
Interventions to Improve Child Physical Activity in the Early Childhood Education and Care Setting: An Umbrella Review

 , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.1.1. Population
2.1.2. Intervention
2.1.3. Comparison
2.1.4. Outcomes
2.2. Information Sources and Search Strategy
2.3. Screening
2.4. Data Collection Process
- Review information: author, year of publication, objectives of the review, inclusion/exclusion criteria, method of analysis (e.g., meta-analysis, narrative synthesis), search details (e.g., date of search, limiters), sources searched.
- Participant information as summarised by the review: (where relevant to the outcomes reported within the review) age range, gender, socioeconomic status, ethnicity, total number of participants.
- Primary study information: setting/context, range (years) of the included studies, number of studies included, types of studies included, country of origin of the included studies.
- Intervention information: description of interventions.
- Outcome information: child physical activity outcomes assessed.
- Appraisal instrument and rating: appraisal instruments used, appraisal rating.
- Results: significance/direction, heterogeneity, authors’ conclusions.
- Sources of funding and conflicts of interest: sources of funding for review.
- Comments: other relevant information not extracted elsewhere.
2.5. Quality Assessment
2.6. Data Synthesis
3. Results
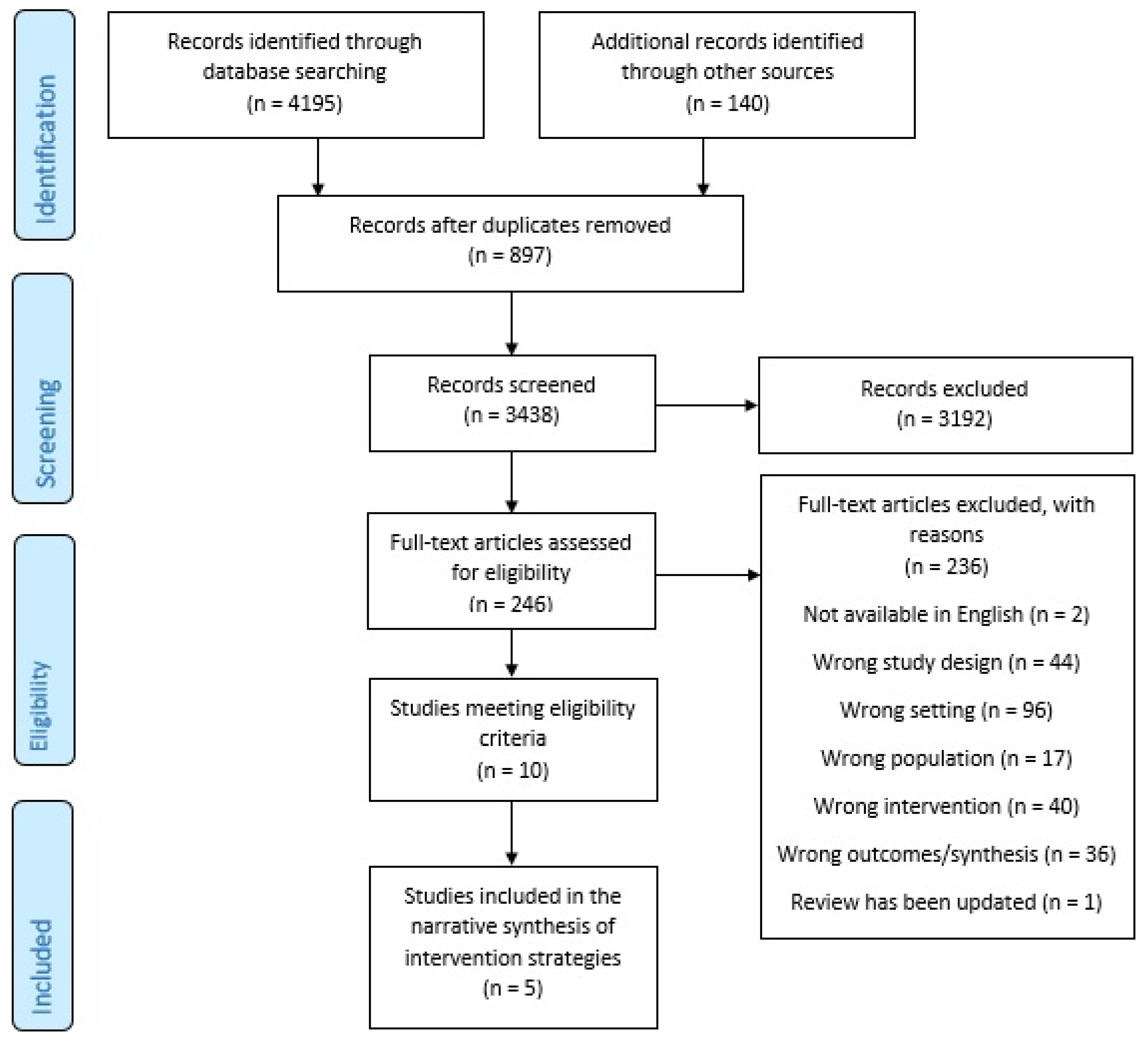
3.1. Review Selection
3.2. Review Characteristics
3.3. Quality of the Included Reviews
3.4. Effectiveness of Physical Activity Interventions in ECEC Overall
3.5. Effectiveness of Intervention Strategies Mapped to the Recommended Practices
3.6. Additional Strategies
4. Discussion
4.1. Main Findings
4.2. Quality of the Included Reviews
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| # | Medline Search: Inception—November 2020 |
|---|---|
| 1 | exp Exercise/ |
| 2 | physical inactivity.mp. |
| 3 | physical activit*.mp. |
| 4 | Motor Activity/ |
| 5 | (physical education and training).mp. |
| 6 | “Physical Education and Training”/ |
| 7 | sedentary.mp. |
| 8 | sport*.mp. |
| 9 | exp Life Style/ |
| 10 | Physical Fitness/ |
| 11 | exp Leisure Activities/ |
| 12 | Dancing/ |
| 13 | (dance* or dancing).mp. |
| 14 | (exercise* adj2 aerobic*).mp. |
| 15 | ((life style or lifestyle) adj5 activ*).mp. |
| 16 | 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 |
| 17 | Child, Preschool/ |
| 18 | Child Day Care Centers/ |
| 19 | (childcare* or child care*).mp. |
| 20 | (daycare* or day care*).mp. |
| 21 | early child*.mp. |
| 22 | Kinder*.mp. |
| 23 | (nursery or nurseries).mp. |
| 24 | (pre-school* or preschool*).mp. |
| 25 | 17 or 18 or 19 or 21 or 22 or 23 or 24 |
| 26 | 16 and 25 |
| 27 | MEDLINE.tw. |
| 28 | systematic review.tw. |
| 29 | meta-analysis.pt. |
| 30 | intervention$.ti. |
| 31 | or/27–30 |
| 32 | 26 and 31 |
Appendix B
- Provide opportunities for children to be physically active (more is better).
- 1.1.
- Ensure physical activity is incorporated into daily routines and formal childcare curriculum.
- 1.2.
- Include at least 180 min of physical activity of any intensity, spread throughout the day.
- 1.3.
- For children 3–4 years, include at least 60 min of moderate-to-vigorous physical activity during the day.
- 1.4.
- Include opportunities for adult-led, structured physical activity.
- 1.5.
- Include opportunities for unstructured physical activity, free play (playtime).
- 1.6.
- Provide daily opportunities for activity through outdoor playtime (should be supervised).
- 1.7.
- Provide opportunities for children to develop and practice gross motor and movement skills.
- 1.8.
- Include culturally appropriate physical activities.
- Adopt standards for physical activity and physical education programs.
- 2.1.
- Engage staff and parent support for physical activity standards.
- 2.2.
- Seek consultation from experts annually on the PA programs delivered in the childcare.
- 2.3.
- Provide parent education at least 2 times a year (to reduce screen time).
- 2.4.
- Develop a written policy promoting physical activity and the removal of barriers to physical activity participation (including limiting screen time).
- Offer educator training to provide safe and developmentally appropriate physical activity.
- 3.1.
- Staff should be trained to provide guidance to parents to encourage physical activity.
- 3.2.
- Staff should be trained to provide guidance to parents in appropriate sleep duration.
- 3.3.
- Staff should be trained in encouraging child physical activity and decreasing sedentary behavior.
- 3.4.
- Offer staff annual training opportunities in physical activity programs and practices.
- Educators to promote the benefits of physical activity with children.
- 4.1.
- Educators should model physical activity by participating in activities.
- 4.2.
- Engage children in physical activity they enjoy, including games and sport (age appropriate, fun and offer variety).
- 4.3.
- Expressive play is encouraged e.g., music, dancing and make believe.
- 4.4.
- Educators embed physical activity into educational activities.
- 4.5.
- Avoid punishing children for being physical active.
- 4.6.
- Avoid withholding physical activity as a punishment.
- 4.7.
- Elimination games should be avoided as well as competitive activities and games.
- 4.8.
- Engage equal participation from boys and girls in physical activity.
- 4.9.
- Celebrate special occasions with physical activity (games, dancing and extra playground time).
- Limit the time children spend sitting (less is best).
- 5.1.
- Children should not be sitting for extended periods (or be restrained) for more than 30–60 min at a time.
- 5.2.
- When sedentary, children should be engaged in educational and creative pursuits, and be engaged socially.
- 5.3.
- Engage children that tend to be sedentary in active play.
- Limit the use of screen time (less is best).
- 6.1.
- No screen time is recommended for children <2 years.
- 6.2.
- No more than 1 h of screen time/week is recommended for children aged 2 or above.
- 6.3.
- Screens should not be used/available during mealtimes or nap times.
- 6.4.
- Limit the use of screen time for educational activities or active movement programs.
- 6.5.
- Parent permission should be requested for children to participate in any screen based activity.
- 6.6.
- Screen time should be supervised by an adult (to help children apply what they are learning).
- 6.7.
- When offered, screen/digital media should be free from advertising, violence or should that tempt children to overuse.
- 6.8.
- Work with parents to limit overall screen time.
- Support healthy sleeping habits.
- 7.1.
- Include a nap within the daily routine, with regular sleep and wake-up times.
- 7.2.
- Provide an environment that provides restful sleep: remove screen media from sleeping/napping areas and low noise.
- 7.3.
- Maintain a calm nap-time routine.
- Create a physical environment that promotes physical activity.
- 8.1.
- Provide play equipment that encourages physical activity.
- 8.2.
- Provide simple play equipment to encourage creative play and exploration (e.g., cardboard boxes) and portable play equipment that encourages indoor and outdoor play.
- 8.3.
- Provide adequate space for children to be physically active.
- 8.4.
- Ensure the outdoor area offers variety in terms of secure equipment in shade, open grass and varying surfaces.
- 8.5.
- Ensure that the educator to child ratio is fairly low (i.e., less than 10 children to one educator).
References
- World Health Organization. Physical Activity Fact Sheet: World Health Organization. 2021. Available online: https://www.who.int/publications/i/item/WHO-HEP-HPR-RUN-2021.2 (accessed on 12 October 2021).
- Katzmarzyk, P.T.; Friedenreich, C.; Shiroma, E.J.; Lee, I.M. Physical inactivity and non-communicable disease burden in low-income, middle-income and high-income countries. Br. J. Sports Med. 2022, 56, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Timmons, B.W.; Leblanc, A.G.; Carson, V.; Connor Gorber, S.; Dillman, C.; Janssen, I.; Kho, M.; Spence, J.C.; Stearns, J.; Tremblay, M.S. Systematic review of physical activity and health in the early years (aged 0–4 years). Appl. Physiol. Nutr. Metab. 2012, 37, 773–792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hidayat, K.; Zhou, H.J.; Shi, B.M. Influence of physical activity at a young age and lifetime physical activity on the risks of 3 obesity-related cancers: Systematic review and meta-analysis of observational studies. Nutr. Rev. 2020, 78, 1–18. [Google Scholar] [CrossRef]
- Telama, R.; Yang, X.; Leskinen, E.; Kankaanpää, A.; Hirvensalo, M.; Tammelin, T.; Viikari, J.S.A.; Raitakari, O.T. Tracking of physical activity from early childhood through youth into adulthood. Med. Sci. Sports Exerc. 2014, 46, 955–962. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Standards for Healthy Eating, Physical Activity, Sedentary Behaviour and Sleep in Early Childhood Education and Care Settings: A Toolkit; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Pate, R.R.; O’Neill, J.R.; Brown, W.H.; Pfeiffer, K.A.; Dowda, M.; Addy, C.L. Prevalence of compliance with a new physical activity guideline for preschool-age children. Child Obes. 2015, 11, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Scholes, S. Health Survey for England 2015 Physical Activity in Children; Health and Social Care Information Centre, NHS Digital: Leeds, UK, 2016. [Google Scholar]
- Australian Institute of Health and Welfare. Physical Activity across the Life Stages; Australian Government, Ed.; AIHW: Canberra, Australia, 2018.
- PF3.2: Enrolment in Childcare and Pre-School. OECD. 2021. Available online: https://www.oecd.org/els/soc/PF3_2_Enrolment_childcare_preschool.pdf (accessed on 30 July 2021).
- World Health Organization. Population-Based Approaches to Childhood Obesity Prevention; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Jackson, J.K.; Jones, J.; Nguyen, H.; Davies, I.; Lum, M.; Grady, A.; Yoong, S. Obesity prevention within the early childhood education and care setting: A systematic review of dietary behavior and physical activity policies and guidelines in high income countries. Int. J. Environ. Res. Public Health 2021, 18, 838. [Google Scholar] [CrossRef] [PubMed]
- Bastian, H.; Glasziou, P.; Chalmers, I. Seventy-five trials and eleven systematic reviews a day: How will we ever keep up? PLoS Med. 2010, 7, e1000326. [Google Scholar] [CrossRef] [PubMed]
- Blackwood, D. Taking it to the next level: Reviews of sytematic reviews. HLA News 2016, 1, 13–15. [Google Scholar] [CrossRef]
- Aromataris, E.; Fernandez, R.S.; Godfrey, C.; Holly, C.; Khalil, H.; Tungpunkom, P. Methodology for JBI Umbrella Reviews. 2014. Available online: https://ro.uow.edu.au/cgi/viewcontent.cgi?article=4367&context=smhpapers (accessed on 14 May 2020).
- Pollock, M.; Fernandes, R.M.; Becker, L.A.; Pieper, D.; Hartling, L. Chapter V: Overviews of Reviews. In Cochrane Handbook for Systematic Reviews of Interventions, 62nd ed.; The Cochrane Collaboration: London, UK, 2021. [Google Scholar]
- Stacey, F.G.; Finch, M.; Wolfenden, L.; Grady, A.; Jessop, K.; Wedesweiler, T.; Bartlem, K.; Jones, J.; Sutherland, R.; Vandevijvere, S.; et al. Evidence of the potential effectiveness of centre-based childcare policies and practices on child diet and physical activity: Consolidating evidence from systematic reviews of intervention trials and observational studies. Curr. Nutr. Rep. 2017, 6, 228–246. [Google Scholar] [CrossRef]
- Wolfenden, L.; Barnes, C.; Lane, C.; McCrabb, S.; Brown, H.M.; Gerritsen, S.; Barquera, S.; Véjar, L.S.; Munguía, A.; Yoong, S.L. Consolidating evidence on the effectiveness of interventions promoting fruit and vegetable consumption: An umbrella review. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 11. [Google Scholar] [CrossRef]
- Veritas Health Innovation. Covidence Systematic Review Software; Veritas Health Innovation: Melbourne, Australia, 2021. [Google Scholar]
- Aromataris, E.; Munn, Z. (Eds.) JBI Manual for Evidence Synthesis: JBI. 2020. Available online: https://synthesismanual.jbi.global (accessed on 14 May 2020). [CrossRef]
- Schultz, T.J.; Roupas, P.; Wiechula, R.; Krause, D.; Gravier, S.; Tuckett, A.; Hines, S.; Kitson, A. Nutritional interventions for optimizing healthy body composition in older adults in the community: An umbrella review of systematic reviews. JBI Database Syst. Rev. Implement Rep. 2016, 14, 257–308. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Broekhuizen, K.; Scholten, A.M.; de Vries, S.I. The value of (pre)school playgrounds for children’s physical activity level: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finch, M.; Jones, J.; Yoong, S.; Wiggers, J.; Wolfenden, L. Effectiveness of centre-based childcare interventions in increasing child physical activity: A systematic review and meta-analysis for policymakers and practitioners. Obes. Rev. 2016, 17, 412–428. [Google Scholar] [CrossRef] [PubMed]
- Hnatiuk, J.A.; Brown, H.E.; Downing, K.L.; Hinkley, T.; Salmon, J.; Hesketh, K.D. Interventions to increase physical activity in children 0–5 years old: A systematic review, meta-analysis and realist synthesis. Obes. Rev. 2019, 20, 75–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peden, M.E.; Okely, A.D.; Eady, M.J.; Jones, R.A. What is the impact of professional learning on physical activity interventions among preschool children? A systematic review. Clin. Obes. 2018, 8, 285–299. [Google Scholar] [CrossRef] [Green Version]
- Van Capelle, A.; Broderick, C.R.; van Doorn, N.; Ward, R.E.; Parmenter, B.J. Interventions to improve fundamental motor skills in pre-school aged children: A systematic review and meta-analysis. J. Sci. Med. Sport 2017, 20, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Mehtälä, M.A.K.; Sääkslahti, A.K.; Inkinen, M.E.; Poskiparta, M.E.H. A socio-ecological approach to physical activity interventions in childcare: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 22. [Google Scholar] [CrossRef] [Green Version]
- Ward, S.; Bélanger, M.; Donovan, D.; Carrier, N. Systematic review of the relationship between childcare educators’ practices and preschoolers’ physical activity and eating behaviours. Obes. Rev. 2015, 16, 1055–1070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolfenden, L.; Barnes, C.; Jones, J.; Finch, M.; Wyse, R.J.; Kingsland, M.; Tzelepis, F.; Grady, A.; Hodder, R.K.; Booth, D.; et al. Strategies to improve the implementation of healthy eating, physical activity and obesity prevention policies, practices or programmes within childcare services. Cochrane Database Syst. Rev. 2020, 2, CD011779. [Google Scholar] [CrossRef] [PubMed]
- Engel, A.C.; Broderick, C.R.; van Doorn, N.; Hardy, L.L.; Parmenter, B.J. Exploring the relationship between fundamental motor skill interventions and physical activity levels in children: A systematic review and meta-analysis. Sports Med. 2018, 48, 1845–1857. [Google Scholar] [CrossRef] [PubMed]
- Ling, J.; Robbins, L.B.; Wen, F.; Peng, W. Interventions to increase physical activity in children aged 2–5 years: A systematic review. Pediatr. Exerc. Sci. 2015, 27, 314–333. [Google Scholar] [CrossRef] [PubMed]
- Hesketh, K.R.; Lakshman, R.; van Sluijs, E.M.F. Barriers and facilitators to young children’s physical activity and sedentary behaviour: A systematic review and synthesis of qualitative literature. Obes. Rev. 2017, 18, 987–1017. [Google Scholar] [CrossRef] [PubMed]
- Saunders, R.P.; Schenkelberg, M.A.; Moyer, C.; Howie, E.K.; Brown, W.H.; Pate, R.R. The translation of an evidence-based preschool physical activity intervention from in-person to online delivery of professional development to preschool teachers. Transl. Behav. Med. 2019, 9, 1186–1196. [Google Scholar] [CrossRef] [PubMed]
- Tonge, K.L.; Jones, R.A.; Okely, A.D. Correlates of children’s objectively measured physical activity and sedentary behavior in early childhood education and care services: A systematic review. Prev. Med. 2016, 89, 129–139. [Google Scholar] [CrossRef] [Green Version]
- Truelove, S.; Bruijns, B.A.; Vanderloo, L.M.; O’Brien, K.T.; Johnson, A.M.; Tucker, P. Physical activity and sedentary time during childcare outdoor play sessions: A systematic review and meta-analysis. Prev. Med. 2018, 108, 74–85. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, A.; Greaney, M.; Wallington, S.; Mesa, T.; Salas, C. A review of early influences on physical activity and sedentary behaviors of preschool-age children in high-income countries. J. Spec. Pediatr. Nurs. 2017, 22, e12182. [Google Scholar] [CrossRef] [Green Version]
- Trost, S.G.; Loprinzi, P.D. Parental influences on physical activity behavior in children and adolescents: A brief review. Am. J. Lifestyle Med. 2011, 5, 171–181. [Google Scholar] [CrossRef]
- Yao, C.A.; Rhodes, R.E. Parental correlates in child and adolescent physical activity: A meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 1–38. [Google Scholar] [CrossRef] [Green Version]
- Department of Health. For Children and Young People (5 to 17 Years); Department of Health, Australian Government: Canberra, Australia, 2021.
- Willumsen, J.; Bull, F. Development of WHO guidelines on physical activity, sedentary behavior, and sleep for children less than 5 years of age. J. Phys. Act. Health 2020, 17, 96–100. [Google Scholar] [CrossRef] [Green Version]
- McKeown, S.; Mir, Z.M. Considerations for conducting systematic reviews: Evaluating the performance of different methods for de-duplicating references. Syst. Rev. 2021, 10, 38. [Google Scholar] [CrossRef] [PubMed]
- Andersen, E.; Øvreås, S.; Jørgensen, K.A.; Borch-Jenssen, J.; Moser, T. Children’s physical activity level and sedentary behaviour in Norwegian early childhood education and care: Effects of a staff-led cluster-randomised controlled trial. BMC Public Health 2020, 20, 1651. [Google Scholar] [CrossRef] [PubMed]
- Razak, L.A.; Yoong, S.L.; Wiggers, J.; Morgan, P.J.; Jones, J.; Finch, M.; Sutherland, R.; Lecathelnais, C.; Gillham, K.; Clinton-McHarg, T.; et al. Impact of scheduling multiple outdoor free-play periods in childcare on child moderate-to-vigorous physical activity: A cluster randomised trial. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okely, A.D.; Stanley, R.M.; Jones, R.A.; Cliff, D.P.; Trost, S.G.; Berthelsen, D.; Salmon, J.; Batterham, M.; Eckermann, S.; Reilly, J.J.; et al. ‘Jump start’ childcare-based intervention to promote physical activity in pre-schoolers: Six-month findings from a cluster randomised trial. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 6. [Google Scholar] [CrossRef] [Green Version]
| Author, Year | Eligibility (Population, Setting, Design) | Recommended Broad Practices [12] Addressed | Intervention (Duration) Comparator | Number of Relevant Studies; Year of Publication Range; Countries; Total Number of Studies Included in Each Review | Relevant Outcomes; Method of Synthesis |
|---|---|---|---|---|---|
| Broekhuizen, 2014 [23] | Population: Aged 2–18 years Setting: (Pre)schools Design: Noncontrolled trials and RCTs | Create a physical environment that promotes physical activity | Intervention: Interventions on (pre)school playgrounds, defined as spaces located on (pre)school properties that were specifically designed for outdoor play and sports activities for children (range: from 18 weeks to 12 months) Comparator: NR | 5 relevant studies; 2006 to 2012; US (3), Belgium (2) Total included: 33 studies | Physical activity levels; Narrative |
| Engel, 2018 [31] | Population: Aged 3–5 years and/or 5–12 years Setting: NR Design: Controlled trials | Provide opportunities for children to be physically active (the more the better) | Intervention: Fundamental movement skill interventions in preschool (range: from 10 weeks to 18 months) Comparator: Any control | 10 relevant studies; 2006 to 2016; NR Total included: 14 studies | Physical activity, MVPA, sedentary behaviour; Meta-analysis |
| Finch, 2016 [24] | Population: Aged < 6 years, with no diagnosed diseases or health problems Setting: Centre-based childcare Design: RCTs | Provide opportunities for children to be physically active (the more the better); Create a physical environment that promotes physical activity | Intervention: Interventions to improve physical activity among children aged 0–6 years attending childcare (range: from 2 days to 12 months) Comparator: Any control | 17 relevant studies; 2006 to 2014; US (7), Australia (2), Switzerland (2), Belgium (2), Germany (1), Israel (1), England (1), Scotland (1) Total included: 17 studies | Physical activity levels;Meta-analysis |
| Hnatuik, 2019 [25] | Population: Aged 0–5.9 years Setting: NR Design: RCTs and controlled trials | Educators to promote the benefits of physical activity with children | Intervention: Interventions to increase physical activity in 0–5-year-olds (NR) Comparator: Any control | 27 relevant studies; 2006 to 2016; NR for relevant studies Total included: 34 studies | MVPA; Meta-analysis and narrative |
| Ling, 2015 [32] | Population: Preschool age (2–5 years); Setting: Any setting Design: Included a control or comparison group | NA | Intervention: Interventions to increase physical activity or decrease sedentary activity in any setting (range: from 6 weeks to 12 months) Comparator: Any control or comparison | 21 relevant studies; 2003 to 2014; US (10), Switzerland (2), Australia (2), United Kingdom (2), Belgium (2), Germany (1), Scotland (1), Israel (1) Total included: 23 studies | Physical activity levels; Narrative |
| Mehtala, 2014 [28] | Population: Aged 2–6 years with no diagnosed diseases or health problems Setting: Centre-based childcare Design: RCTs, quasi-experimental, before/after, pilot and feasibility study designs | Provide opportunities for children to be physically active (the more the better); Offer educator training to provide safe and developmentally appropriate physical activity | Intervention: Childcare-aged children’s physical activity promotion programs in a childcare setting (range: from 2 days to 12 months) Comparator: NR | 23 relevant studies; 1993 to 2013; US (17), Belgium (2), Switzerland (1), Scotland (1), Australia (1), Israel (1) Total included: 23 studies | Physical activity levels; Narrative |
| Peden, 2018 [26] | Population: Aged 0–5 years Setting: Licenced public or commercial early childhood and care settings Design: RCTs or pilot studies | Offer educator training to provide safe and developmentally appropriate physical activity | Intervention: Childcare-based physical activity interventions, incorporated professional learning and reported objectively measured physical activity (range: from 8 weeks to 2 years) Comparator: Any control | 11 relevant studies; 2008 to 2016; US (7), Australia (2), United Kingdom (1), Switzerland (1) Total included: 11 studies | Physical activity levels; Narrative |
| Van Capelle, 2017 [27] | Population: Aged 3–5 years Setting: Preschool Design: RCTs and controlled trials | Provide opportunities for children to be physically active (the more the better) | Intervention: Fundamental movement skills intervention (>4 weeks) Comparator: Usual playground activity | 4 relevant studies; 1996 to 2016; NR Total: 20 studies | Counts per minute, % time in MVPA, sedentary duration; Meta-analysis |
| Ward, 2015 [29] | Population: Preschoolers Setting: Formal childcare Design: All types | Educators to promote the benefits of physical activity to children | Intervention: Childcare educators’ practices or behaviours affect children’s physical activity or eating behaviours (NR) Comparator: NR | 6 relevant studies; 2008 to 2015; US (6) Total included: 15 studies | Physical activity levels; Narrative |
| Wolfenden, 2020 [30] | Population: Centre-based childcare services (and staff thereof) such as preschools, nurseries, long-day care services and kindergartens that cater for children prior to compulsory schooling. Setting: Centre-based childcare services Design: Any study (randomised, including cluster-randomised, or nonrandomised) with a parallel control group | NA | Intervention: Any strategy with the primary intent of improving the implementation of policies, practices or programmes in centre-based childcare services to promote healthy eating, physical activity or prevent unhealthy weight gain (NR) Comparator: Any parallel control | 5 relevant studies; 2014 to 2018; US (3), Australia (2) Total included: 21 studies | Physical activity levels; Narrative |
| Criteria | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Included Review | C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | C9 | C10 | C11 | Criteria Met (%) |
| Broekhuizen, 2014 | Y | Y | Y | Y | Y | Y | Y | Y | N | N | Y | 82% |
| Engel, 2018 | N | Y | Y | Y | Y | Y | N | Y | N | Y | Y | 73% |
| Finch, 2016 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 100% |
| Hnatuik, 2019 | Y | Y | Y | Y | Y | Y | N | Y | N | Y | Y | 82% |
| Ling, 2015 | N | Y | Y | Y | Y | Y | N | Y | N | Y | Y | 73% |
| Mehtala, 2014 | N | Y | Y | Y | Y | Y | U | Y | N | Y | Y | 73% |
| Peden, 2018 | Y | Y | Y | Y | Y | Y | N | U | N | Y | Y | 73% |
| Van Capelle, 2017 | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 91% |
| Ward, 2015 | Y | Y | Y | Y | Y | N | U | Y | N | Y | Y | 73% |
| Wolfenden, 2020 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 100% |
| Recommended Practics | 1. PROVIDE OPPORTUNITIES FOR CHILDREN TO BE PHYSICALLY ACTIVE (MORE IS BETTER) | 2. DEVELOP AND ADOPT POLICIES FOR PHYSICAL ACTIVITY AND PHYSICAL ACTIVITY EDUCATION PROGRAMS | 3. OFFER EDUCATOR TRAINING TO PROVIDE SAFE AND DEVELOPMENTALLY APPROPRIATE PHYSICAL ACTIVITY | 4. EDUCATORS TO PROMOTE THE BENEFITS OF PHYSICAL ACTIVITY WITH CHILDREN [25] | 5. LIMIT THE TIME CHILDREN SPEND SITTING (LESS IS BEST) | 6. LIMIT THE USE OF SCREEN TIME (LESS IS BEST) | 7. SUPPORT HEALTHY SLEEPING HABITS | 8. CREATE A PHYSICAL ENVIRONMENT THAT PROMOTES PHYSICAL ACTIVITY [24] |
|---|---|---|---|---|---|---|---|---|
| Recommended sub-practices | 1.1 Ensure physical activity is incorporated into daily routines and formal childcare curriculum | 2.1 Engage staff and parent support for physical activity standards | 3.1 Staff should be trained to counsel parents about their child’s physical activity | 4.1. Educators should model physical activity by participating in activities | 5.1 Children should not be sitting for extended periods (or be restrained for more than 1 h) | 6.1 No screen time is recommended for children <2 years | 7.1 Include a nap within the daily routine, with regular sleep and wake-up times | 8.1 Provide play equipment that encourages physical activity [23] |
| 1.2 Include at least 180 min of physical activity of any intensity, spread throughout the day | 2.2 Seek consultation from experts annually on the physical activity programs delivered in the childcare | 3.2 Staff should be trained in counselling parents in appropriate sleep duration | 4.2 Engage children in physical activity they enjoy, including games and sport (age appropriate, fun and offer variety) | 5.2 When sedentary, children should be engaged in educational and creative pursuits, and be engaged socially. | 6.2 No more than 1 h of screen time/week is recommended for children >2 years | 7.2 Provide an environment that provides restful sleep: remove screen media from sleeping/napping areas and low noise | 8.2 Provide simple play equipment to encourage creative play and exploration (e.g., cardboard boxes) and portable play equipment that encourages indoor and outdoor play | |
| 1.3 For children 3–4 years, include at least 60 min of moderate-to-vigorous physical activity during the day | 2.3 Provide parent education at least 2 times a year (to reduce screen time) | 3.3 Staff should be trained in encouraging child physical activity and decreasing sedentary behaviour [26] | 4.3 Expressive play is encouraged e.g., music, dancing and make believe | 5.3 Engage children that tend to be sedentary in active play | 6.3 Screens should not be used/available during mealtimes or nap times | 7.3 Maintain a calm nap-time routine | 8.3 Provide adequate space for children to be physically active | |
| 1.4 Include opportunities for adult-led, structured physical activity [24] | 2.4 Develop a written policy promoting physical activity and the removal of barriers to physical activity participation (including limiting screen time) | 3.4 Offer staff annual training opportunities in physical activity programs and practices | 4.4 Educators embed physical activity into educational activities | 6.4 Limit the use of screen time for educational activities or active movement programs | 8.4 Ensure the outdoor area offers variety in terms of secure equipment in shade, open grass and varying surfaces | |||
| 1.5 Include opportunities for unstructured physical activity, free play (play-time) | 4.5 Avoid punishing children for being physical active | 6.5 Parent permission should be requested for children to participate in any screen based activity | 8.5 Ensure that the educator to child ratio is fairly low (i.e., less than 10 children to one educator) | |||||
| 1.6 Provide daily opportunities for activity through outdoor playtime (should be supervised) | 4.6 Avoid withholding physical activity as a punishment | 6.6 Screen time should be supervised by an adult (to help children apply what they are learning) | ||||||
| 1.7 Provide opportunities for children to develop and practice gross motor and movement skills [27] | 4.7 Elimination games should be avoided as well as competitive activates and games | 6.7 When offered, screen/digital media should be free from advertising, violence or should that tempt children to overuse | ||||||
| 1.8 Include culturally appropriate physical activities | 4.8 Engage equal participation from boys and girls in physical activity | 6.8 Work with parents to limit overall screen time | ||||||
| 4.9 Celebrate special occasions with physical activity (games, dancing and extra playground time). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lum, M.; Wolfenden, L.; Jones, J.; Grady, A.; Christian, H.; Reilly, K.; Yoong, S.L. Interventions to Improve Child Physical Activity in the Early Childhood Education and Care Setting: An Umbrella Review. Int. J. Environ. Res. Public Health 2022, 19, 1963. https://doi.org/10.3390/ijerph19041963
Lum M, Wolfenden L, Jones J, Grady A, Christian H, Reilly K, Yoong SL. Interventions to Improve Child Physical Activity in the Early Childhood Education and Care Setting: An Umbrella Review. International Journal of Environmental Research and Public Health. 2022; 19(4):1963. https://doi.org/10.3390/ijerph19041963
Chicago/Turabian StyleLum, Melanie, Luke Wolfenden, Jannah Jones, Alice Grady, Hayley Christian, Kathryn Reilly, and Sze Lin Yoong. 2022. "Interventions to Improve Child Physical Activity in the Early Childhood Education and Care Setting: An Umbrella Review" International Journal of Environmental Research and Public Health 19, no. 4: 1963. https://doi.org/10.3390/ijerph19041963
APA StyleLum, M., Wolfenden, L., Jones, J., Grady, A., Christian, H., Reilly, K., & Yoong, S. L. (2022). Interventions to Improve Child Physical Activity in the Early Childhood Education and Care Setting: An Umbrella Review. International Journal of Environmental Research and Public Health, 19(4), 1963. https://doi.org/10.3390/ijerph19041963