Unit: Shotgun Approach or Silver Bullet. J. Pediatr. 2018, 198, 10–11. [Google Scholar] [CrossRef] [Green Version]
- Bardanzellu, F.; Neroni, P.; Dessì, A.; Fanos, V. Paracetamol in Patent Ductus Arteriosus Treatment: Efficacious and Safe? Biomed. Res. Int. 2017, 2017, 1438038. [Google Scholar] [CrossRef]
- Saliba, S.W.; Marcotegui, A.R.; Fortwängler, E.; Ditrich, J.; Perazzo, J.C.; Muñoz, E.; de Oliveira, A.C.P.; Fiebich, B.L. AM404, paracetamol metabolite, prevents prostaglandin synthesis in activated microglia by inhibiting COX activity. J. Neuroinflammation 2017, 14, 246. [Google Scholar] [CrossRef] [Green Version]
- Przybyła, G.W.; Szychowski, K.A.; Gmiński, J. Paracetamol—An old drug with new mechanisms of action. Clin. Exp. Pharmacol. Physiol 2020. ahead of print. [Google Scholar] [CrossRef]
- Farquhar, H.; Stewart, A.; Mitchell, E.; Crane, J.; Eyers, S.; Weatherall, M.; Beasley, R. The role of paracetamol in the pathogenesis of asthma. Clin. Exp. Allergy 2010, 40, 32–41. [Google Scholar] [CrossRef]
- Allegaert, K.; Van Den Anker, J. How to translate neuro-cognitive and behavioural outcome data in animals exposed to paracetamol to the human perinatal setting? Arch. Med. Sci. 2020, 1–13. [Google Scholar] [CrossRef]
- Aromataris, E.; Munn, Z. JBI Manual for Evidence Synthesis. 2020. Available online: https://synthesismanual.jbi.global (accessed on 31 October 2021).
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ionnidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies that Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samiee-Zafarghandy, S.; Sushko, K.; Van Den Anker, J. Long-Term Safety of Prenatal and Neonatal Exposure to Paracetamol: A Protocol for a Systematic Review. BMJ Paediatr. Open 2020, 4, e000907. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2013. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 31 October 2021).
- Dufault, B.; Klar, N. The quality of modern cross-sectional ecologic studies: A bibliometric review. Am. J. Epidemiol. 2011, 174, 1101–1107. [Google Scholar] [CrossRef] [PubMed]
- Betran, A.P.; Torloni, M.R.; Zhang, J.; Ye, J.; Mikolajczyk, R.; Deneux-Tharaux, C.; Oladapo, O.T.; Souza, J.P.; Tunçalp, Ö.; Vogel, J.P. What is the optimal rate of caesarean section at population level? A systematic review of ecologic studies. Reprod. Health 2015, 12, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cortes-Ramirez, J.; Naish, S.; Sly, P.D.; Jagals, P. Mortality and morbidity in populations in the vicinity of coal mining: A systematic review. BMC Public Health 2018, 18, 721. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Granholm, A.; Alhazzani, W.; Møller, M.H. Use of the GRADE approach in systematic reviews and guidelines. Br. J. Anaesth. 2019, 123, 554–559. [Google Scholar] [CrossRef]
- Murad, M.H.; Mustafa, R.A.; Schünemann, H.J.; Sultan, S.; Santesso, N. Rating the certainty in evidence in the absence of a single estimate of effect. Evid. Based Med. 2017, 22, 85–87. [Google Scholar] [CrossRef] [Green Version]
- Bauer, A.Z.; Kriebel, D. Prenatal and perinatal analgesic exposure and autism: An ecological link. Environ. Health 2013, 12, 41. [Google Scholar] [CrossRef] [Green Version]
- Stergiakouli, E.; Thapar, A.; Davey Smith, G. Association of Acetaminophen Use During Pregnancy with Behavioral Problems in Childhood: Evidence Against Confounding. JAMA Pediatr. 2016, 170, 964–970. [Google Scholar] [CrossRef] [Green Version]
- Bertoldi, A.D.; Rifas-Shiman, S.L.; Boing, A.C.; da Silva Dal Pizzol, T.; Miranda, V.I.A.; Silveira, M.P.T.; Freitas Silveira, M.; Domingues, M.R.; Santos, I.S.; Bassani, D.G.; et al. Associations of acetaminophen use during pregnancy and the first year of life with neurodevelopment in early childhood. Paediatr. Perinat. Epidemiol. 2020, 34, 267–277. [Google Scholar] [CrossRef] [PubMed]
- Ji, Y.; Riley, A.W.; Lee, L.C.; Hong, X.; Wang, G.; Tsai, H.J.; Mueller, N.T.; Pearson, C.; Thermitus, J.; Panjwani, A.; et al. Maternal Biomarkers of Acetaminophen Use and Offspring Attention Deficit Hyperactivity Disorder. Brain Sci. 2018, 8, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ji, Y.; Azuine, R.E.; Zhang, Y.; Hou, W.; Hong, X.; Wang, G.; Riley, A.; Pearson, C.; Zuckerman, B.; Wang, X. Association of Cord Plasma Biomarkers of In Utero Acetaminophen Exposure with Risk of Attention-Deficit/Hyperactivity Disorder and Autism Spectrum Disorder in Childhood. JAMA Psychiatry 2020, 77, 180–189. [Google Scholar] [CrossRef] [PubMed]
- Golding, J.; Gregory, S.; Clark, R.; Ellis, G.; Iles-Caven, Y.; Northstone, K. Associations between paracetamol (acetaminophen) intake between 18 and 32 weeks gestation and neurocognitive outcomes in the child: A longitudinal cohort study. Paediatr. Perinat. Epidemiol. 2020, 34, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Vlenterie, R.; Wood, M.E.; Brandlistuen, R.E.; Roeleveld, N.; van Gelder, M.M.; Nordeng, H. Neurodevelopmental problems at 18 months among children exposed to paracetamol in utero: A propensity score matched cohort study. Int. J. Epidemiol. 2016, 45, 1998–2008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ystrom, E.; Gustavson, K.; Brandlistuen, R.E.; Knudsen, G.P.; Magnus, P.; Susser, E.; Davey Smith, G.; Stoltenberg, C.; Surén, P.; Håberg, S.E.; et al. Prenatal Exposure to Acetaminophen and Risk of ADHD. Pediatrics 2017, 140, e20163840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liew, Z.; Bach, C.C.; Asarnow, R.F.; Ritz, B.; Olsen, J. Paracetamol use during pregnancy and attention and executive function in offspring at age 5 years. Int. J. Epidemiol. 2016, 45, 2009–2017. [Google Scholar] [CrossRef]
- Rifas-Shiman, S.L.; Cardenas, A.; Hivert, M.F.; Tiemeier, H.; Bertoldi, A.D.; Oken, E. Associations of prenatal or infant exposure to acetaminophen or ibuprofen with mid-childhood executive function and behaviour. Paediatr. Perinat. Epidemiol. 2020, 34, 287–298. [Google Scholar] [CrossRef]
- Streissguth, A.P.; Treder, R.P.; Barr, H.M.; Shepard, T.H.; Bleyer, W.A.; Sampson, P.D.; Martin, D.C. Aspirin and acetaminophen use by pregnant women and subsequent child IQ and attention decrements. Teratology 1987, 35, 211–219. [Google Scholar] [CrossRef]
- Thompson, J.M.; Waldie, K.E.; Wall, C.R.; Murphy, R.; Mitchell, E.A.; ABC Study Group. Associations between acetaminophen use during pregnancy and ADHD symptoms measured at ages 7 and 11 years. PLoS ONE 2014, 9, e108210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, T.G.; Liew, Z.; Andersen, A.N.; Andersen, G.L.; Andersen, P.K.; Martinussen, T.; Olsen, J.; Rebordosa, C.; Tollånes, M.C.; Uldall, P.; et al. Use of paracetamol, ibuprofen or aspirin in pregnancy and risk of cerebral palsy in the child. Int. J. Epidemiol. 2018, 47, 121–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, A.B.; Farkas, D.K.; Mehnert, F.; Ehrenstein, V.; Erichsen, R. Use of prescription paracetamol during pregnancy and risk of asthma in children: A population-based Danish cohort study. Clin. Epidemiol. 2012, 4, 33–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Marcos, L.; Sanchez-Solis, M.; Perez-Fernandez, V.; Pastor-Vivero, M.D.; Mondejar-Lopez, P.; Valverde-Molina, J. Is the effect of prenatal paracetamol exposure on wheezing in preschool children modified by asthma in the mother? Int. Arch. Allergy Immunol. 2009, 149, 33–37. [Google Scholar] [CrossRef]
- Piler, P.; Švancara, J.; Kukla, L.H. Role of combined prenatal and postnatal paracetamol exposure on asthma development: The Czech ELSPAC study. J. Epidemiol. Community Health 2018, 72, 349–355. [Google Scholar] [CrossRef]
- Shaheen, S.O.; Newson, R.B.; Sherriff, A.; Henderson, A.J.; Heron, J.E.; Burney, P.G.; Golding, J.; ALSPAC Study Team. Paracetamol use in pregnancy and wheezing in early childhood. Thorax 2002, 57, 958–963. [Google Scholar] [CrossRef] [Green Version]
- Jedrychowski, W.; Spengler, J.D.; Maugeri, U.; Miller, R.L.; Budzyn-Mrozek, D.; Perzanowski, M.; Flak, E.; Mroz, E.; Majewska, R.; Kaim, I.; et al. Effect of prenatal exposure to fine particulate matter and intake of Paracetamol (Acetaminophen) in pregnancy on eczema occurrence in early childhood. Sci Total Environ. 2011, 409, 5205–5209. [Google Scholar] [CrossRef] [Green Version]
- Persky, V.; Piorkowski, J.; Hernandez, E.; Chavez, N.; Wagner-Cassanova, C.; Vergara, C.; Pelzel, D.; Enriquez, R.; Gutierrez, S.; Busso, A. Prenatal exposure to acetaminophen and respiratory symptoms in the first year of life. Ann Allergy Asthma Immunol. 2008, 101, 271–278. [Google Scholar] [CrossRef] [Green Version]
- Rebordosa, C.; Kogevinas, M.; Sørensen, H.T.J. Pre-natal exposure to paracetamol and risk of wheezing and asthma in children: A birth cohort study. Int. J. Epidemiol. 2008, 37, 583–590. [Google Scholar] [CrossRef] [Green Version]
- Magnus, M.C.; Karlstad, Ø.; Håberg, S.E.; Nafstad, P.; Davey Smith, G.; Nystad, W. Prenatal and infant paracetamol exposure and development of asthma: The Norwegian Mother and Child Cohort Study. Int. J. Epidemiol. 2016, 45, 512–522. [Google Scholar] [CrossRef] [Green Version]
- Sordillo, J.E.; Scirica, C.V.; Rifas-Shiman, S.L.; Gillman, M.W.; Bunyavanich, S.; Camargo CAJr Weiss, S.T.; Gold, D.R.; Litonjua, A.A. Prenatal and infant exposure to acetaminophen and ibuprofen and the risk for wheeze and asthma in children. J. Allergy Clin. Immunol. 2015, 135, 441–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakkeheim, E.; Mowinckel, P.; Carlsen, K.H.; Håland, G.; Carlsen, K.C. Paracetamol in early infancy: The risk of childhood allergy and asthma. Acta Paediatr. 2011, 100, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Ernst, A.; Brix, N.; Lauridsen, L.L.B.; Olsen, J.; Parner, E.T.; Liew, Z.; Olsen, L.H.; Ramlau-Hansen, C.H. Acetaminophen (Paracetamol) Exposure During Pregnancy and Pubertal Development in Boys and Girls from a Nationwide Puberty Cohort. Am. J. Epidemiol. 2019, 188, 34–46. [Google Scholar] [CrossRef] [PubMed]
- Fisher, B.G.; Thankamony, A.; Hughes, I.A.; Ong, K.K.; Dunger, D.B.; Acerini, C.L. Prenatal paracetamol exposure is associated with shorter anogenital distance in male infants. Hum. Reprod. 2016, 31, 2642–2650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lind, D.V.; Main, K.M.; Kyhl, H.B.; Kristensen, D.M.; Toppari, J.; Andersen, H.R.; Andersen, M.S.; Skakkebæk, N.E.; Jensen, T.K. Maternal use of mild analgesics during pregnancy associated with reduced anogenital distance in sons: A cohort study of 1027 mother-child pairs. Hum. Reprod. 2017, 32, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Snijder, C.A.; Kortenkamp, A.; Steegers, E.A.; Jaddoe, V.W.; Hofman, A.; Hass, U.; Burdorf, A. Intrauterine exposure to mild analgesics during pregnancy and the occurrence of cryptorchidism and hypospadia in the offspring: The Generation R Study. Hum. Reprod. 2012, 27, 1191–1201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaheen, S.O.; Newson, R.B.; Ring, S.M.; Rose-Zerilli, M.J.; Holloway, J.W.; Henderson, A.J. Prenatal and infant acetaminophen exposure, antioxidant gene polymorphisms, and childhood asthma. J. Allergy Clin. Immunol. 2010, 126, 1141–1148. [Google Scholar] [CrossRef] [Green Version]
- Oncel, M.Y.; Eras, Z.; Uras, N.; Canpolat, F.E.; Erdeve, O.; Oguz, S.S. Neurodevelopmental Outcomes of Preterm Infants Treated with Oral Paracetamol Versus Ibuprofen for Patent Ductus Arteriosus. Am. J. Perinatol. 2017, 34, 1185–1189. [Google Scholar] [CrossRef]
- Juujärvi, S.; Saarela, T.; Hallman, M.; Aikio, O. Trial of paracetamol for premature newborns: Five-year follow-up. J. Matern. Fetal Neonatal Med. 2021, 21, 1–3. [Google Scholar] [CrossRef]
- Nitsche, J.F.; Patil, A.S.; Langman, L.J.; Penn, H.J.; Derleth, D.; Watson, W.J.; Brost, B.C. Transplacental Passage of Acetaminophen in Term Pregnancy. Am. J. Perinatol. 2017, 34, 541–543. [Google Scholar] [CrossRef] [Green Version]
- Addo, K.A.; Bulka, C.; Dhingra, R.; Santos, H.P., Jr.; Smeester, L.; O’Shea, T.M.; Fry, R.C. Acetaminophen use during pregnancy and DNA methylation in the placenta of the extremely low gestational age newborn (ELGAN) cohort. Environ. Epigenet. 2019, 5, dvz010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, B.B.; Karagas, M.R.; Punshon, T.; Jackson, B.P.; Robbins, D.J.; Houseman, E.A.; Marsit, C.J. Epigenome-Wide Assessment of DNA Methylation in the Placenta and Arsenic Exposure in the New Hampshire Birth Cohort Study (USA). Environ. Health Perspect. 2016, 124, 1253–1260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maccani, J.Z.; Koestler, D.C.; Houseman, E.A.; Armstrong, D.A.; Marsit, C.J.; Kelsey, K.T. DNA methylation changes in the placenta are associated with fetal manganese exposure. Reprod. Toxicol. 2015, 57, 43–49. [Google Scholar] [CrossRef] [Green Version]
- Marsit, C.J.; Maccani, M.A.; Padbury, J.F.; Lester, B.M. Placental 11-beta hydroxysteroid dehydrogenase methylation is associated with newborn growth and a measure of neurobehavioral outcome. PLoS ONE 2012, 7, e33794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slattery, W.T.; Klegeris, A. Acetaminophen metabolites p-aminophenol and AM404 inhibit microglial activation. Neuroimmunol. Neuroinflammation 2018, 5. [Google Scholar] [CrossRef] [Green Version]
- Fride, E.; Gobshtis, N.; Dahan, H.; Weller, A.; Giuffrida, A.; Ben-Shabat, S. The endocannabinoid system during development: Emphasis on perinatal events and delayed effects. Vitam. Horm. 2009, 81, 139–158. [Google Scholar] [CrossRef]
- Blecharz-Klin, K.; Piechal, A.; Jawna-Zboińska, K.; Pyrzanowska, J.; Wawer, A.; Joniec-Maciejak, I.; Widy-Tyszkiewicz, E. Paracetamol—Effect of early exposure on neurotransmission, spatial memory and motor performance in rats. Behav. Brain Res. 2017, 323, 162–171. [Google Scholar] [CrossRef]
- Cohen, I.V.; Cirulli, E.T.; Mitchell, M.W.; Jonsson, T.J.; Yu, J.; Shah, N.; Spector, T.D.; Guo, L.; Venter, J.C.; Telenti, A. Acetaminophen (Paracetamol) Use Modifies the Sulfation of Sex Hormones. EBioMedicine 2018, 28, 316–323. [Google Scholar] [CrossRef] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).