
Predictors of Child’s Health in Pakistan and the Moderating Role of Birth Spacing

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Variables and Measurement
3. Results
4. Discussions
5. Recommendations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
List of Abbreviations
| ANC | Antenatal care |
| LMICs | Low- middle-income countries |
| MHCSU | Mother’s health care services utilization |
| PDHS | Pakistan Demographic and Health Survey |
| SBA | Skilled birth attendance |
| SDGs | Sustainable Development Goals |
| SES | Socio-economic status |
| TV | Television |
| UMNFP | Unmet Need for Family Planning |
| USA | United States of America |
References
- Allen, M.L.; Martinez, S. The politics of children’s issues: Challenges and opportunities for advancing a children’s agenda in the political arena. In Applied Developmental Science an Advanced Textbook; Lerner, R.M., Jacobs, F., Wertlieb, D., Eds.; SAGE Publications: London, UK, 2005; pp. 325–352. [Google Scholar]
- Government of Pakistan. Pakistan Economic Survey; Ministry of Finance: Islamabad, Pakistan, 2020. [Google Scholar]
- UNICEF. Levels and Trends in Child Mortality: Estimates Developed by the UN Inter-Agency Group for Child Mortality Estimation; UNICEF: New York, NY, USA, 2021. [Google Scholar]
- Victorino, C.C.; Gauthier, A.H. The social determinants of child health: Variations across health outcomes—A population-based cross-sectional analysis. BMC Pediatr. 2009, 9, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegler, M.; Epstein, R.A. Organizers’ introduction to the conference on Social Determinants of Health and Disease. Perspect. Biol. Med. 2003, 46, S1–S8. [Google Scholar] [CrossRef]
- Irwin, A.; Valentine, N.; Brown, C.; Loewenson, R.; Solar, O.; Brown, H.; Koller, T.; Vega, J. The commission on social determinants of health: Tackling the social roots of health inequities. PLoS Med. 2006, 3, 749–751. [Google Scholar] [CrossRef]
- Wu, Y.; Zhou, H.; Wang, Q.; Cao, M.; Medina, A.; Rozelle, S. Use of maternal health services among women in the ethnic rural areas of western China. BMC Health Serv. Res. 2019, 19, 179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahmood, N.; Mahmood, M.A.; Ahmed, T. Gender Differences in Child Health-care Practices: Evidence from the Pakistan Demographic and Health Survey, 1990–1991. Pak. Dev. Rev. 1995, 34, 693–707. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Child Mortality. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/children-reducing-mortality (accessed on 18 August 2021).
- National Institute of Population Studies. Pakistan Demographic Health Survey 2017–18; National Institute of Population Studies: Islamabad, Pakistan, 2018. [Google Scholar]
- Rosenbaum, S. Child health and poor children. Am. Behav. Sci. 1992, 35, 275–289. [Google Scholar] [CrossRef]
- Scholer, S.J.; Hickson, G.B.; Ray, W.A. Sociodemographic factors identify US infants at high risk for injury mortality. Pediatrics 1999, 103, 1183–1188. [Google Scholar] [CrossRef]
- Séguin, L.; Xu, Q.; Gauvin, L.; Zunzunegui, M.-V.; Potvin, L.; Frohlich, K.L. Understanding the dimensions of socioeconomic status that influence toddlers’ health: Unique impact of lack of money for basic needs in Quebec’s birth cohort. J. Epidemiol. Community Health 2005, 59, 42–48. [Google Scholar] [CrossRef]
- Brooks-Gunn, J.; Duncan, G.J. The effects of poverty on children. Future Child. 1997, 7, 55–71. [Google Scholar] [CrossRef] [Green Version]
- Schnittker, J. Education and the changing shape of the income gradient in health. J. Health Soc. Behav. 2004, 45, 286–305. [Google Scholar] [CrossRef]
- Herd, P.; Goesling, B.; House, J.S. Socioeconomic Position and Health: The Differential Effects of Education versus Income on the Onset versus Progression of Health Problems. J. Health Soc. Behav. 2007, 48, 223–238. [Google Scholar] [CrossRef] [PubMed]
- Pawlinska-Chmara, R.; Wronka, I. Assessment of the effect of socioeconomic factors on the prevalence of respiratory disorders in children. J. Physiol. Pharmacol. 2007, 58, 523–529. [Google Scholar] [PubMed]
- Pederson, C.R.; Madsen, M.; Kohler, L. Does financial strain explain the association between children’s morbidity and parental non-employment? J. Epidemiol. Community Health 2005, 59, 316–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mondal, M.N.; Hossain, M.K.; Ali, M.K. Factors influencing infant and child mortality: A case study of Rajshahi District, Bangladesh. J. Hum. Ecol. 2009, 26, 31–39. [Google Scholar] [CrossRef]
- Fawole, O.I.; Adeoye, I.A. Women’s status within the household as a determinant of maternal health care use in Nigeria. Afr. Health Sci. 2015, 15, 217–225. [Google Scholar] [CrossRef] [Green Version]
- Santrock, J.W. Life-Span Development, 14th ed.; McGraw Hill: New York, NY, USA, 2013; pp. 82–83. [Google Scholar]
- Bennett, J. Correlates of child mortality in Pakistan: A hazards model analysis. Pak. Dev. Rev. 1999, 38, 85–118. [Google Scholar] [CrossRef]
- Bhutta, Z.A.; Hafeez, A. What can Pakistan do to address maternal and child health over the next decade? Health Res. Policy Syst. 2015, 13, 13–16. [Google Scholar] [CrossRef] [Green Version]
- Mumtaz, S.; Bahk, J.; Khang, Y.H. Current status and determinants of maternal healthcare utilization in Afghanistan: Analysis from Afghanistan Demographic and Health Survey 2015. PLoS ONE 2019, 14, e0217827. [Google Scholar] [CrossRef] [Green Version]
- Zhao, P.; Han, X.; You, L.; Zhao, Y.; Yang, L.; Liu, Y. Maternal health services utilization and maternal mortality in China: A longitudinal study from 2009 to 2016. BMC Pregnancy Childbirth 2020, 20, 220. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Report of a WHO Technical Consultation on Birth Spacing: Geneva, Switzerland 13–15 June 2005 (No. WHO/RHR/07.1); World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Asif, M.F.; Pervaiz, Z.; Afridi, J.R.; Safdar, R.; Abid, G.; Lassi, Z.S. Socio-economic determinants of child mortality in Pakistan and the moderating role of household’s wealth index. BMC Pediatr. 2022, 22, 3. [Google Scholar] [CrossRef]
- Zakar, R.; Zakar, M.Z.; Aqil, N.; Chaudhry, A.; Nasrullah, M. Determinants of maternal health care services utilization in Pakistan: Evidence from Pakistan demographic and health survey, 2012–2013. Obstet. Gynecol. 2017, 37, 330–337. [Google Scholar]
- Murtaza, F.; Mustafa, T.; Awan, R. Determinants of nonimmunization of children under 5 years of age in Pakistan. Fam. Med. Community Health 2016, 23, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agopian, A.J.; Lupo, P.J.; Herdt-Losavio, M.L.; Langlois, P.H.; Rocheleau, C.M.; Mitchell, L.E.; Study, T.N. Differences in folic acid use, prenatal care, smoking, and drinking in early pregnancy by occupation. Prev. Med. 2012, 55, 341–345. [Google Scholar] [CrossRef] [Green Version]
- Asif, M.F.; Safdar, H.; Ali, S. Factors affecting the performance of school students: A case study of Bahawalpur. Ilkogr. Online 2020, 19, 3650–3660. [Google Scholar]
- Asif, M.F.; Khalid, S.; Khalid, K.R.; Abid, G. Effect of mother’s employment on child mortality in Pakistan: Moderating role of mother’s empowerment. J ISOSS. 2021, 7(4), 175–186. [Google Scholar]
- Furuta, M.; Salway, S. Women’s position within the household as a determinant of maternal health care use in Nepal. Int. Fam. Plan. 2006, 32, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Bloom, D.E.; Canning, D.; Jamison, D.T. Health, wealth, and welfare. Financ. Dev. 2004, 41, 10–15. [Google Scholar]
- Ali, S.; Asif, M.F.; Khan, M.K.; Fatima, N.; Safdar, H.; Lassi, Z.S. Moderating role of husband’s education and their employment on female labor force participation in Pakistan. Ilkogr. Online 2020, 19, 5265–5276. [Google Scholar]
- Nisar, N.; White, F. Factors affecting utilization of antenatal care among reproductive age group women (15–49 years) in an urban squatter settlement of Karachi. J. Pak. Med. Assoc. 2003, 53, 47. [Google Scholar]
- Matsumura, M.; Gubhaju, B. Women’s Status, Household Structure and the Utilization of Maternal Health Services in Nepal: Even primary-leve1 education can significantly increase the chances of a woman using maternal health care from a modem health facility. Asia-Pac. Popul. J. 2001, 16, 23–44. [Google Scholar] [CrossRef]
- Gage, A.J. Barriers to the utilization of maternal health care in rural Mali. Soc. Sci. Med. 2007, 65, 1666–1682. [Google Scholar] [CrossRef]
- Hurt, H.; Brodsky, N.L.; Roth, H.; Malmud, E.; Giannetta, J.M. School performance of children with gestational cocaine exposure. Neurotoxicol. Teratol. 2005, 27, 203–211. [Google Scholar] [CrossRef]
- USAID. Multi-Sectoral Nutrition Strategy 2014–2025; Agency for International Development: Washington, DC, USA, 2014. [Google Scholar]
- Wagstaff, A. Poverty and health sector inequalities. Bull. World Health Organ. 2002, 80, 97–105. [Google Scholar] [PubMed]
- Obermeyer, C.M.; Potter, J.E. Maternal health care utilization in Jordan: A study of patterns and determinants. Stud. Fam. Plan. 1991, 22, 177–187. [Google Scholar] [CrossRef]
- Rahat, R.; Zakar, R.; Zakar, M.Z. Factors associated with non-utilization of child immunization in Pakistan: Evidence from the Demographic and Health Survey 2006–07. BMC Public Health 2014, 14, 232. [Google Scholar]
- Iqbal, S.; Maqsood, S.; Zakar, R.; Zakar, M.Z.; Fischer, F. Continuum of care in maternal, newborn and child health in Pakistan: Analysis of trends and determinants from 2006 to 2012. BMC Health Serv. Res. 2017, 17, 189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conde-Agudelo, A.; Rosas-Bermúdez, A.; Kafury-Goeta, A.C. Birth spacing and risk of adverse perinatal outcomes: A meta-analysis. JAMA 2006, 295, 1809–1823. [Google Scholar] [CrossRef] [PubMed]
- Zafar, R.; Abid, G.; Rehmat, M.; Ali, M.; Hassan, Q.; Asif, M.F. So hard to say goodbye: Impact of punitive supervision on turnover intention. Total Qual. Manag. Bus. Excell. 2021. [Google Scholar] [CrossRef]
- Abid, G.; Shaikh, S.; Asif, M.F.; Elahi, N.S.; Anwar, A.; Butt, G.T. Influence of perceived organizational support on job satisfaction: Role of proactive personality and thriving. Int. J. Entrep. 2021, 25, 1–11. [Google Scholar]
- Yasir, A.; Abid, G.; Afridi, J.H.; Elahi, N.S.; Asif, M.F. Social media communication and behavioral intention of customers in hospitality industry: The mediating role of customer satisfaction. Int. J. Entrep. 2021, 25, 1–14. [Google Scholar]
- DaVanzo, J.; Hale, L.; Razzaque, A.; Rahman, M. The effects of pregnancy spacing on infant and child mortality in Matlab, Bangladesh: How they vary by the type of pregnancy outcome that began the interval. Popul Stud. 2008, 62, 131–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asif, M.F.; Pervaiz, Z. Socio-demographic determinants of unmet need for family planning among married women in Pakistan. BMC Public Health 2019, 19, 1226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asif, M.F.; Pervaiz, Z.; Afridi, J.R.; Abid, G.; Lassi, Z.S. Role of husband’s attitude towards the usage of contraceptives for unmet need of family planning among married women of reproductive age in Pakistan. BMC Women’s Health 2021, 21, 163. [Google Scholar] [CrossRef] [PubMed]
- Black, S.E.; Devereux, P.J.; Salvanes, K.G. From the cradle to the labor market? The effect of birth weight on adult outcomes. Q. J. Econ. 2007, 122, 409–439. [Google Scholar] [CrossRef]
- Conley, D.; Bennett, N.G. Is biology destiny? Birth weight and life chances. Am. Sociol. Rev. 2000, 65, 458–467. [Google Scholar] [CrossRef] [Green Version]
- Leon, D.A.; Lithell, H.O.; Vågerö, D.; Koupilová, I.; Mohsen, R.; Berglund, L.; Lithell, U.B.; McKeigue, P.M. Reduced fetal growth rate and increased risk of death from ischaemic heart disease: Cohort study of 15,000 Swedish men and women born 1915–29. BMJ 1998, 317, 241–245. [Google Scholar] [CrossRef] [Green Version]
- Moster, D.; Lie, R.T.; Markestad, T. Long-term medical and social consequences of preterm birth. N. Engl. J. Med. 2008, 359, 262–273. [Google Scholar] [CrossRef] [Green Version]
- Swamy, G.K.; Østbye, T.; Skjærven, R. Association of preterm birth with long-term survival, reproduction, and next-generation preterm birth. JAMA 2008, 299, 1429–1436. [Google Scholar] [CrossRef] [Green Version]
- Zajonc, R.B. Family configuration and intelligence. Science 1976, 192, 227–236. [Google Scholar] [CrossRef]
- Qaiser, N.; Sattar, N.; Arshi, S.; Asif, M.F.; Afridi, J.R. Impact of thriving on job performance, positive health and turnover intention: Consequences of thriving at workplace. Int. J. Inf. Bus. Manag. 2021, 13, 97–107. [Google Scholar]
- Hydari, M.A.; Abid, G.; Asif, M.F.; Butt, T.H.; Lassi, Z.S. The Effects of COVID-19 (Corona Virus Disease 2019) Pandemic: An Exploratory Study of Pakistan. Int. J. Dis. Rec. Bus. Cont. 2019, 12, 1431–1449. [Google Scholar]
- Pebley, A.R.; Millman, S. Birth spacing and child survival. Int. Fam. Plan. 1986, 1, 71–79. [Google Scholar] [CrossRef]
- Swaminathan, A.; Fell, D.B.; Regan, A.; Walker, M.; Corsi, D.J. Association between interpregnancy interval and subsequent stillbirth in 58 low-income and middle-income countries: Retrospective analysis using Demographic and Health Surveys. Lancet Glob. Health 2020, 8, 113–122. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Symbol | Variables | Definition of Variables | Measurement |
|---|---|---|---|
| CH | Child’s Health | Child weight at birth has been used as a proxy of child health. If a child’s weight at birth is less than 2.5 kg, this is considered unhealthy, and if a child’s weight at birth is at least 2.5 kg, this is considered healthy. | 1 = Unhealthy child 2 = Healthy child |
| M.Age | Mother’s Age | Mother’s age has been classified into two different groups: mothers aged 15–34, and mothers aged 35–49 years. | 1 = 15–34 2 = 35–49 |
| M.Edu | Mother’s Education | Mother’s education is divided into two categories. If the mother has no education and has attended primary school only, this is considered as “less than secondary,” and if the mother has completed secondary school education and has completed higher education, then this is considered as “at least secondary.” | 1 = Less than secondary 2= At least secondary |
| M.Emp | Mother’s Employment Status | Mother’s employment status is divided into two categories, i.e., mothers currently not working, and mothers currently working. | 0 = Currently not working (unemployed) 1 = Currently working (employed) |
| MHCSU | Mother’s Health Care Services Utilization | This variable was constructed based on whether the mother had at least 4 or more antenatal care visits (ANC), skilled birth attendance (SBA), and received postpartum care within 42 days of delivery. If the mother had received all these services, this is considered more accessible, and if the mother had not received all these services, this is considered less accessible. We used ANC, SBA, and postpartum care as indicators to measure maternal health care utilization, which had been used in several earlier primary studies from neighboring countries [24,25]. | 1 = Less accessible 2 = More accessible |
| WSH | Wealth Status of Household | Wealth status was divided into quintiles from poorest to richest. Women belonging to the poorest, poorer, and middle quintiles are considered low wealth status, and if women belonging to the richer and richest quintiles are considered high wealth status. | 1 = Low wealth status 2 = High wealth status |
| F.Edu | Father’s Education | Father’s education is divided into two categories. If the father has no education and has attended primary school, this is considered “less than secondary,” and if the father has completed secondary school or higher education, this is considered “at least secondary.” | 1 = Less than secondary 2= At least secondary |
| EMM | Exposure to Mass Media | The PDHS 2017-18 provides information on households’ ownership of a radio or television, along with the type of health message delivered to women through these media. In this study, the presence of a television (TV) in the household has been used as a proxy for this variable. | 1 = Presence of TV 0 = Otherwise |
| BS | Birth Spacing | The World Health Organization has recommended a minimum birth interval of 33 months between two births, or at least 24 months before attempting the subsequent pregnancy, to reduce the risk of adverse maternal, perinatal, and infant outcomes [26]. | 1 = Women take less than 33 months birth spacing between two children 2 = Women take at least 33 months birth spacing between two children |
| MHCSU * BS | Mother’s Health Care Services Utilization * Birth Spacing | The interaction term of mother’s health care services utilization and birth spacing. The interaction term has been used to examine the moderating effect of birth spacing on the relationship between a mother’s health care services utilization and a child’s health. |
| Socio-Economic Characteristics | Frequency | Percentage (%) | |
|---|---|---|---|
| Child’s Health | Unhealthy | 415 | 18.5 |
| Healthy | 1831 | 81.5 | |
| Mother’s Age | <35 years | 1821 | 81.1 |
| >35 years | 425 | 18.9 | |
| Mother’s Education | Less than secondary | 643 | 28.6 |
| At least secondary | 1603 | 71.4 | |
| Mother’s Employment Status | Unemployed | 1938 | 86.3 |
| Employed | 308 | 13.7 | |
| Mother’s Health Care Services Utilization | Less accessible | 257 | 11.4 |
| More accessible | 1989 | 88.6 | |
| Wealth Status of Household | Low | 787 | 35.0 |
| High | 1459 | 65.0 | |
| Father’s Education | Less than secondary | 464 | 20.7 |
| At least secondary | 1782 | 79.3 | |
| Exposure to Mass Media | No | 397 | 17.7 |
| Yes | 1849 | 82.3 | |
| Birth Spacing | Less than 33 months | 1633 | 72.7 |
| At least 33 months | 613 | 27.3 | |
| Independent Variables | Β | p-Value | Odds Ratio | 95% C.I. for EXP(β) | ||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Constant | 0.749 | 0.000 | 2.115 | |||
| Mother’s Age | <35 years | Reference | ||||
| >35 years | 0.195 * | 0.013 | 1.215 | 0.863 | 1.592 | |
| Mother’s Education | Less than secondary | Reference | ||||
| At least secondary | 0.115 * | 0.039 | 1.122 | 0.835 | 1.298 | |
| Mother’s Employment Status | Unemployed | Reference | ||||
| Employed | −0.199 * | 0.020 | 0.819 | 0.587 | 1.171 | |
| Mother’s Health Care Services Utilization | Less accessible | Reference | ||||
| More accessible | 0.206 * | 0.011 | 1.500 | 1.091 | 1.916 | |
| Wealth Status of Household | Low | Reference | ||||
| High | 0.263 * | 0.045 | 1.301 | 1.116 | 1.672 | |
| Father’s Education | Less than secondary | Reference | ||||
| At least secondary | 0.197 * | 0.016 | 1.218 | 0.797 | 1.583 | |
| Exposure of Mass Media | No | Reference | ||||
| Yes | 0.034 * | 0.021 | 1.014 | 0.851 | 1.396 | |
| Birth Spacing | Less than 33 months | Reference | ||||
| At least 33 months | 0.179 | 0.058 | 1.196 | 0.827 | 1.528 | |
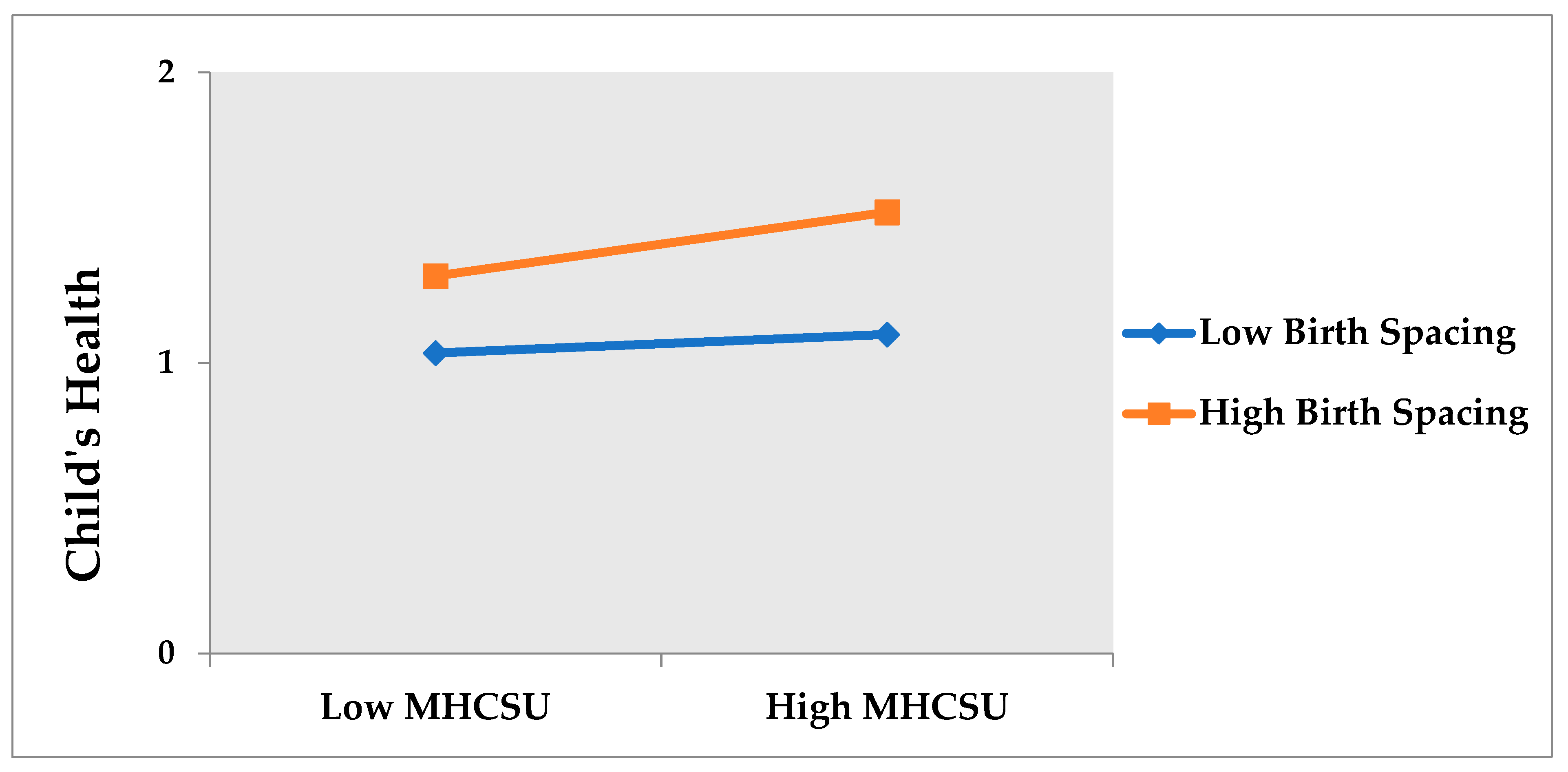
| Mother’s Health Care Services Utilization * Birth Spacing | 0.236 * | 0.034 | 1.279 | 0.831 | 1.729 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asif, M.F.; Meherali, S.; Abid, G.; Khan, M.S.; Lassi, Z.S. Predictors of Child’s Health in Pakistan and the Moderating Role of Birth Spacing. Int. J. Environ. Res. Public Health 2022, 19, 1759. https://doi.org/10.3390/ijerph19031759
Asif MF, Meherali S, Abid G, Khan MS, Lassi ZS. Predictors of Child’s Health in Pakistan and the Moderating Role of Birth Spacing. International Journal of Environmental Research and Public Health. 2022; 19(3):1759. https://doi.org/10.3390/ijerph19031759
Chicago/Turabian StyleAsif, Muhammad Farhan, Salima Meherali, Ghulam Abid, Muhammad Safdar Khan, and Zohra S. Lassi. 2022. "Predictors of Child’s Health in Pakistan and the Moderating Role of Birth Spacing" International Journal of Environmental Research and Public Health 19, no. 3: 1759. https://doi.org/10.3390/ijerph19031759
APA StyleAsif, M. F., Meherali, S., Abid, G., Khan, M. S., & Lassi, Z. S. (2022). Predictors of Child’s Health in Pakistan and the Moderating Role of Birth Spacing. International Journal of Environmental Research and Public Health, 19(3), 1759. https://doi.org/10.3390/ijerph19031759