
Depressive and Sexual Disorders during the First and Second Wave of the COVID-19 Pandemic among Young Polish Women

 ,
,  ,
,  , ,
, ,  , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Variable | First Wave (N = 1644) | Second Wave (N = 720) | p-Value |
|---|---|---|---|
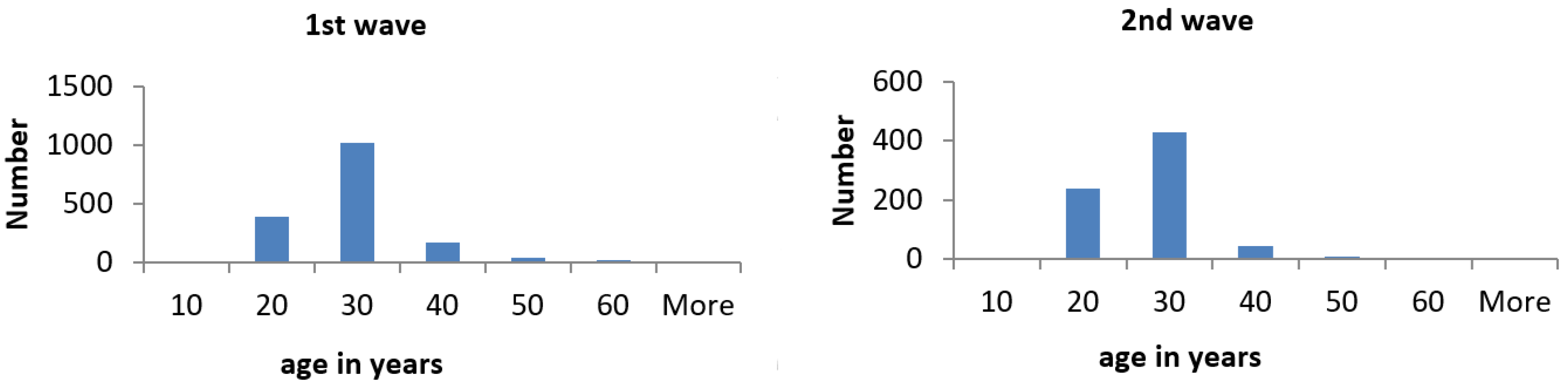
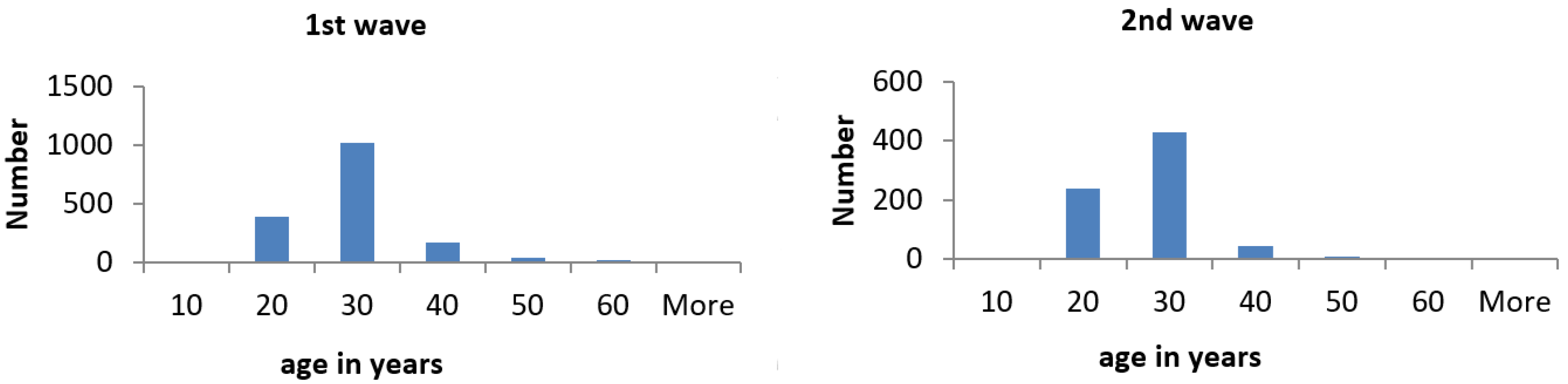
| Age, years (distribution other than normal) | Mean 25.11 ± 7.09 | Mean 23.23 ± 5.34 | <0.001 |
| Median 23 | Median 22.00 | ||
| IQR (21–27) | IQR (18–25) | ||
| Range (18–67) | Range (18–55) | ||
| Education | |||
| Primary | 88 (5.4%) | 42 (5.83%) | <0.001 |
| Vocational | 74 (4.5%) | 15 (2.08%) | |
| Secondary | 780 (47.4%) | 414 (57.5%) | |
| Higher | 702 (42.7%) | 249 (34.58%) | |
| Employment status | |||
| Employed—working at work place | 407 (24.8%) | 165 (22.92%) | <0.001 |
| Remote work | 331 (20.1%) | 66 (9.17%) | |
| Employment issues due to pandemic | 55 (3.3%) | 4 (0.56%) | |
| Sick leave | 60 (3.6%) | 19 (2.64%) | |
| Unemployed due to other reasons | 58 (3.5%) | 20 (2.78%) | |
| Full-time student | 637 (38.8%) | 435 (60.42%), including: students 391(54.31%) and pupils 44 (6.11%). | |
| Student—income lost | 24 (1.5%) | 2 (0.28%) | |
| Maternity leave/stay-at-home-mum | 58 (3.5%) | 5 (0.69%) | |
| Childcare due to COVID-19 pandemic | 9 (0.5%) | 1 (0.14%) | |
| Pensioner | 5 (0.3%) | 3 (0.42%) | |
| Marital status | |||
| Single | 278 (16.9%) | 150 (20.84%) | <0.001 |
| Married | 302 (18.4%) | 79 (10.97%) | |
| In partnership | 1064 (64.7%) | 491 (68.19%) | |
| Place of living | |||
| Rural area | 311 (18.9%) | 139 (19.30%) | <0.001 |
| City >50,000 inhabitants | 267 (16.2%) | 99 (13.75%) | |
| City from 50,000 to 100,000 | 142 (8.6%) | 73 (1 0.14%) | |
| City from 100,000 to 250,000 | 186 (11.3%) | 82 (11.39%) | |
| City above 250,000 inhabitants | 738 (44.9%) | 327 (45.42%) |
| Variable | First Wave (N = 1644) | Second Wave (N = 720) | p-Value |
|---|---|---|---|
| Comorbid chronic disease | |||
| No | 1306 (79.4%) | 560 (77.78%) | 0.362 |
| Yes | 338 (20.6%) | 160 (22.22%) | |
| On treatment due to any disease | |||
| No | 1072 (65.2%) | 440 (61.11%) | 0.056 |
| Yes | 572 (34.8%) | 280 (38.89%) | |
| In quarantine | |||
| No | 1590 (96.7%) | 598 (83.06%) | <0.001 |
| Yes | 54 (3.3%) | 122 (16.94%) | |
| Friends/family in quarantine | |||
| No | 1351 (82.2%) | 336 (46.67%) | <0.001 |
| Yes | 293 (17.8%) | 384 (53.33%) | |
| History of contact with infected with COVID-19 | |||
| No | 1615 (98.2%) | 473 (65.69%) | <0.001 |
| Yes | 29 (1.8%) | 247 (34.31%) | |
| Diagnosed with COVID-19 | |||
| No | 1638 (99.6%) | 674 (93.61%) | <0.001 |
| Yes | 6 (0.4%) | 46 (6.39%) | |
| Friends/family infected with COVID-19 | |||
| No | 1544 (93.9%) | 260 (36.11%) | <0.001 |
| Yes | 100 (6.1%) | 460 (63.89%) | |
| Friends/family died of COVID-19 | |||
| No | 1620 (98.5%) | 649 (90.14%) | <0.001 |
| Yes | 24 (1.5%) | 71 (9.86%) |
| Variable | First Wave (N = 1644) | Second Wave (N = 720) | p-Value |
|---|---|---|---|
| Under psychiatric/psychological care during COVID-19 pandemic | |||
| No | 1537 (93.5%) | 616 (85.56%) | <0.001 |
| Yes | 107 (6.5%) | 104 (14.44%) | |
| On sedatives during COVID-19 pandemic | |||
| No | 1520 (92.5%) | 668 (92.78%) | 0.785 |
| Yes | 124 (7.5%) | 52 (7.22%) | |
| Fear of infection with coronavirus has negative impact on my mental health | |||
| Strongly agree | 125 (7.6%) | 61 (8.47%) | |
| Agree | 410 (24.9%) | 180 (25.00%) | |
| Undecided | 382 (23.2%) | 134 (18.61%) | 0.139 |
| Disagree | 393 (23.9%) | 189 (26.25%) | |
| Strongly disagree | 334 (20.3%) | 156 (21.67%) | |
| Fear of heath condition of the loved ones is a source of stress and depressed mood | |||
| Strongly agree | 302 (18.4%) | 179 (24.86%) | |
| Agree | 642 (39.1%) | 290 (40.28%) | 0.003 |
| Undecided | 234 (14.2%) | 96 (13.33%) | |
| Disagree | 305 (18.6%) | 93 (12.92%) | |
| Strongly disagree | 161 (9.8%) | 62 (8.61%) | |
| Following the media reports is a source of a significant deterioration of my mental state | |||
| Strongly agree | 344 (20.9%) | 189 (26.25%) | |
| Agree | 461 (28.0%) | 209 (29.03%) | 0.017 |
| Undecided | 307 (18.7%) | 106 (14.72%) | |
| Disagree | 295 (17.9%) | 116 (16.11%) | |
| Strongly disagree | 237 (14.4%) | 100 (13.89%) | |
| Perceived loneliness caused by isolation from the world/loved ones | |||
| Strongly agree | 528 (32.1%) | 223(30.97%) | |
| Agree | 191 (11.6%) | 223 (30.97%) | |
| Undecided | 176 (10.7%) | 91 (12.64%) | <0.001 |
| Disagree | 191 (11.6%) | 107 (14.86%) | |
| Strongly disagree | 187 (11.4%) | 76 (10.56%) | |
| More frequent use of alcohol/cigarettes cause by pandemic | |||
| Strongly agree | 165 (10.0%) | 49 (6.81%) | |
| Agree | 235 (14.3%) | 105 (14.58%) | 0.118 |
| Undecided | 154 (9.4%) | 61 (8.47%) | |
| Disagree | 257 (15.6%) | 121 (16.81%) | |
| Strongly disagree | 833 (50.7%) | 384 (53.33%) |
| Variable | Variable | I Wave | II Wave | Fisher’s z | ||
|---|---|---|---|---|---|---|
| Correlation Coef. | p Value | Correlation Coef. | p Value | |||
| BDI | FSFI | −0.3261 | <0.001 | −0.2769 | <0.001 | 0.2267 |
| FSFI | Age | 0.04983 | 0.0434 | 0.0662 | 0.076 | 0.5573 |
| In quarantine | 0.02175 | 0.3782 | ||||
| Diagnosed with COVID-19 | −0.01121 | 0.6496 | ||||
| Comorbid chronic disease | −0.08747 | <0.001 | ||||
| Fear of infection | −0.08848 | <0.001 | −0.1290 | 0.01 | 0.3597 | |
| Fear of heath condition | −0.1016 | <0.001 | −0.0824 | 0.027 | 0.6654 | |
| Following the media | −0.1046 | <0.001 | −0.0426 | <0.084 | 0.1679 | |
| Perceived loneliness | −0.1527 | <0.001 | −0.1141 | <0.01 | 0.38 | |
| More frequent use of alcohol/cigarettes | −0.03532 | 0.1523 | 0.0064 | 0.864 | 0.3515 | |
| BDI | Age | −0.3261 | <0.001 | −0.1970 | <0.001 | <0.001 |
| In quarantine | −0.02053 | 0.4055 | ||||
| Diagnosed with COVID-19 | 0.01882 | 0.4456 | ||||
| Comorbid chronic disease | 0.05604 | 0.0231 | ||||
| Fear of infection | 0.2936 | <0.001 | 0.2556 | <0.001 | 0.3586 | |
| Fear of heath condition | 0.3047 | <0.001 | 0.2502 | <0.001 | 0.2952 | |
| Following the media | 0.2738 | <0.001 | 0.2260 | <0.001 | 0.262 | |
| Perceived loneliness | 0.3923 | <0.001 | 0.3083 | <0.001 | 0.324 | |
| More frequent use of alcohol/cigarettes | 0.2308 | <0.001 | 0.2744 | <0.001 | 0.2982 | |
References
- Coronavirus Important Information. Available online: https://www.gov.pl/ (accessed on 15 November 2021).
- Pennanen-Iire, C.; Prereira-Lourenço, M.; Padoa, A.; Ribeirinho, A.; Samico, A.; Gressler, M.; Jatoi, N.A.; Mehrad, M.; Girard, A. Sexual Health Implications of COVID-19 Pandemic. Sex. Med. Rev. 2021, 9, 3–14. [Google Scholar] [CrossRef]
- De Oliveira, L.; Carvalho, J. Women’s Sexual Health During the Pandemic of COVID-19: Declines in Sexual Function and Sexual Pleasure. Curr. Sex. Health Rep. 2021, 13, 76–88. [Google Scholar] [CrossRef] [PubMed]
- Silva, F.J.G., Jr.; Sales, J.C.e.S.; Monteiro, C.F.S.; Costa, A.P.C.; Campos, L.R.B.; Miranda, P.I.G.; Monteiro, T.A.S.; Lima, R.A.G.; Lopes-Junior, L.C. Impact of COVID-19 pandemic on mental health of young people and adults: A systematic review protocol of observational studies. BMJ Open 2020, 10, e039426. [Google Scholar] [CrossRef] [PubMed]
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 20 September 2021).
- Dragun, R.; Veček, N.N.; Marendić, M.; Pribisalić, A.; Đivić, G.; Cena, H.; Polašek, O.; Kolčić, I. Have Lifestyle Habits and Psychological Well-Being Changed among Adolescents and Medical Students Due to COVID-19 Lockdown in Croatia? Nutrients 2020, 13, 97. [Google Scholar] [CrossRef] [PubMed]
- Döring, N. How is the COVID-19 Pandemic Affecting Our Sexualities? An Overview of the Current Media Narratives and Research Hypotheses. Arch. Sex. Behav. 2020, 49, 2765–2778. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xie, S.; Wang, P.; Wang, G.; Zhang, L.; Cao, X.; Wu, W.; Bian, Y.; Huang, F.; Luo, N.; et al. Factors Influencing Mental Health of Medical Workers During the COVID-19 Outbreak. Front. Public Health 2020, 8, 491. [Google Scholar] [CrossRef] [PubMed]
- Güzel, A.; Döndü, A. Changes in sexual functions and habits of healthcare workers during the ongoing COVID-19 outbreak: A cross-sectional survey study. Ir. J. Med. Sci. 2021. [Google Scholar] [CrossRef]
- Culha, M.G.; Demir, O.; Sahin, O.; Altunrende, F. Sexual attitudes of healthcare professionals during the COVID-19 outbreak. Int. J. Impot. Res. 2021, 33, 102–109. [Google Scholar] [CrossRef]
- Nowak, B.M.; Miedziarek, C.; Pełczyński, S.; Rzymski, P. Misinformation, Fears and Adherence to Preventive Measures during the Early Phase of COVID-19 Pandemic: A Cross-Sectional Study in Poland. Int. J. Environ. Res. Public Health 2021, 18, 12266. [Google Scholar] [CrossRef] [PubMed]
- Idzik, A.; Leńczuk-Gruba, A.; Kobos, E.; Pietrzak, M.; Dziedzic, B. Loneliness and Depression among Women in Poland during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 10698. [Google Scholar] [CrossRef]
- Carrington, A.E. NYC Health Department Offers New Recommendations on Safe Sex during COVID. Available online: https://abcnews.go.com/Health/york-city-health-department-offers-recommendations-safe-sex/story?id=71184094 (accessed on 20 September 2021).
- Hensel, D.J.; Rosenberg, M.; Luetke, M.; Fu, T.-C.; Herbenick, D. Changes in Solo and Partnered Sexual Behaviors during the COVID-19 Pandemic: Findings from a U.S. Probability Survey. medRxiv 2020. [Google Scholar] [CrossRef]
- Duarte, M.; Pereira, H. The Impact of COVID-19 on Depressive Symptoms through the Lens of Sexual Orientation. Brain Sci. 2021, 11, 523. [Google Scholar] [CrossRef] [PubMed]
- El-Nimr, N.A.; Mamdouh, H.M.; Ramadan, A.; El Saeh, H.M.; Shata, Z.N. Intimate partner violence among Arab women before and during the COVID-19 lockdown. J. Egypt Public Health Assoc. 2021, 96, 15. [Google Scholar] [CrossRef]
- Banerjee, D.; Vargas, S.E.; Guthrie, K.M.; Wickham, B.M.; Allahua, M.; Whittenhall, M.E.; Palmisciano, A.J.; Ventetuolo, C.E. Sexual health and health-related quality of life among women with pulmonary arterial hypertension. Pulm. Circ. 2018, 8, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Leblanc, N.M.; Alexander, K.; Carter, S.; Crean, H.; Ingram, L.; Kobie, J.; McMahon, J. The Effects of Trauma, Violence, and Stress on Sexual Health Outcomes Among Female Clinic Clients in a Small Northeastern U.S. Urban Center. Womens Health Rep. (New Rochelle) 2020, 1, 132–142. [Google Scholar] [CrossRef] [PubMed]
- Ilgen, O.; Kurt, S.; Aydin, C.; Bilen, E.; Kula, H. COVID-19 pandemic effect on female sexual function. Ginekol. Pol. 2021, 92, 856–859. [Google Scholar] [CrossRef] [PubMed]
- Szuster, E.; Kostrzewska, P.; Pawlikowska, A.; Mandera, A.; Biernikiewicz, M.; Kałka, D. Mental and Sexual Health of Polish Women of Reproductive Age During the COVID-19 Pandemic-An Online Survey. Sex. Med. 2021, 9, 100367. [Google Scholar] [CrossRef] [PubMed]
- Rosen, R.; Brown, C.; Heiman, J.; Leiblum, S.; Meston, C.; Shabsigh, R.; Ferguson, D.; D’Agostino, R., Jr. The Female Sexual Function Index (FSFI): A multidimensional self-report instrument for the assessment of female sexual function. J. Sex. Marital Ther. 2000, 26, 191–208. [Google Scholar] [CrossRef] [PubMed]
- Nowosielski, K.; Wróbel, B.; Sioma-Markowska, U.; Poręba, R. Development and validation of the Polish version of the Female Sexual Function Index in the Polish population of females. J. Sex. Med. 2013, 10, 386–395. [Google Scholar] [CrossRef]
- Beck, A.T.; Guth, D.; Steer, R.A.; Ball, R. Screening for major depression disorders in medical inpatients with the Beck Depression Inventory for Primary Care. Behav. Res. Ther. 1997, 35, 785–791. [Google Scholar] [CrossRef]
- Wenham, C.; Smith, J.; Morgan, R. COVID-19: The gendered impacts of the outbreak. Lancet 2020, 395, 846–848. [Google Scholar] [CrossRef] [Green Version]
- Bartoszek, A.; Walkowiak, D.; Bartoszek, A.; Kardas, G. Mental Well-Being (Depression, Loneliness, Insomnia, Daily Life Fatigue) during COVID-19 Related Home-Confinement—A Study from Poland. Int. J. Environ. Res. Public Health 2020, 17, 7417. [Google Scholar] [CrossRef] [PubMed]
- Durankuş, F.; Aksu, E. Effects of the COVID-19 pandemic on anxiety and depressive symptoms in pregnant women: A preliminary study. J. Matern. Fetal Neonatal Med. 2020, 35, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Schuch, F.B.; Bulzing, R.A.; Meyer, J.; Vancampfort, D.; Firth, J.; Stubbs, B.; Grabovac, I.; Willeit, P.; Tavares, V.D.O.; Calegaro, V.C.; et al. Associations of moderate to vigorous physical activity and sedentary behavior with depressive and anxiety symptoms in self-isolating people during the COVID-19 pandemic: A cross-sectional survey in Brazil. Psychiatry Res. 2020, 292, 113339. [Google Scholar] [CrossRef] [PubMed]
- Bhambhvani, H.P.; Chen, T.; Kasman, A.M.; Wilson-King, G.; Enemchukwu, E.; Eisenberg, M.L. Female Sexual Function During the COVID-19 Pandemic in the United States. Sex. Med. 2021, 9, 100355. [Google Scholar] [CrossRef]
- Fuchs, A.; Matonóg, A.; Pilarska, J.; Sieradzka, P.; Szul, M.; Czuba, B.; Drosdzol-Cop, A. The Impact of COVID-19 on Female Sexual Health. Int. J. Environ. Res. Public Health 2020, 17, 7152. [Google Scholar] [CrossRef] [PubMed]
- Hall, K.S.; Kusunoki, Y.; Gatny, H.; Barber, J. Stress symptoms and frequency of sexual intercourse among young women. J. Sex. Med. 2014, 11, 1982–1990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuksel, B.; Ozgor, F. Effect of the COVID-19 pandemic on female sexual behavior. Int. J. Gynaecol. Obstet. 2020, 150, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kühn, K.U.; Bender, S.; Erfurth, A.; Gastpar, M.; Murafi, A.; Rothermundt, M.; Signerski, J.; Sträter, B.; Teusch, L.; et al. Sexual impairment in psychiatric inpatients: Focus on depression. Pharmacopsychiatry 2007, 40, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Tartof, S.Y.; Slezak, J.M.; Fischer, H.; Hong, V.; Ackerson, B.K.; Ranasinghe, O.N.; Frankland, T.B.; Ogun, O.A.; Zamparo, J.M.; Gray, S.; et al. Effectiveness of mRNA BNT162b2 COVID-19 vaccine up to 6 months in a large integrated health system in the USA: A retrospective cohort study. Lancet 2021, 398, 1407–1416. [Google Scholar] [CrossRef]
- Madison, A.A.; Shrout, M.R.; Renna, M.E.; Kiecolt-Glaser, J.K. Psychological and Behavioral Predictors of Vaccine Efficacy: Considerations for COVID-19. Perspect. Psychol. Sci. 2021, 16, 191–203. [Google Scholar] [CrossRef] [PubMed]
- Brydon, L.; Walker, C.; Wawrzyniak, A.; Whitehead, D.; Okamura, H.; Yajima, J.; Tsuda, A.; Steptoe, A. Synergistic effects of psychological and immune stressors on inflammatory cytokine and sickness responses in humans. Brain Behav. Immun. 2009, 23, 217–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rusiecki, L.; Zdrojowy, R.; Gebala, J.; Sobieszczańska, M.; Smoliński, R.; Pilecki, W.; Piestrak, P.; Janocha, A.; Kawałko, W.; Womperski, M.; et al. The Influence of Socioeconomic Status on the Presence and Degree of Erectile Dysfunction in Men With Coronary Artery Disease—A Cross-Sectional Study. Am. J. Mens. Health 2019, 13, 1–10. [Google Scholar] [CrossRef] [Green Version]
| Variable | First Wave (N = 1644) | Second Wave (N = 720) | ||
|---|---|---|---|---|
| Frequency of sexual activity before/during pandemic | I wave p < 0.001 | II wave p = 0.028 | ||
| Several times a day | 27 (1.6%) | 36 (2.2%) | 17 (2.36%) | 19 (2.64%) |
| Every day | 93 (5.7%) | 84 (5.1%) | 32 (4.44%) | 37 (5.14%) |
| Several times a week | 749 (45.6%) | 579 (35.2%) | 326 (45.28%) | 260 (36.11%) |
| Once a week | 221 (13.4%) | 228 (13.9%) | 99 (13.75%) | 107 (14.86%) |
| Several times a month | 325 (19.8%) | 320 (19.5%) | 132 (18.34%) | 151 (20.97%) |
| Once a moth | 55 (3.3%) | 84 (5.1%) | 23 (3.19%) | 36 (5.00%) |
| Fewer than once a month | 174 (10.6%) | 313 (19.0%) | 91 (12.64%) | 110 (15.28%) |
| Libido level before/during pandemic | p < 0.001 | p < 0.001 | ||
| High | 521 (31.7%) | 504 (30.7%) | 234 (32.50%) | 228 (31.67%) |
| Moderate | 909 (55.3%) | 747 (45.4%) | 407 (56.53%) | 320 (44.44%) |
| Decreased libido | 214 (13.0%) | 393 (23.9%) | 79 (10.97%) | 172 (23.89%) |
| First Wave, N = 1644 | Second Wave, N = 720 | ||
|---|---|---|---|
| Total score | |||
| median | 11 | 12 | |
| range | 0–51 | 0–55 | |
| IQR | 5–18 | 7–20 | |
| minimal depression—0–11 scores | 858 (52.2%) | 328 (45.55%) | |
| mild depression—12–19 scores | 437 (26.6%) | 211 (29.31%) | p = 0.024 |
| moderate depression—20–25 scores | 183 (11.1%) | 91 (12.64%) | |
| severe depression—26–63 scores | 166 (10.1%) | 90 (12.50%) | |
| Domain | Score, Mean ± SD | Range | ||
|---|---|---|---|---|
| I Wave | II Wave | I Wave | II Wave | |
| Desire | 4.16 ± 1.17 | 4.05 ± 1.19 | 1.2–6 | 1.2–6 |
| Arousal | 4.60 ± 1.52 | 4.54 ± 1.49 | 0–6 | 0–6 |
| Lubrication | 4.90± 1.60 | 4.88± 1.58 | 0–6 | 0–6 |
| Orgasm | 4.32 ± 1.69 | 4.17 ± 1.73 | 0–6 | 0–6 |
| Satisfaction | 4.53 ± 1.55 | 4.53 ± 1.55 | 0–6 | 0–6 |
| Pain | 4.49 ± 1.75 | 4.48 ± 1.74 | 0–6 | 0–6 |
| Overall score | 27.01 ± 7.61 | 26.38 ± 7.76 | 2–36 | 1.2–36 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szuster, E.; Kostrzewska, P.; Pawlikowska, A.; Mandera, A.; Biernikiewicz, M.; Sobieszczańska, M.; Rożek-Piechura, K.; Jarząbek-Bielecka, G.; Rusiecka, A.; Kałka, D. Depressive and Sexual Disorders during the First and Second Wave of the COVID-19 Pandemic among Young Polish Women. Int. J. Environ. Res. Public Health 2022, 19, 1887. https://doi.org/10.3390/ijerph19031887
Szuster E, Kostrzewska P, Pawlikowska A, Mandera A, Biernikiewicz M, Sobieszczańska M, Rożek-Piechura K, Jarząbek-Bielecka G, Rusiecka A, Kałka D. Depressive and Sexual Disorders during the First and Second Wave of the COVID-19 Pandemic among Young Polish Women. International Journal of Environmental Research and Public Health. 2022; 19(3):1887. https://doi.org/10.3390/ijerph19031887
Chicago/Turabian StyleSzuster, Ewa, Paulina Kostrzewska, Anna Pawlikowska, Amanda Mandera, Małgorzata Biernikiewicz, Małgorzata Sobieszczańska, Krystyna Rożek-Piechura, Grażyna Jarząbek-Bielecka, Agnieszka Rusiecka, and Dariusz Kałka. 2022. "Depressive and Sexual Disorders during the First and Second Wave of the COVID-19 Pandemic among Young Polish Women" International Journal of Environmental Research and Public Health 19, no. 3: 1887. https://doi.org/10.3390/ijerph19031887
APA StyleSzuster, E., Kostrzewska, P., Pawlikowska, A., Mandera, A., Biernikiewicz, M., Sobieszczańska, M., Rożek-Piechura, K., Jarząbek-Bielecka, G., Rusiecka, A., & Kałka, D. (2022). Depressive and Sexual Disorders during the First and Second Wave of the COVID-19 Pandemic among Young Polish Women. International Journal of Environmental Research and Public Health, 19(3), 1887. https://doi.org/10.3390/ijerph19031887