
Spatial-Temporal Evolution of Health Impact and Economic Loss upon Exposure to PM2.5 in China

Abstract
:1. Introduction
2. Methods and Data Sources
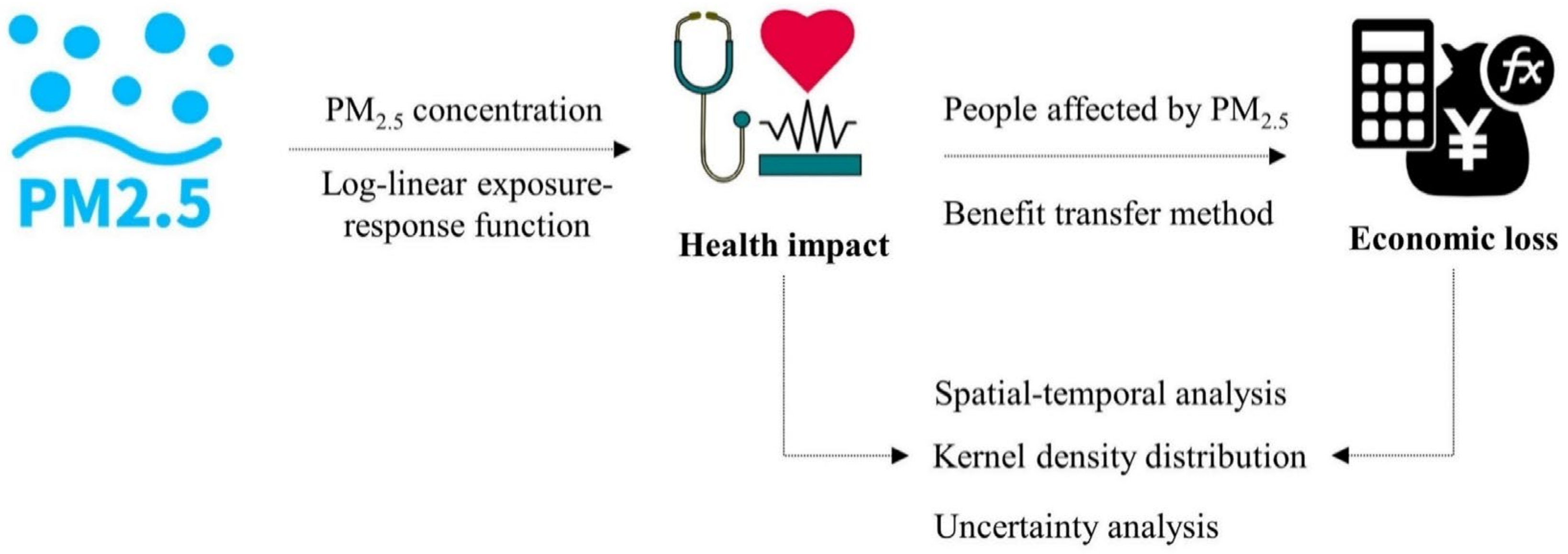
2.1. Health Impact Assessment
2.2. Economic Loss Estimation
2.3. Data Sources
3. Results
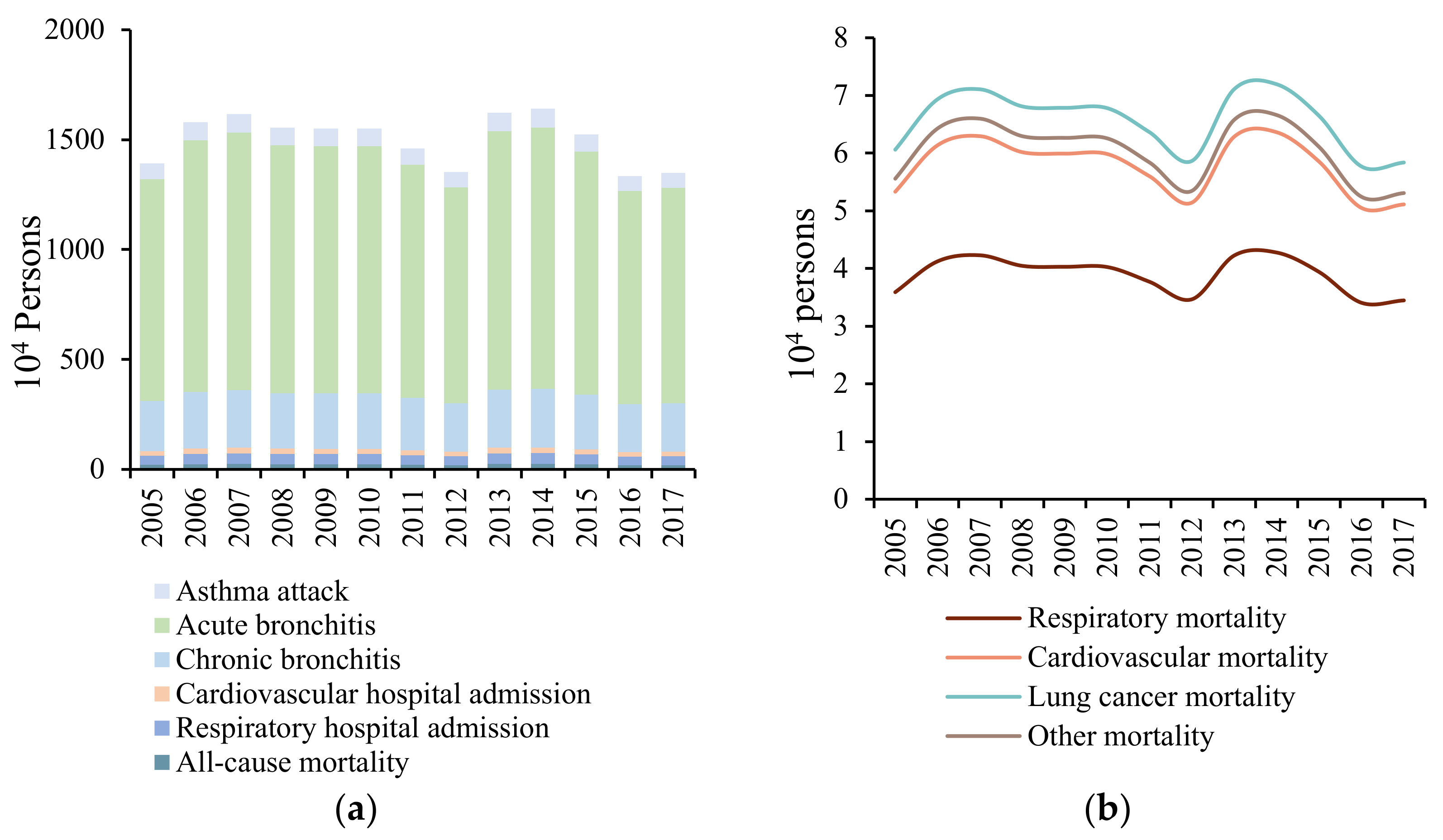
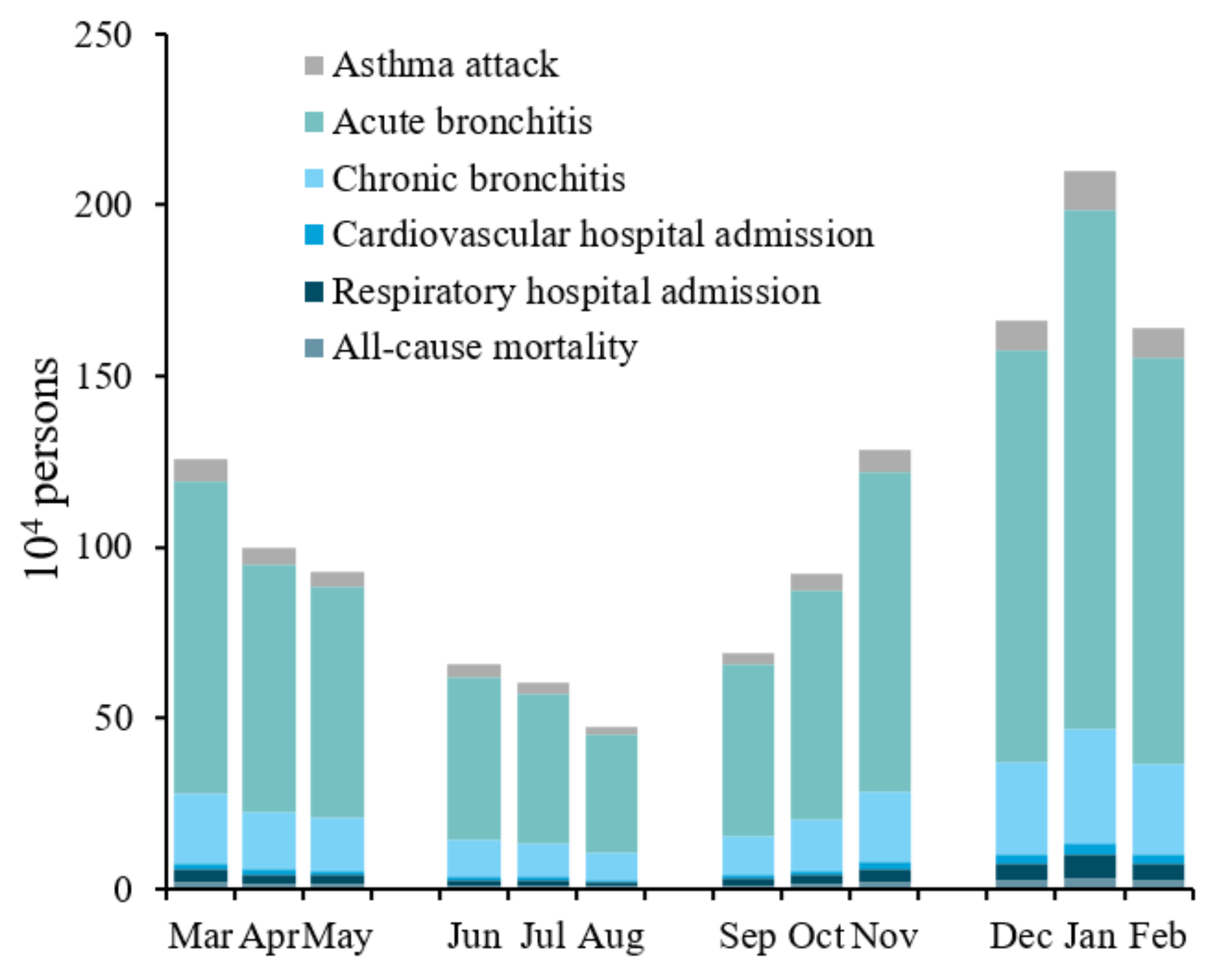
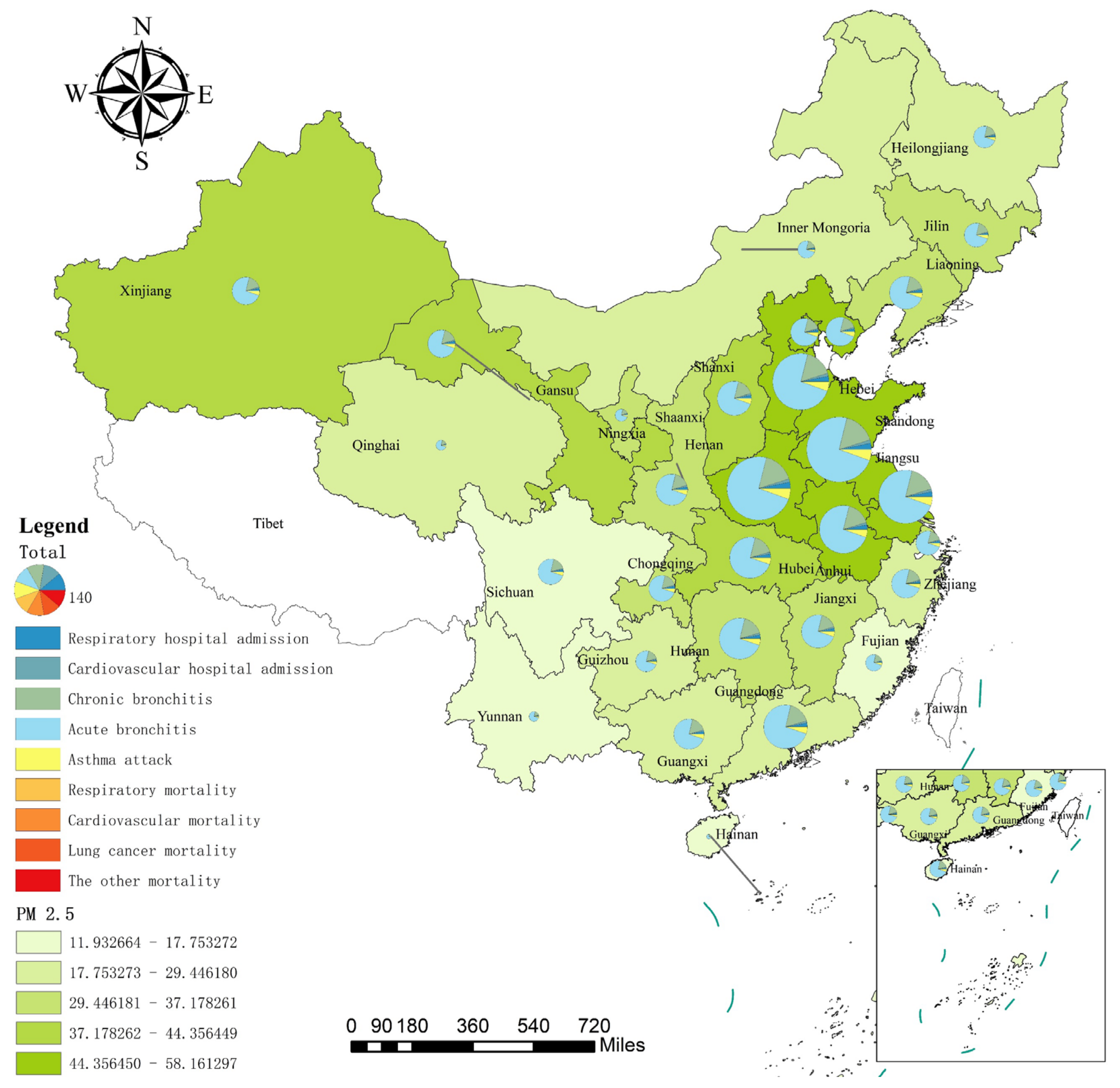
3.1. Evaluating Health Impact
3.2. Estimating Economic Loss
3.3. Dynamic Evolution Analysis of the Kernel Density
3.4. Uncertainty Analysis
4. Conclusions and Policy Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Health Effects Institute. State of Global Air 2020: A Special Report on Globle Exposure to Air Pollution and Its Health Impacts; Health Effects Institute: Boston, MA, USA, 2020. [Google Scholar]
- Mazidi, M.; Speakman, J.R. Ambient particulate air pollution (PM2.5) is associated with the ratio of type 2 diabetes to obesity. Sci. Rep. 2017, 7, 9144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, R.A.; West, J.J.; Lamarque, J.; Shindell, D.T.; Collins, W.J.; Faluvegi, G.; Folberth, G.A.; Horowitz, L.W.; Nagashima, T.; Naik, V.; et al. Future global mortality from changes in air pollution attributable to climate change. Nat. Clim. Chang. 2017, 7, 647–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDuffie, E.E.; Martin, R.V.; Spadaro, J.V.; Burnett, R.; Smith, S.J.; O’Rourke, P.; Hammer, M.S.; van Donkelaar, A.; Bindle, L.; Shah, V.; et al. Source sector and fuel contributions to ambient PM2.5 and attributable mortality across multiple spatial scales. Nat. Commun. 2021, 12, 3594. [Google Scholar] [CrossRef]
- Liu, M.; Saari, R.K.; Zhou, G.; Li, J.; Han, L.; Liu, X. Recent trends in premature mortality and health disparities attributable to ambient PM2.5 exposure in China: 2005–2017. Environ. Pollut. 2021, 279, 116882. [Google Scholar] [CrossRef] [PubMed]
- Ou, Y.; West, J.J.; Smith, S.J.; Nolte, C.G.; Loughlin, D.H. Air pollution control strategies directly limiting national health damages in the US. Nat. Commun. 2020, 11, 957. [Google Scholar] [CrossRef] [Green Version]
- Sokoty, L.; Rimaz, S.; Hassanlouei, B.; Kermani, M.; Janani, L. Short-term effects of air pollutants on hospitalization rate in patients with cardiovascular disease: A case-crossover study. Environ. Sci. Pollut. Res. 2021, 28, 26124–26131. [Google Scholar] [CrossRef]
- Wang, Q.; Liu, C.; Hou, Y.; Xin, F.; Mao, Z.; Xue, X. Study of the spatio-temporal variation of environmental sustainability at national and provincial levels in China. Sci. Total Environ. 2022, 807, 150830. [Google Scholar] [CrossRef]
- Jin, G.; Bingmei, G.; Xialing, S.; Jinli, X.; Baiyun, Y. Communication barrier, spillover effect and industrial-technological innovation. Sustainability 2019, 11, 4841. [Google Scholar]
- Yang, J.; Song, D.; Fang, D.; Wu, F. Drivers of consumption-based PM2.5 emission of Beijing: A structural decomposition analysis. J. Clean. Prod. 2019, 219, 734–742. [Google Scholar] [CrossRef]
- Creutzig, F.; Niamir, L.; Bai, X.; Callaghan, M.; Cullen, J.; Diaz-Jose, J.; Figueroa, M.; Grubler, A.; Lamb, W.F.; Leip, A.; et al. Demand-side solutions to climate change mitigation consistent with high levels of well-being. Nat. Clim. Chang. 2021, 12, 36–46. [Google Scholar] [CrossRef]
- Yue, H.; He, C.; Huang, Q.; Yin, D.; Bryan, B.A. Stronger policy required to substantially reduce deaths from PM2.5 pollution in China. Nat. Commun. 2020, 11, 1462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, P.; Liang, J.; Qiu, Y.; Li, Q.; Xing, B. Increase in domestic electricity consumption from particulate air pollution. Nat. Energy 2020, 5, 985–995. [Google Scholar] [CrossRef]
- Hong, C.; Zhang, Q.; Zhang, Y.; Davis, S.J.; Zhang, X.; Tong, D.; Guan, D.; Liu, Z.; He, K. Weakening aerosol direct radiative effects mitigate climate penalty on Chinese air quality. Nat. Clim. Chang. 2020, 10, 845–850. [Google Scholar] [CrossRef]
- Sun, X.; Zhang, R.; Wang, G.; Guo, J.; Liu, Z. Factor decomposition, reduction potential, and rebound effect of energy consumption related PM2.5 in China. J. Clean. Prod. 2021, 322, 129088. [Google Scholar] [CrossRef]
- Lin, X.; Du, Z.; Liu, Y.; Hao, Y. The short-term association of ambient fine particulate air pollution with hypertension clinic visits: A multi-community study in Guangzhou, China. Sci. Total Environ. 2021, 774, 145707. [Google Scholar] [CrossRef] [PubMed]
- Han, C.; Xu, R.; Gao, C.X.; Yu, W.; Zhang, Y.; Han, K.; Yu, P.; Guo, Y.; Li, S. Socioeconomic disparity in the association between long-term exposure to PM2.5 and mortality in 2640 Chinese counties. Environ. Int. 2021, 146, 106241. [Google Scholar] [CrossRef]
- Wang, J.; Xu, X.; Wang, S.; He, S.; He, P. Heterogeneous effects of COVID-19 lockdown measures on air quality in Northern China. Appl. Energy 2021, 282, 116179. [Google Scholar] [CrossRef]
- Chen, J.; Gao, M.; Li, D.; Li, L.; Song, M.; Xie, Q. Changes in PM2.5 emissions in China: An extended chain and nested refined laspeyres index decomposition analysis. J. Clean. Prod. 2021, 294, 126248. [Google Scholar] [CrossRef]
- Czwojdzińska, M.; Terpińska, M.; Kuźniarski, A.; Płaczkowska, S.; Piwowar, A. Exposure to PM2.5 and PM10 and COVID-19 infection rates and mortality: A one-year observational study in Poland. Biomed. J. 2021, in press. [Google Scholar] [CrossRef]
- Luo, G.; Zhang, L.; Hu, X.; Qiu, R. Quantifying public health benefits of PM2.5 reduction and spatial distribution analysis in China. Sci. Total Environ. 2020, 719, 137445. [Google Scholar] [CrossRef]
- Thiankhaw, K.; Chattipakorn, N.; Chattipakorn, S.C. PM2.5 exposure in association with AD-related neuropathology and cognitive outcomes. Environ. Pollut. 2022, 292, 118320. [Google Scholar] [CrossRef]
- Zhu, N.; Ji, X.; Geng, X.; Yue, H.; Li, G.; Sang, N. Maternal PM2.5 exposure and abnormal placental nutrient transport. Ecotoxicol. Environ. Saf. 2021, 207, 111281. [Google Scholar] [CrossRef] [PubMed]
- Bu, X.; Xie, Z.; Liu, J.; Wei, L.; Wang, X.; Chen, M.; Ren, H. Global PM2.5-attributable health burden from 1990 to 2017: Estimates from the global burden of disease study 2017. Environ. Res. 2021, 197, 111123. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Zhang, T.; Zhang, Y.; Chen, H.; Sang, S. Global burden of COPD attributable to ambient PM2.5 in 204 countries and territories, 1990 to 2019: A systematic analysis for the Global Burden of Disease Study 2019. Sci. Total Environ. 2021, 796, 148819. [Google Scholar] [CrossRef] [PubMed]
- Maji, K.J.; Arora, M.; Dikshit, A.K. Burden of disease attributed to ambient PM2.5 and exposure in 190 cities in China. Environ. Sci. Pollut. Res. 2017, 24, 11559–11572. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Dai, H.; Dong, H.; Hanaoka, T.; Masui, T. Economic impacts from PM2.5 pollution-related health effects in China: A provincial-level analysis. Environ. Sci. Technol. 2016, 50, 4836–4843. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Zhang, Z.; Shao, C.; Zhao, R.; Guan, Y.; Chen, C. Spatio-temporal variation and driving factors analysis of PM2.5 health risks in Chinese cities. Ecol. Indic. 2021, 129, 107937. [Google Scholar] [CrossRef]
- Chen, H.; Li, L.; Lei, Y.; Wu, S.; Yan, D.; Dong, Z. Public health effect and its economics loss of PM2.5 pollution from coal consumption in China. Sci. Total Environ. 2020, 732, 138973. [Google Scholar] [CrossRef]
- Xue, T.; Liu, J.; Zhang, Q.; Geng, G.; Zheng, Y.; Tong, D.; Liu, Z.; Guan, D.; Bo, Y.; Zhu, T.; et al. Rapid improvement of PM2.5 pollution and associated health benefits in China during 2013–2017. Sci. China Earth Sci. 2019, 62, 1847–1856. [Google Scholar] [CrossRef]
- Zhang, B.; Wu, B.; Liu, J. PM2.5 pollution-related health effects and willingness to pay for improved air quality: Evidence from China’s prefecture-level cities. J. Clean. Prod. 2020, 273, 122876. [Google Scholar] [CrossRef]
- Li, L.; Lei, Y.; Wu, S.; Huang, Z.; Luo, J.; Wang, Y.; Chen, J.; Yan, D. Evaluation of future energy consumption on PM2.5 emissions and public health economic loss in Beijing. J. Clean. Prod. 2018, 187, 1115–1128. [Google Scholar] [CrossRef]
- Wang, J.; Zhang, L.; Niu, X.; Liu, Z. Effects of PM2.5 on health and economic loss: Evidence from Beijing-Tianjin-Hebei region of China. J. Clean. Prod. 2020, 257, 120605. [Google Scholar] [CrossRef]
- Guan, Y.; Kang, L.; Wang, Y.; Zhang, N.; Ju, M. Health loss attributed to PM2.5 pollution in China’s cities: Economic impact, annual change and reduction potential. J. Clean. Prod. 2019, 217, 284–294. [Google Scholar] [CrossRef]
- Maji, K.J.; Ye, W.; Arora, M.; Shiva Nagendra, S.M. PM2.5-related health and economic loss assessment for 338 Chinese cities. Environ. Int. 2018, 121, 392–403. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Fang, D.; Chen, B. Human health impact and economic effect for PM2.5 exposure in typical cities. Appl. Energ. 2019, 249, 316–325. [Google Scholar] [CrossRef]
- ICD-10. International Statistical Classification of Diseases and Related Health Problems 10th Revision. Available online: https://icd.who.int/browse10/2019/en# (accessed on 10 August 2021).
- Yin, H.; Pizzol, M.; Xu, L. External costs of PM2.5 pollution in Beijing, China: Uncertainty analysis of multiple health impacts and costs. Environ. Pollut. 2017, 226, 356–369. [Google Scholar] [CrossRef]
- Chen, R.; Li, Y.; Ma, Y.; Pan, G.; Zeng, G.; Xu, X.; Chen, B.; Kan, H. Coarse particles and mortality in three Chinese cities: The China Air Pollution and Health Effects Study (CAPES). Sci. Total Environ. 2011, 409, 4934–4938. [Google Scholar] [CrossRef]
- Guo, H.; Li, W.; Wu, J. Ambient PM2.5 and annual lung cancer incidence: A nationwide study in 295 Chinese counties. Int. J. Environ. Res. Public Health 2020, 17, 1481. [Google Scholar] [CrossRef] [Green Version]
- Lelieveld, J.; Evans, J.S.; Fnais, M.; Giannadaki, D.; Pozzer, A. The contribution of outdoor air pollution sources to premature mortality on a global scale. Nature 2015, 525, 367–371. [Google Scholar] [CrossRef]
- Cao, J.; Yang, C.; Li, J.; Chen, R.; Chen, B.; Gu, D.; Kan, H. Association between long-term exposure to outdoor air pollution and mortality in China: A cohort study. J. Hazard. Mater. 2011, 186, 1594–1600. [Google Scholar] [CrossRef]
- Huang, Q.; Xu, Q.; Chai, Y. Assessment of PM2.5 pollution and its influence on health and economic benefits based on BenMAP in China. J. Saf. Environ. 2017, 37, 2278–2779. [Google Scholar]
- Peng, X.; Xiaoyun, L.; Zhaorong, L.; Tiantian, L.; Yuhua, B. Study of exposure-response relationship of air particulate pollution in China. China Environ. Sci. 2009, 29, 1034–1040. [Google Scholar]
- Huang, D.S.; Zhang, S.Q. Health benefit evaluation for PM2.5 pollution control in Beijing-Tianjin-Hebei region of China. China Environ. Sci. 2013, 33, 166–174. [Google Scholar]
- Wang, G.; Wu, L.; Chen, J.; Song, Y.; Chen, R. A CGE-based analysis on PM2.5-induced health-related economic effect in Beijing. China Environ. Sci. 2017, 37, 2779–2785. [Google Scholar]
- National Health and Family Planning Commission. China Health and Family Planning Statistical Yearbook 2005; Peking Union Medical College Press: Beijing, China, 2005. [Google Scholar]
- Giannadaki, D.; Giannakis, E.; Pozzer, A.; Lelieveld, J. Estimating health and economic benefits of reductions in air pollution from agriculture. Sci. Total Environ. 2018, 622–623, 1304–1316. [Google Scholar] [CrossRef]
- Lu, X.; Lin, C.; Li, Y.; Yao, T.; Fung, J.C.H.; Lau, A.K.H. Assessment of health burden caused by particulate matter in southern China using high-resolution satellite observation. Environ. Int. 2017, 98, 160–170. [Google Scholar] [CrossRef]
- OECD. The Cost of air Pollution: Health Impact of Road Transport. Available online: https://www.oecd-ilibrary.org/content/publication/9789264210448-en (accessed on 10 August 2021).
- Guo, X.R.; Cheng, S.Y.; Chen, D.S.; Zhou, Y.; Wang, H.Y. Estimation of economic costs of particulate air pollution from road transport in China. Atmos. Environ. 2010, 44, 3369–3377. [Google Scholar] [CrossRef]
- Hammitt, J.K.; Zhou, Y. The economic value of air-pollution-related health risks in China: A contingent valuation study. Environ. Resour. Econ. 2006, 33, 399–423. [Google Scholar] [CrossRef]
- World Health Organization. Air Quality Guidelines for Particulate Matter, Ozone, Nitrogen Dioxide and Sulfur Dioxide. Available online: http://apps.who.int/iris/bitstream/10665/69477/1/WHO_SDE_PHE_OEH_06.02_eng.pdf (accessed on 10 August 2021).
- National Bureau of Statistics of China. (2006a–2018a); China Statistical Yearbook 2006–2018; China Statistics Press: Beijing, China, 2006–2018.
- Wang, Z.; Li, Y.; Chen, T. Spatial-temporal characteristics of PM2.5 in Beijing in 2013. Acta Geogr. Sin. 2015, 70, 110–120. [Google Scholar]
- Li, J.; Ye, S. Regional policy synergy and haze governance-empirical evidence from 281 prefecture-level cities in China. Environ. Sci. Pollut. Res. 2021, 28, 10763–10779. [Google Scholar] [CrossRef]
- Liu, Y.; Sun, X.; Sun, Y.; Li, C. Evolution of spatial pattern of atmospheric PM2.5 pollution concentration in China from 1998 to 2016: Based on an empirical study of 339 cities. Resour. Environ. Yangtze Basin 2020, 5, 1163–1173. [Google Scholar]
- Sun, X.; Zhang, R.; Chen, X.; Li, P.; Guo, J. Impact of nanotechnology patents on green development of China’s building industry. Recent Pat. Nanotechnol. 2020, 14, 141–152. [Google Scholar] [CrossRef] [PubMed]
- Quah, E.; Boon, T.L. The economic cost of particulate air pollution on health in Singapore. J. Asian Econ. 2003, 14, 73–90. [Google Scholar] [CrossRef]
- Guo, J.; Niu, H.; Xiao, D.; Sun, X.; Fan, L. Urban green-space water-consumption characteristics and its driving factors in China. Ecol. Indic. 2021, 130, 108076. [Google Scholar] [CrossRef]
- Huang, J.; Zhu, Y.; Kelly, J.T.; Jang, C.; Wang, S.; Xing, J.; Chiang, P.; Fan, S.; Zhao, X.; Yu, L. Large-scale optimization of multi-pollutant control strategies in the Pearl River Delta region of China using a genetic algorithm in machine learning. Sci. Total Environ. 2020, 722, 137701. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Dai, H.; Zhang, Y.; Wu, Y.; Hanaoka, T.; Masui, T. Comparison of health and economic impacts of PM2.5 and ozone pollution in China. Environ. Int. 2019, 130, 104881. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Health Endpoint | (95% CI) | Reference |
|---|---|---|
| All-cause mortality | 0.00090 (0.00000, 0.00180) | Cao et al. [42]; Huang et al. [43]; Yin et al. [38] |
| Respiratory mortality | 0.00143 (0.00085, 0.00201) | Peng et al. [44]; Yin et al. [38] |
| Cardiovascular mortality | 0.00053 (0.00015, 0.00090) | Peng et al. [44]; Yin et al. [38] |
| Lung cancer mortality | 0.00340 (0.00000, 0.00710) | Cao et al. [42]; Huang et al. [43]; Yin et al. [38] |
| Respiratory hospital admission | 0.00109 (0.00000, 0.00221) | Huang and Zhang [45]; Wang et al. [33]; Yang et al. [36] |
| Cardiovascular hospital admission | 0.00068 (0.00043, 0.00093) | Huang and Zhang [45]; Wang et al. [33]; Yang et al. [36]; Yin et al. [38] |
| Chronic bronchitis | 0.01009 (0.00366, 0.01559) | Huang and Zhang [45]; Wang et al. [46]; Wang et al. [33] |
| Acute bronchitis | 0.00790 (0.00270, 0.01300) | Huang and Zhang [45]; Wang et al. [33]; Yin et al. [38] |
| Asthma attack | 0.00210 (0.00145, 0.00274) | Huang and Zhang [45]; Yang et al. [36]; Yin et al. [38] |
| Health Endpoint | Reference | |
|---|---|---|
| All-cause mortality | 0.006136 | National Health and Family Planning Commission [47] |
| Respiratory mortality | 0.000680 | National Health and Family Planning Commission [47] |
| Cardiovascular mortality | 0.002690 | Yin et al. [38] |
| Lung cancer mortality | 0.000497 | Yin et al. [38] |
| Respiratory hospital admission | 0.010200 | National Health and Family Planning Commission [47] |
| Cardiovascular hospital admission | 0.008550 | Wang et al. [46] |
| Chronic bronchitis | 0.006900 | National Health and Family Planning Commission [47] |
| Acute bronchitis | 0.038000 | Yin et al. [38] |
| Asthma attack | 0.009400 | Yin et al. [38] |
| Health Endpoint | Method | Reference | |
|---|---|---|---|
| All-cause mortality | 132,000 | Adjusted human capital (AHC) | Guo et al. [51]; Hammitt and Zhou, [52]; Yin et al. [38] |
| Respiratory mortality | |||
| Cardiovascular mortality | |||
| Lung cancer mortality | |||
| Respiratory hospital admission | 792.90 | Cost of illness (COI) | Maji et al. [35] |
| Cardiovascular hospital admission | 1600 | Cost of illness (COI) | Yin et al. [38] |
| Chronic bronchitis | 7000 | Adjusted human capital (AHC) | Guo et al. [51]; Maji et al. [35]; Yin et al. [38] |
| Acute bronchitis | 9 | Willingness to pay (WTP) | Guo et al. [51]; Yin et al. [38] |
| Asthma attack | 7 | Willingness to pay (WTP) | Guo et al. [51]; Maji et al. [35]; Yin et al. [38] |
| Year | Baseline Concentration 0 µg/m3 | Baseline Concentration 10 µg/m3 | ||
|---|---|---|---|---|
| Health Impact (104 Persons) | (95% Confidence Interval) | Health Impact (104 Persons) | (95% Confidence Interval) | |
| 2005 | 1800.712 | (695.872, 2685.142) | 1392.344 | (526.008, 2118.382) |
| 2006 | 1978.924 | (771.993, 2926.691) | 1580.378 | (602.849, 2383.763) |
| 2007 | 2016.671 | (787.824, 2978.886) | 1617.336 | (617.836, 2436.388) |
| 2008 | 1962.916 | (763.791, 2909.477) | 1555.026 | (591.624, 2351.009) |
| 2009 | 1962.826 | (763.109, 2911.493) | 1550.647 | (589.445, 2346.207) |
| 2010 | 1966.307 | (764.018, 2918.132) | 1550.397 | (589.000, 2347.077) |
| 2011 | 1885.919 | (729.167, 2810.957) | 1461.029 | (552.2416, 2221.853) |
| 2012 | 1789.161 | (687.764, 2680.348) | 1353.639 | (508.623, 2069.571) |
| 2013 | 2041.683 | (795.224, 3023.635) | 1622.542 | (617.935, 2450.876) |
| 2014 | 2061.576 | (803.365, 3051.796) | 1640.878 | (625.232, 2477.466) |
| 2015 | 1956.514 | (757.594, 2912.364) | 1524.168 | (576.990, 2314.685) |
| 2016 | 1783.839 | (684.017, 2678.245) | 1334.372 | (500.109, 2044.817) |
| 2017 | 1801.503 | (691.031, 2703.931) | 1349.800 | (506.072, 2067.790) |
| Year | Baseline Concentration 0 µg/m3 | Baseline Concentration 10 µg/m3 | ||||
|---|---|---|---|---|---|---|
| Economic Loss (million USD) | (95% Confidence Interval) | Proportion in GDP | Economic Loss (million USD) | (95% Confidence Interval) | Proportion in GDP | |
| 2005 | 57,522.02 | (8660.47, 101,210.74) | 2.72% | 43,775.81 | (6573.66, 77,554.43) | 2.07% |
| 2006 | 70,763.42 | (10,663.94, 124,171.13) | 2.87% | 55,618.70 | (8361.95, 98,241.52) | 2.26% |
| 2007 | 82,384.33 | (12,416.80, 144,505.27) | 2.78% | 65,026.05 | (9777.93, 114,807.88) | 2.20% |
| 2008 | 89,543.43 | (13,490.81, 157,239.73) | 2.47% | 69,815.93 | (10,493.16, 123,417.55) | 1.92% |
| 2009 | 96,165.01 | (14,487.25, 168,908.35) | 2.33% | 74,771.21 | (11,236.75, 132,212.59) | 1.82% |
| 2010 | 106,659.00 | (16,067.26, 187,371.65) | 2.27% | 82,770.70 | (12,438.028, 146,384.33) | 1.76% |
| 2011 | 112,843.20 | (16,990.46, 198,519.83) | 2.05% | 86,041.52 | (12,921.40, 152,408.87) | 1.56% |
| 2012 | 115,170.90 | (17,330.35, 202,960.71) | 1.85% | 85,764.00 | (12,869.78, 152,202.44) | 1.38% |
| 2013 | 142,425.00 | (21,460.06, 250,030.15) | 2.06% | 111,397.80 | (16,744.83, 196,863.19) | 1.61% |
| 2014 | 152,784.00 | (23,021.99, 268,178.29) | 2.02% | 119,684.30 | (17,991.49, 211,474.72) | 1.58% |
| 2015 | 151,470.60 | (22,809.95, 266,359.28) | 1.90% | 116,137.40 | (17,444.45, 205,620.39) | 1.46% |
| 2016 | 144,049.50 | (21,669.92, 254,040.29) | 1.80% | 106,058.80 | (15,909.77, 188,372.44) | 1.33% |
| 2017 | 152,775.30 | (22,983.47, 269,400.71) | 1.82% | 112,668.00 | (16,902.03, 200,088.18) | 1.34% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, X.; Zhang, R.; Wang, G. Spatial-Temporal Evolution of Health Impact and Economic Loss upon Exposure to PM2.5 in China. Int. J. Environ. Res. Public Health 2022, 19, 1922. https://doi.org/10.3390/ijerph19041922
Sun X, Zhang R, Wang G. Spatial-Temporal Evolution of Health Impact and Economic Loss upon Exposure to PM2.5 in China. International Journal of Environmental Research and Public Health. 2022; 19(4):1922. https://doi.org/10.3390/ijerph19041922
Chicago/Turabian StyleSun, Xialing, Rui Zhang, and Geyi Wang. 2022. "Spatial-Temporal Evolution of Health Impact and Economic Loss upon Exposure to PM2.5 in China" International Journal of Environmental Research and Public Health 19, no. 4: 1922. https://doi.org/10.3390/ijerph19041922
APA StyleSun, X., Zhang, R., & Wang, G. (2022). Spatial-Temporal Evolution of Health Impact and Economic Loss upon Exposure to PM2.5 in China. International Journal of Environmental Research and Public Health, 19(4), 1922. https://doi.org/10.3390/ijerph19041922