1. Introduction
Children in sub-Saharan Africa suffer from the simultaneous occurrence of multiple diseases. Disease co-occurrence is partly attributed to common risk factors such as poor sanitation and water quality, air pollution, and poor access to breast milk and nutrient-dense foods [
1,
2,
3,
4]. Several studies have shown that growth faltering is related to diarrheal morbidity in children under 5 years of age in low-income settings [
5,
6,
7,
8]. While evidence of associations between child growth retardation and acute respiratory infection is not conclusive [
5,
7], several studies have found a significant association between diarrhoea and the risk of ARI in children [
3,
9,
10]. The association is more pronounced in malnourished children as they are more susceptible to diarrhoea, and subsequent dehydration and micronutrient loss [
3,
11]. The combined effect weakens the immune system, further predisposing the child to more infections. Malnourishment in children leads to growth faltering (Stewart et al., 2013). An ecological analysis of the spatial co-occurrence of ART, diarrhoea, and stunting is important to public health policymakers, in that identifying and reducing common risk factors to these three conditions could result in a very significant improvement in child health.
Previous ecological studies on child illnesses in sub-Saharan Africa have mostly used univariate spatial statistics methods, even if multiple diseases were analysed [
1,
12,
13,
14,
15]. A few studies have been conducted to model multiple diseases in children using joint spatial models [
16,
17,
18,
19]. Joint spatial models are of both methodological and epidemiological importance, in that they avoid the specific problems of multiple testing and the identifiability issues in random effect parameter estimations [
20,
21,
22]. A widely applied spatial joint model is the shared-component model [
21], which allows for separation of the area-specific risks of each disease into the underlying spatial pattern, which is common to all diseases, and another, which is a disease-specific component to capture the difference of disease-spatial pattern from the spatial shared component. This spatial joint model was used here to assess the state-level co-occurrence of ARI, diarrhoea, and stunting among children aged under 5 years. A total of 61,579 children from the 2008, 2013, and 2018 Nigeria Demographic and Health Surveys (DHSs) were used. We analysed each of the three survey datasets, as well as the pooled data, using Bayesian inference employing the integrated nested Laplace approximation approach (INLA) [
23]. To the best of our knowledge, no other study has examined the trends over time in spatial variations of some of the common diseases among children under the ages of five years in sub-Saharan Africa.
3. Results
Table 2 shows the distribution of the characteristics of the children studied. A total of 61,579 children under 5 years of age were included, of which 23,851, 27,524, and 10, 204 were from 2008, 2013, and 2018, respectively. Out of the 61,579 children considered, 2923 had ARI, 6675 had diarrhoea, and 8940 were stunted. A total of 1013 had ARI and diarrhoea, 468 had ARI and stunting, 1054 had diarrhoea and were stunted, while 173 suffered from all of the illnesses. A larger percentage (68%) of children was from a rural settlement, while 46% of their mothers had no education.
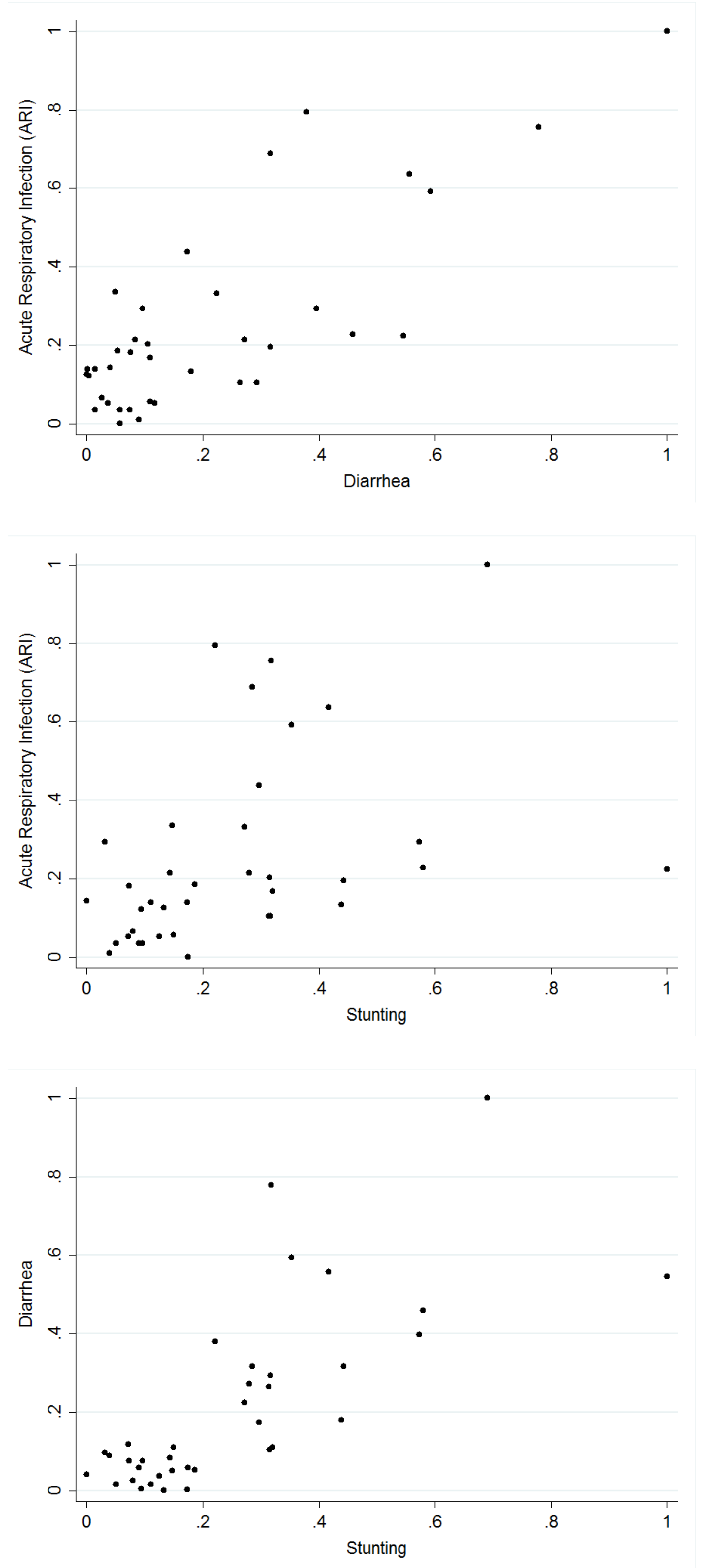
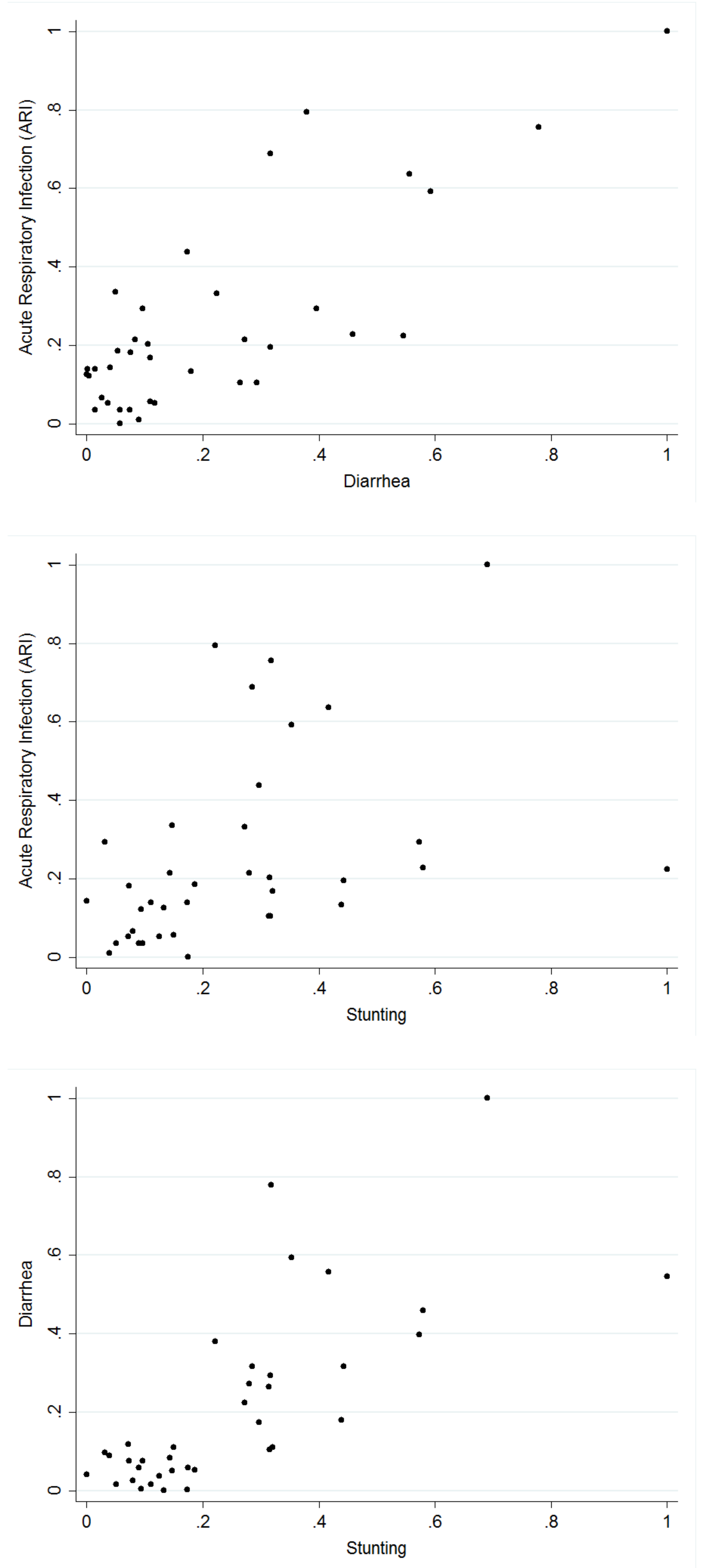
Table 3 presents the tetrachoric correlation coefficients for each pair of the three health indicators computed. The tetrachoric correlation measures were in agreement with the binary outcomes. A strong correlation exists between ARI and diarrhoea. In the case of ARI and stunting, and diarrhoea and stunting, the correlation at the national level was weak, but when estimated for each state (estimates not presented), the results showed significant relationships in some of the states. Thus, correlation estimates at the national level concealed information on possible local variations.
Figure 1 shows, for each pair of the diseases, the empirical correlation for the proportion of children who suffered from the diseases in the different states of Nigeria.
Table 4,
Table 5 and
Table 6 present the odds ratios for the fixed effects for each of the diseases from the surveys carried out in 2008, 2013, and 2018, respectively. Children from urban settlements in 2013 were less likely to be stunted. In 2018, children from urban settlements were more likely to have diarrhoea. Children whose mothers attained at least a primary level of education were less likely to have any of the diseases in all the survey years. This was also true for children from rich households and female children. Estimates also show that children between the age of 12 to 23 months were more likely to have diarrhoea in all the survey years, and as the mothers’ age increased, the likelihood of any of the diseases decreased.
Table 7 presents the odds ratio for the fixed linear effects for each of the diseases considered, including the 95% credible intervals using the combined dataset. The findings show that children who were between 12 to 23 months were less likely to suffer from ARI and stunting, but more likely to suffer from diarrhoea, while children who were 24 months or older had a significantly lower likelihood of suffering from any of the diseases. Children whose mothers attained at least a primary level of education were less likely to have suffered from the diseases, although the estimate was not significant for ARI. Surprisingly, children from an urban settlement were more likely to have diarrhoea when compared with children from a rural settlement. Estimates for ARI and stunting based on settlement (urban or rural) were not significant. However, children from poorer households and above were less like to have any of the diseases, and the estimates were significant. Female children had a lower likelihood of having any of the diseases. As mothers’ age increased, the children were less likely to contract any of the illnesses. In addition, the results show that compared with 2008, the odds for any of the diseases were significantly lower in 2013, but for 2018, the estimates were only lower for ARI and diarrhoea.
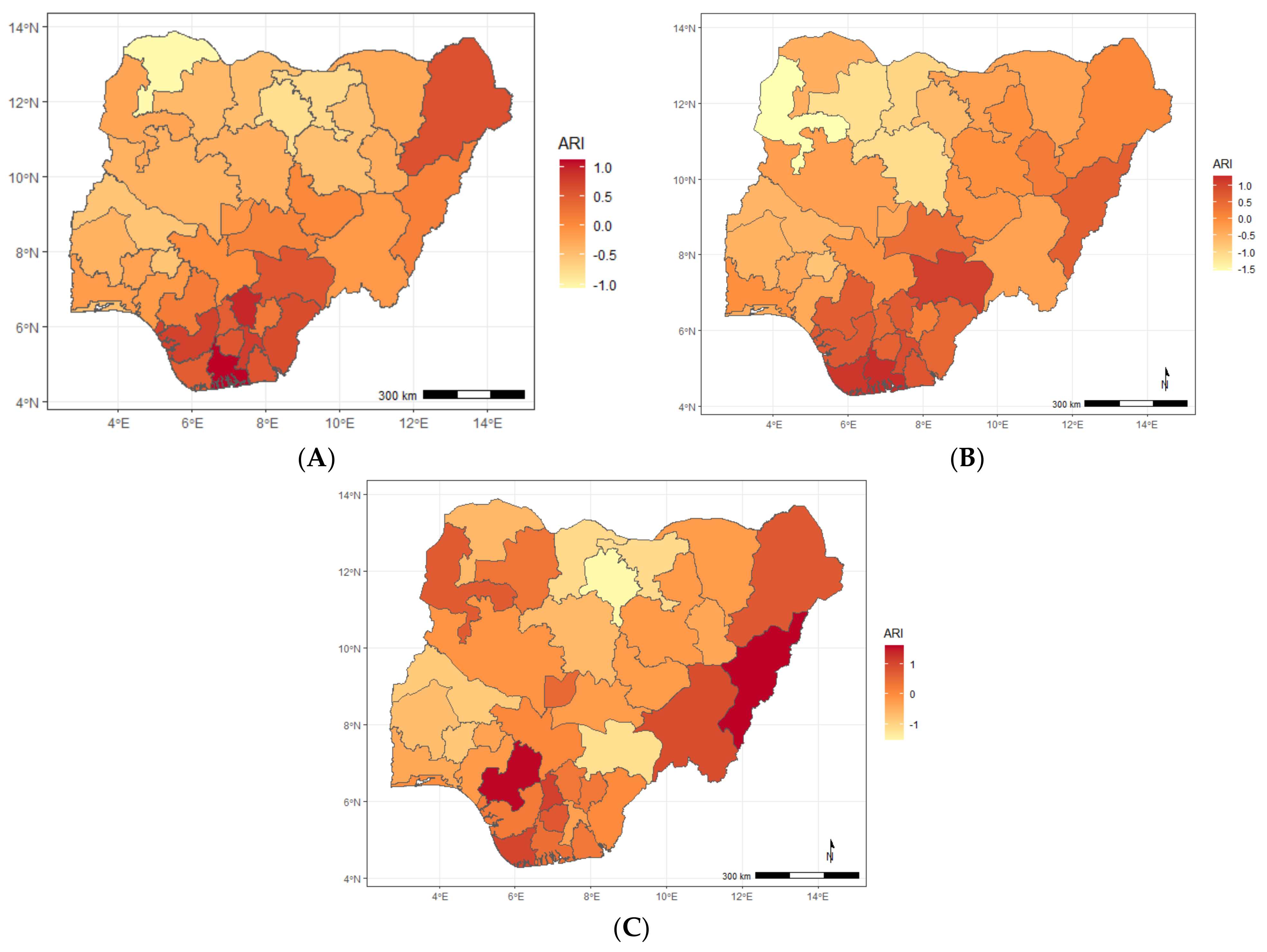
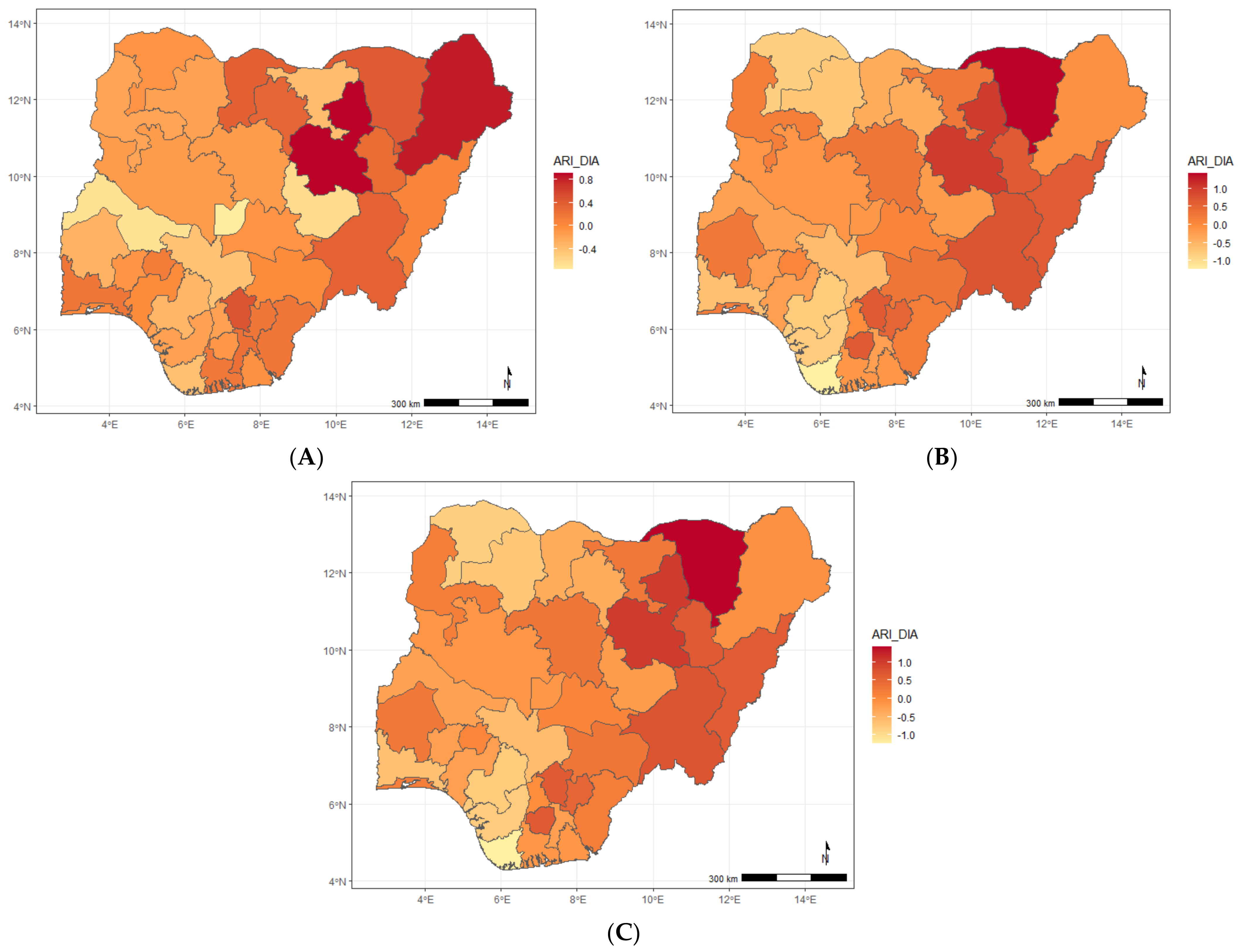
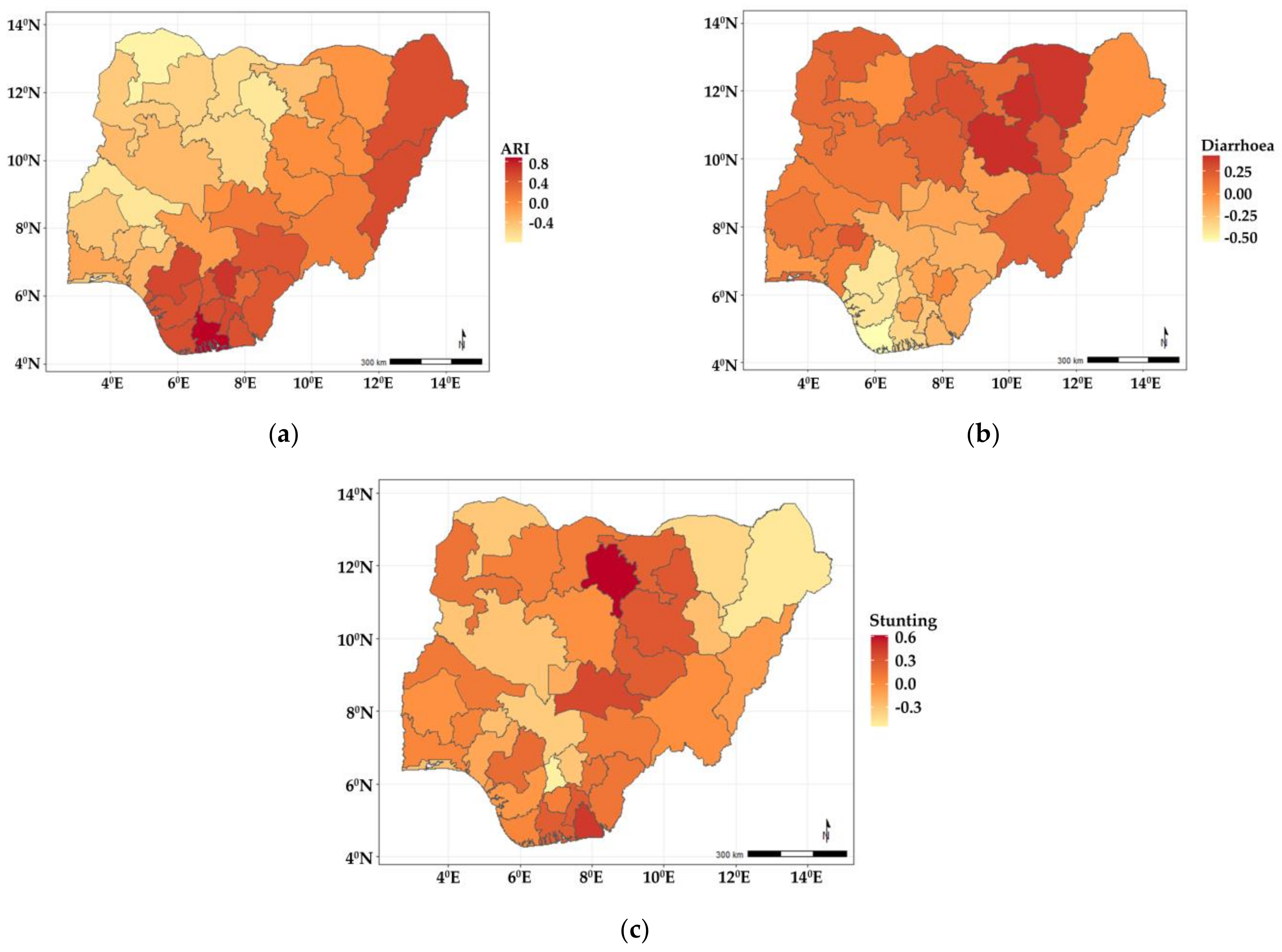
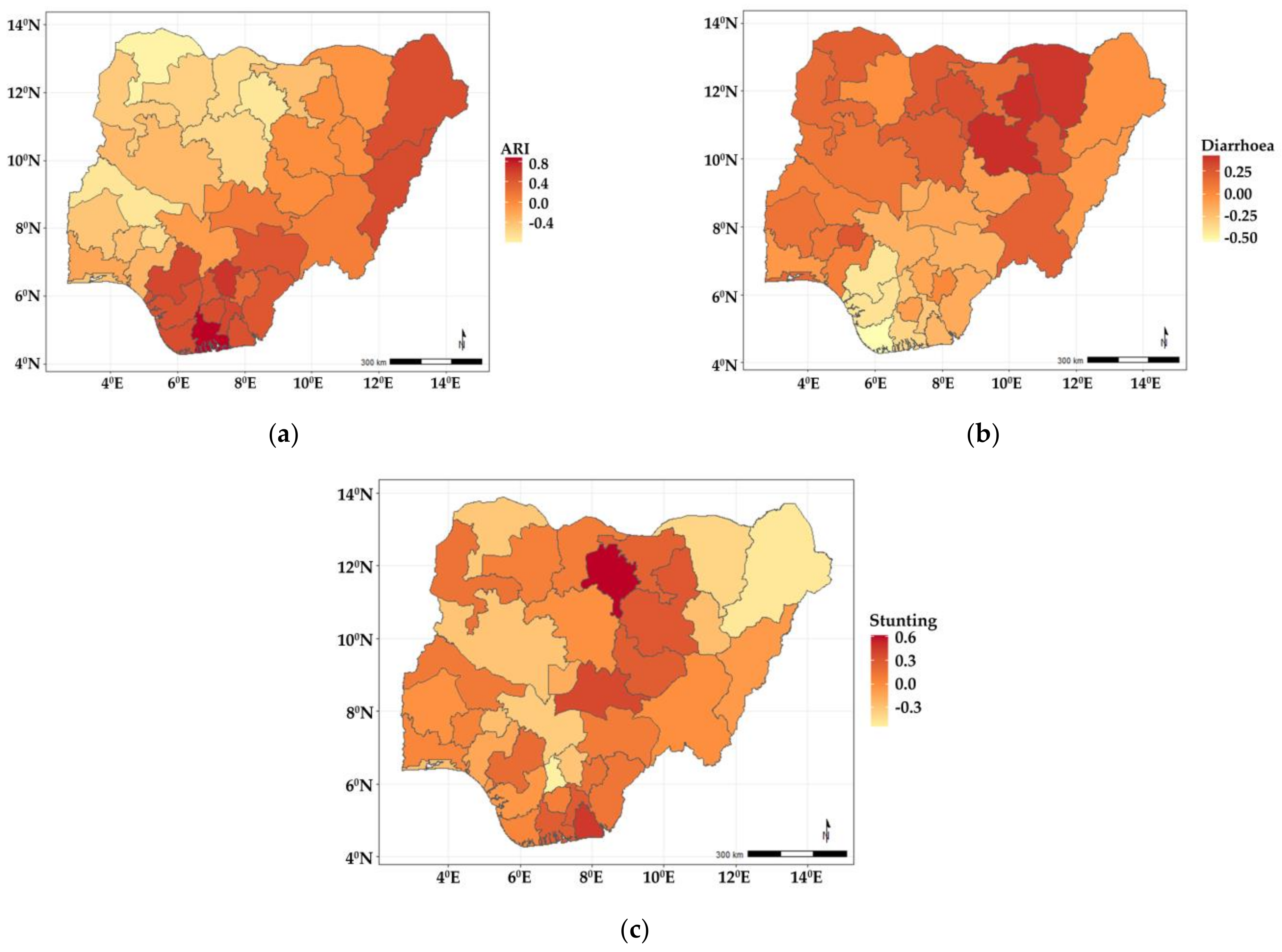
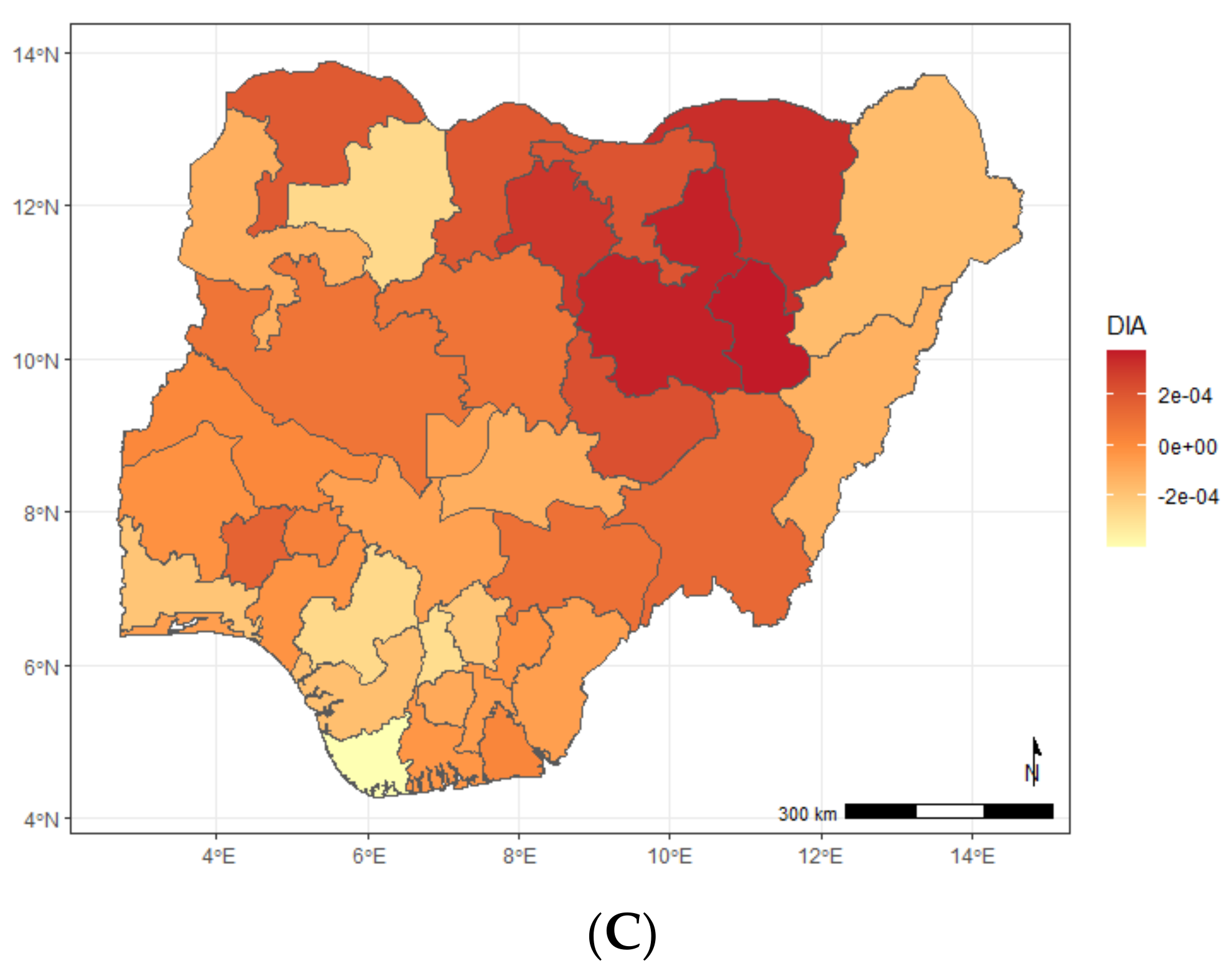
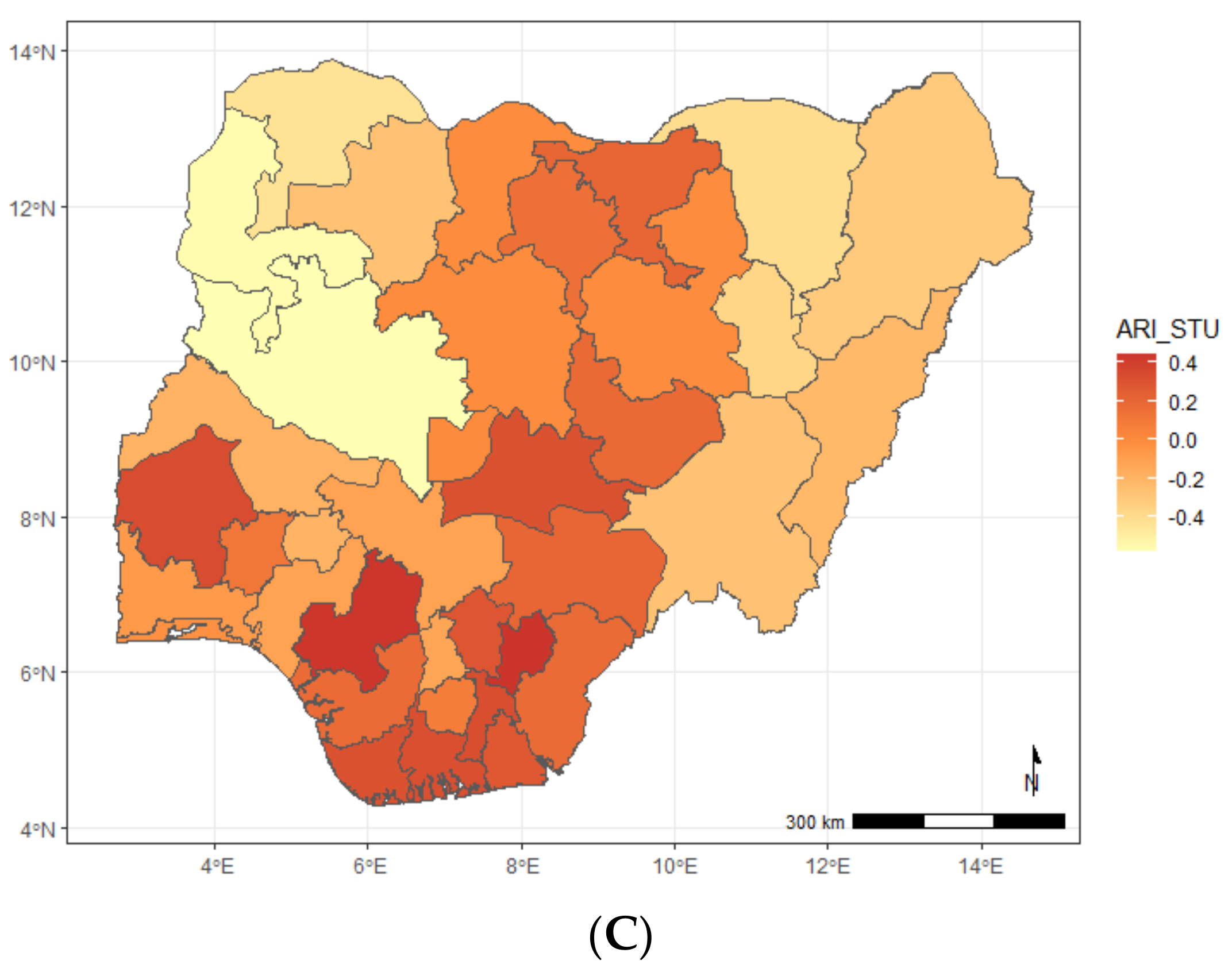
The findings from the spatial effects for the specific diseases as estimated from the shared component model are presented in
Figure 2. The maps reveal that whereas diarrhoea has higher odds of occurring among children living in the northern states, ARI is more widespread in the southern fringe. Specifically, children residing in Benue, Enugu, Anambra, Ebonyi, Imo, Abia, Cross River, Akwa Ibom, Rivers, Bayelsa, Delta, Edo, and two states from the northern fringe (Borno and Adamawa) were more likely to have suffered more from ARI, but were less likely in the states belonging to north and southwestern regions of the country. In the case of diarrhoea (
Figure 2b), the odds were higher among children living in Yobe, Gombe, and Ekiti, but less likely for those in Edo, Delta, and Bayelsa, while for stunting (
Figure 2c), the odds were higher in some neighbouring northern states—Kano, Plateau, Jigawa, Bauchi, Nasarawa, and two southern states (Akwa Ibom and Edo).
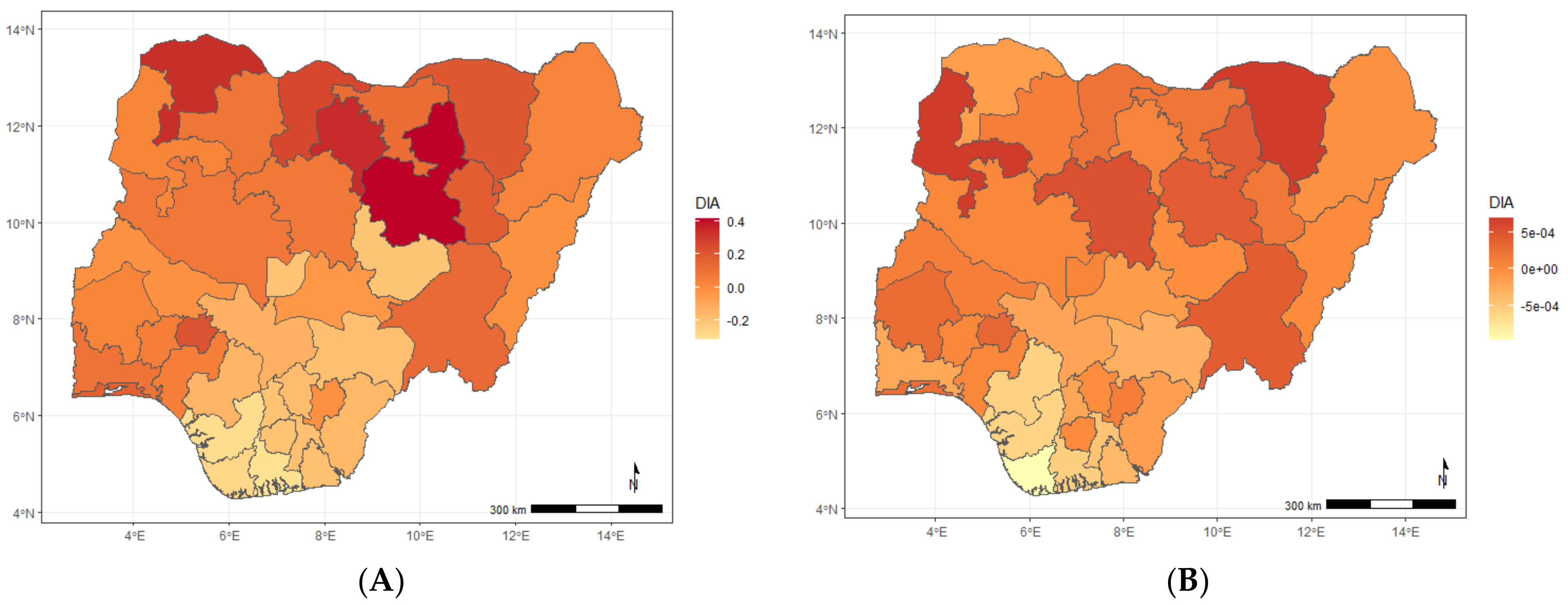
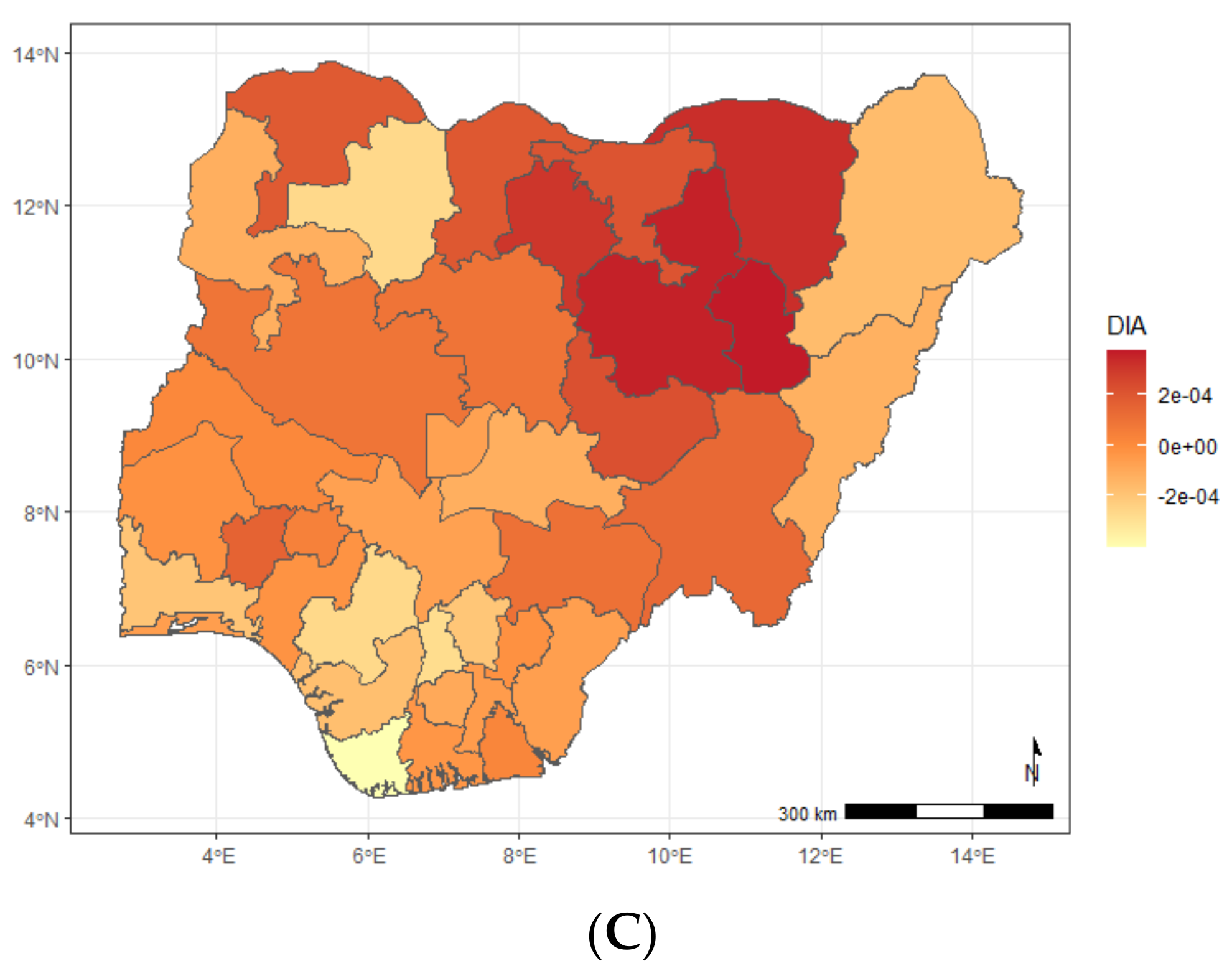
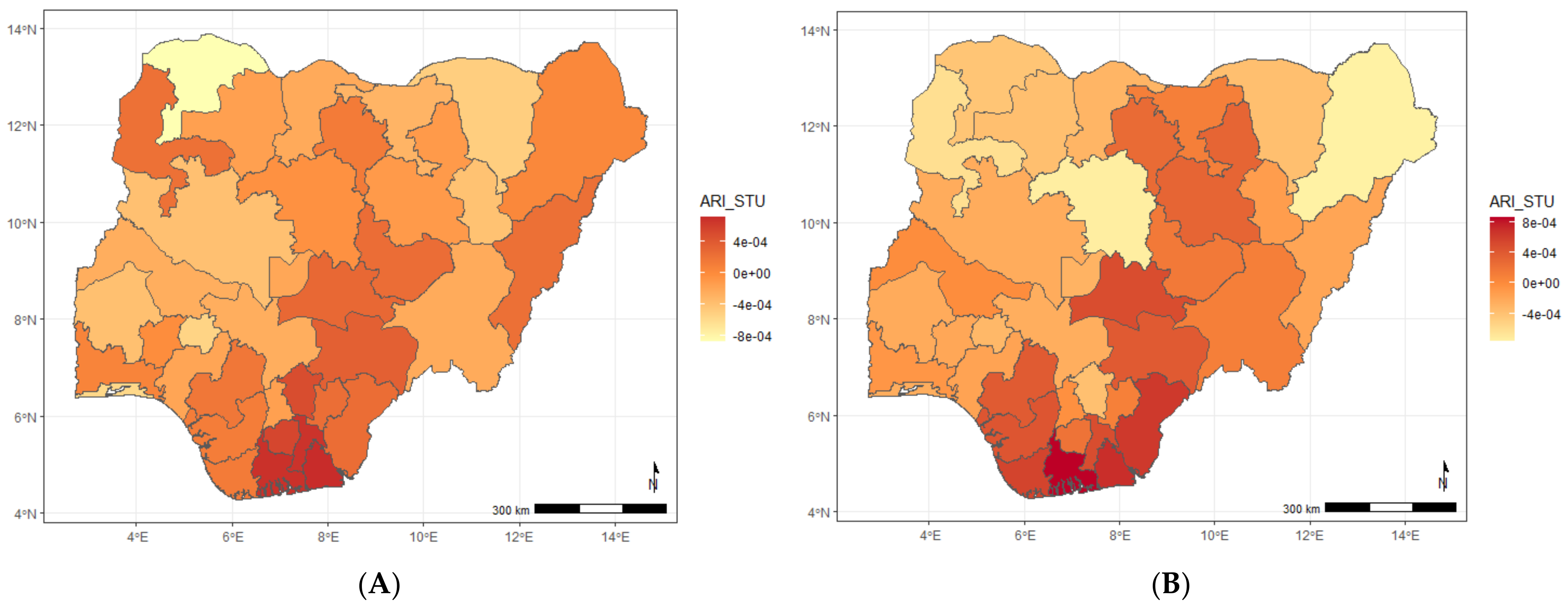
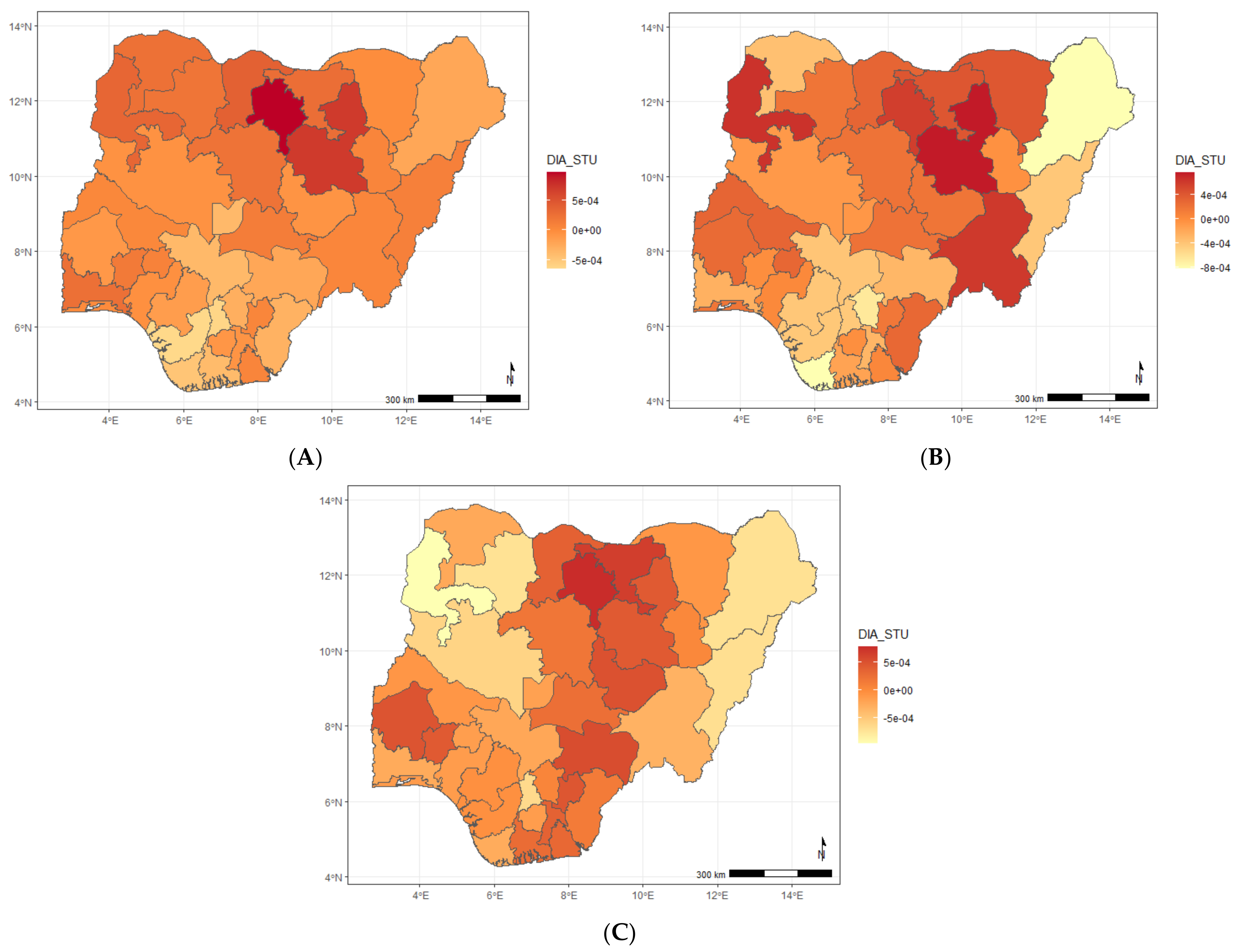
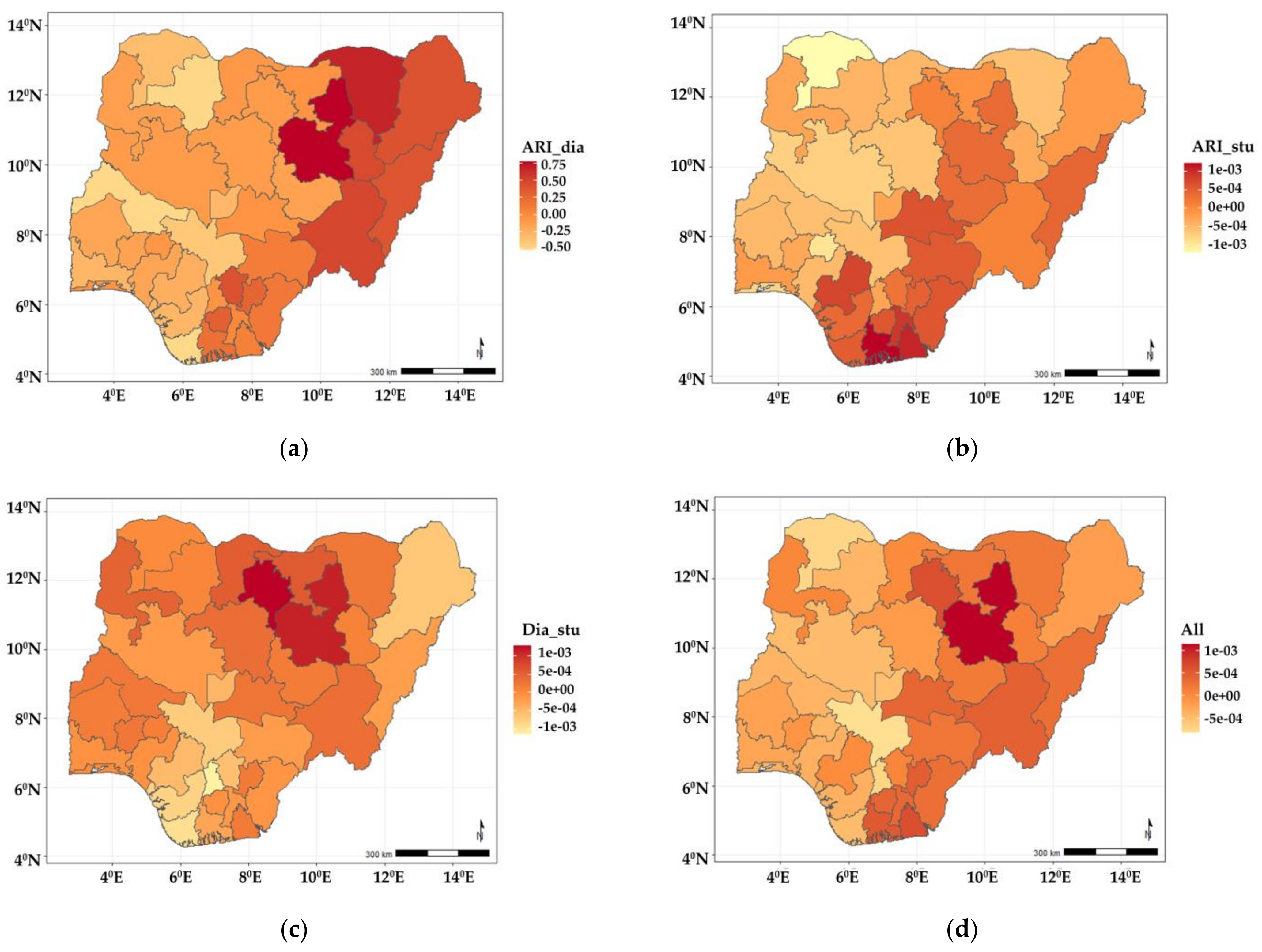
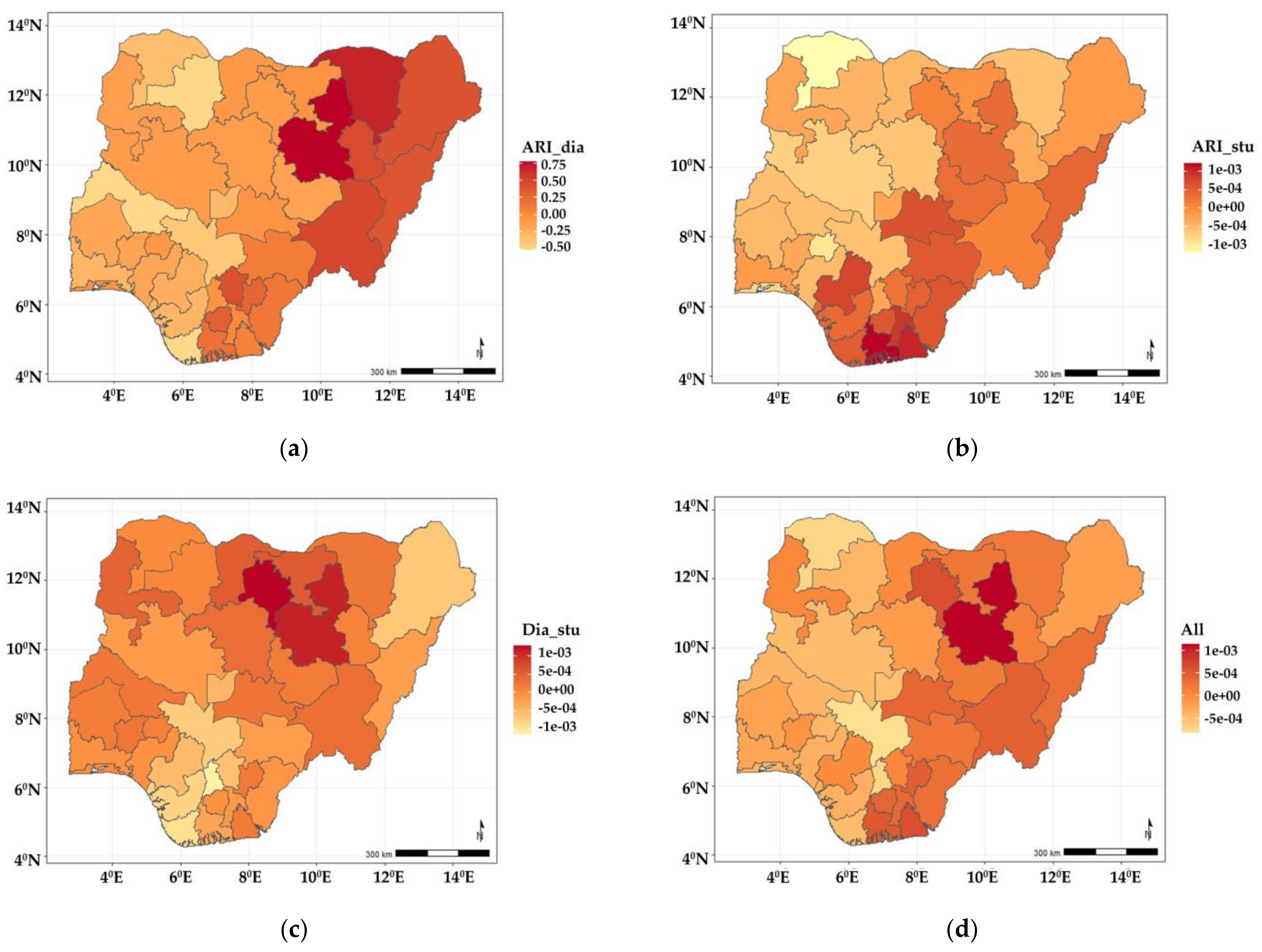
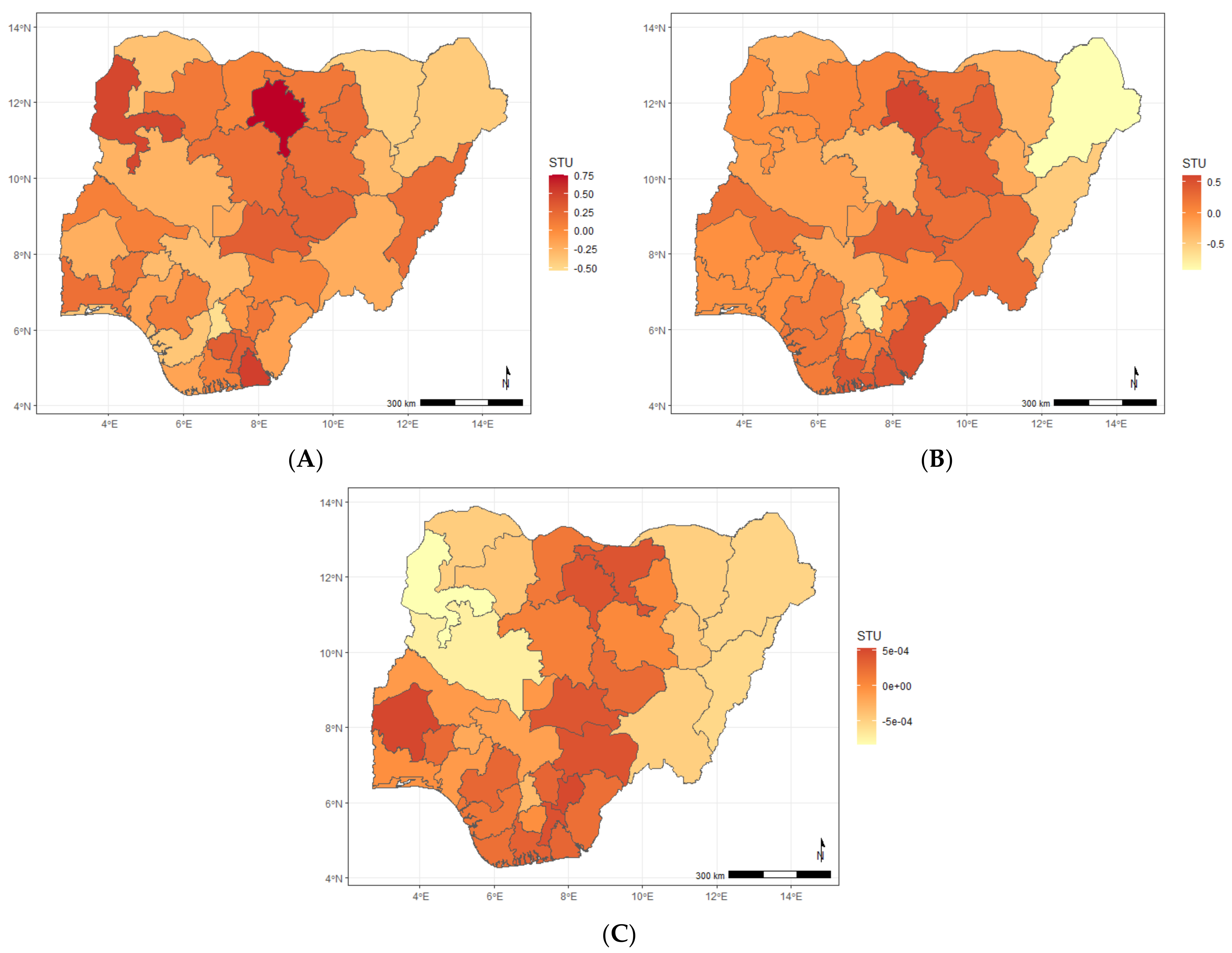
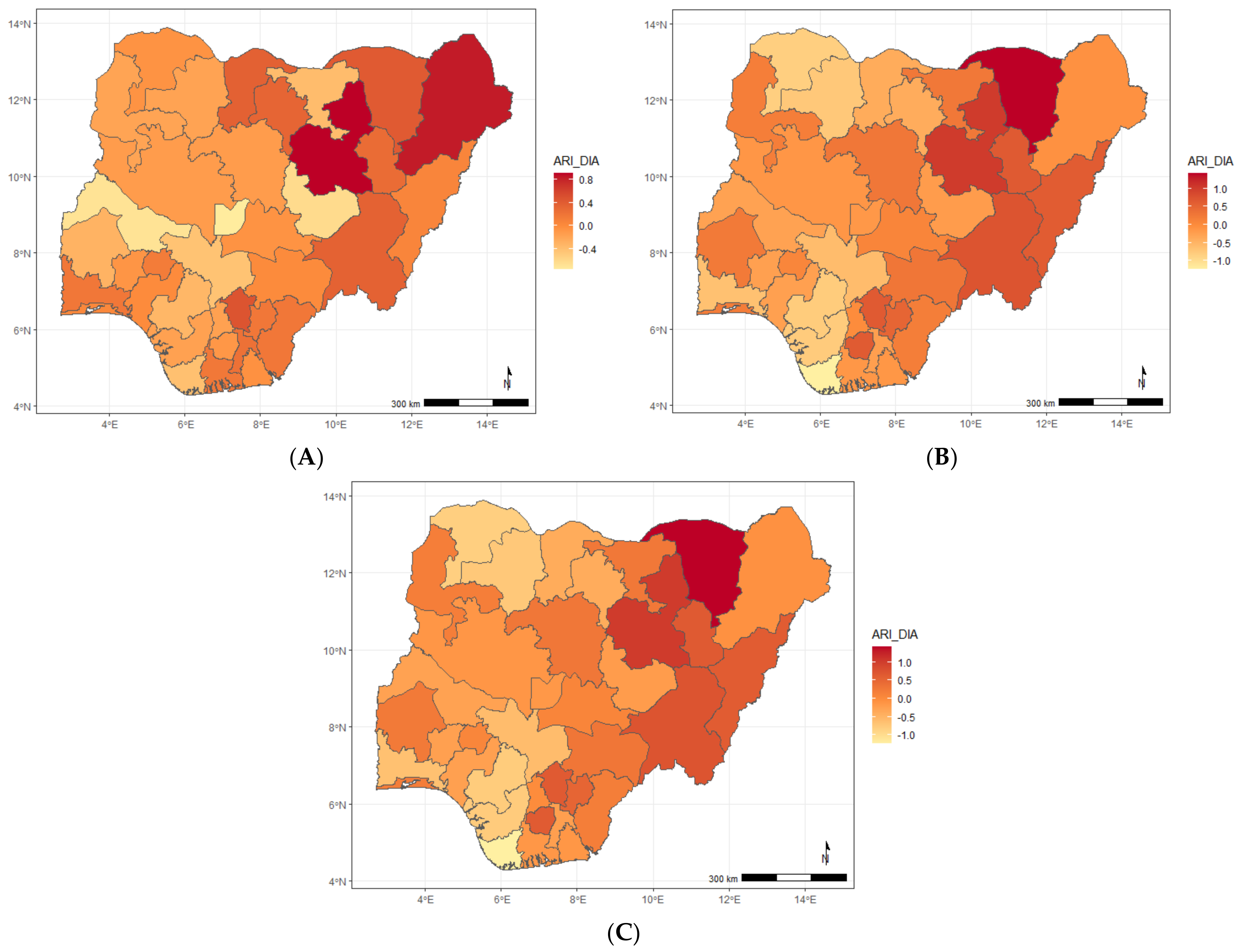
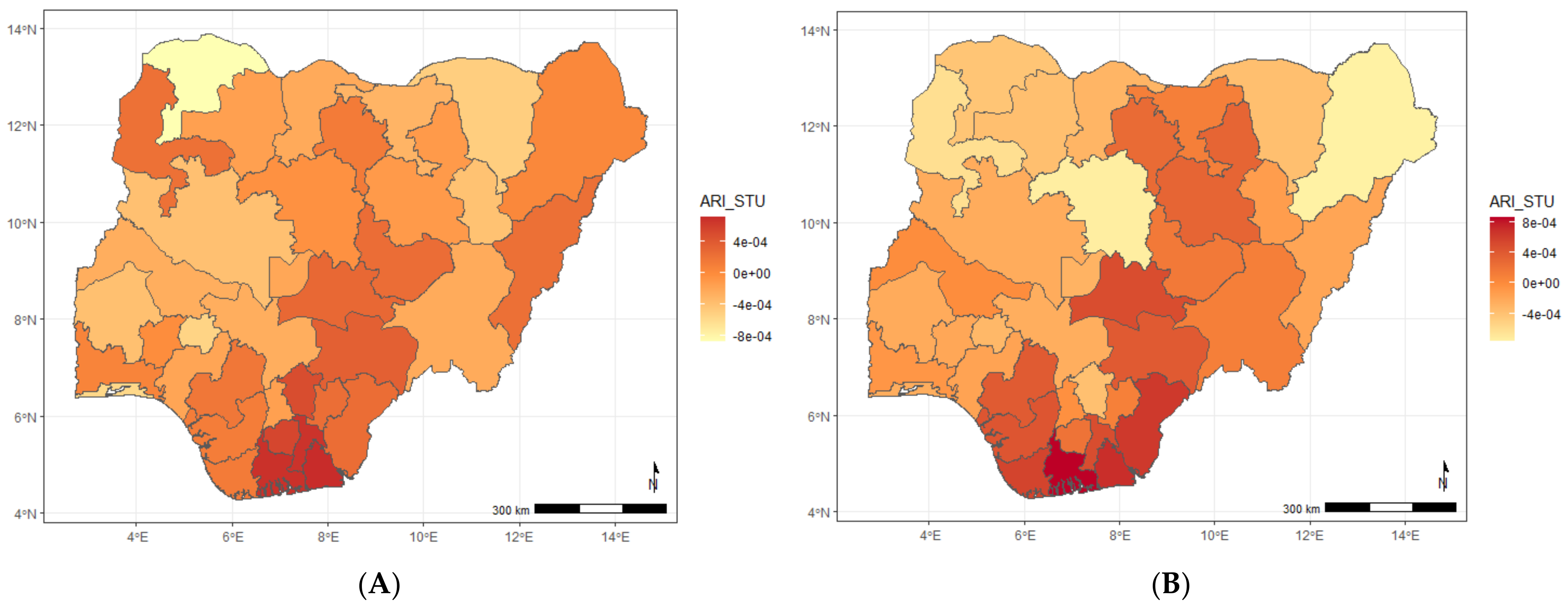
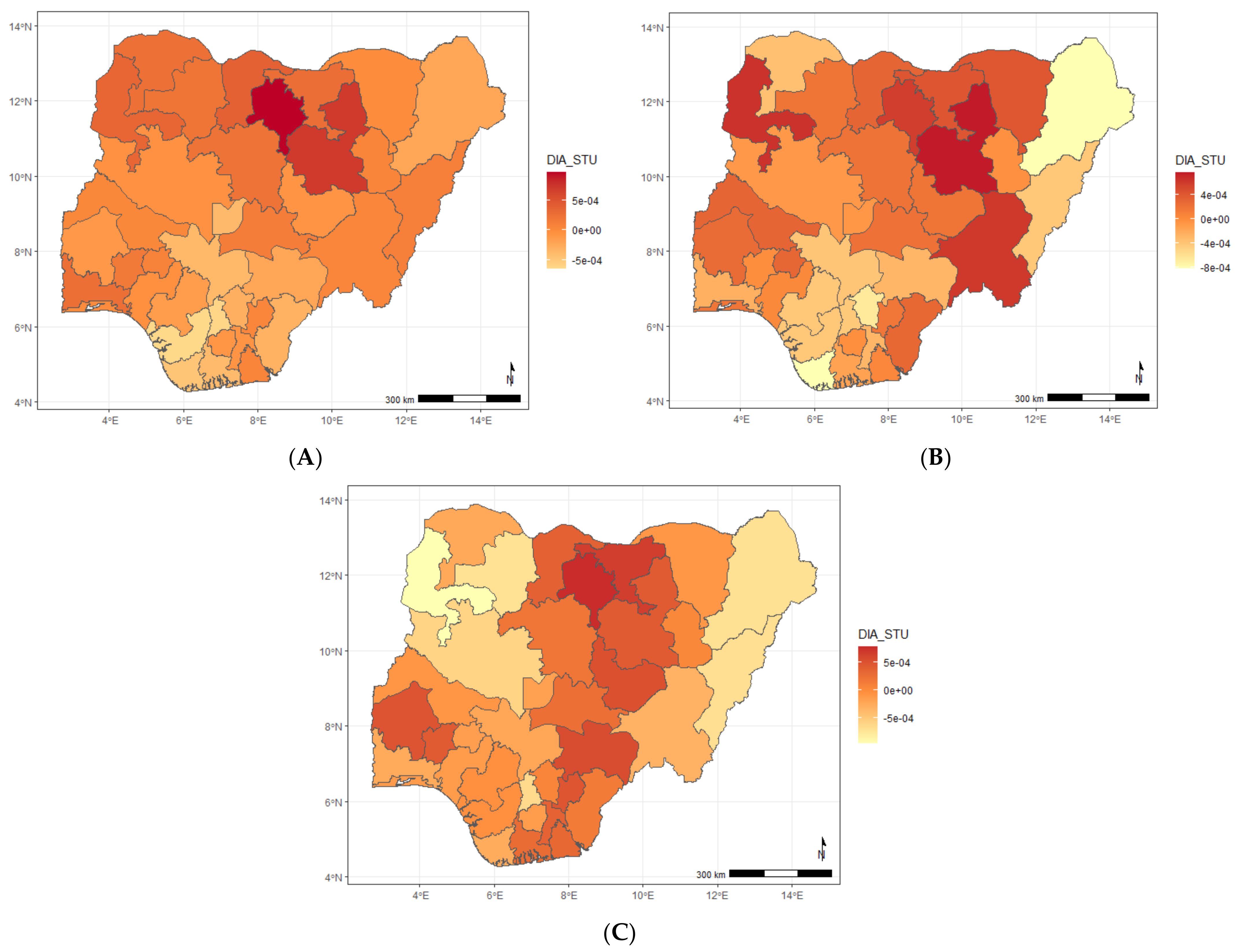
Figure 3a–d show the estimated spatial shared components across the states in Nigeria. The findings show that the shared effects of ARI and diarrhoea (
Figure 3a) were higher in neighbouring north-eastern states of Yobe, Bauchi, Borno, Gombe, Adamawa, Taraba, and a few neighbouring southern states (Enugu, Ebonyi, and Anambra) but lower among children residing in states belonging to the northwest and south-west regions of the country. The shared effects for ARI and stunting (
Figure 3b) showed higher odds among children living in Adamawa, Bauchi, Plateau, Nasarawa, Benue, Cross-River, Enugu, Ebony, Abia, Imo, Rivers, Edo, Delta, and Bayelsa, but were lower among those residing in the north-western and south-western regions of the country. As for diarrhoea and stunting (
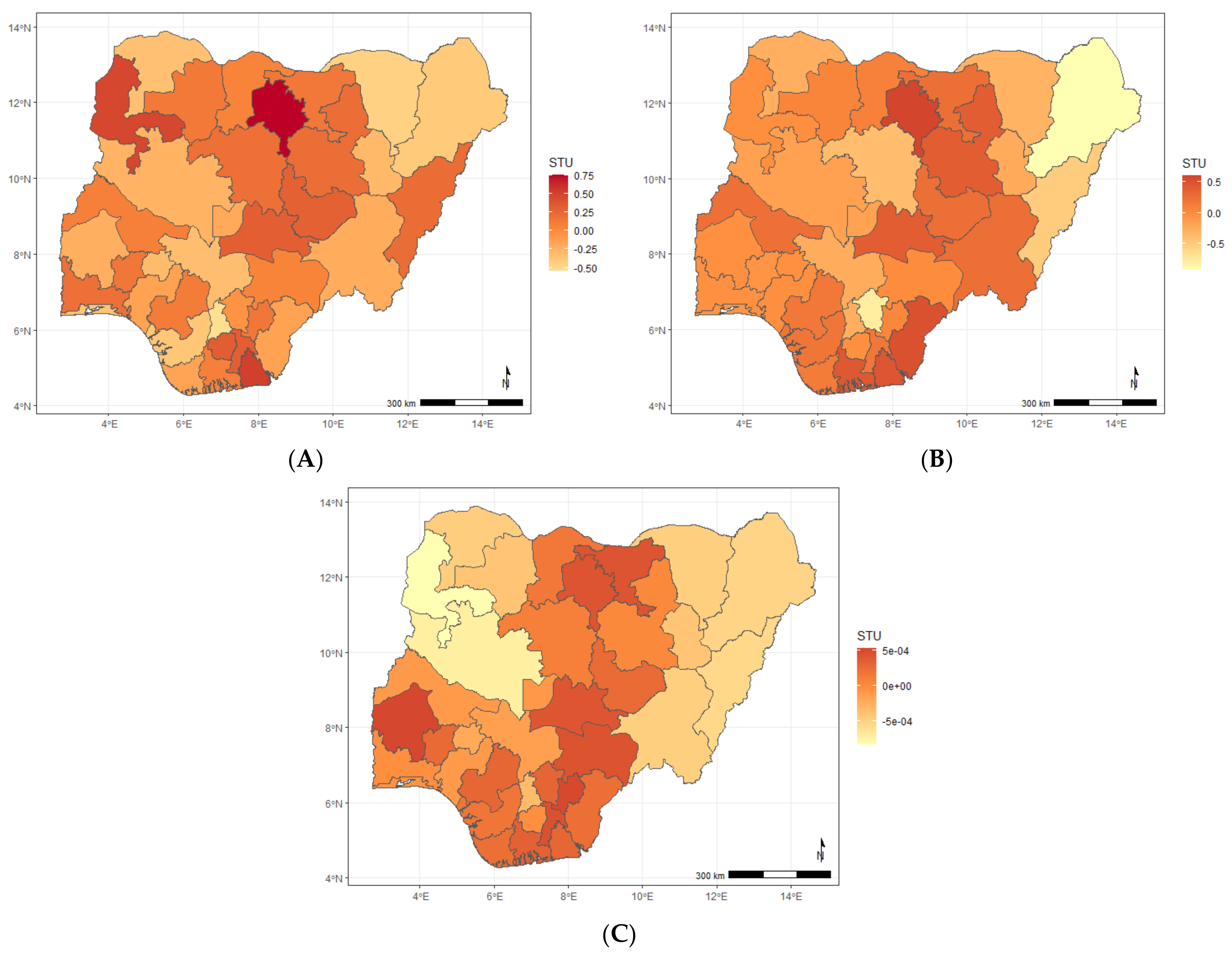
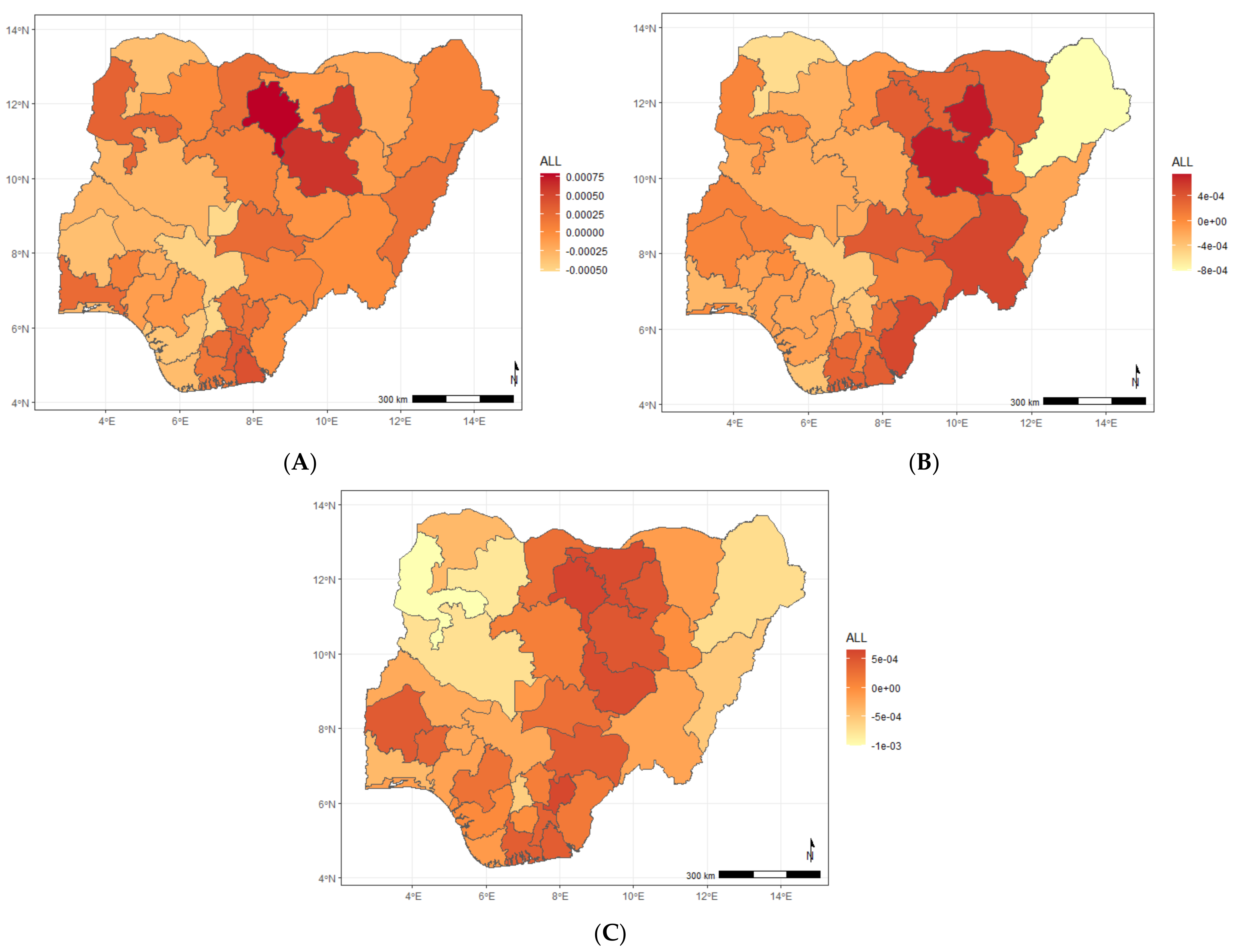
Figure 3c), the shared effects revealed higher odds among children living in Bauchi, Kano, and some of the neighbouring states, while they were less likely in Borno, Kogi, Enugu, Abia, Anambra, Imo, Edo, Delta, and Bayelsa. The shared effects for the three diseases presented in
Figure 3d revealed higher odds of suffering from the three diseases among children living in Bauchi, Kano, Taraba, Nasarawa, Adamawa, and some south southern states (Enugu, Ebonyi, Imo, Rivers, Abia, and Akwa Ibom). Year-specific disease estimates of disease-specific and shared state components are shown in
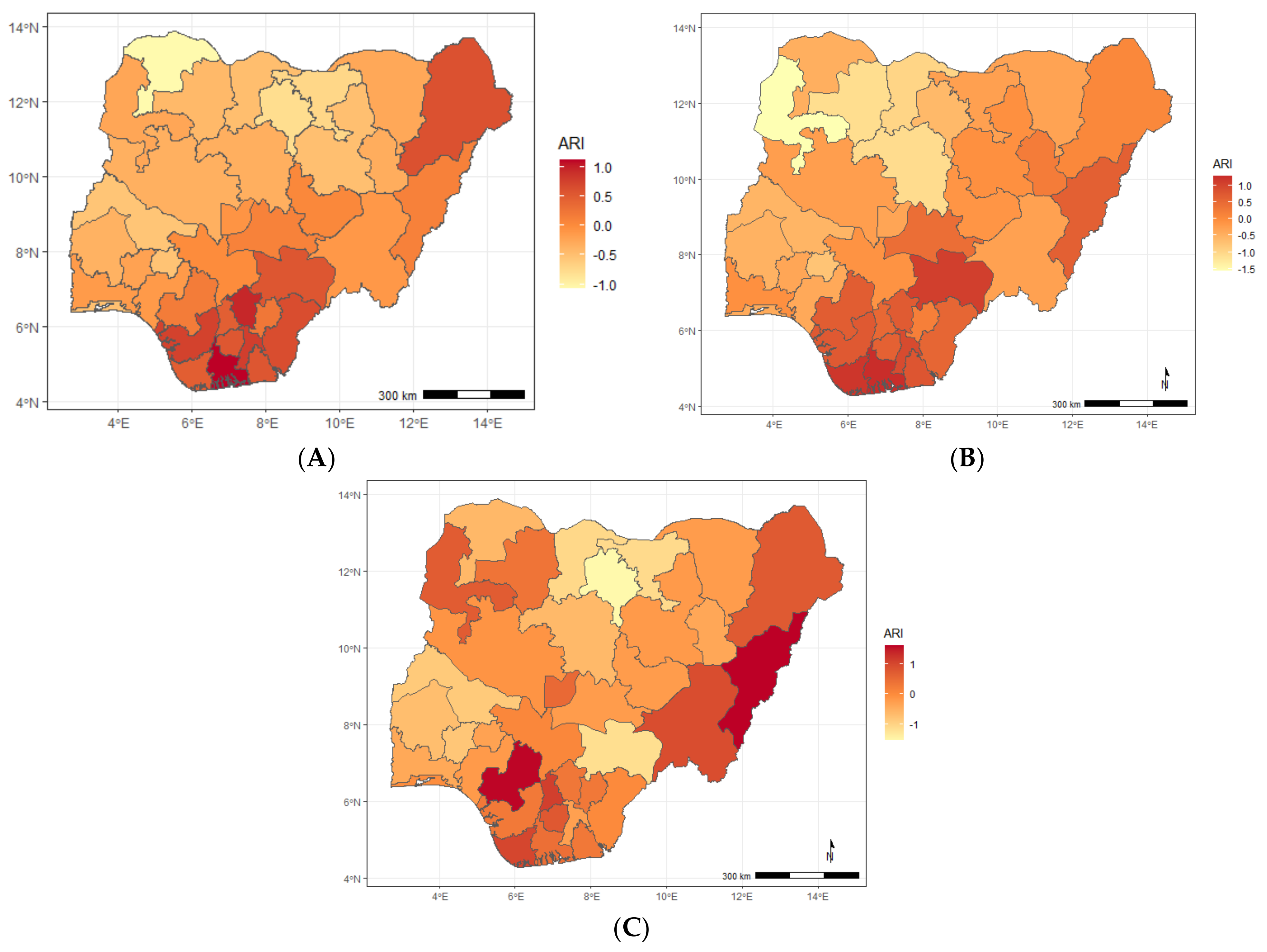
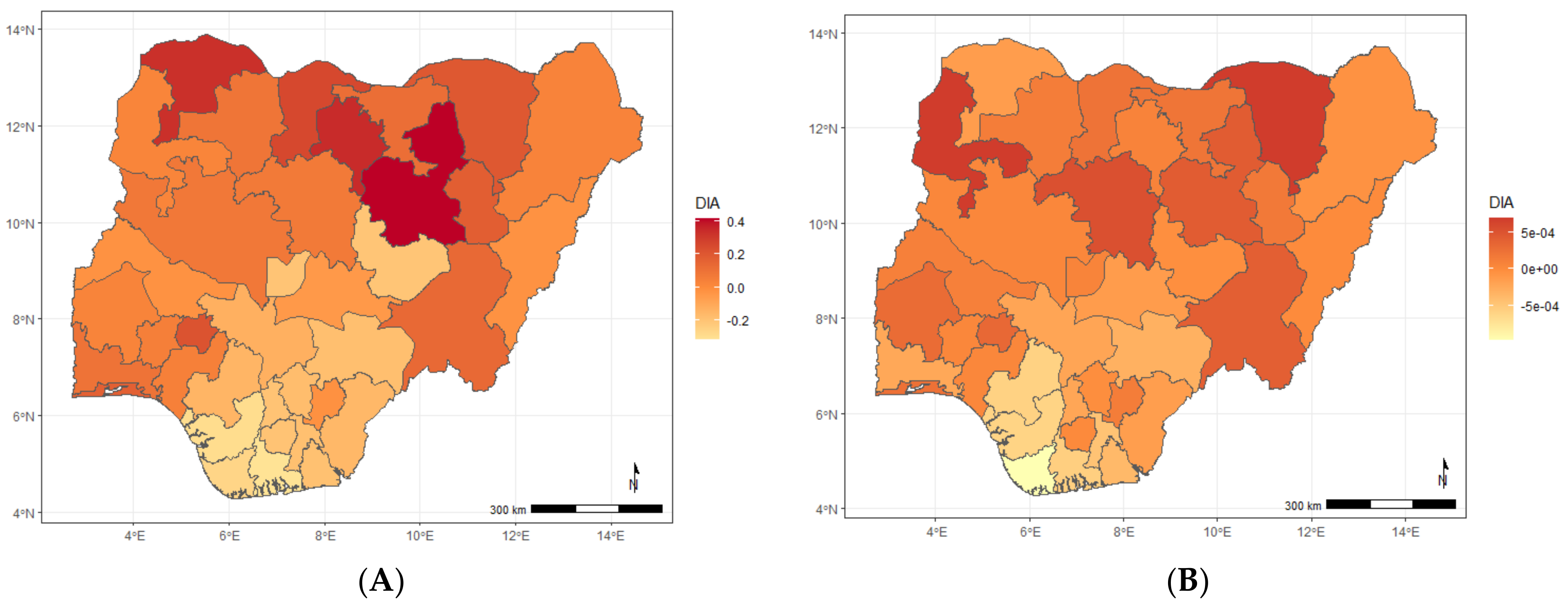
Appendix A, and similar patterns are observed.
4. Discussion
This study simultaneously examined the common and disease-specific spatial components of ARI, diarrhoea, and stunting in children under the age of 5 years old in Nigeria. We employed the shared spatial component model, which allowed us to split the geographical risk of child illnesses into common and uncommon spatial patterns. Childhood illness data obtained from 2008, 2013, and 2018 Nigerian Demographic and Health Surveys were used in the analyses. Our analysis could be considered an extension to the univariate spatial statistical application on childhood illnesses in Nigeria [
19,
29,
30,
31], most of which have relied on using univariate spatial models [
12,
34].
Our study found that the state-level co-morbidity of ARI and diarrhoea; ARI and stunting; diarrhoea and stunting; and ARI, diarrhoea, and stunting were predominant in the northeast and southern parts of the country. Our findings are consistent with previous works that found a higher prevalence of stunting and diarrhoeas among children living in the northern part of the country [
33,
35,
36]. Our findings of higher ARI-related co-morbidity in the southern parts of the country could be linked to oil spillage, leading to adverse air pollution and sand, which could adversely impact child health [
32,
33,
34,
35,
36,
37,
38,
39]. Regarding the effect of covariates, our findings are consistent with previous studies [
40,
41,
42,
43].
This study has some limitations, including that the child illnesses analysed were based on self-reporting from mothers and caregivers. Inaccuracies due to errors in reporting and recall could have been introduced into the data [
44]. A longer recall period of infections may underestimate their prevalence rates, as well as missing disease data [
45], which could adversely affect the estimate of the health indicators. We did not undertake any quality assessment of the data not accounting for the missing data. However, as the NDHS dataset analyses here ascertained acute respiratory infection and diarrhoea outcomes using mothers or caregiver-reported symptoms for a 2-week recall period, we believe the observed spatial patterns would not be affected.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}