
Group Triple P Intervention Effects on Children and Parents: A Systematic Review and Meta-Analysis

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Search Methods
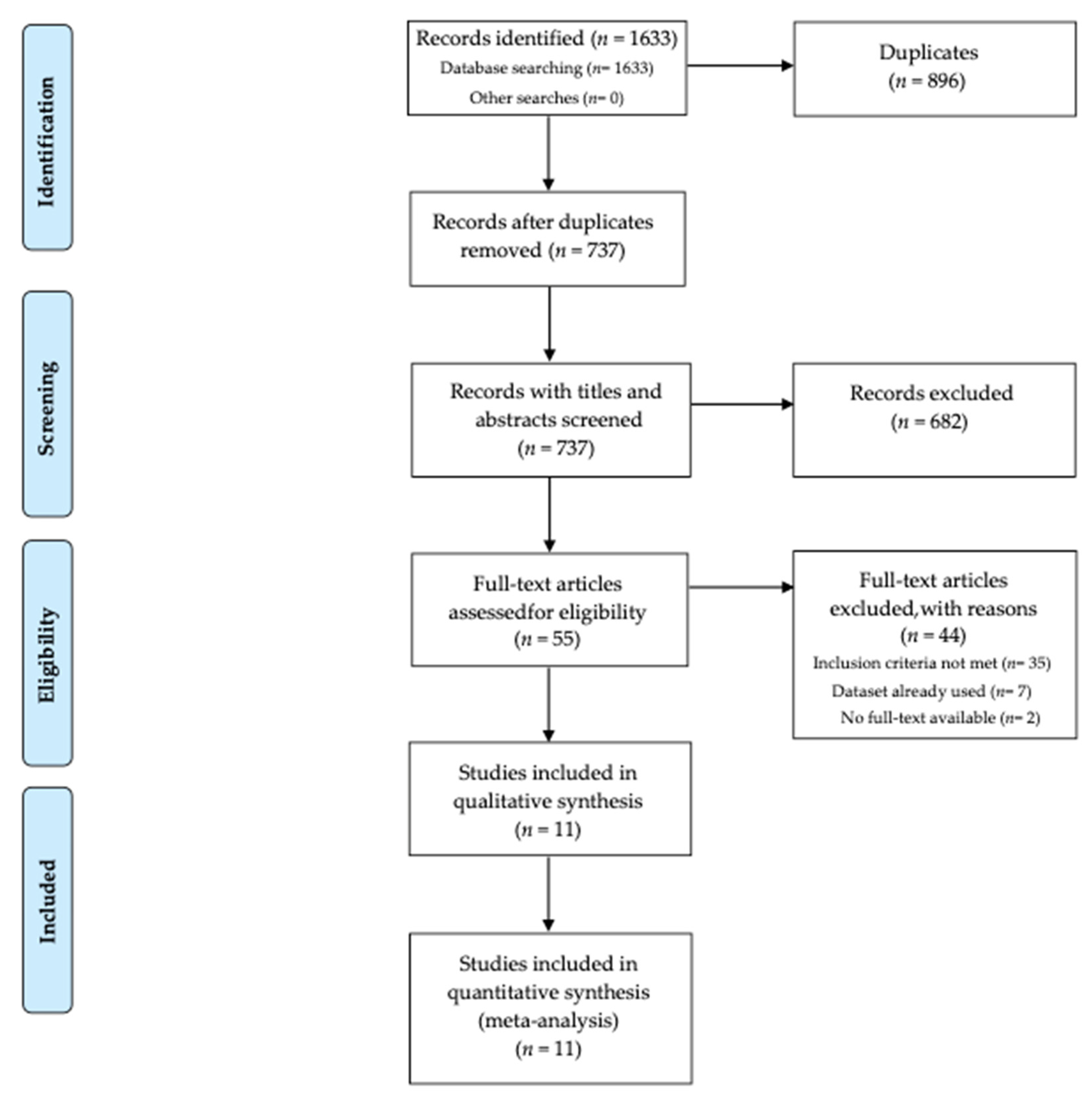
2.4. Data Selection and Analysis
2.5. Data Extraction and Management

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors, Year | Design | Groups | Triple P Intervention/Control Group (I1/I2/C) | Study Approach | Setting | Measurement Time Points | Sample Size (N) | Child Mean Age (Range) | % Boys | Developer Involvement | Country | Attrition Rate Post-Intervention I1/C or I1/I2/C | SES | Parent Measures | Child Measures |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Au et al., 2014 [25] | RCT | 1 I, 1 C | GTP + 1 ADHD booster session/waitlist | Target | clinical (ADHD) | Pre, Post, 3-moFU | 17 | 7.81 years (5–10) | 94.1 | 2 | Hong Kong | NR | NR | PSOC | ECBI |
| Bodenmann et al., 2008 [26] | RCT | 2 I, 1 C | GTP/CCET/ waitlist | Universal | community | Pre, Post, 6-mo FU, 12-moFU | 300 | 6.6 years (2–12) | 55.0 | 1 | Switzerland | 4%/20% | medium | PS, PSOC, PPC | ECBI |
| Chung et al., 2015 [27] | RCT | 2 I, 1 C | GTP/DI/waitlist | Universal | community | Pre, Post | 88 | 50.7 months (2–6) | 53.3 | 1 | Hong Kong | 11%/ 10%/0% | NR | PSS | ECBI |
| Frank et al., 2015 [28] | RCT | 1 I, 1 C | GTP/ waitlist | Universal | community | Pre, Post, 6-moFU | 84 | 5.55 years (3–8) | 69.0 | 1 | New Zealand | NR | high | PS, PTC, PPC, RQI | ECBI |
| Glazemakers, 2012 [29] | RCT | 1 I, 1 C | GTP/ waitlist | Treatment | clinical (psychiatric problems) | Pre, Post | 50 | 8.01 (<12) | 74.4 | 2 | Belgium | NR | NR | PS, PSI | SDQ |
| Leung et al., 2003 [30] | RCT | 1 I, 1 C | GTP/ waitlist | Target | clinic | Pre, Post | 91 | 4.23 years (3–7) | 63.8 | 1 | Hong Kong | 28.3%/20% | NR | PS, PSOC, PPC, RQI | ECBI |
| Leung et al., 2013 [31] | RCT | 1 I, 1 C | GTP/ waitlist | Target | clinical (developmental disability) | Pre, Post, 6-moFU | 81 | 49.6 months (NR) | 70.4 | 1 | Hong Kong | 7.1%/10.3% | NR | PSS, PS, PPC | ECBI |
| Matsumoto et al., 2007 [32] | RCT | 1 I, 1 C | GTP/ waitlist | Universal | community | Pre, Post, 3-moFU | 50 | 4.9 years (2–10) | 54.0 | 1 | Australia (Japanese parents) | 0 %/0 % | NR | PS, PPC, RQI, PSBC, DASS | ECBI |
| Matsumoto et al., 2010 [33] | RCT | 1 I, 1 C | GTP/ waitlist | Universal | community | Pre, Post | 54 | 5.8 years (2.2–10.3) | NR | 1 | Japan | 10.7%/0% | NR | PS, PPC, RQI, PSBC, DASS | ECBI |
| Ozyurt et al., 2019 [34] | RCT | 1 T, 1 C | GTP/ waitlist | Treatment | clinical (anxiety problems) | Pre, Post | 74 | 9.96 years (8–12) | 62.5 | 2 | Turkey | 29.7%/21.6% | NR | NR | SDQ |
| Tully & Hunt, 2017 [35] | RCT | 2 I, 1 C | GTP/BPI/ waitlist | Universal | community | Pre, Post, 6-moFU | 132 | 31 months (24–46) | 69.6 | 2 | Australia | 13%/ 8.3%/9.1 % | NR | PTC, QMI, DASS | CBCL |
2.6. Procedures to Evaluate Risk of Bias within and across Studies
2.7. Data Analyses and Statistical Approach
| Outcome Variables | Measures |
|---|---|
| Child behavior problems | Child Behavior Checklist (CBCL) [40]; Eyberg Child Behavior Inventory (ECBI) [41]; Strengths and Difficulties Questionnaire (SDQ) [42]. |
| Dysfunctional parenting practices (total score), laxness subscale, and over-reactivity subscale | Parenting Scale (PS) [43]. |
| Parenting sense of competence | Problem Setting and Behavior Checklist (PSBC) [44]; Parenting Sense of Competence (PSOC) [45]; Parenting Tasks Checklist (PTC) [46]. |
| Parental adjustment, depression levels, anxiety levels, and stress levels | Depression Anxiety Stress Scales (DASS) [47]. |
| Parental stress levels | Parenting Stress Index (PSI) [48]; Chinese Parental Stress Scale (PSS) [49]. |
| Parental conflict | Parent Problem Checklist (PPC) [50]. |
| Parental relationship | Relationship Quality Index (RQI) [51]; Quality of Marriage Index (QMI) [51]. |
3. Results
3.1. Study Characteristics
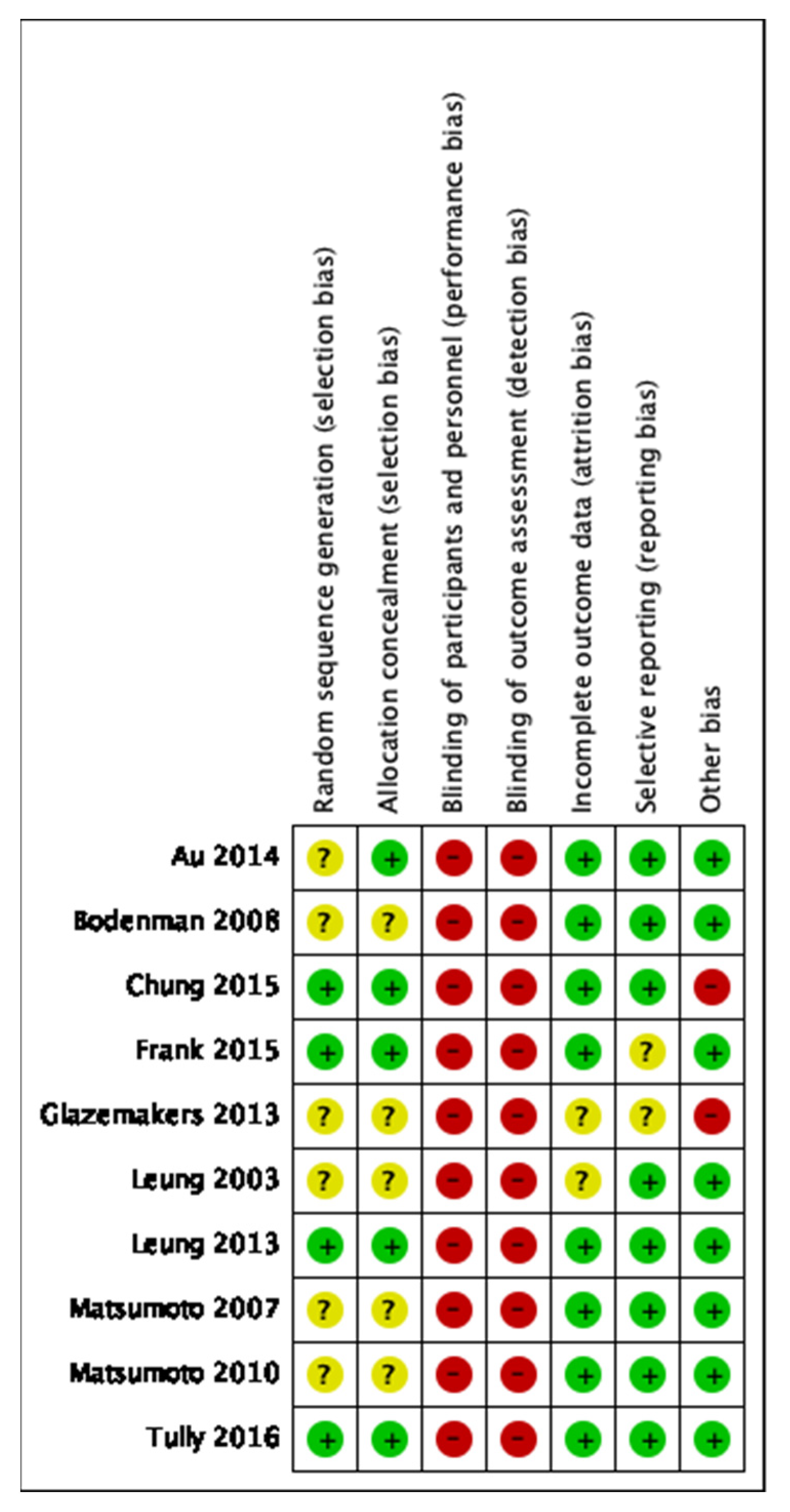
3.2. Risk of Bias within and across Studies
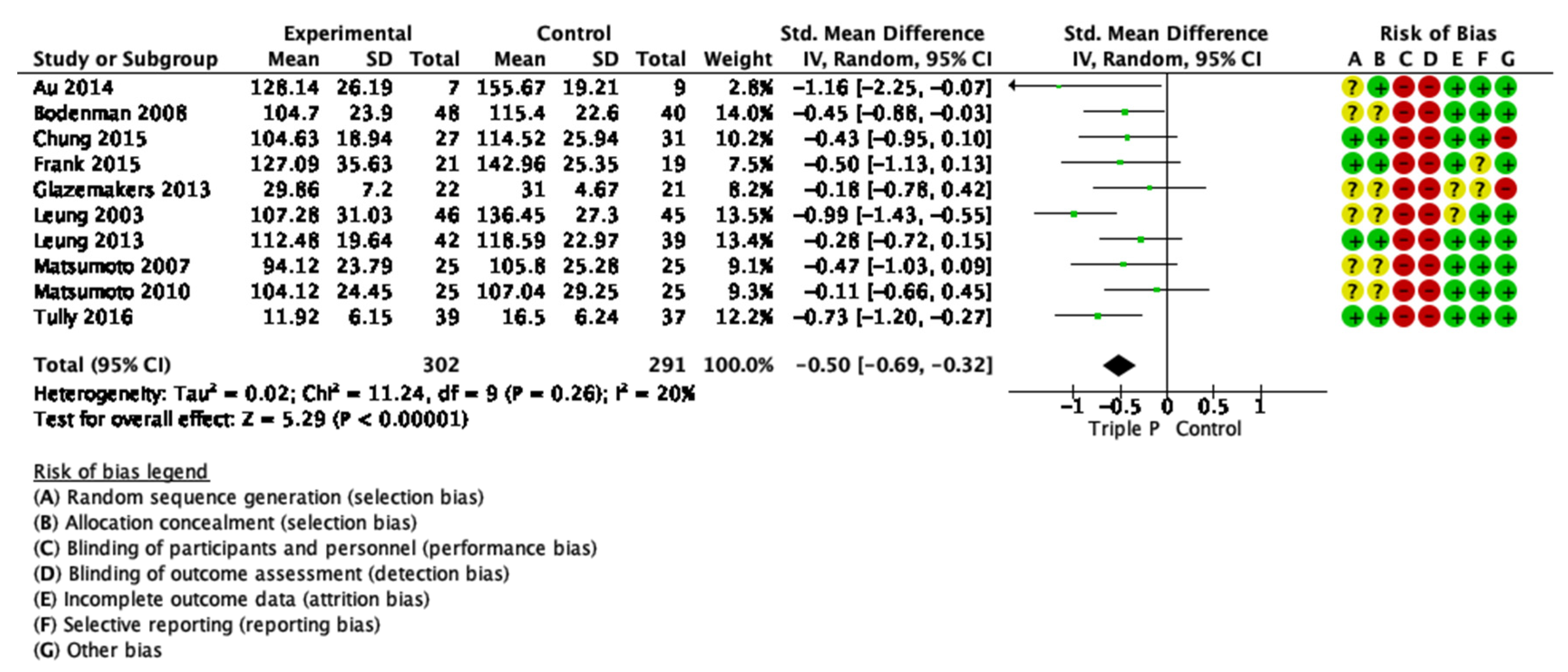
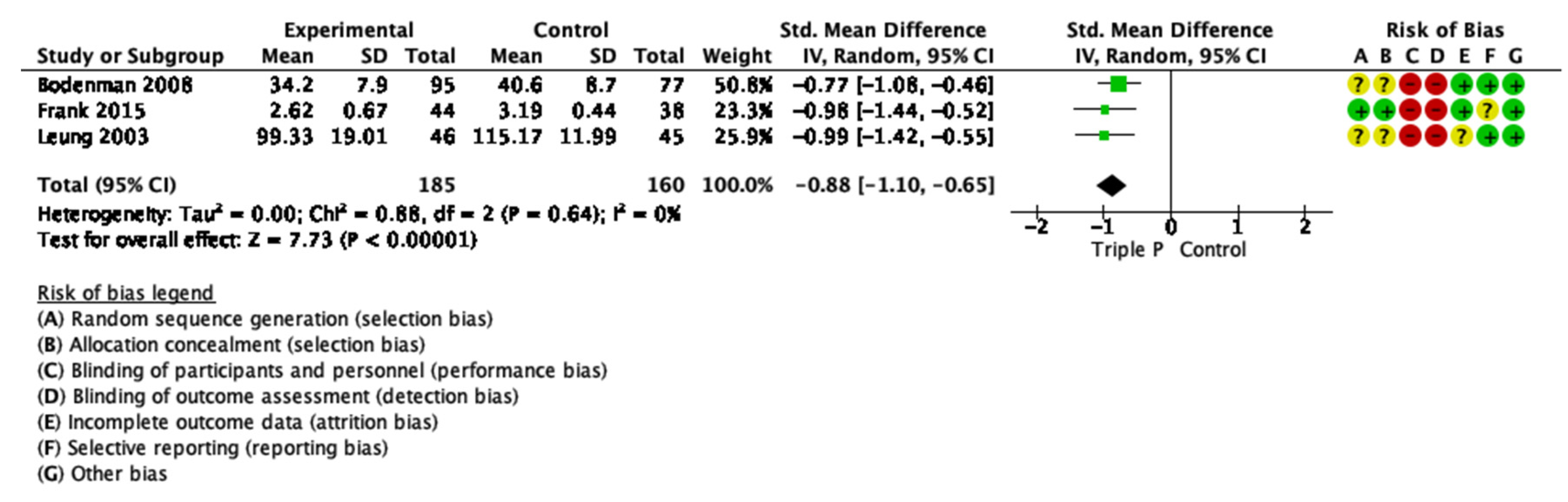
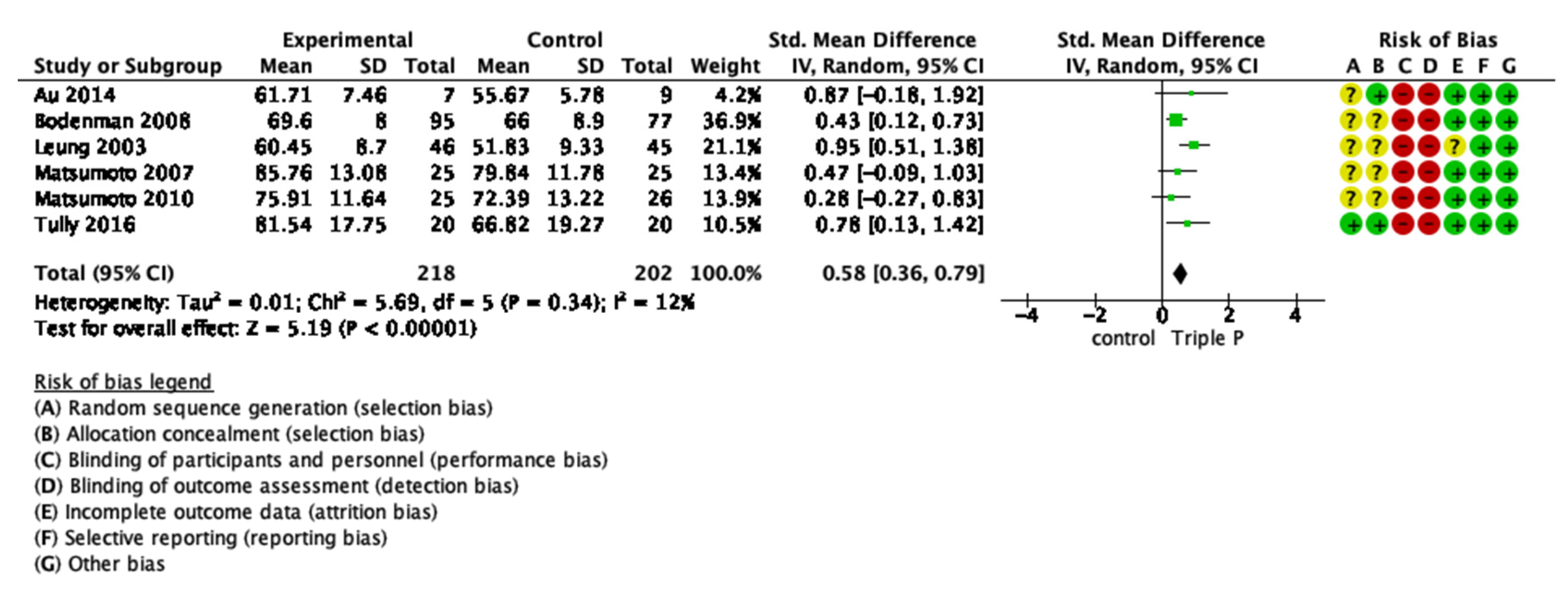
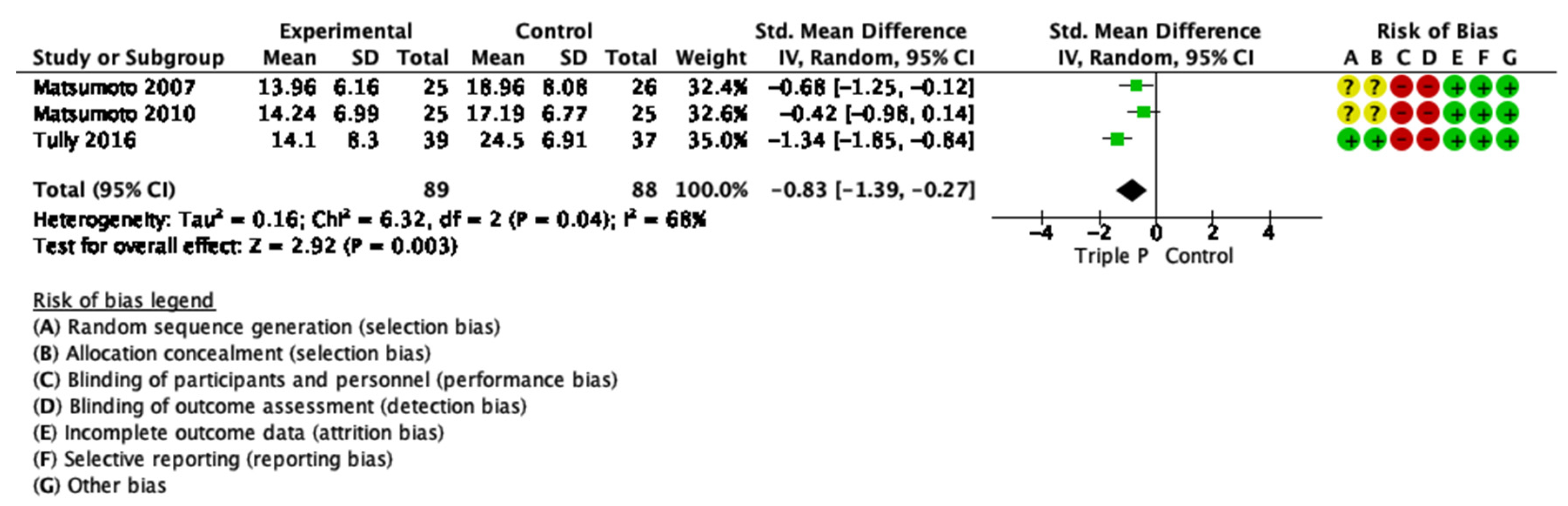
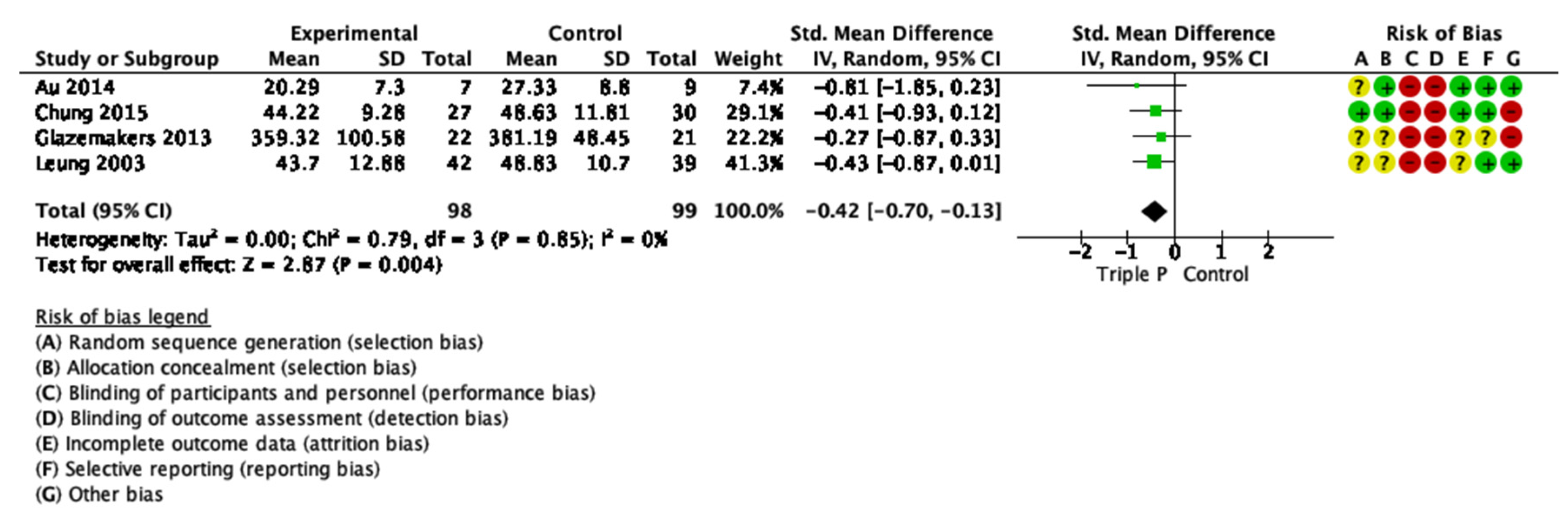
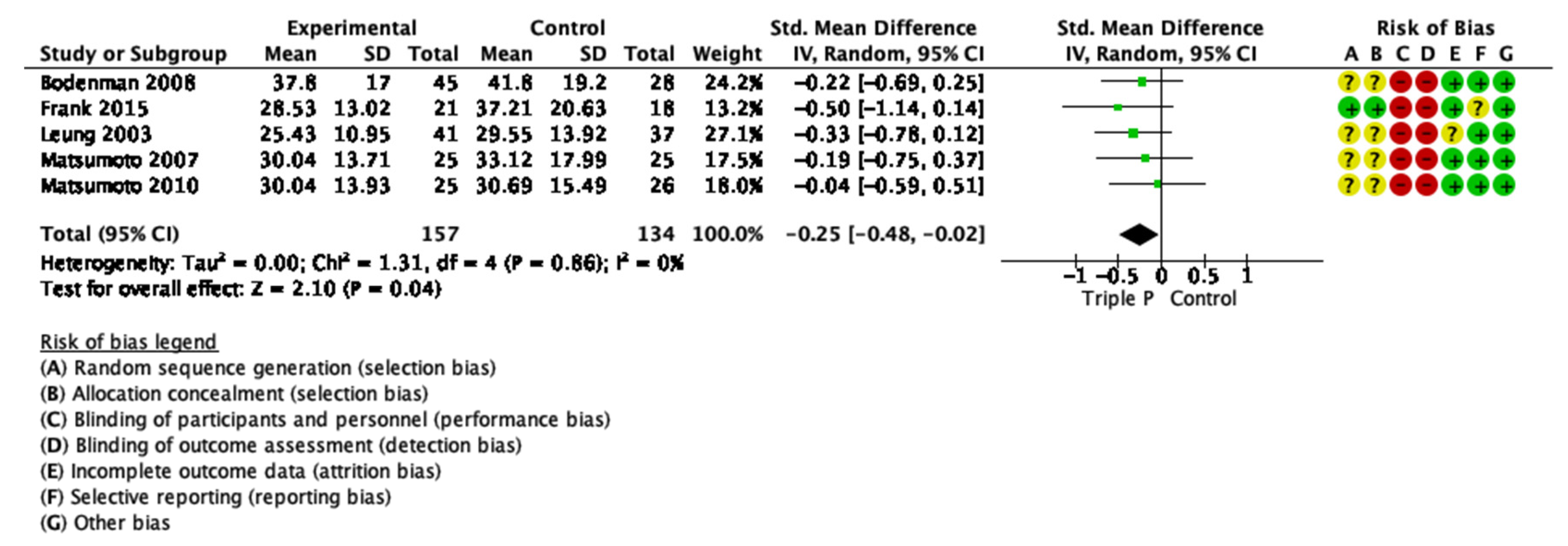
3.3. Short-Term Intervention Effects
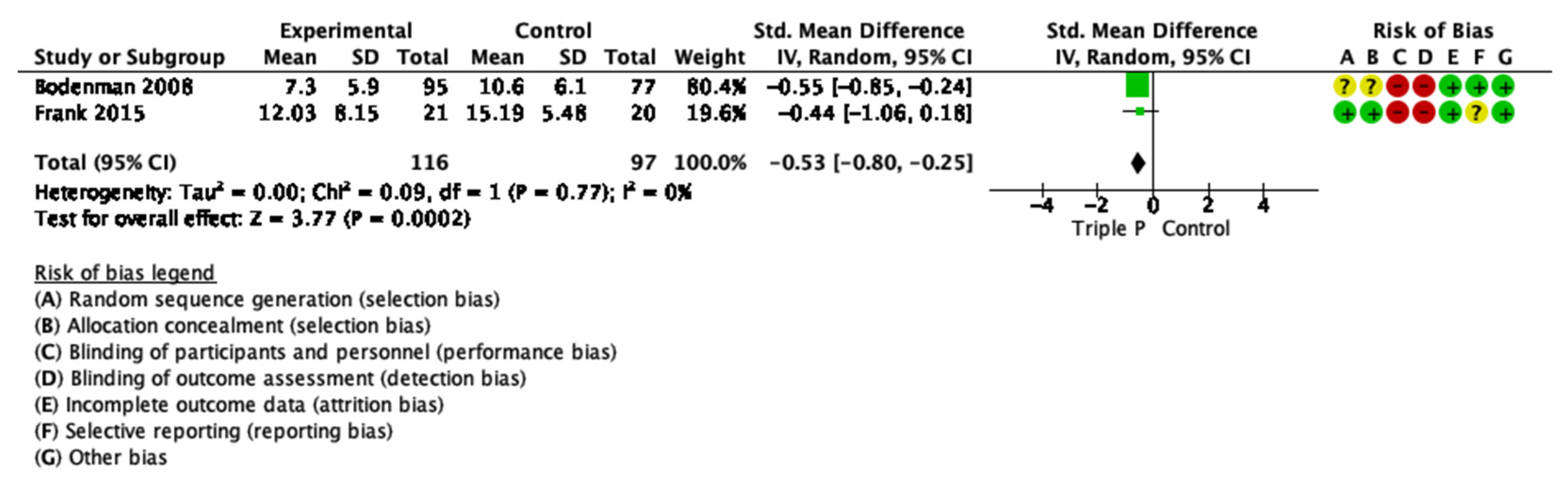
3.4. Longer-Term Intervention Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Search Term 1 | Search Term 2 | |
|---|---|---|
| Database | “Triple P positive parenting program AND level 4” | “Group Triple P AND Positive Parenting Program” |
| Triple P Evidence Base website | 79 | 0 |
| Academic Search Ultimate | 10 | 28 |
| CINAHL Plus | 5 | 18 |
| Education Source | 5 | 11 |
| ERIC | 4 | 3 |
| Fonte Académica | 0 | 0 |
| MedicLatina | 0 | 0 |
| MEDLINE | 3 | 19 |
| PsycARTICLES | 1 | 5 |
| PsycINFO | 11 | 39 |
| Psychology and Behavioral Sciences Collection | 1 | 9 |
| American Doctoral Dissertation | 0 | 3 |
| Sociology Source Ultimate | 2 | 10 |
| Criminal Justice Abstracts | 3 | 5 |
| Scopus | 15 | 103 |
| Web of Science | 18 | 106 |
| PubMed | 12 | 50 |
| ProQuest | 520 | 535 |
| Total (N=1633) | 689 | 944 |
Appendix B

Appendix C





References
- Haslam, D.M.; Burke, K. Work, Poverty, and financial stress. In Handbook of Parenting and Child Development across the Lifespan; Morawska, S., Ed.; Springer International Publishing: Brisbane, Australia, 2018; pp. 495–510. ISBN 978-3-319-94598-9. [Google Scholar]
- Sanders, M.R. Development, evaluation, and multinational dissemination of the Triple P-Positive Parenting Program. Annu. Rev. Clin. Psychol. 2012, 8, 345–379. [Google Scholar] [CrossRef] [Green Version]
- Moran, P.; Ghate, D.; van der Merwe, A. What Works in Parenting Support? A Review of the International Evidence; Report No.: E RR574; Department for Education and Skills: Nottingham, UK, 2004; pp. 1–203.
- Piquero, A.R.; Jennings, W.G.; Diamond, B.; Farrington, D.; Tremblay, R.E.; Welsh, B.C.; Gonzalez, J.M.R. A meta-analysis update on the effects of early family/parent training programs on antisocial behavior and delinquency. J. Exp. Criminol. 2016, 12, 229–248. [Google Scholar] [CrossRef]
- Sanders, M.R. Triple P-Positive Parenting Program as a public health approach to strengthening parenting. J. Fam. Psychol. 2008, 22, 506–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanders, M.; Turner, K.M.T.; Markie-Dadds, C. The development and dissemination of the Triple P—Positive Parenting Program: A multilevel, evidence-based system of parenting and family support. Prev. Sci. 2002, 3, 173–189. [Google Scholar] [CrossRef] [PubMed]
- Turner, K.M.; Richards, M.; Sanders, M. Randomised clinical trial of a group parent education programme for Australian Indigenous families. J. Paediatr. Child Health 2007, 43, 429–437. [Google Scholar] [CrossRef]
- Tellegen, C.L.; Sanders, M. Stepping Stones Triple P-Positive Parenting Program for children with disability: A systematic review and meta-analysis. Res. Dev. Disabil. 2013, 34, 1556–1571. [Google Scholar] [CrossRef]
- Sanders, M.R.; Stallman, H.M.; McHale, M. Workplace Triple P: A controlled evaluation of a parenting intervention for working parents. J. Fam. Psychol. 2011, 25, 581–590. [Google Scholar] [CrossRef]
- Stallman, H.M.; Sanders, M.R. Family Transitions Triple P. J. Divorce Remarriage 2007, 47, 133–153. [Google Scholar] [CrossRef]
- Barlow, J.; Smailagic, N.; Huband, N.; Roloff, V.; Bennett, C. Group-based parent training programmes for improving parental psychosocial health. Campbell Syst. Rev. 2012, 8, 1–197. [Google Scholar] [CrossRef] [Green Version]
- Buchanan-Pascall, S.; Gray, K.M.; Gordon, M.; Melvin, G.A. Systematic review and meta-analysis of parent group interventions for primary school children aged 4–12 years with externalizing and/or internalizing problems. Child Psychiatry Hum. Dev. 2017, 49, 244–267. [Google Scholar] [CrossRef]
- Furlong, M.; McGilloway, S.; Bywater, T.; Hutchings, J.; Smith, S.; Donnelly, M. Cochrane Review: Behavioural and cognitive-behavioural group-based parenting programmes for early-onset conduct problems in children aged 3 to 12 years (Review). Evidence-Based Child Health Cochrane Rev. J. 2013, 8, 318–692. [Google Scholar] [CrossRef] [PubMed]
- Sanders, M.R.; Kirby, J.N.; Tellegen, C.L.; Day, J. The Triple P-Positive Parenting Program: A systematic review and meta-analysis of a multi-level system of parenting support. Clin. Psychol. Rev. 2014, 34, 337–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Graaf, I.; Speetjens, P.; Smit, H.; De Wolff, M.; Tavecchio, L. Effectiveness of the Triple P Positive Parenting Program on parenting: A meta-analysis. Fam. Relat. 2008, 57, 553–566. [Google Scholar] [CrossRef]
- Thomas, R.; Zimmer-Gembeck, M.J. Behavioral outcomes of Parent-Child Interaction Therapy and Triple P—Positive Parenting Program: A review and meta-analysis. J. Abnorm. Child Psychol. 2007, 35, 475–495. [Google Scholar] [CrossRef]
- De Graaf, I.; Speetjens, P.; Smit, H.; De Wolff, M.; Tavecchio, L. Effectiveness of the Triple P Positive Parenting Program on behavioral problems in children: A meta-analysis. Behav. Modif. 2008, 32, 714–735. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, R.; Freeman, E.; Matthey, S. The impact of behavioural parent training on fathers’ parenting: A meta-analysis of the Triple P-Positive Parenting Program. Father. J. Theory Res. Pract. Men Father. 2011, 9, 291–312. [Google Scholar] [CrossRef]
- Nowak, C.; Heinrichs, N. A comprehensive meta-analysis of Triple P-Positive Parenting Program using hierarchical linear modeling: Effectiveness and moderating variables. Clin. Child Fam. Psychol. Rev. 2008, 11, 114–144. [Google Scholar] [CrossRef]
- Wilson, P.; Rush, R.; Hussey, S.; Puckering, C.; Sim, F.; Allely, C.S.; Doku, P.; McConnachie, A.; Gillberg, C. How evidence-based is an ’evidence-based parenting program’? A PRISMA systematic review and meta-analysis of Triple P. BMC Med. 2012, 10, 130. [Google Scholar] [CrossRef] [Green Version]
- Eames, C.; Daley, D.; Hutchings, J.; Whitaker, C.; Jones, K.; Hughes, J.; Bywater, T. Treatment fidelity as a predictor of behavior change in parents attending group-based parent training. Child Care Health Dev. 2009, 35, 603–612. [Google Scholar] [CrossRef] [PubMed]
- Forgatch, M.S.; Patterson, G.R.; DeGarmo, D.S. Evaluating fidelity: Predictive validity for a measure of competent adherence to the oregon model of parent management training (PMTO). Behav. Ther. 2005, 36, 3–13. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Au, A.; Lau, K.M.; Wong, A.H.; Lam, C.; Leung, C.; Lau, J.; Lee, Y.K. The efficacy of a Group Triple P (Positive Parenting Program) for chinese parents with a child diagnosed with ADHD in Hong Kong: A pilot randomised controlled study. Aust. Psychol. 2014, 49, 151–162. [Google Scholar] [CrossRef]
- Bodenmann, G.; Cina, A.; Ledermann, T.; Sanders, M. The efficacy of the Triple P-Positive Parenting Program in improving parenting and child behavior: A comparison with two other treatment conditions. Behav. Res. Ther. 2008, 46, 411–427. [Google Scholar] [CrossRef]
- Chung, S.; Leung, C.; Sanders, M. The Triple P-Positive Parenting Programme: The effectiveness of group Triple P and brief parent discussion group in school settings in Hong Kong. J. Child. Serv. 2015, 10, 339–352. [Google Scholar] [CrossRef]
- Frank, T.J.; Keown, L.J.; Sanders, M.R. Enhancing father engagement and interparental teamwork in an evidence-based parenting intervention: A randomized-controlled trial of outcomes and processes. Behav. Ther. 2015, 46, 749–763. [Google Scholar] [CrossRef] [Green Version]
- Glazemakers, I. Adding Evidence-Based Parent Training Routine Care in Child Psychiatry. A Population Health Approach to Parenting Support: Disseminating the Triple P- Positive Parenting Program in the province of Antwerp. Ph.D. Dissertation, University of Antwerp, Antwerpen, Belgium, 2013. [Google Scholar]
- Leung, C.; Sanders, M.R.; Leung, S.; Mak, R.; Lau, J. An outcome evaluation of the implementation of the Triple P-Positive Parenting Program in Hong Kong. Fam. Process 2003, 42, 531–544. [Google Scholar] [CrossRef] [Green Version]
- Leung, C.; Fan, A.; Sanders, M.R. The effectiveness of a Group Triple P with Chinese parents who have a child with developmental disabilities: A randomized controlled trial. Res. Dev. Disabil. 2013, 34, 976–984. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Sofronoff, K.; Sanders, M.R. The efficacy and acceptability of the Triple P-Positive Parenting Program with Japanese parents. Behav. Chang. 2007, 24, 205–218. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Sofronoff, K.; Sanders, M.R. Investigation of the effectiveness and social validity of the Triple P Positive Parenting Program in Japanese society. J. Fam. Psychol. 2010, 24, 87–91. [Google Scholar] [CrossRef]
- Özyurt, G.; Özlem, G.; Öztürk, Y.; Özbek, A. Is Triple P effective in childhood anxiety disorder? A randomized controlled study. Psychiatry Clin. Psychopharmacol. 2019, 29, 570–578. [Google Scholar] [CrossRef] [Green Version]
- Tully, L.A.; Hunt, C. A randomized controlled trial of a brief versus standard group parenting program for toddler aggression. Aggress. Behav. 2017, 43, 291–303. [Google Scholar] [CrossRef]
- Schulz, K.; Altman, D.; Moher, D. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomized trials. BMC Med. 2010, 8, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grant, S.; on behalf of the CONSORT-SPI Group. The CONSORT-SPI 2018 extension: A new guideline for reporting social and psychological intervention trials. Addiction 2019, 114, 4–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connor, D.; Green, S.; Higgins, J. Cochrane Handbook for Systematic Reviews of Interventions; Cochrane Book Series; John Wiley & Sons: Chichester, UK, 2008; pp. 81–94. ISBN 978-0-470-51845-8. [Google Scholar]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons: Chichester, UK, 2009. [Google Scholar] [CrossRef]
- Achenbach, T.M.; Rescorla, L.A. Manual for the ASEBA School-Age Forms & Profiles; University of Vermont, Research Center for Children, Youth, & Families: Burlington, VT, USA, 2001. [Google Scholar]
- Eyberg, S.M.; Pincus, D.B. Eyberg Child Behavior Inventory and Sutter-Eyberg Behavior Inventory-Revised: Professional Manual; Psychological Assessment Resources: Odessa, FL, USA, 1999. [Google Scholar]
- Goodman, R. The extended version of the Strengths and Difficulties Questionnaire as a guide to child psychiatric caseness and consequent burden. J. Child Psychol. Psychiatry 1999, 40, 791–799. [Google Scholar] [CrossRef]
- Arnold, D.S.; O’Leary, S.G.; Wolff, L.S.; Acker, M.M. The Parenting Scale: A measure of dysfunctional parenting in discipline situations. Psychol. Assess. 1993, 5, 137–144. [Google Scholar] [CrossRef]
- Turner, K.M.T.; Markie-Dadds, C.; Sanders, M. Practitioner’s Manual for Primary Care Triple P; Families International Publishing: Brisbane, Australia, 2000. [Google Scholar]
- Gibaud-Wallston, J.; Wandersaman, L.P. Development and utility of the Parenting Sense of Competence Scale. Presented at the Meeting of the American Psychological Association, Toronto, ON, Canada, 28 August–1 September 1978. [Google Scholar]
- Sanders, M.R.; Woolley, M.L. Parenting Tasks Checklist; PFSC: Brisbane, Australia, 2001. [Google Scholar]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Abidin, R. Parenting Stress Index; Professional Manual; Psychological Assessment Resources: Odessa, FL, USA, 1991. [Google Scholar]
- Cheung, S.K. Psychometric properties of the Chinese version of the Parental Stress Scale. Int. J. Psychol. Orient 2000, 43, 253–261. [Google Scholar]
- Stallman, H.M.; Morawska, A.; Sanders, M. Parent Problem Checklist: Tool for assessing parent conflict. Aust. Psychol. 2009, 44, 78–85. [Google Scholar] [CrossRef]
- Norton, R. Measuring Marital Quality: A critical look at the dependent variable. J. Marriage Fam. 1983, 45, 141–151. [Google Scholar] [CrossRef]
- Hedges, V.; Olkin, I. Statistical Methods for Meta-Analysis; Academic Press: New York, NY, USA, 1985; ISBN 0-12-336380-2. [Google Scholar]
- Becker, B.J. Introduction to the special section on metric in meta-analysis. Psychol. Methods 2003, 8, 403–405. [Google Scholar] [CrossRef]
- Morris, S.B.; DeShon, R.P. Combining effect size estimates in meta-analysis with repeated measures and independent-groups designs. Psychol. Methods 2002, 7, 105–125. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: New York, NY, USA, 1988; ISBN 0-12-179060-6. [Google Scholar]
- Lindsay, G.; Strand, S.; Davis, H. A comparison of the effectiveness of three parenting programmes in improving parenting skills, parent mental-well being and children’s behaviour when implemented on a large scale in community settings in 18 English local authorities: The parenting early intervention pathfinder (PEIP). BMC Public Health 2011, 11, 962. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T. Commentary: Heterogeneity in meta-analysis should be expected and appropriately quantified. Int. J. Epidemiol. 2008, 37, 1158–1160. [Google Scholar] [CrossRef] [Green Version]
- van Aar, J.; Leijten, P.; de Castro, B.O.; Overbeek, G. Sustained, fade-out or sleeper effects? A systematic review and meta-analysis of parenting interventions for disruptive child behavior. Clin. Psychol. Rev. 2017, 51, 153–163. [Google Scholar] [CrossRef]
| Outcome Categories | k | g | d 95%CI | z | p (for g) | Q2 | p (for Q2) | I2 |
|---|---|---|---|---|---|---|---|---|
| Primary outcomes | ||||||||
| Child behavior problems | 11 | −0.53 | [−0.71, −0.35] | 5.85 | 0.00 | 12.50 | 0.26 | 20 |
| Laxness subscale (PS) | 8 | −0.50 | [−0.68, −0.32] | 5.37 | 0.00 | 5.41 | 0.61 | 0 |
| Over-reactivity subscale (PS) | 7 | −0.64 | [−0.83, −0.45] | 6.53 | 0.00 | 2.17 | 0.90 | 0 |
| Parenting sense of competence | 6 | 0.58 | [0.36, −0.79] | 5.19 | 0.00 | 5.69 | 0.34 | 12 |
| Secondary outcomes | ||||||||
| Depression level (DASS) | 3 | −0.38 | [−68, −0.09] | 2.52 | 0.01 | 1.48 | 0.48 | 0 |
| Anxiety level (DASS) | 3 | −0.30 | [−0.59, 0.00] | 1.97 | 0.05 | 0.25 | 0.88 | 0 |
| Stress level (DASS) | 3 | −0.43 | [−0.73, −0.14] | 2.85 | 0.00 | 1.38 | 0.50 | 0 |
| Parental stress level | 4 | −0.42 | [−0.70, −0.13] | 2.87 | 0.00 | 0.79 | 0.85 | 0 |
| Parental conflict | 5 | −0.25 | [−0.48, −0.02] | 2.10 | 0.04 | 1.31 | 0.86 | 0 |
| Relationship quality | 5 | 0.25 | [0.01, 0.49] | 2.01 | 0.04 | 2.04 | 0.73 | 0 |
| Outcome Categories | k | g | d 95%CI | z | p (for g) | Q | p (for Q) | I2 |
|---|---|---|---|---|---|---|---|---|
| Primary outcomes | ||||||||
| Child behavior problems | 2 | −0.53 | [−0.91, −0.14] | 2.69 | 0.00 | 1.87 | 0.17 | 46 |
| Dysfunctional parenting practices | 2 | −0.46 | [−0.73, −0.19] | 3.37 | 0.00 | 0.99 | 0.32 | 0 |
| Secondary outcomes | ||||||||
| Parental conflict | 2 | −0.08 | [−0.34, 0.19] | 0.58 | 0.56 | 0.66 | 0.42 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nogueira, S.; Canário, A.C.; Abreu-Lima, I.; Teixeira, P.; Cruz, O. Group Triple P Intervention Effects on Children and Parents: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 2113. https://doi.org/10.3390/ijerph19042113
Nogueira S, Canário AC, Abreu-Lima I, Teixeira P, Cruz O. Group Triple P Intervention Effects on Children and Parents: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(4):2113. https://doi.org/10.3390/ijerph19042113
Chicago/Turabian StyleNogueira, Sandra, Ana Catarina Canário, Isabel Abreu-Lima, Pedro Teixeira, and Orlanda Cruz. 2022. "Group Triple P Intervention Effects on Children and Parents: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 4: 2113. https://doi.org/10.3390/ijerph19042113
APA StyleNogueira, S., Canário, A. C., Abreu-Lima, I., Teixeira, P., & Cruz, O. (2022). Group Triple P Intervention Effects on Children and Parents: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 19(4), 2113. https://doi.org/10.3390/ijerph19042113