
Changes in Active Behaviours, Physical Activity, Sedentary Time, and Physical Fitness in Chilean Parents during the COVID-19 Pandemic: A Retrospective Study



 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Characteristics and Ethical Considerations
2.2. Participants
2.3. Study Design and Primary Outcomes
2.4. Covariates
2.5. Statistical Analysis
3. Results
4. Discussion
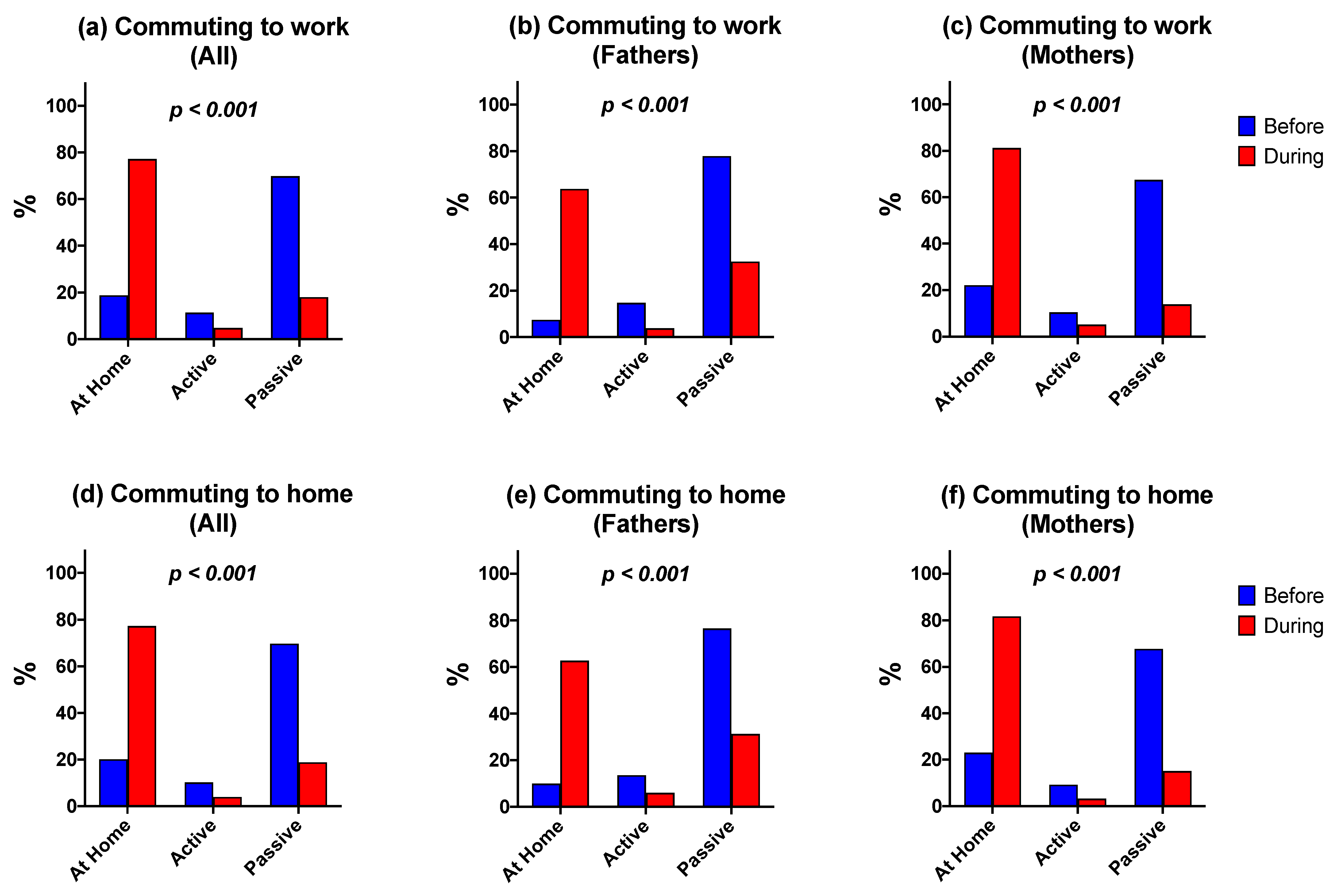
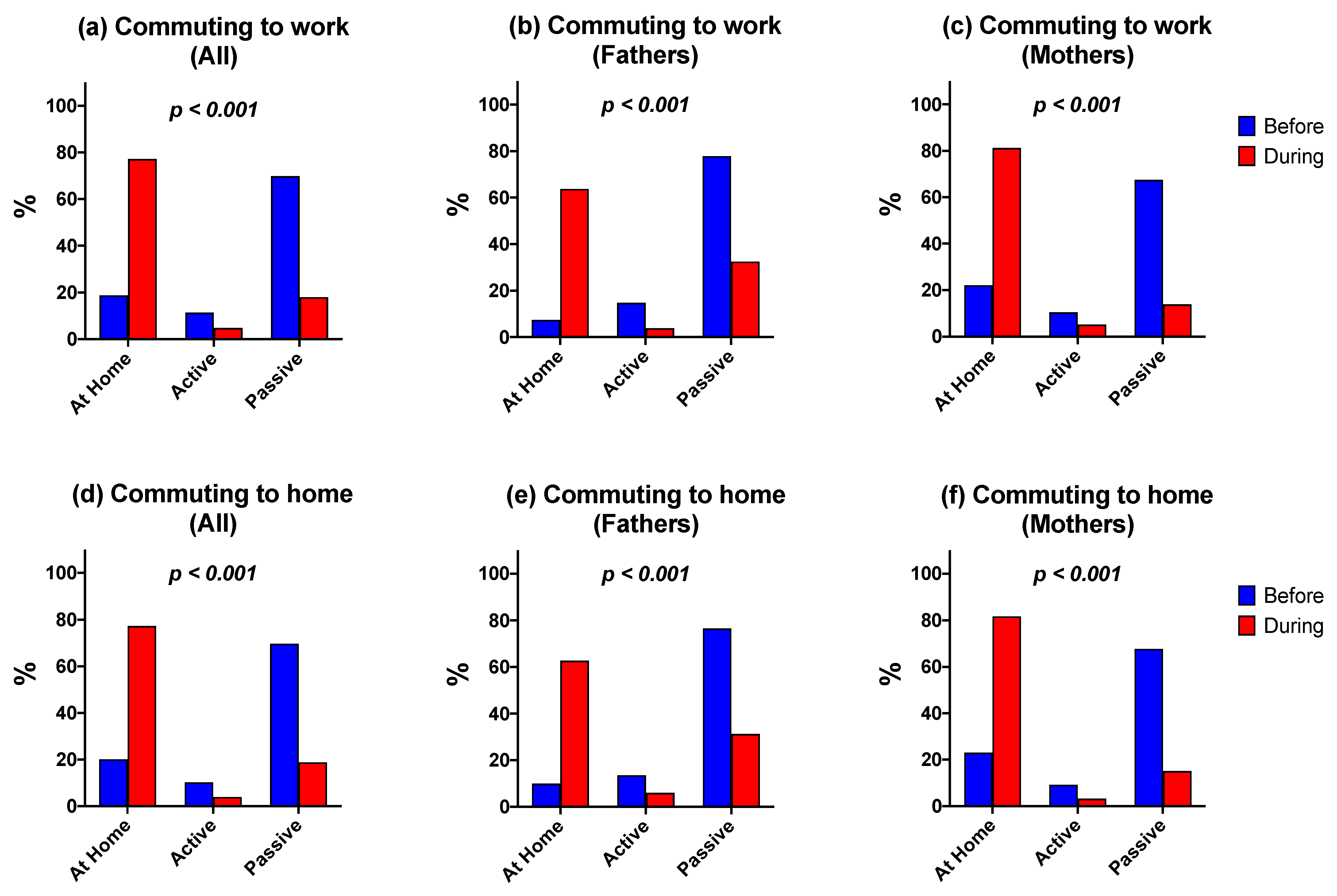
4.1. Active Commuting
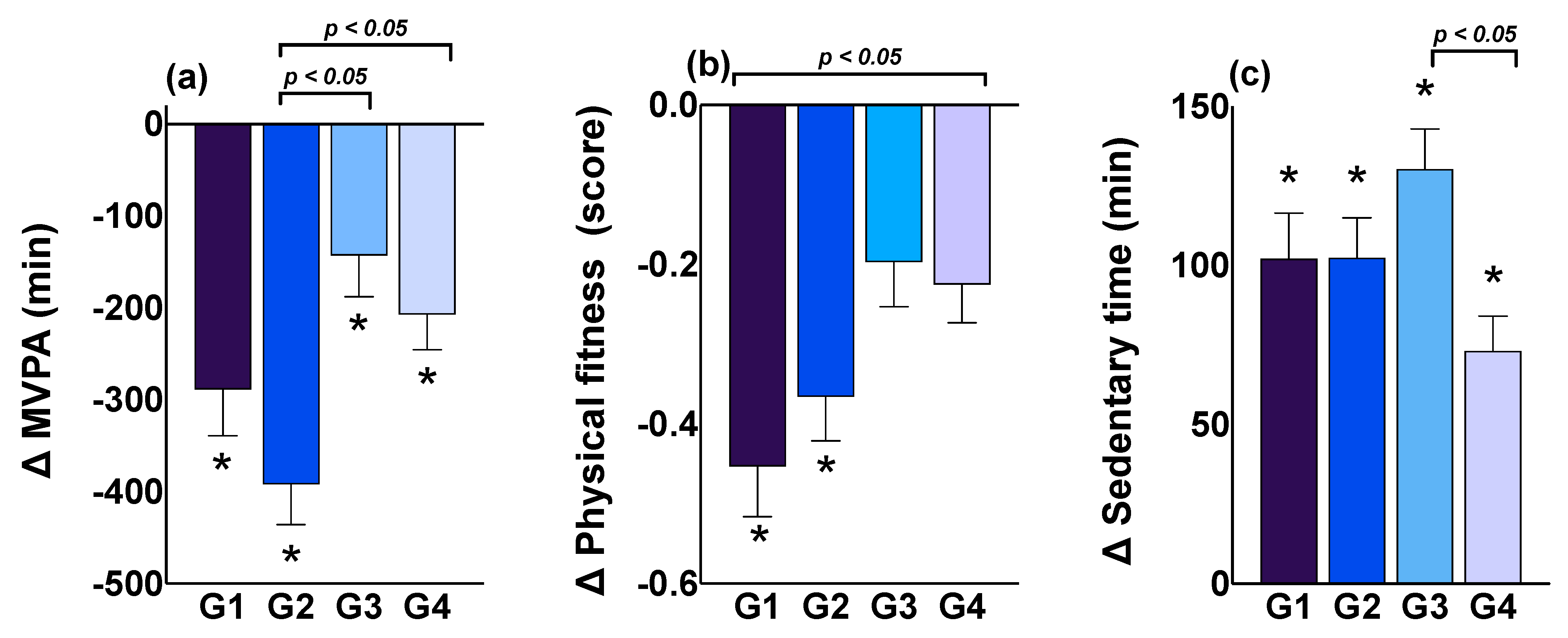
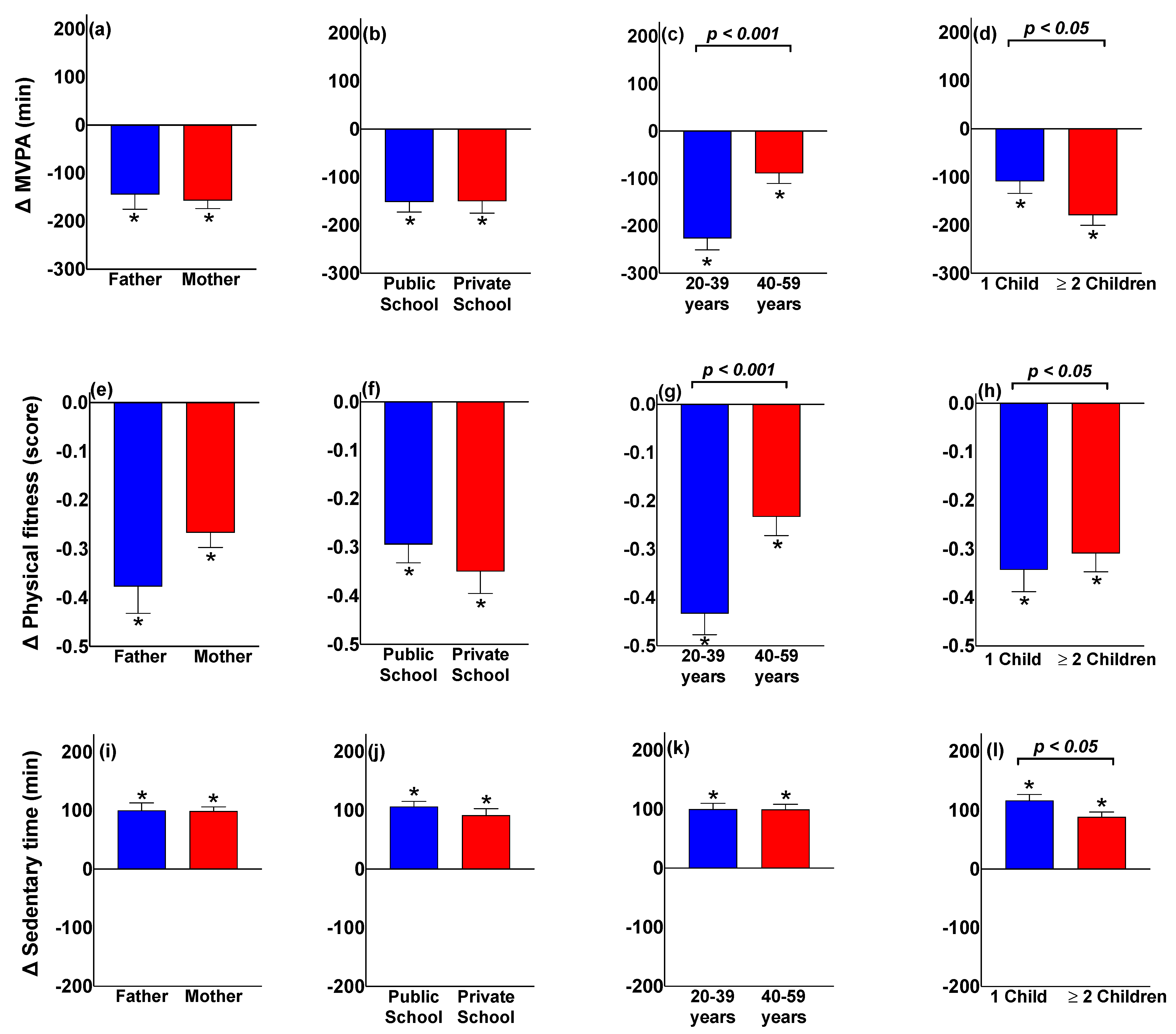
4.2. Physical Activity
4.3. Physical Fitness
4.4. Sedentary Time
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Coronavirus Disease (COVID-19) Situation Reports 51. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 1 November 2021).
- del Rio, C.; Collins, L.F.; Malani, P. Long-Term Health Consequences of COVID-19. JAMA 2020, 324, 1723–1724. [Google Scholar] [CrossRef] [PubMed]
- Pak, A.; Adegboye, O.A.; Adekunle, A.I.; Rahman, K.M.; McBryde, E.S.; Eisen, D.P. Economic Consequences of the COVID-19 Outbreak: The Need for Epidemic Preparedness. Front. Public Health 2020, 8, 241. [Google Scholar] [CrossRef] [PubMed]
- Belot, M.; Choi, S.; Tripodi, E.; Broek-Altenburg, E.; van den Jamison, J.C.; Papageorge, N.W. Unequal Consequences of Covid 19: Representative Evidence from Six Countries. Rev. Econ. Househ. 2021, 19, 769–783. [Google Scholar] [CrossRef] [PubMed]
- Gozzi, N.; Tizzoni, M.; Chinazzi, M.; Ferres, L.; Vespignani, A.; Perra, N. Estimating the Effect of Social Inequalities on the Mitigation of COVID-19 across Communities in Santiago de Chile. Nat. Commun. 2021, 12, 2429. [Google Scholar] [CrossRef]
- Wilder-Smith, A.; Freedman, D.O. Isolation, Quarantine, Social Distancing and Community Containment: Pivotal Role for Old-Style Public Health Measures in the Novel Coronavirus (2019-nCoV) Outbreak. J. Travel Med. 2020, 27. [Google Scholar] [CrossRef]
- Cusack, M. Individual, Social, and Environmental Factors Associated with Active Transportation Commuting during the COVID-19 Pandemic. J. Transp. Health 2021, 22, 101089. [Google Scholar] [CrossRef]
- Sañudo, B.; Fennell, C.; Sánchez-Oliver, A.J. Objectively-Assessed Physical Activity, Sedentary Behavior, Smartphone Use, and Sleep Patterns Pre- and during-COVID-19 Quarantine in Young Adults from Spain. Sustainability 2020, 12, 5890. [Google Scholar] [CrossRef]
- Imboden, M.T.; Harber, M.P.; Whaley, M.H.; Finch, W.H.; Bishop, D.L.; Kaminsky, L.A. Cardiorespiratory Fitness and Mortality in Healthy Men and Women. J. Am. Coll. Cardiol. 2018, 72, 2283–2292. [Google Scholar] [CrossRef]
- Lubans, D.; Richards, J.; Hillman, C.; Faulkner, G.; Beauchamp, M.; Nilsson, M.; Kelly, P.; Smith, J.; Raine, L.; Biddle, S. Physical Activity for Cognitive and Mental Health in Youth: A Systematic Review of Mechanisms. Pediatrics 2016, 138, e20161642. [Google Scholar] [CrossRef] [Green Version]
- Warburton, D.E.R.; Bredin, S.S.D. Health Benefits of Physical Activity: A Systematic Review of Current Systematic Reviews. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef]
- Celis-Morales, C.A.; Lyall, D.M.; Anderson, J.; Iliodromiti, S.; Fan, Y.; Ntuk, U.E.; Mackay, D.F.; Pell, J.P.; Sattar, N.; Gill, J.M.R. The Association between Physical Activity and Risk of Mortality Is Modulated by Grip Strength and Cardiorespiratory Fitness: Evidence from 498 135 UK-Biobank Participants. Eur. Heart J. 2017, 38, 116–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rezende, L.F.M.; de Lopes, M.R.; Rey-López, J.P.; Matsudo, V.K.R.; Luiz, O.d.C. Sedentary Behavior and Health Outcomes: An Overview of Systematic Reviews. PLoS ONE 2014, 9, e105620. [Google Scholar] [CrossRef] [PubMed]
- Caputo, E.L.; Reichert, F.F. Studies of Physical Activity and COVID-19 during the Pandemic: A Scoping Review. J. Phys. Act. Health 2020, 17, 1275–1284. [Google Scholar] [CrossRef] [PubMed]
- Radha, R.; Mahalakshmi, K.; Sathis Kumar, V.; Saravanakumar, A. E-Learning during Lockdown of COVID-19 Pandemic: A Global Perspective. Int. J. Control Autom. 2020, 13, 1088–1099. [Google Scholar]
- Carson, V.; Langlois, K.; Colley, R. Associations between Parent and Child Sedentary Behaviour and Physical Activity in Early Childhood. Health Rep. 2020, 31, 3–10. [Google Scholar] [CrossRef]
- Jelleyman, C.; McPhee, J.; Brussoni, M.; Bundy, A.; Duncan, S. A Cross-Sectional Description of Parental Perceptions and Practices Related to Risky Play and Independent Mobility in Children: The New Zealand State of Play Survey. Int. J. Environ. Res. Public Health 2019, 16, 262. [Google Scholar] [CrossRef] [Green Version]
- Wright, K.E.; Furzer, B.J.; Licari, M.K.; Dimmock, J.A.; Jackson, B. The Effect of Parental Logistic Support on Physical Activity in Children with, or at Risk of, Movement Difficulties. J. Sci. Med. Sport 2020, 23, 372–376. [Google Scholar] [CrossRef]
- McMinn, A.M.; Griffin, S.J.; Jones, A.P.; van Sluijs, E.M.F. Family and Home Influences on Children’s After-School and Weekend Physical Activity. Eur. J. Public Health 2013, 23, 805–810. [Google Scholar] [CrossRef] [Green Version]
- Martin, A.; Kelly, P.; Boyle, J.; Corlett, F.; Reilly, J.J. Contribution of Walking to School to Individual and Population Moderate-Vigorous Intensity Physical Activity: Systematic Review and Meta-Analysis. Pediatr. Exerc. Sci. 2016, 28, 353–363. [Google Scholar] [CrossRef]
- Prince, S.A.; Butler, G.P.; Rao, D.P.; Thompson, W. Evidence Synthesis Where Are Children and Adults Physically Active and Sedentary?—A Rapid Review of Location-Based Studies. Health Promot. Chron. Dis. Prev. Can. Res. Policy Pract. 2019, 39, 67–103. [Google Scholar] [CrossRef] [Green Version]
- Costa, F.F.; Silva, K.S.; Schmoelz, C.P.; Campos, V.C.; de Assis, M.A. A Longitudinal and Cross-Sectional Changes in Active Commuting to School among Brazilian Schoolchildren. Prev. Med. 2012, 55, 212–214. [Google Scholar] [CrossRef] [PubMed]
- Pavelka, J.; Sigmundová, D.; Hamřík, Z.; Kalman, M.; Sigmund, E.; Mathisen, F. Trends in Active Commuting to School among Czech Schoolchildren from 2006 to 2014. Cent. Eur. J. Public Health 2017, 25 (Suppl. S1), S21–S25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reimers, A.K.; Marzi, I.; Schmidt, S.C.; Niessner, C.; Oriwol, D.; Worth, A.; Woll, A. Trends in Active Commuting to School from 2003 to 2017 among Children and Adolescents from Germany: The MoMo Study. Eur. J. Public Health 2021, 31, 373–378. [Google Scholar] [CrossRef] [PubMed]
- McDonald, N.C. Active Transportation to School: Trends among US Schoolchildren, 1969–2001. Am. J. Prev. Med. 2007, 32, 509–516. [Google Scholar] [CrossRef] [PubMed]
- D’Haese, S.; Van Dyck, D.; De Bourdeaudhuij, I.; Deforche, B.; Cardon, G. The Association between Objective Walkability, Neighborhood Socio-Economic Status, and Physical Activity in Belgian Children. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 104. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Garcia, H.; Muñoz, A.P.; Crespo, J.L.C. Protective Parents, Democratic Parents and Support to Physical Activity and Sport. Cult. Cienc. Deporte 2019, 14, 51–59. [Google Scholar] [CrossRef]
- Rodriguez-Lopez, C.; Villa-Gonzalez, E.; Perez-Lopez, I.J.; Delgado-Fernandez, M.; Ruiz, J.R.; Chillon, P. Family Factors Influence Active Commuting to School in Spanish Children. Nutr. Hosp. 2013, 28, 756–763. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Segura-Díaz, J.M.; Rojas-Jiménez, Á.; Barranco-Ruiz, Y.; Murillo-Pardo, B.; Saucedo-Araujo, R.G.; Aranda-Balboa, M.J.; Herrador-Colmenero, M.; Villa-González, E.; Chillón, P. Feasibility and Reliability of a Questionnaire to Assess the Mode, Frequency, Distance and Time of Commuting to and from School: The PACO Study. Int. J. Environ. Res. Public Health 2020, 17, 5039. [Google Scholar] [CrossRef]
- Herrador-Colmenero, M.; Perez-Garcia, M.; Ruiz, J.R.; Chillon, P. Assessing Modes and Frequency of Commuting to School in Youngsters: A Systematic Review. Pediatr. Exerc. Sci. 2014, 26, 291–341. [Google Scholar] [CrossRef]
- Herrador-Colmenero, M.; Ruiz, J.R.; Ortega, F.B.; Segura-Jimenez, V.; Alvarez-Gallardo, I.C.; Camiletti-Moiron, D.; Estevez-Lopez, F.; Delgado-Fernandez, M.; Chillon, P. Reliability of the ALPHA Environmental Questionnaire and Its Association with Physical Activity in Female Fibromyalgia Patients: The al-Andalus Project. J. Sports Sci. 2015, 33, 850–862. [Google Scholar] [CrossRef] [PubMed]
- Escobar-Gomez, D.; Rodriguez-Rodriguez, F.; Villa-Gonzalez, E.; Esteban-Cornejo, I.; Chillon, P. Fiabilidad y Viabilidad de un Cuestionario Autorreportado Sobre el Modo Tiempo y Distancia de Desplazamiento en Niños y Adolescentes. Retos 2020, 37, 379–385. [Google Scholar]
- Bull, F.C.; Maslin, T.S.; Armstrong, T. Global Physical Activity Questionnaire (GPAQ): Nine Country Reliability and Validity Study. J. Phys. Act. Health 2009, 6, 790–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cleland, C.L.; Hunter, R.F.; Kee, F.; Cupples, M.E.; Sallis, J.F.; Tully, M.A. Validity of the Global Physical Activity Questionnaire (GPAQ) in Assessing Levels and Change in Moderate-Vigorous Physical Activity and Sedentary Behaviour. BMC Public Health 2014, 14, 1255. [Google Scholar] [CrossRef] [Green Version]
- Aguilar-Farias, N.; Leppe Zamora, J. Is a Single Question of the Global Physical Activity Questionnaire (GPAQ) Valid for Measuring Sedentary Behaviour in the Chilean Population? J. Sports Sci. 2017, 35, 1652–1657. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 Guidelines on Physical Activity and Sedentary Behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; España-Romero, V.; Vicente-Rodriguez, G.; Martínez-Gómez, D.; Manios, Y.; Béghin, L.; Molnar, D.; Widhalm, K.; Moreno, L.A.; et al. The International Fitness Scale (IFIS): Usefulness of Self-Reported Fitness in Youth. Int. J. Epidemiol. 2011, 40, 701–711. [Google Scholar] [CrossRef] [Green Version]
- Dang, H.-A.H.; Viet Nguyen, C. Gender Inequality during the COVID-19 Pandemic: Income, Expenditure, Savings, and Job loss. World Dev. 2021, 140, 105296. [Google Scholar] [CrossRef]
- Harris, M.; Branion-Calles, M. Changes in Commute Mode Attributed to COVID-19 Risk in Canadian National Survey Data. Transp. Find. 2021. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide Trends in Insufficient Physical Activity from 2001 to 2016: A Pooled Analysis of 358 Population-Based Surveys with 1·9 Million Participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Verdejo, R.; Suárez Reyes, M. Inactividad Física versus Sedentarismo: Análisis de la Encuesta Nacional de Salud de Chile 2016–2017. Rev. Med. Chile 2021, 149, 103–109. [Google Scholar] [CrossRef]
- Castañeda-Babarro, A.; Arbillaga-Etxarri, A.; Gutiérrez-Santamaría, B.; Coca, A. Physical Activity Change during COVID-19 Confinement. Int. J. Environ. Res. Public Health 2020, 17, 6878. [Google Scholar] [CrossRef] [PubMed]
- Roche, B.; Garchitorena, A.; Roiz, D. The Impact of Lockdown Strategies Targeting Age Groups on the Burden of COVID-19 in France. Epidemics 2020, 33, 100424. [Google Scholar] [CrossRef] [PubMed]
- Hansen, B.H.; Kolle, E.; Dyrstad, S.M.; Holme, I.; Anderssen, S.A. Accelerometer-Determined Physical Activity in Adults and Older People. Med. Sci. Sports Exerc. 2012, 44, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Telama, R. Tracking of Physical Activity from Childhood to Adulthood: A Review. Obes. Facts 2009, 2, 187–195. [Google Scholar] [CrossRef]
- Zimmermann-Sloutskis, D.; Wanner, M.; Zimmermann, E.; Martin, B.W. Physical Activity Levels and Determinants of Change in Young Adults: A Longitudinal Panel Study. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawkins, R.B.; Charles, E.J.; Mehaffey, J.H. Socio-Economic Status and COVID-19–Related Cases and Fatalities. Public Health 2020, 189, 129–134. [Google Scholar] [CrossRef]
- Tison, G.H.; Avram, R.; Kuhar, P.; Abreau, S.; Marcus, G.M.; Pletcher, M.J.; Olgin, J.E. Worldwide Effect of COVID-19 on Physical Activity: A Descriptive Study. Ann. Intern. Med. 2020, 173, 767–770. [Google Scholar] [CrossRef]
- Stekhoven, D.J.; Bühlmann, P. MissForest—Non-Parametric Missing Value Imputation for Mixed-Type Data. Bioinformatics 2020, 28, 112–118. [Google Scholar] [CrossRef] [Green Version]
- Zar, J. Biostatistical Analysis; Prentice-Hall: Hoboken, NJ, USA, 2010. [Google Scholar]
- Atalan, A. Is the Lockdown Important to Prevent the COVID-19 Pandemic? Effects on Psychology, Environment and Economy-Perspective. Ann. Med. Surg. 2020, 56, 38–42. [Google Scholar] [CrossRef]
- Brooks, J.H.M.; Tingay, R.; Varney, J. Social Distancing and COVID-19: An Unprecedented Active Transport Public Health Opportunity. Br. J. Sports Med. 2021, 55, 411–412. [Google Scholar] [CrossRef] [PubMed]
- Government UK. 2-Billion Package to Create New Era for Cycling and Walking. 2021. Available online: https://www.gov.uk/government/news/2-billion-package-to-create-new-era-for-cycling-and-walking (accessed on 17 December 2021).
- Baxter, J.; Gray, M.; Alexander, M.; Strazdins, L.; Bittman, M. Mothers and Fathers with Young Children: Paid Employment, Caring and Wellbeing. FaHCSIA Soc. Policy Res. Pap. 2007, 30. [Google Scholar] [CrossRef] [Green Version]
- Solomon-Moore, E.; Toumpakari, Z.; Sebire, S.J.; Thompson, J.L.; Lawlor, D.A.; Jago, R. Roles of Mothers and Fathers in Supporting Child Physical Activity: A Cross-Sectional Mixed-Methods Study. BMJ Open 2018, 8, e019732. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Rodríguez, F.; Huertas-Delgado, F.J.; Barranco-Ruiz, Y.; Aranda-Balboa, M.J.; Chillón, P. Are the Parents’ and Their Children’s Physical Activity and Mode of Commuting Associated? Analysis by Gender and Age Group. Int. J. Environ. Res. Public Health 2020, 17, 6864. [Google Scholar] [CrossRef] [PubMed]
- Lesser, I.A.; Nienhuis, C.P. The Impact of COVID-19 on Physical Activity Behavior and Well-Being of Canadians. Int. J. Environ. Res. Public Health 2020, 17, 3899. [Google Scholar] [CrossRef]
- Bassett, D.R.J.; Wyatt, H.R.; Thompson, H.; Peters, J.C.; Hill, J.O. Pedometer-Measured Physical Activity and Health Behaviors in U.S. Adults. Med. Sci. Sports Exerc. 2010, 42, 1819–1825. [Google Scholar] [CrossRef] [Green Version]
- Carson, V.; Adamo, K.; Rhodes, R.E. Associations of Parenthood with Physical Activity, Sedentary Behavior, and Sleep. Am. J. Health Behav. 2018, 42, 80–89. [Google Scholar] [CrossRef]
- Nelson, S.K.; Kushlev, K.; Lyubomirsky, S. The Pains and Pleasures of Parenting: When, Why, and How Is Parenthood Associated with More or Less Well-Being? Psychol. Bull. 2014, 140, 846–895. [Google Scholar] [CrossRef]
- Adamo, K.B.; Langlois, K.A.; Brett, K.E.; Colley, R.C. Young Children and Parental Physical Activity Levels: Findings from the Canadian Health Measures Survey. Am. J. Prev. Med. 2012, 43, 168–175. [Google Scholar] [CrossRef]
- Nomaguchi, K.M.; Bianchi, S.M. Exercise Time: Gender Differences in the Effects of Marriage, Parenthood, and Employment. J. Marriage Fam. 2004, 66, 413–430. [Google Scholar] [CrossRef]
- Abell, L.P.; Tanase, K.A.; Gilmore, M.L.; Winnicki, A.E.; Holmes, V.L.; Hartos, J.L. Do Physical Activity Levels Differ by Number of Children at Home in Women Aged 25–44 in the General Population? Women’s Health 2019, 15, 1745506519871186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rooney, S.; Webster, A.; Paul, L. Systematic Review of Changes and Recovery in Physical Function and Fitness After Severe Acute Respiratory Syndrome-Related Coronavirus Infection: Implications for COVID-19 Rehabilitation. Phys. Ther. 2020, 100, 1717–1729. [Google Scholar] [CrossRef] [PubMed]
- Pinho, C.S.; Caria, A.C.I.; Aras Júnior, R.; Pitanga, F.J.G. The Effects of the COVID-19 Pandemic on Levels of Physical Fitness. Rev. Assoc. Méd. Bras. 2020, 66, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Af Geijerstam, A.; Mehlig, K.; Börjesson, M.; Robertson, J.; Nyberg, J.; Adiels, M.; Rosengren, A.; Åberg, M.; Lissner, L. Fitness, Strength and Severity of COVID-19: A Prospective Register Study of 1 559 187 Swedish Conscripts. BMJ Open 2021, 11, e051316. [Google Scholar] [CrossRef] [PubMed]
- Steell, L.; Ho, F.K.; Sillars, A.; Petermann-Rocha, F.; Li, H.; Lyall, D.M.; Iliodromiti, S.; Welsh, P.; Anderson, J.; MacKay, D.F.; et al. Dose-Response Associations of Cardiorespiratory Fitness with All-Cause Mortality and Incidence and Mortality of Cancer and Cardiovascular and Respiratory Diseases: The UK Biobank Cohort Study. Br. J. Sports Med. 2019, 53, 1371–1378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saunders, T.J.; McIsaac, T.; Douillette, K.; Gaulton, N.; Hunter, S.; Rhodes, R.E.; Prince, S.A.; Carson, V.; Chaput, J.-P.; Chastin, S.; et al. Sedentary Behaviour and Health in Adults: An Overview of Systematic Reviews. Appl. Physiol. Nutr. Metab. 2020, 45 (Suppl. S2), S197–S217. [Google Scholar] [CrossRef]
- Fukushima, N.; Machida, M.; Kikuchi, H.; Amagasa, S.; Hayashi, T.; Odagiri, Y.; Takamiya, T.; Inoue, S. Associations of Working from Home with Occupational Physical Activity and Sedentary Behavior under the COVID-19 Pandemic. J. Occup. Health 2020, 63, e12212. [Google Scholar] [CrossRef]
- Alomari, M.A.; Khabour, O.F.; Alzoubi, K.H. Changes in Physical Activity and Sedentary Behavior Amid Confinement: The BKSQ-COVID-19 Project. Risk Manag. Healthc. Policy 2020, 13, 1757–1764. [Google Scholar] [CrossRef]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.; Lee, I.-M. Does Physical Activity Attenuate, or Even Eliminate, the Detrimental Association of Sitting Time with Mortality? A Harmonised Meta-Analysis of Data from More than 1 Million Men and Women. Lancet 2016, 388, 1302–1310. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Parental Sociodemographic | All (n = 380) | Fathers (n = 86) | Mothers (n = 294) | p-Value |
|---|---|---|---|---|
| Age (years) | 40.8 ± 6.9 | 41.3 ± 6.8 | 40.7 ± 6.9 | 0.462 |
| 20–39 years | 34.5 ± 3.9 | 35.2 ± 3.7 | 34.3 ± 3.9 | 0.229 |
| 40–59 years | 45.7 ± 4.2 | 45.9 ± 4.6 | 45.7 ± 4.1 | 0.697 |
| Children’s school type | ||||
| Public | 231 (60.8%) | 51 (59.3%) | 180 (61.2%) | 0.748 |
| Private | 149 (39.2%) | 35 (40.7%) | 114 (38.8%) | |
| Number of school-age children | ||||
| One | 164 (43.2%) | 35 (40.7%) | 129 (43.9%) | 0.600 |
| Two or more | 216 (56.8%) | 51 (59.3%) | 165 (56.1%) | |
| Employment situation | ||||
| Normal, I moved to my job normally | 49 (12.9%) | 21 (24.4%) | 28 (9.5%) | <0.001 |
| I have always worked in my home | 19 (5.0%) | 4 (4.7%) | 15 (5.1%) | |
| I stayed in my home unable to work | 37 (9.7%) | 7 (8.1%) | 30 (10.2%) | |
| I can work almost normally from my home | 116 (30.5%) | 29 (33.7%) | 87 (29.6%) | |
| I can work for a few moments in my home | 34 (8.9%) | 6 (7.0%) | 28 (9.5%) | |
| My job has been affected | 32 (8.4%) | 13 (15.1%) | 19 (6.5%) | |
| Fired or my source income was suspended | 25 (6.6%) | 6 (7.0%) | 19 (6.5%) | |
| My situation has not changed | 62 (16.3%) | 0 (0.0%) | 62 (21.1%) | |
| I have been with prenatal/postnatal rest | 6 (1.6%) | 0 (0.0%) | 6 (2.0%) | |
| MVPA (min/week) | 583.0 ± 686.9 | 618.2 ± 629.9 | 572.7 ± 703.8 | 0.589 |
| Physical fitness (score) | 3.1 ± 0.8 | 3.4 ± 0.8 | 3.0 ± 0.8 | <0.001 |
| Sedentary time (min/day) | 196.8 ± 155.4 | 220.9 ± 156.1 | 189.8 ± 154.7 | 0.102 |
| Parental Physical Characteristic | All (n = 380) | Fathers (n = 86) | Mothers (n = 294) | p-Value |
|---|---|---|---|---|
| Mode of commuting to work | ||||
| Stay home | 68 (18.8%) | 6 (7.4%) | 62 (22.1%) | |
| Active | 41 (11.4%) | 12 (14.8%) | 29 (10.4%) | 0.010 |
| Passive | 252 (69.8%) | 63 (77.8%) | 189 (67.5%) | |
| Mode of commuting to home | ||||
| Stay home | 73 (20.1%) | 8 (9.9%) | 65 (23.0%) | |
| Active | 37 (10.2%) | 11 (13.6%) | 26 (9.2%) | 0.026 |
| Passive | 253 (69.7%) | 62 (76.5%) | 191 (67.7%) | |
| MVPA (min/week) | ||||
| Public schools | 601.9 ± 723.0 | 619.3 ± 7 45.8 | 597.0 ± 718.5 | 0.847 |
| Private schools | 553.7 ± 628.0 | 616.7 ± 417.4 | 534.3 ± 680.1 | 0.499 |
| 20–39 years | 677.8 ± 792.3 | 763.4 ± 767.0 | 653.3 ± 800.6 | 0.458 |
| 40–59 years | 509.4 ± 583.8 | 508.6 ± 482.7 | 509.7 ± 612.0 | 0.991 |
| 1 child | 518.2 ± 544.6 | 734.8 ± 847.0 | 459.5 ± 413.3 | 0.008 |
| ≥2 children | 632.2 ± 775.4 | 538.2 ± 413.3 | 661.2 ± 855.9 | 0.323 |
| Physical fitness (score) | ||||
| Public schools | 3.0 ± 0.8 | 3.4 ± 0.6 | 3.0 ± 0.8 | <0.001 |
| Private schools | 3.3 ± 0.9 | 3.6 ± 0.9 | 3.2 ± 0.8 | 0.017 |
| 20–39 years | 3.2 ± 0.8 | 3.6 ± 0.7 | 3.1 ± 0.7 | <0.001 |
| 40–59 years | 3.1 ± 0.8 | 3.3 ± 0.8 | 3.0 ± 0.8 | 0.020 |
| 1 child | 3.1 ± 0.8 | 3.5 ± 0.6 | 3.0 ± 0.8 | <0.001 |
| ≥2 children | 3.1 ± 0.8 | 3.4 ± 0.8 | 3.1 ± 0.8 | 0.015 |
| Sedentary time (min/day) | ||||
| Public schools | 186.4 ± 149.4 | 197.2 ± 143.0 | 183.4 ± 151.4 | 0.560 |
| Private schools | 213.0 ± 163.5 | 255.5 ± 169.6 | 199.9 ± 160.0 | 0.078 |
| 20–39 years | 184.7 ± 137.3 | 178.7 ± 109.4 | 186.4 ± 144.7 | 0.764 |
| 40–59 years | 206.3 ± 167.7 | 252.8 ± 178.2 | 192.4 ± 162.5 | 0.027 |
| 1 child | 205.5 ± 161.0 | 235.2 ± 149.2 | 197.5 ± 163.6 | 0.219 |
| ≥2 children | 190.3 ± 151.0 | 211.1 ± 161.4 | 183.8 ± 147.6 | 0.260 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández-Jaña, S.; Escobar-Gómez, D.; Cristi-Montero, C.; Castro-Piñero, J.; Rodríguez-Rodríguez, F. Changes in Active Behaviours, Physical Activity, Sedentary Time, and Physical Fitness in Chilean Parents during the COVID-19 Pandemic: A Retrospective Study. Int. J. Environ. Res. Public Health 2022, 19, 1846. https://doi.org/10.3390/ijerph19031846
Hernández-Jaña S, Escobar-Gómez D, Cristi-Montero C, Castro-Piñero J, Rodríguez-Rodríguez F. Changes in Active Behaviours, Physical Activity, Sedentary Time, and Physical Fitness in Chilean Parents during the COVID-19 Pandemic: A Retrospective Study. International Journal of Environmental Research and Public Health. 2022; 19(3):1846. https://doi.org/10.3390/ijerph19031846
Chicago/Turabian StyleHernández-Jaña, Sam, Danica Escobar-Gómez, Carlos Cristi-Montero, José Castro-Piñero, and Fernando Rodríguez-Rodríguez. 2022. "Changes in Active Behaviours, Physical Activity, Sedentary Time, and Physical Fitness in Chilean Parents during the COVID-19 Pandemic: A Retrospective Study" International Journal of Environmental Research and Public Health 19, no. 3: 1846. https://doi.org/10.3390/ijerph19031846
APA StyleHernández-Jaña, S., Escobar-Gómez, D., Cristi-Montero, C., Castro-Piñero, J., & Rodríguez-Rodríguez, F. (2022). Changes in Active Behaviours, Physical Activity, Sedentary Time, and Physical Fitness in Chilean Parents during the COVID-19 Pandemic: A Retrospective Study. International Journal of Environmental Research and Public Health, 19(3), 1846. https://doi.org/10.3390/ijerph19031846