
The Effect of Static Compression via Vibration Foam Rolling on Eccentrically Damaged Muscle

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
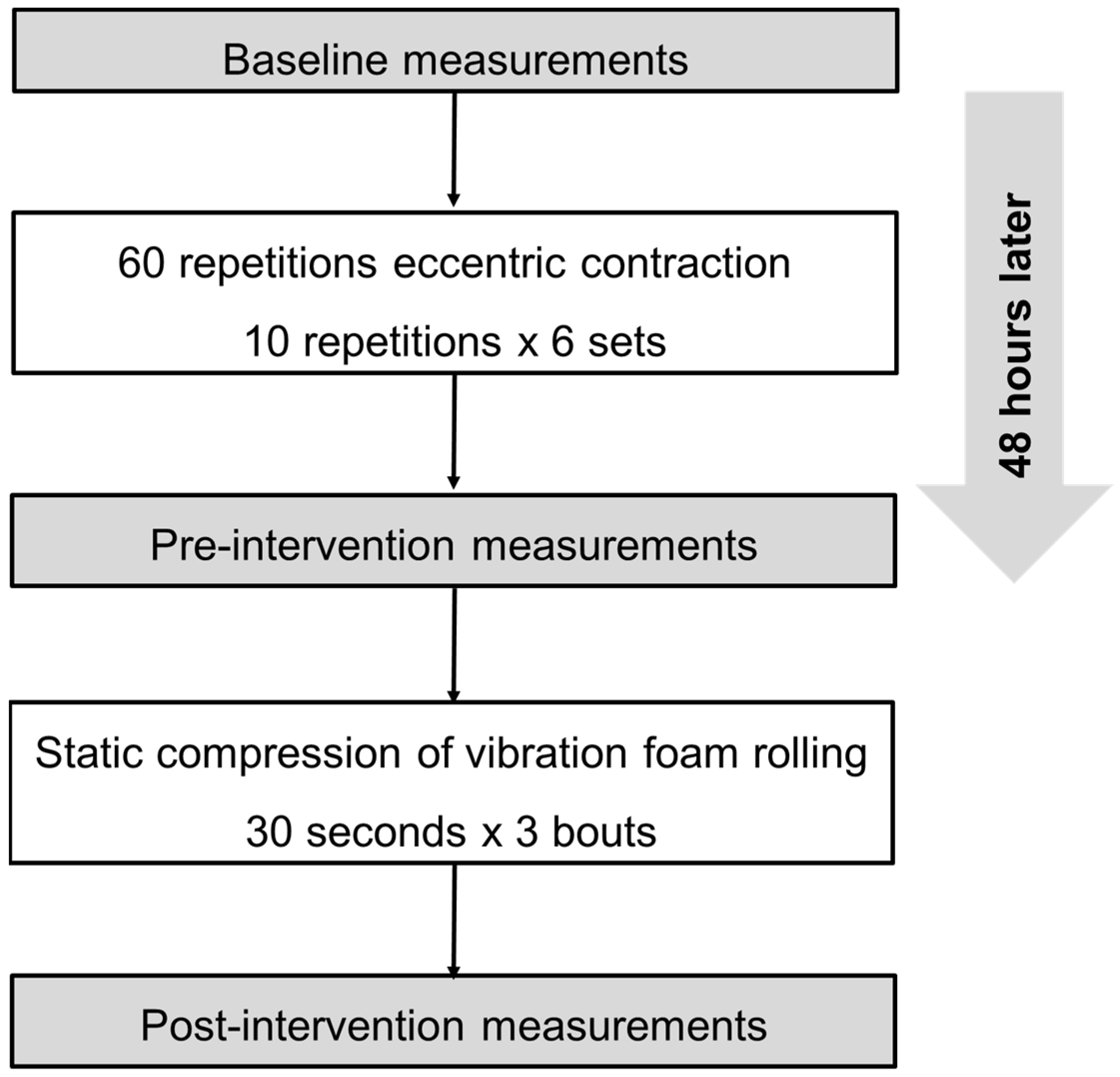
2.1. Experimental Design
2.2. Participants
2.3. MVC-ISO and MVC-CON
2.4. Knee Flexion ROM
2.5. Muscle Soreness
2.6. Pain Pressure Threshold
2.7. Tissue Hardness
2.8. Countermovement Jump Height
2.9. Eccentric Exercise Task
2.10. Static Compression via Vibration Foam Rolling
2.11. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wilke, J.; Müller, A.L.; Giesche, F.; Power, G.; Ahmedi, H.; Behm, D.G. Acute Effects of Foam Rolling on Range of Motion in Healthy Adults: A Systematic Review with Multilevel Meta-analysis. Sports Med. 2020, 50, 387–402. [Google Scholar] [CrossRef] [PubMed]
- Konrad, A.; Tilp, M.; Nakamura, M. A Comparison of the Effects of Foam Rolling and Stretching on Physical Performance. A Systematic Review and Meta-Analysis. Front. Physiol. 2021, 12, 720531. [Google Scholar] [CrossRef] [PubMed]
- Reiner, M.M.; Glashüttner, C.; Bernsteiner, D.; Tilp, M.; Guilhem, G.; Morales-Artacho, A.; Konrad, A. A comparison of foam rolling and vibration foam rolling on the quadriceps muscle function and mechanical properties. Eur. J. Appl. Physiol. 2021, 121, 1461–1471. [Google Scholar] [CrossRef] [PubMed]
- Park, S.J.; Lee, S.I.; Jeong, H.J.; Kim, B.G. Effect of vibration foam rolling on the range of motion in healthy adults: A systematic review and meta-analysis. J. Exerc. Rehabil. 2021, 17, 226–233. [Google Scholar] [CrossRef]
- Nakamura, M.; Sato, S.; Kiyono, R.; Yoshida, R.; Murakami, Y.; Yasaka, K.; Yahata, K.; Konrad, A. Acute Effect of Vibration Roller With and Without Rolling on Various Parts of the Plantar Flexor Muscle. Front. Physiol. 2021, 12, 716668. [Google Scholar] [CrossRef]
- Nakamura, M.; Sato, S.; Kiyono, R.; Yoshida, R.; Yasaka, K.; Yahata, K.; Konrad, A. Comparison Between Foam Rolling With and Without Vibration on Passive and Active Plantar Flexor Muscle Properties. J. Strength Cond. Res. 2021. [Google Scholar] [CrossRef]
- Behm, D.G.; Wilke, J. Do Self-Myofascial Release Devices Release Myofascia? Rolling Mechanisms: A Narrative Review. Sports Med. 2019, 49, 1173–1181. [Google Scholar] [CrossRef]
- Wilke, J.; Vogt, L.; Banzer, W. Immediate effects of self-myofascial release on latent trigger point sensitivity: A randomized, placebo-controlled trial. Biol. Sport 2018, 35, 349–354. [Google Scholar] [CrossRef]
- Chen, T.C.; Nosaka, K.; Sacco, P. Intensity of eccentric exercise, shift of optimum angle, and the magnitude of repeated-bout effect. J. Appl. Physiol. 2007, 102, 992–999. [Google Scholar] [CrossRef]
- Chen, T.C.; Chen, H.L.; Lin, M.J.; Wu, C.J.; Nosaka, K. Potent protective effect conferred by four bouts of low-intensity eccentric exercise. Med. Sci. Sports Exerc. 2010, 42, 1004–1012. [Google Scholar] [CrossRef] [Green Version]
- Matsuo, S.; Suzuki, S.; Iwata, M.; Hatano, G.; Nosaka, K. Changes in force and stiffness after static stretching of eccentrically-damaged hamstrings. Eur. J. Appl. Physiol. 2015, 115, 981–991. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Yasaka, K.; Kiyono, R.; Onuma, R.; Yahata, K.; Sato, S.; Konrad, A. The Acute Effect of Foam Rolling on Eccentrically-Induced Muscle Damage. Int. J. Environ. Res. Public Health 2020, 18, 75. [Google Scholar] [CrossRef] [PubMed]
- Romero-Moraleda, B.; González-García, J.; Cuéllar-Rayo, Á.; Balsalobre-Fernández, C.; Muñoz-García, D.; Morencos, E. Effects of Vibration and Non-Vibration Foam Rolling on Recovery after Exercise with Induced Muscle Damage. J. Sports Sci. Med. 2019, 18, 172–180. [Google Scholar]
- Takeuchi, K.; Takemura, M.; Nakamura, M.; Tsukuda, F.; Miyakawa, S. Effects of Active and Passive Warm-ups on Range of Motion, Strength, and Muscle Passive Properties in Ankle Plantarflexor Muscles. J. Strength Cond. Res. 2021, 35, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Konrad, A.; Kasahara, K.; Yoshida, R.; Yahata, K.; Sato, S.; Murakami, Y.; Aizawa, K.; Nakamura, M. Relationship between Eccentric-Exercise-Induced Loss in Muscle Function to Muscle Soreness and Tissue Hardness. Healthcare 2022, 10, 96. [Google Scholar] [CrossRef]
- Mavropalias, G.; Koeda, T.; Barley, O.R.; Poon, W.C.K.; Fisher, A.J.; Blazevich, A.J.; Nosaka, K. Comparison between high- and low-intensity eccentric cycling of equal mechanical work for muscle damage and the repeated bout effect. Eur. J. Appl. Physiol. 2020, 120, 1015–1025. [Google Scholar] [CrossRef]
- Kim, S.J.; Lee, J.H. Effects of sternocleidomastoid muscle and suboccipital muscle soft tissue release on muscle hardness and pressure pain of the sternocleidomastoid muscle and upper trapezius muscle in smartphone users with latent trigger points. Medicine 2018, 97, e12133. [Google Scholar] [CrossRef]
- Naderi, A.; Rezvani, M.H.; Degens, H. Foam Rolling and Muscle and Joint Proprioception After Exercise-Induced Muscle Damage. J. Athl. Train. 2020, 55, 58–64. [Google Scholar] [CrossRef]
- Fort-Vanmeerhaeghe, A.; Gual, G.; Romero-Rodriguez, D.; Unnitha, V. Lower Limb Neuromuscular Asymmetry in Volleyball and Basketball Players. J. Hum. Kinet. 2016, 50, 135–143. [Google Scholar] [CrossRef]
- Cohen, J. (Ed.) Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: Hillsdale, MI, USA, 1988. [Google Scholar]
- Nakamura, M.; Sato, S.; Hiraizumi, K.; Kiyono, R.; Fukaya, T.; Nishishita, S. Effects of static stretching programs performed at different volume-equated weekly frequencies on passive properties of muscle-tendon unit. J. Biomech. 2020, 103, 109670. [Google Scholar] [CrossRef]
- Tsai, W.C.; Chen, Z.R. The Acute Effect of Foam Rolling and Vibration Foam Rolling on Drop Jump Performance. Int. J. Environ. Res. Public Health 2021, 18, 3489. [Google Scholar] [CrossRef] [PubMed]
- Lamont, H.S.; Cramer, J.T.; Bemben, D.A.; Shehab, R.L.; Anderson, M.A.; Bemben, M.G. The acute effect of whole-body low-frequency vibration on countermovement vertical jump performance in college-aged men. J. Strength Cond. Res. 2010, 24, 3433–3442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aboodarda, S.J.; Spence, A.J.; Button, D.C. Pain pressure threshold of a muscle tender spot increases following local and non-local rolling massage. BMC Musculoskelet. Disord. 2015, 16, 265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavanaugh, M.T.; Döweling, A.; Young, J.D.; Quigley, P.J.; Hodgson, D.D.; Whitten, J.H.; Reid, J.C.; Aboodarda, S.J.; Behm, D.G. An acute session of roller massage prolongs voluntary torque development and diminishes evoked pain. Eur. J. Appl. Physiol. 2017, 117, 109–117. [Google Scholar] [CrossRef]

{kind=link}
| Knee Flexion ROM (deg) | MVC-ISO Torque (Nm) | MVC-CON Torque (Nm) | CMJ Height (cm) | |
|---|---|---|---|---|
| Baseline | 135.5 ± 8.1 | 157.8 ± 32.1 | 168.1 ± 36.7 | 18.4 ± 3.2 |
| Pre-intervention | 118.2 ± 10.2 * | 101.9 ± 34.8 * | 103.7 ± 41.3 * | 13.4 ± 3.8 * |
| Post-intervention | 125.6 ± 9.2 *, # | 106.6 ± 31.7 * | 112.5 ± 42.7 *, # | 15.0 ± 3.0 *, # |
| ANOVA results | p < 0.01, F = 46.3, ηp2 = 0.78 | p < 0.01, F = 27.1, ηp2 = 0.68 | p < 0.01, F = 19.5, ηp2 = 0.62 | p < 0.01, F = 23.8, ηp2 = 0.65 |
| PPT (kg) | Tissue Hardness (N) | Muscle Soreness at MVC-ISO (mm) | Muscle Soreness at MVC-CON (mm) | Muscle Soreness at Stretching (mm) | Muscle Soreness at Palpation (mm) | |
|---|---|---|---|---|---|---|
| Baseline | 2.2 ± 0.8 | 18.2 ± 3.6 | 7.7 ± 6.1 | 7.0 ± 7.7 | 2.1 ± 4.6 | 12.9 ± 10.7 |
| Pre-intervention | 0.9 ± 0.5 * | 20.8 ± 2.5 * | 46.3 ± 20.2 * | 49.0 ± 22.9 * | 42.6 ± 21.9 * | 44.3 ± 17.3 * |
| Post-intervention | 2.3 ± 0.7 # | 18.6 ± 3.0 # | 32.3 ± 20.2 *, # | 31.2 ± 20.2 *, # | 30.3 ± 19.4 *, # | 33.6 ± 14.2 *, # |
| ANOVA results | p < 0.01, F = 41.0, ηp2 = 0.76 | p < 0.01, F = 10.2, ηp2 = 0.44 | p < 0.01, F = 29.4, ηp2 = 0.69 | p < 0.01, F = 29.1, ηp2 = 0.71 | p < 0.01, F = 35.1, ηp2 = 0.73 | p < 0.01, F = 33.0, ηp2 = 0.72 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakamura, M.; Kasahara, K.; Yoshida, R.; Yahata, K.; Sato, S.; Murakami, Y.; Aizawa, K.; Konrad, A. The Effect of Static Compression via Vibration Foam Rolling on Eccentrically Damaged Muscle. Int. J. Environ. Res. Public Health 2022, 19, 1823. https://doi.org/10.3390/ijerph19031823
Nakamura M, Kasahara K, Yoshida R, Yahata K, Sato S, Murakami Y, Aizawa K, Konrad A. The Effect of Static Compression via Vibration Foam Rolling on Eccentrically Damaged Muscle. International Journal of Environmental Research and Public Health. 2022; 19(3):1823. https://doi.org/10.3390/ijerph19031823
Chicago/Turabian StyleNakamura, Masatoshi, Kazuki Kasahara, Riku Yoshida, Kaoru Yahata, Shigeru Sato, Yuta Murakami, Kodai Aizawa, and Andreas Konrad. 2022. "The Effect of Static Compression via Vibration Foam Rolling on Eccentrically Damaged Muscle" International Journal of Environmental Research and Public Health 19, no. 3: 1823. https://doi.org/10.3390/ijerph19031823
APA StyleNakamura, M., Kasahara, K., Yoshida, R., Yahata, K., Sato, S., Murakami, Y., Aizawa, K., & Konrad, A. (2022). The Effect of Static Compression via Vibration Foam Rolling on Eccentrically Damaged Muscle. International Journal of Environmental Research and Public Health, 19(3), 1823. https://doi.org/10.3390/ijerph19031823